
Abstract
Purpose
A large literature shows important effects of self-esteem and stress on mental and physical health in young adulthood. Negative life events are one type of stressor associated with poor health, but it is less clear whether more neutral stressors are also associated with poor health. This study contributes to the existing literature by investigating the association between different types of stressful life events, self-esteem, and health during the transition from adolescence to early adulthood in Switzerland.
Methods
We draw on the “Transitions from Education to Employment” (TREE) panel study, a nationally representative longitudinal survey of a cohort of Swiss young adults, using logistic regression analysis. The study includes eight waves over a 10-year period, from 2001, average age 16, to 2010, average age 26. Our dependent variable is a dichotomized health self-assessment, and key independent variables include self-esteem and three measures of cumulative significant life events (SLEs): total cumulative SLEs, cumulative negative SLEs, and cumulative neutral SLEs.
Results
Self-esteem had a significant positive impact on health, whereas cumulative SLEs had a significant negative impact. Negative SLEs had a larger negative impact than total SLEs, and neutral SLEs had a smaller impact. Considered individually, negative SLEs were more likely to have a significant negative impact on health.
Conclusions
In addition to their known influence on mental health, stress and self-esteem are important factors influencing individuals’ general health, even in adolescence and young adulthood. While all types of stressors have a negative impact on health, the negative stressors seem to have more prominent effects than neutral stressors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The transition from childhood to adulthood involves various physical, psychological, and socio-emotional changes. During this period, mental health problems like anxiety and depression emerge or become more prevalent [1,2,3,4]. Self-esteem and stress are two important factors associated with adolescent health outcomes.
Self-esteem is an important part of adolescent health and well-being [5, 6]. Self-esteem can be defined as an “individual’s set of thoughts and feelings about his or her own worth and importance” [5]. Self-esteem tends to stabilize during adolescence and young adulthoods [7], with young men typically having somewhat higher levels of self-esteem than young women [8, 9]. Self-esteem has a protective effect on health, with high self-esteem associated with better mental and physical health outcomes in adolescence and adulthood [10,11,12,13,14,15].
Stress is often defined as “any environmental, social, or internal demand which requires the individual to readjust his/her usual behavior patterns” [16]. Studies in adult populations show that high levels of stress are associated with numerous physical health problems, including greater risk of cardiovascular disease and immune-suppressant effects [17, 18], but fewer studies look at the effects of stress on general health for adolescents and young adults [19]. Some authors have suggested that the time-frame over which stress affects general health is too long to be observed in adolescence [20]. However, several recent studies in young adults find associations between various stress measures and physical health outcomes, including cardiovascular and metabolic disease risks [21] and adiposity levels [22].
Stress is often measured through life events [23]. Significant life events (SLEs) are acute changes, such as parents’ divorce or a severe accident. Research suggests that experiencing multiple, consecutive SLEs may have a cumulative effect on health outcomes [24, 25]. Research evidence further highlights that increased cumulative adversity is associated with the increased risk of psychological distress, mental health disorders, and poor health behaviors. It is also linked to the onset of depression and anxiety [26]. Some scholars criticize SLE measures, arguing that such “check-list approaches” are driven by researchers’ opinions regarding what is stressful, rather than by adolescents’ perceptions [19]. There is further debate about which types of events are stressful. Some scholars focus on negative or traumatic events [23, 26], whereas others find that even more neutral events, like moving or changing schools, can have negative effects if they are frequent enough [24].
This study contributes to the existing literature by investigating the association between cumulative stress, self-esteem, and general health during the transition from adolescence to early adulthood. Health self-assessments have been shown to be an important indicator of general health in adult and adolescent populations [27], so we use self-assessed health as our general health measure.
Drawing on longitudinal data on experiences of SLEs over a 10-year period, it also examines whether different types of SLEs have different impacts on health. We hypothesize that the association between mental health issues and stress and self-esteem are also found when examining general health and that negative SLEs have a greater negative impact on health than neutral SLEs. This leads to three hypotheses:
Higher average self-esteem in adolescence and early adulthood decreases odds of less than good health in early adulthood.
FormalPara Hypothesis 2Higher levels of cumulative SLEs in adolescence and early adulthood increase odds of less than good health in early adulthood.
FormalPara Hypothesis 3Higher levels of cumulative negative SLEs in adolescence and early adulthood have a greater negative impact on health than higher levels of cumulative neutral/ambivalent SLEs.
