
Abstract
Introduction/objective
To examine the effect of depressive symptoms on health-related quality of life (HR-QoL) in Venezuelan patients with rheumatoid arthritis (RA).
Methods
HR-QoL was assessed in a cross-sectional, single-center study of 212 consecutive Venezuelan patients with RA (1987 American College of Rheumatology criteria) using the Medical Outcomes Study Short Form (SF-36), which includes a Physical Composite Scale (PCS) and a Mental Composite Scale (MCS); depressive symptoms were assessed using the Center for Epidemiologic Studies Depression Scale. Covariates included socio-demographics, comorbidities, disease characteristics, body mass index, and disability. Unadjusted and multivariable linear regression analysis were used to determine the effect of depressive symptoms on HR-QoL.
Results
Mean age was 50.2 years and 89.6% were female. Twenty-five percent of patients had depressive symptoms. In the multivariable regression analysis, the presence of depressive symptoms changed the mental SF-36 scores by − 4.81 (p = 0.0052) and the physical SF-36 scores by − 3.33 (p = 0.0527). Other factors significantly associated with scores on the PCS of the SF-36 were functional class, disability and job loss due to RA.
Conclusions
The presence of depressive symptoms negatively affected the HR-QoL in our patients, with a predominant effect on the MCS of the SF-36. The PCS of the SF-36 was mainly affected by those symptoms related to the functional impairment and inflammatory activity of the disease. The routine assessment and early treatment of depressive symptoms, targeting mental and mood manifestations, may improve the HR-QoL and thus contribute to healthier outcomes in Venezuelan RA patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory rheumatic condition affecting 0.5 to 1% of the general population [1]. Previous studies have shown that 13% to 17% of RA patients have a major depressive disorder [2,3,4]. Among several comorbid conditions, depression ranks high among those contributing the most to clinical disease activity [5,6,7], compromising the response to treatment [8, 9], predisposing the patient to disability [10], increasing the risk of stroke [11], suicide [12] and decreasing life expectancy [13]. Depression is a frequent comorbidity in RA patients from Latin America [14,15,16,17], with a reported higher prevalence than in non-Hispanic RA patients [18]. Unfortunately, comorbid depression in RA patients often goes unrecognized and untreated [19].
As a multidimensional concept of individual well-being, health-related quality of life (HR-QoL) is known to be a major determinant of physical, mental, and medical interventions outcomes in chronic diseases in general [20] and in RA, in particular [21, 22]. Previous studies have addressed the impact of depression in the HR-QoL of patients with RA [22, 23,24,25], but to the best of our knowledge such information is scant in patients from Latin America. An inverse correlation between depressive symptoms and HR-QoL was reported in studies of RA patients from Colombia and Uruguay [15, 26, 27]. It is possible that, due to socioeconomic and cultural characteristics, Hispanic RA patients may show differences in responses of their HR-QoL to comorbid conditions such as depression. For instance, Asians patients with RA seem to be less affected by depression as compared to other ethnic populations [28]. In Korean RA patients, pain or fatigue had an effect on QoL only when clustered with depression [22], and in Polish patients with RA the physical symptoms associated with depression had a higher impact on HR-QoL compared with the mental features [23].
Identifying depression in RA is hampered by the commonality of some physical symptoms such as fatigue and sleep disturbances in both conditions. Luckily, a frequently used tool to identify symptoms related to depression, the 20-item questionnaire Center for Epidemiologic Studies Depression Scale (CES-D), contains only three questions actually addressing the physical symptoms of depression [29]. In turn, one of the most commonly used instruments to assess HR-QoL, the 36-item Medical Outcomes Study Short Form (SF-36), produces separate scores for the mental and physical components of HR-QoL [30, 31]. Therefore, both instruments may make it possible to separately attribute the impact of mental and mood depressive symptoms contained in the CES-D scale on either the mental or the physical component of HR-QoL as assessed by the SF-36 instrument. The goal of this study was to examine the effect of depressive symptoms on HR-QoL in Venezuelan patients with RA. We hypothesized that RA patients with depression will have a decreased HR-QoL as compared to those without depression.