Methods
Data
We drew on data from the “Transitions from Education to Employment” (TREE) panel study, a longitudinal survey of a representative sample of Swiss young adults who finished compulsory schooling in 2000 [28]. As a social science survey with no medical component, this study is not subject to institutional review in Switzerland. We analyzed data from eight waves of the survey, including data collected annually between 2001 and 2007 and once more in 2010. The average age of the young adults was 16 years in 2000, at the beginning of the study, and 26 years in 2010.
The initial sample included 6343 students who participated in the PISA 2000 study. Response rates per wave are strong overall, ranging from a high of 89% in 2005 to a low of 75% in 2010. Due to sample attrition, only 4505 participants were contacted for wave 8 of the survey. Of these, 3424 individuals responded, representing 54% of the 2001 sample. Analysis found several factors that were associated with non-response or sample attrition, including reading proficiency, foreign origin, gender, and having an incomplete family. The final sample underrepresents youth with low reading proficiency, young men, youths of foreign origin, and youth from incomplete families who did not live in the family home over the whole study period [29]. In all analyses, we employed wave eight panel weights to correct for this.
Dependent variable: self-assessed health
In wave eight of the survey, respondents were asked to assess their health on a 5-point ordinal scale, ranging from very bad to very good. The 2749 individuals who answered this health self-assessment question are included in our analysis. This represents 80.3% of the wave eight sample. Non-responders to the health self-assessment question are slightly more likely to be male than female, to come from the French- or Italian-speaking parts of Switzerland, to have low education, and to experience fewer SLEs of all kinds.
In this young sample, responses to the health self-assessment question are heavily skewed toward “good” and “very good,” with over 80% of both men and women choosing one of these two options. As such, we recoded this variable as a binary variable, with 1 indicating average health or worse and 0 indicating good health or better.
Independent variables
Our main interest is the effect cumulative stress and self-esteem on health, but we included other relevant control variables, including gender, education, area of residence (urban or rural), and language region (German-speaking, French-speaking, and Italian-speaking). Controlling for language region is particularly important in the Swiss context as past studies have found substantial differences in the general health status of young adults across different language regions [30]. Gender, urban/rural residence, and language region were determined at the time of the original PISA 2000 survey. There are no missing data for these variables.
We determined respondents’ education based on diplomas and certificates received since the second TREE survey wave in 2002. In addition, certificate and diploma data were comprehensively verified and corrected in TREE survey wave seven in 2007. Based on these data, we constructed a measure of respondents’ education with three levels: less than upper secondary, upper secondary, and tertiary. We call these low, medium, and high education. There are no missing data for this variable.
Self-esteem
We measured self-esteem using a modified version of the Rosenberg self-esteem scale [31], which is the most commonly used and well-validated measure of global self-esteem [32]. Most survey waves only included eight of the items included on the scale, so we only include those items. We averaged the scores for those eight items in all waves to determine the average Rosenberg Self-Esteem Score (RSES), with a score ranging from 0 to 4. For analysis, respondents were allocated into quartiles based on their average RSES. The first quartile has average RSES ranging from 0 to 2.69, the second quartile has average RSES ranging from 2.69 to 3.025, the third quartile has average RSES ranging from 3.025 to 3.358, and the fourth quartile has average RSES ranging from 3.358 to 4.
Missing data on various index questions in various waves pose a problem for this measure. Slightly under half of respondents (1286) are missing responses at least one item in one wave. However, no respondent is missing data across all waves. As such, no exclusions were made due to missing values, and average RSES represents the average RSES for all waves including data on this measure. Analyses including this measure included a control variable indicating missing data on some items.
Cumulative stress
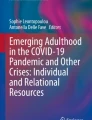
All waves of the survey asked individuals about SLEs experienced in the last year or since the last survey wave. Figure 1 shows which questions were asked in which waves and indicates what proportion of respondents experienced at least one event of that type and the range in the number of events per type respondents experienced.

Significant life event questions by wave
Events included in the lists vary across survey waves, reflecting new stages in the life course. Further, not all events are clearly negative. Some may be neutral or even positive events, like moving or getting married. Others, like getting pregnant/getting someone pregnant and having a child, are ambivalent. They may have been negative or positive events, depending on individual circumstances.
We explored the impact each of these types of events had on health individually as well as the impact of three separate measures of cumulative SLEs: a measure including all SLEs, a measure including only negative SLEs, and a measure including only neutral or ambivalent SLEs. To calculate the measures, we summed all reports of included SLEs across all waves, representing cumulative stress over a decade from approximately age 16 to approximately age 26. For the total SLE measure, we included all 16 SLE types. For the negative SLE measure, we included 10 SLE types, all except the ones related to moving, “I got married,” “I became a mum/dad,” and “I got pregnant/I got a girl pregnant.” The neutral SLE measure included a count of the remaining 6 SLE types.
For analysis, respondents were allocated into quartiles based on their cumulative SLE scores. For the total SLE measure, the first quartile has cumulative SLE score of 0–4, the second quartile of 5–7, the third quartile of 8–10, and the fourth quartile of 11 or more. For the negative SLE measure, the first quartile has a cumulative negative SLE score of 0–2, the second quartile of 3–4, the third quartile of 5–7, and the fourth quartile of 8 or more. For the neutral SLE measure, the first quartile has a cumulative neutral SLE score of 0–1, the second quartile of 2, the third quartile of 3–4, and the fourth quartile of 5 or more.
Missing data pose a problem for these measures. Most respondents (1755) are missing data on at least one SLE question in one survey wave, although no respondent is missing data for all SLE questions. No exclusions were made due to missing values, and cumulative SLEs represent the total number of SLEs reported. Analyses including this measure included a control variable indicating missing data on some items.
Statistical analysis
We conducted all analyses using Stata 12 [33]. To correct for sample attrition and clustering, we employed wave eight sample weights in all analyses [29]. We calculated the unadjusted and adjusted odds of reporting less than good health for each independent variable. To account for missing data on some items included in our three cumulative SLE measures and the average RSES measure, we included missing data dummy variables in all logistic regression analyses including these measures. We constructed one missing data dummy per measure, coded one if the respondent is missing data on any item in any wave.
Our dependent variable is the binary transformation of the health self-assessment discussed above, coded one for average health or worse. To account for this, we used logistic regression techniques. Results are reported as odds ratios with 95% confidence intervals.
We began by testing five models. First, we employed bivariate logistic regression analyses to calculate unadjusted odds of reporting less than good health for each independent variable in turn. We then carried out multivariate logistic regression analyses to test the effects of our various cumulative SLE measures and average RSES on health. Model 0 reports unadjusted odds ratios. Our baseline model, Model 1, included gender, language region, urban/rural residence, and education, and Model 2 added average RSES to the baseline model. Model 3 added cumulative SLEs to the baseline model, and Model 4 included both the cumulative SLE and average RSES measures. Models with the average RSES or cumulative SLE measures included corresponding missing data controls. Results, not reported here, found no significant association between missing data on these measures and self-assessed health. We also tested 16 alternative cumulative SLE measures, each excluding one type of SLE, to confirm that effects were consistent across measures and not driven by a single potential stressor. Effects with alternative measures were similar to those reported above and are available on request.
To test Hypothesis 3, we first examined the individual effect of each type of SLE on health. It was not possible to allocate respondents into quartiles when examining individual SLEs, so we examined the effects of SLEs as a count variable, reporting β-coefficients and standard errors from Models 0, 3, and 4 bi- and multivariate logistic regressions. Finally, we repeated analyses from Models 3 and 4 for neutral and negative SLEs separately and then together.
In addition to these analyses, we also examined the interaction of gender with self-esteem and stress on self-assessed health, which is a point of debate in the literature [34, 35]. We found no significant differences between the effects of self-esteem or stress on health by gender. Results of these analyses are not reported here, but they are available on request.
Results
Descriptive statistics
Sample characteristics for the total sample and by gender are summarized in Table 1. We report proportions and unweighted N for all variables.
Bivariate analyses found no significant differences between men and women for health status (design-based F = 1.39, p = 0.2383), language region (design-based F = 1.90, p = 0.1643), urban/rural residence (design-based F = 0.04, p = 0.8372), or education (design-based F = 1.28, p = 0.2762). However, women are over-represented in higher cumulative SLE quartiles for all measures (total SLE: design-based F = 12.89, p = 0.0000; negative SLE: design-based F = 4.77, p = 0.0030; neutral SLE: design-based F = 21.99, p = 0.0000) and lower self-esteem quartiles (design-based F = 4.77, p = 0.0031).
Logistic regression analyses
We report results from our logistic regressions in three tables. Table 2 shows results from our five models for average RSES and the cumulative SLE measure. Tables 3 and 4 examine the effects of different types of SLEs in greater detail, reporting results from Models 0, 3, and 4 with different SLE measures. Table 3 reports for individual SLEs, and Table 4 for negative and neutral SLEs.