Material and methods
Sample
This was a cross-sectional study conducted in a cohort of 224 patients consecutively recruited from the outpatient clinic of the Hospital Universitario de Caracas, a tertiary care center. Patients fulfilled the 1987 criteria of the American College of Rheumatology (ACR) for RA [32] and were all 18-year-old or older. Exclusion criteria were not fulfilling the criteria for Venezuelan nationality (namely, not born in Venezuela, from non-Venezuelan parents) (n = 1), unwillingness to sign the informed consent form (n = 1) and incomplete clinical data (n = 10). Data were collected between 2008 and 2013. Inclusion criteria were age 18 years or older, no co-existing additional autoimmune conditions and willingness to participate in the study by signing an informed consent. Our sample size reached a power of 0.98 to detect a difference of 5.0 in the mean score of the mental component of HR-QoL, and a power of 0.80 to detect a difference of 5.7 in the mean score of the physical component of the HR-QoL between depressed and not depressed patients (STATA/MP 4.2). The study was revised and approved by the Ethics Committee of our hospital and all patients signed an informed consent form.
Measures
Patients underwent clinical assessment and the following data were collected: (a) demographics (age, gender, education, job loss due to RA and marital status); (b) socioeconomic status (SES) assessed with the Graffar classification system as adapted to Venezuela by Mendez-Castellanos and Mendez (I to V, with higher level indicative of lower SES [33]); (c) clinical activity assessed using the Disease Activity Index 28 (DAS28) [34]; (d) disability assessed with the Health Assessment Questionnaire Disability Index (HAQ-DI) [35]; (e) the ACR functional class classification [36] dichotomized into class 1 = normal and non-class 1 = abnormal; (f) body mass index (BMI) calculated by dividing weight in kilograms by the square of height in meters; (g) comorbid conditions (hypertension, diabetes, thyroid disease, asthma, coronary heart disease, cerebrovascular disease, peripheral vascular disease, ulcer gastric, liver disease and cancer); (h) rheumatoid factor (RF), assessed by the latex agglutination test (serum dilution > 1/40); and (i) anti-citrullinated protein antibodies (ELISA ≥ 20 U/dL), assessed by enzyme-linked immunosorbent assay.
Dependent variable
The dependent variable was HR-QoL measured with the SF-36, which consists of 36 items scored in 8 domains relating to an individual’s physical and mental status [30]. The PPCS is a summary of physical functioning (10-items), role limitation because of physical functioning (4-items), bodily pain (2-items) and general health perceptions (5-items). The MCS is a summary of general mental health (5-items), role limitations because of emotional problems (3-items), social functioning (2-items) and vitality (4-items) ratings. The PCS and MCS are global scores that range from 0 to 100, with higher scores indicating better HRQoL [30, 37]. The SF-36 has been translated into Spanish [38] using the methodology of the International Quality of Life Assessment Project [39].
Independent variable
Depressive symptoms were assessed using the Center for Epidemiologic Studies Depression Scale (CES-D) [29] in the version translated into Spanish [40]. The scale consists of 20 items that ask how often specific symptoms were experienced during the past week; responses were scored on a four-point scale (ranging from rarely or none of the time to most or all of the time: 0, 1, 2, 3) with total scores ranging from 0 to 60. A cut-point of 16 or over indicates high depressive symptoms [41]. This was the cut-off selected in our study to identify the presence of depressive symptoms.
Statistical analysis
Descriptive statistics are shown as mean and standard deviations (SD) for continuous variables, and frequencies and percentages for categorical variables. Chi-square and t test were used to describe the characteristics of the sample by depressive symptoms. Unadjusted and adjusted linear regression modeling was used to estimate the β coefficients for the mental and physical components of SF-36 as a function of the depressive symptoms. The multivariable analysis included socio-demographic variables, disease duration (years), job loss due to RA, ACR functional class, BMI, DAS28, HAQ-DI, presence of RF and presence of ACPA. Interaction terms between depressive symptoms and socio-demographics, clinical features and functional status were performed. A p value < 0.05 was considered significant. All analyses were performed using SAS, version 9.4 (SAS Institute, Inc., Cary, NC).