For the total sample, our baseline model identified only two variables that were significantly associated with less than good health. Odds of reporting less than good health ranged from a low of 2.86 (unadjusted odds, Model 0) to a high of 3.80 (adjusted odds, Model 4), meaning that young adults from the Italian-speaking region had approximately three times larger odds of reporting less than good health than young adults from the French-speaking region. In addition, we found that high education was associated with better health. Young adults with high education had half the odds of reporting less than good health than the reference group, young adults with medium education (ranging 0.48–0.57, depending on the model).
We found that higher average self-esteem was associated with decreasing odds of reporting less than good health. Odds of reporting less than good health decreased progressively as average RSES increased. While there were no significant differences in health outcomes for individuals in the second quartile, individuals in the third quartile had half the odds of reporting less than good health of individual in the first quartile (ranging from 0.41 to 0.47), and individuals in the fourth quartile had one-tenth the odds of doing so (ranging from 0.08 to 0.10).
In support of Hypothesis 2, individuals in the highest cumulative SLE quartile had higher odds of reporting less than good health than respondents in the lowest quartile, indicating that individuals in this group had approximately two and half times the odds of reporting less than good health than individuals in the reference group. However, no other quartile group showed significant differences from the low-SLE reference group.
Eight SLE types had a negative effect on health in at least one model: “my parents got separated or divorced,” “I had a grave accident or illness,” “A person who was close to me died,” “I went through an unhappy relationship,” “I had a serious row at school or work,” “I became a mum/dad” “Somebody I am very close to had a grave accident or illness,” and “Somebody I am very close to lost his/her job.” Effects held across all models for all SLE types except “I became a mum/dad” (only significant in bivariate analysis) and “I went through an unhappy relationship” (not significant when we controlled for self-esteem). Seven of these SLE types were included in our negative SLE measure, and only one (“I became a mum/dad”) was included in our neutral/ambivalent SLE measure.
The patterns of results for negative SLEs were very similar to findings regarding all SLEs. Individuals in the highest quartile of cumulative negative SLEs had significantly higher odds of reporting less than good health than individuals in the lowest quartile, with individuals in this group having three to four times the odds of reporting less than good health than individuals in the reference group across all models, including bivariate analysis, multivariate analysis not controlling for neutral SLEs, and multivariate analysis controlling for neutral SLEs.
The pattern of effects for neutral SLEs was different and more complex. In bivariate analysis, respondents in the second quartile of cumulative neutral SLEs had significantly lower odds of reporting less than good health than individuals in the first quartile, with individuals in this group having half the odds of reporting less than good health than individuals in the reference group. In multivariate analysis not controlling for negative SLEs, respondents in the third quartile had significantly increased odds of reporting less than good health (ranging from 1.83 to 1.94). In multivariate analysis controlling for negative SLEs, the second cumulative neutral SLE quartile group had decreased odds of reporting less than good health in the Model 3 specification. This effect disappeared when controlling for self-esteem in Model 4.
Discussion
Three key findings from our study are as follows:
-
1.
Higher average RSES is strongly associated with decreased odds of reporting less than good health (in support of Hypothesis 1).
-
2.
Reporting large numbers of SLEs increases odds of reporting less than good health (in support of Hypothesis 2).
-
3.
Negative SLEs have a larger negative effect on health than neutral or ambivalent SLEs.
In keeping with past studies [14, 15], we found a strong positive association between higher self-esteem and better self-rated health. This finding particularly held true for respondents with very high self-esteem, who had approximately ten times greater odds of reporting good health than respondents with very low self-esteem.
Also in keeping with the literature [23, 24, 26], we found that reporting more cumulative SLEs was associated with increased odds of reporting worse health. However, all SLEs did not have the same effect. When examining SLEs individually, we found that seven of the ten negative SLE types had a significant negative association with health. Only one neutral SLE type had a negative association, and it disappeared in multivariate analysis. These individual effects provide support for Hypothesis 3. Further supporting Hypothesis 3, when we examined the effect of negative and neutral SLEs on health separately, we found stronger negative effects for the cumulative negative SLE measure than for the cumulative neutral SLE measure. Furthermore, this negative effect held when testing the effect of cumulative negative and neutral SLEs simultaneously, whereas the effect of cumulative neutral SLEs disappeared. This suggests that negative or traumatic events, like divorce or the death of a loved one, have a larger or longer-lasting impact on health than more neutral or ambivalent SLEs, like moving.
Our analysis of neutral SLEs still found an association between higher numbers of SLEs and health, but both the direction and the strength of associations varied by model, suggesting that any effects are not robust.