Results
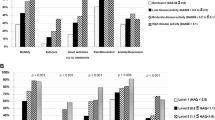
Of the total 224 patients, 10 patients were excluded because of missing information on the CES-D and SF-36, leaving a final sample of 212 patients. The average age was 50.2 ± 11.6 years (mean ± SD), 89.6% were female, and all were of Hispanic ancestry. Mean years of education was 8.6 ± 3.8 (mean ± SD), the majority were in the low SES level (67.9%), and 15.5% had lost their job due to RA. The disease duration was 9.0 ± 8.8 years (mean ± SD), 57.2% were classified as normal ACR functional class, rheumatoid nodules were present in 15.1% of patients and the mean DAS28 and HAQ-DI were 3.4 ± 1.6 and 0.5 ± 0.6 (mean ± SD), respectively. Eighty-five percent and 76.2% tested positive for RF and ACPA, respectively. The mean CES-D score was 12.8 ± 10.08 (mean ± SD). Twenty-five percent of patients had depressive symptoms (CES-D ≥ 16). The mean score for the CMS and PCS of the SF-36 were 49.3 ± 8.2 and 41.9 ± 10.2 (mean ± SD), respectively. Hypertension (34.4%), asthma (9.9%), thyroid disease (5.6%) and diabetes (3.3%) were the most common comorbid conditions (Table 1). Ninety-nine percent of patients were taking a disease modifying anti-rheumatic drug (DMARD) at the time of the study, either as monotherapy or in combination. The most commonly used DMARD was methotrexate (53%), followed by a combination of methotrexate and chloroquine (18.3%), leflunomide (14.9%) and a combination of methotrexate and leflunomide (7.7%). Sixteen percent of patients were receiving a biological DMARD. Table 2 shows the distribution of the sample according to the presence or absence of depressive symptoms. Both groups were comparable, except for higher HAQ-DI scores and asthma prevalence in those RA patients with depressive symptoms (Table 2). No statistically significant differences were seen in the distribution of DMARD or biologics by depressive symptoms. The mean MCS and PCS scores were lower in patients with depressive symptoms (Table 2). To examine the potential effect of disease clinical activity, on depression we stratified our patients in remission < 2.5, low-activity 2.5 to < 3.2, moderate activity 3.2 to ≤ 5.1 and high activity > 5.1, as assessed by the DAS-28 instrument. There was not a statistically significantly association between the level of clinical activity of the disease and depression (p = 0.802).
Tables 3 and 4 present the linear regression analysis for the MCS and PCS of the SF-36. In unadjusted linear regression analysis, depressive symptoms decreased the mental SF-36 scores by 5.64 (p value < 0.0001). After controlling for all covariates, the presence of depressive symptoms showed the same effect in the MCS (β = − 4.81; standard error = 1.69, p value = 0.0052). In the unadjusted linear regression analysis, RA depressive symptoms changed the PCS in RA patients by − 5.03 (p value = 0.0019) and by − 3.33 after controlling for all covariates (p value = 0.0527). Job loss due to RA, ACR functional class and HAQ-DI were all significantly associated with lower PCS scores. Significant interaction terms between depressive symptoms and SES (β = − 14.47 (p value < 0.0001) and between depressive symptoms and job loss (β = − 15.01 (p = 0.0051) were found on the MCS of the SF-36. No significant interaction terms were found on the PCS of the SF-36.
Discussion
In this study, we examined the effect of depression-related symptoms on the mental and physical components of the SF-36 in a sample of Venezuelan patients with RA. Our results suggest that the presence of depressive symptoms has a negative impact on the HR-QoL of RA patients, with a predominant effect on its mental component, and a significant interaction effect between depressive symptoms and low SES and job loss. Psychiatric comorbidities, including anxiety and depression, are very common in RA patients [4], with a peak incidence at age 18–44 and a female predominance [42]. The overwhelming effect of dealing with a painful chronic and incurable condition, and the accompanying social and economic limitations, can take a toll on the patient’s mental and mood status. Limited function, poor coping strategies and weak social support, more common in patients with lower socioeconomic status, are also contributing risk factors [43]. More recent studies have shown that systemic inflammation, via the effect of pro-inflammatory cytokines such as interleukin-6 and interleukin-17, can induce depression by affecting the immune-brain pathway [44]. Besides its deleterious effects in terms of disease outcomes, depression adds to the economic burden of RA by its impact on healthcare utilization, medical expenditure and work productivity [45,46,47]. The prevalence of depressive symptoms in RA varies, ranging from 13 to 42% worldwide [28]. Differences may be related to the diversity of studied populations and mostly to the criteria used for diagnosis of depressive symptoms. In a previous report, we found depression symptoms in 25% of a sample of RA patients using the CES-D instrument [48], similar to our current results in this new cohort. This is a very high frequency when compared to the prevalence of 4% in the Venezuelan general population [49]. Several instruments have been previously used to assess depressive symptoms in RA, including the 14-item Hospital Anxiety and Depression Scale, the Patient Health Questionnaire 9, the Depression Short-Form 8a and the Beck-Depression Inventory, among others. We used the CES-D scale instrument; a cut-off of 16 or greater aids in identifying individuals at risk for depression with good sensitivity, specificity and internal consistency [41]. This is a 20-item questionnaire testing predominantly for the mental and mood status of patients and only three of the 20 questions address depression-related physical symptoms, namely, (1) “I did not feel like eating; my appetite was poor”, (2) “My sleep was restless” and (3) “I could not get ‘going’”. These three symptoms may overlap with physical symptoms due to the underlying chronic inflammation in RA. In turn, the SF-36 instrument allows for a discrimination of the mental and physical components of HR-QoL and provides separate total scores for each [30]. Thus, the use of both instruments may allow for a better discrimination of the effect of mental and mood symptoms related to depression on either the mental or the physical components of HR-QoL. Our results suggest that this can be the case, since the CES-D score correlated strongly with the mental and less with the physical components of HR-QoL. We found an effect of the ACR functional class on the MCS in the multivariable linear regression but not in the unadjusted one, which is probably a negative confounder effect that is, the association of ACR functional class with HR-QoL is biased toward the null hypothesis (no independent effect of ACR function on HR-QoL) in the absence of other explanatory variables in the model. In the adjusted, ACR function loses this negative confounder effect by an interaction with some of the other independent variables in the model. Previous studies have shown correlation between depression and HR-QoL in Asian and Caucasian RA patients [20, 23, 24]. In Latin America, depressive symptoms and disease activity have been observed correlated with lower HR-QoL in RA patients from Colombia [15, 26] and Uruguay [27]. To the best of our knowledge, this is the first report of risk factors affecting HR-QoL in Venezuelan patients with RA. The limitations of our work are its relatively small sample of subjects and its cross-sectional and single-center design that limit its generalizability. In addition, we could not rule out a potential relationship between the severity of the disease and the presence of depression. Its strengths are the ethnic homogeneity of the studied population limiting the influence of race, and the use of a combination of two tests suited to separately identify the effect of mental and mood symptoms of depression on either the mental or the physical components of HR-QoL.
In summary, approximately 25% of this sample of Venezuelan patients with RA have symptoms related to depression. Our results showed that depressive symptoms have a deleterious effect on the mental and physical components of HR-QoL of our patients. As discussed above, depression is a common and serious comorbidity in RA and our study sets a rationale for the systematic assessment and early treatment of depression in RA patients. The therapeutic targeting of mental and mood symptoms can be a way to alleviate the psychological burden in RA patients, improve their HR-QoL and favorably influence their disease course and health outcomes such as response to treatment, work capability, health costs, social independence and increased life expectancy.
References
van der Woude, D., & van der Helm-van Mil, A. H. M. (2018). Update on the epidemiology, risk factors, and disease outcomes of rheumatoid arthritis. Best Practice & Research: Clinical Rheumatology,32, 174–187.
Dickens, C., McGowan, L., Clark-Carter, D., & Med, C. F. (2002). Depression in rheumatoid arthritis: a systematic review of the literature with meta-analysis. Psychosomatic Medicine,64, 52–60.
Matcham, F., Rayner, L., Steer, S., & Hotopf, M. (2013). The prevalence of depression in rheumatoid arthritis. A systematic review and meta-analysis. Rheumatology,52, 2136–2148.
Fiest, K. M., Hitchon, C. A., Bernstein, C. N., et al. (2017). Systematic review and meta-analysis of interventions for depression and anxiety in persons with rheumatoid arthritis. Journal of Clinical Rheumatology,23, 425–434.
Michelsen, B., Kristianlund, E. K., Sexton, J., et al. (2017). Do depression and anxiety reduce the likelihood of remission in rheumatoid arthritis and psoriatic arthritis? Data from prospective multicentre NOR-DMARD study. Annals of the Rheumatic Diseases,76, 1906–1910.
Yilmaz, V., Umay, E., Gϋndoĝdu, I., & Karaahmet, Ö. (2017). Rheumatoid arthritis: Are psychological factors effective in disease flare? European Journal of Rheumatology,4, 127–132.
Leblanc-Trudeau, C., Dobkin, P. L., Carrier, N., et al. (2015). Depressive symptoms predict future simple disease activity index scores and simple disease activity index remission in a prospective cohort of patients with early inflammatory polyarthritis. Rheumatology,54, 2205–2214.
Deb, A., Dwibedi, N., Leasters, T., et al. (2019). Tumor necrosis factor inhibitor therapy and the risk for depression among working-age adults with rheumatoid arthritis. American Health & Drug Benefits,12, 30–38.
Matcham, F., Davies, R., Hotopf, M., et al. (2018). The relationship between depression and biologic treatment response in rheumatoid arthritis. An analysis of the British Society for Rheumatology Biologic Register. Rheumatology,57, 835–843.
Karpouzas, G. A., Draper, T., Moran, R., Moran, R., Hernández, E., Nicassio, P., et al. (2017). Trends in functional disability and determinants of clinically meaningful change over time in Hispanic patients with rheumatoid arthritis in the US. Arthritis Care & Research,69, 294–298.
Tsai, T. Y., Lu, M. C., Livneh, H., Chiu, S. Y., Lai, N. S., & Guo, H. R. (2017). Does depression increase the risk of stroke in patients with rheumatoid arthritis? A population-based cohort study. British Medical Journal Open,7, e014233. https://doi.org/10.1136/bmjopen-2016-014233.
Timonen, M., Viilo, K., Hakko, H., et al. (2003). Suicides in persons suffering from rheumatoid arthritis. Rheumatology,42, 287–291. https://doi.org/10.1093/rheumatology/keg082.
Ang, D. C., Choi, H., Kroenke, K., & Wolfe, F. (2005). Comorbid depression is an independent risk factor for mortality in patients with rheumatoid arthritis. Journal of Rheumatology,32, 1013–1019.
Suárez-Mendoza, A. A., Cardiel, M. H., Caballero-Uribe, C. V., Ortega-Soto, H. A., & Márquez-Marín, M. (1997). Measurement of depression in Mexican patients with rheumatoid arthritis: validity of the Beck depression inventory. Arthritis Care & Research,10, 194–199.
Senra, H., Rogers, H., Leibach, G., Altamar, M. L. P., Plaza, S. L. O., Perrin, P., et al. (2017). Health-related quality of life and depression in a sample of Latin American adults with rheumatoid arthritis. International Journal of Rheumatic Diseases,20, 1684–1693.
Rogers, H. L., Brotherton, H. T., de Luis, A., Olivera-Plaza, S. L., Córdoba-Patiño, A. F., & Peña-Altamar, M. L. (2015). Depressive_symptoms are independently associated with pain perception in Colombians with rheumatoid arthritis. Acta Reumatólogica Portuguesa,40, 40–49.
Juárez-Rojop, I. E., Nolasco-Rosales, G. A., Perez-Mandujano, A., et al. (2019). Prevalence for and factors associated with depression and anxiety in Mexican patients with rheumatoid arthritis. Journal of Clinical Rheumatology. https://doi.org/10.1097/RHU.0000000000001063.
Escalante, A., del Rincon, I., & Mulrow, C. D. (2000). Symptoms of depression and psychological distress among hispanics with rheumatoid arthritis. Arthritis Care & Research,13, 156–167.
Margaretten, M., Julian, L., Katz, P., & Yelin, E. (2011). Depression in patients with rheumatoid arthritis: description, causes and mechanisms. International Journal of Clinical Rheumatology,6, 617–623.
Megari, K. (2013). Quality of life in chronic disease patients. Health Psychology Research,1, e27. https://doi.org/10.4081/hpr.2013.e27.
Wan, S. J., He, H. G., Mak, A., Lahiri, M., Luo, N., Cheung, P. P., et al. (2016). Health-related quality of life and its predictors among patients with rheumatoid arthritis. Applied Nursing Research,30, 176–183.
Kvein, T. S., & Uhlig, T. (2005). Quality of life in rheumatoid arthritis. Scandinavian Journal of Rheumatology,34, 333–341. https://doi.org/10.1080/03009740500327727.
Oh, H., Park, J., & Seo, W. (2019). Identification of symptom clusters and their synergistic effects on quality of life in rheumatoid arthritis patients. International Journal of Nursing Practice,25, e12713. https://doi.org/10.1111/ijn.12713.
Bak, E., Marcisz, B. A., Sternal, D., & Krzemińska, S. (2019). Comparison of health-related quality of life in patients with rheumatoid arthritis during conventional or conventional plus biologic therapy in Poland. Patient Preference and Adherence,13, 223–231.
Hattori, Y., Katayama, M., Kida, D., & Kaneko, A. (2018). Hospital anxiety and depression scale scores is an independent factor associated with the EuroQol 5-dimensional descriptive system in patients with rheumatoid arthritis. Journal of Clinical Rheumatology,24, 308–312.
Cadena, J., Vinaccia, S., Pérez, A., et al. (2003). The impact of disease activity on the quality of life, mental health status, and family disfunction in Colombian patients with rheumatoid arthritis. Journal of Clinical Rheumatology,9, 142–150.
Corbacho, M. I., & Dapueto, J. J. (2010). Assessing the functional status and quality of life of patients with rheumatoid arthritis. Revista Brasileira de Reumatologia,50, 31–43.
Margaretten, M., Yelin, E., Imboden, J., Garf, J., Barton, J., Katz, P., et al. (2009). Predictors of depression in a multiethnic cohort of patients with rheumatoid arthritis. Arthritis and Rheumatism,61, 1586–1591.
Radloff, L. S. (1977). The CES-D scale A self-report depression scale for research in the general population. Applied Psychological Measurement,1, 385–401.
Brazier, J. E., Harper, R., Jones, N. M. B., O’Cathain, A., Thomas, K. J., Usherwood, T., et al. (1992). Validating the SF-36 health survey questionnaire. New outcome measure for primary care. British Medical Journal,305, 160–164.
Khanna, D., & Tsevat, J. (2007). Health-related quality of life. An introduction. The American Journal of Managed Care,13, S218–S223.
Arnett, F. C., Edworthy, S., Bloch, D. A., et al. (1988). The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis and Rheumatism,31, 315–324.
Mendez-Castellanos, H., & Mendez, M. C. (1986). Estratificación social y biológica humana: método Graffar modificado. Archivos Venezolanos de Puericultura y Pediatría,49, 93–104.
van Riel, P. L. C. M. (2014). The development of the disease activity score (DAS) and the disease activity score using 28 joint counts (DAS28). Clinical and Experimental Rheumatology,32(Suppl. 85), S65–74.
Bruce, B., & Fries, J. F. (2003). The Stanford health assessment questionnaire: Dimensions and practical applications. Health and Quality of Life Outcomes,1, 20–25.
Hochberg, M. C., Chang, R. W., Dwosh, I., Lindsay, S., Pincus, T., & Wolfe, F. (1992). The American College of Rheumatology 1991 revised criteria for the classification of global functional status in rheumatoid arthritis. Arthritis and Rheumatism,35, 498–502.
Schalock, R. L., Bonham, G. S., & Verdugo, M. A. (2008). The conceptualization and measurement of quality of life Implications for program planning and evaluation in the field of intellectual disabilities. Evaluation and Program Planning,31, 181–190.
Alonso, J., Prieto, A. J., & Antó, J. M. (1995). The Spanish version of the SF-36 Health Survey (the SF-36 health questionnaire): an instrument for measuring clinical results. Medical Clinics,104, 771–776.
Ware, J. E., Jr., Snow, K. K., Kosinski, M., & Gandek, B. (1993). SF-36 Health Survey: manual and interpretation guide. Boston: New England Medical Center.
González, V. M., Stewart, A., Ritter, P. L., Stewart, A., Ritter, P., & Lorig, K. (1995). Translation and validation of arthritis outcome measures into Spanish. Arthritis and Rheumatism,38, 1429–1446.
Lewinsohn, P. M., Seeley, J. R., Roberts, R. E., & Allen, N. B. (1997). Center for epidemiology studies depression scale (CES-D) as a screening instrument for depression among community-residing older adults. Psychology Aging,12, 277–287.
Marrie, R. A., Hitchon, C. A., Walld, R., et al. (2018). Increased burden of psychiatric disorders in rheumatoid arthritis. Arthritis Care & Research,70, 970–978. https://doi.org/10.1002/acr.23539.
Margaretten, M., Julian, L., Katz, P., & Yelin, E. (2011). Depression in patients with rheumatoid arthritis: Description, causes and mechanisms. International Journal of Clinical Rheumatology,6, 617–623. https://doi.org/10.2217/IJR.11.6.
Li, Y. C., Chou, Y. C., Chen, H. C., Lu, C. C., & Chang, D. M. (2019). Interleukin-6 and interleukin-17 are related to depression in patients with rheumatoid arthritis. J Rheum Dis. https://doi.org/10.1111/1756-185X.13529.
Li, N., Chan, E., & Peterson, S. (2019). The economic burden of depression among adults with rheumatoid arthritis in the United States. J Med Econom,22, 372–378.
Deb, A., Dwbedi, N., LeMasters, T., Hornsby, J. A., Wei, W., & Sambamoorthi, U. (2018). Burden of depression among working-age adults with rheumatoid arthritis. Arthritis. https://doi.org/10.1155/2018/8463632.
Margaretten, M., Barton, J., Julian, L., et al. (2011). Socioeconomic determinants of disability and depression in patients with rheumatoid arthritis. Arthritis Care & Research,63, 240–246.
Rivero-Carrera, N. N., Serra-Bonett, N., Al Snih, S., et al. (2011). Risk factors associated with depressive symptoms in Venezuelan patients with rheumatoid arthritis. Journal of Clinical Rheumatology,17, 218–219. https://doi.org/10.1097/RHU.0b013e31821c7af3.
Depression and Other Common Mental Disorders Global Health Estimates. https://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017.2-eng.pdf.
Acknowledgements
The authors acknowledge the assistance of Sarah Toombs Smith, PhD, ELS, in article preparation. Dr. Toombs Smith received no compensation for this effort beyond her salary at the UTMB Sealy Center on Aging. Dr. Rodriguez is a Visiting Scholar at the Sealy Center on Aging and is partly supported by a grant from IIE-Scholar Rescue Fund.
Funding
Authors received no funding for this work from any public or private organization.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Authors declare no conflict of interest and received no funding for this work from any public or private organization. Dr. Natali Serra-Bonett was working at Centro Nacional de Enfermedades Reumaticas, Hospital Universitario de Caracas, Caracas, Venezuela at the time of her participation in this study. Currently she is MSL Lead Mexico at AbbVie, Santa Cruz Xochitepec, Mexico City, Mexico.
Ethical approval
The study was revised and approved by the Ethics Committee of our hospital and all patients signed an informed consent form. We have full control of all primary data and we agree to allow the journal to review the data supporting our study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Rodríguez, M.A., Rivero-Carrera, N.N., Rey-Puente, J.C. et al. Role of depressive symptoms in the health-related quality of life of Venezuelan patients with rheumatoid arthritis. Results from a tertiary care center. Qual Life Res 29, 2129–2136 (2020). https://doi.org/10.1007/s11136-020-02485-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-020-02485-7