In line with other studies [19, 23, 24, 36], we conclude that efforts should be taken to promote and strengthen adolescents’ self-esteem and help adolescents deal with stress. In keeping with a life-course perspective, our findings highlight the need to address stress and promote self-esteem early—even before adolescence. This would help support both positive mental and physical health outcomes.
Limitations
The study also had some limitations. While the longitudinal design of this study is a significant advantage over cross-sectional studies, health status was only assessed in wave eight of the study. As such, we had no baseline health status and thus cannot measure change in health status. This means that we had no way of knowing how health status at wave 8 differs from health status in earlier waves. Sample attrition and its impact on the representativeness of the sample are also a concern.
In addition, the SLE measure we used to assess cumulative stress forces us as researchers to decide which events are likely to be “negative” or “neutral.” This “check-list approach” [19] does not allow consideration of adolescents’ own perceptions of events. In general, a more nuanced understanding of adolescent stress requires qualitative approaches that allow people to explain what stress means to them and how they experience it [37,38,39].
References
Copeland, W., Shanahan, L., Costello, E. J., & Angold, A. (2011). Cumulative prevalence of psychiatric disorders by young adulthood: A prospective cohort analysis from the Great Smoky Mountains Study. Journal of the American Academy of Child & Adolescent Psychiatry, 50, 252–261. https://doi.org/10.1016/j.jaac.2010.12.014.
Costello, E. J., Copeland, W., & Angold, A. (2011). Trends in psychopathology across the adolescent years: What changes when children become adolescents, and when adolescents become adults? Journal of Child Psychology and Psychiatry, 52, 1015–1025. https://doi.org/10.1111/j.1469-7610.2011.02446.x.
Merikangas, K. R., He, J.-P., Burstein, M., et al. (2010). Lifetime prevalence of mental disorders in U.S. adolescents: Results from the National Comorbidity Survey Replication–Adolescent Supplement (NCS-A). Journal of the American Academy of Child & Adolescent Psychiatry, 49, 980–989. https://doi.org/10.1016/j.jaac.2010.05.017.
Ge, X., Lorenz, F. O., Conger, R. D., et al. (1994). Trajectories of stressful life events and depressive symptoms during adolescence. Developmental Psychology, 30, 467–483. https://doi.org/10.1037/0012-1649.30.4.467.
Moksnes, U. K., Bradley Eilertsen, M.-E., & Lazarewicz, M. (2016). The association between stress, self-esteem and depressive symptoms in adolescents. Scandinavian Journal of Psychology, 57, 22–29. https://doi.org/10.1111/sjop.12269.
Orth, U., & Robins, R. W. (2014). The development of self-esteem. Current Directions in Psychological Science, 23, 381–387. https://doi.org/10.1177/0963721414547414.
Trzesniewski, K. H., Donnellan, M. B., & Robins, R. W. (2003). Stability of self-esteem across the life span. Journal of Personality and Social Psychology, 84, 205–220. https://doi.org/10.1037/0022-3514.84.1.205.
Kling, K. C., Hyde, J. S., Showers, C. J., & Buswell, B. N. (1999). Gender differences in self-esteem: A meta-analysis. Psychological Bulletin, 125, 470–500.
Baldwin, S. A., & Hoffmann, J. P. (2002). The dynamics of self-esteem: A growth-curve analysis. Journal of Youth and Adolescence, 31, 101–113. https://doi.org/10.1023/A:1014065825598.
Dumont, M., & Provost, M. A. (1999). Resilience in adolescents: Protective role of social support, coping strategies, self-esteem, and social activities on experience of stress and depression. Journal of Youth and Adolescence, 28, 343–363. https://doi.org/10.1023/A:1021637011732.
Moksnes, U. K., & Espnes, G. A. (2013). Self-esteem and life satisfaction in adolescents-gender and age as potential moderators. Quality of Life Research, 22, 2921–2928. https://doi.org/10.1007/s11136-013-0427-4.
Bovier, P., Chamot, E., & Perneger, T. V. (2004). Perceived stress, internal resources, and social support as determinants of mental health among young adults. Quality of Life Research, 13, 161–170. https://doi.org/10.1023/B:QURE.0000015288.43768.e4.
Moksnes, U. K., Moljord, I. E. O., Espnes, G. A., & Byrne, D. G. (2010). The association between stress and emotional states in adolescents: The role of gender and self-esteem. Personality and Individual Differences, 49, 430–435. https://doi.org/10.1016/j.paid.2010.04.012.
Orth, U., Robins, R. W., & Widaman, K. F. (2012). Life-span development of self-esteem and its effects on important life outcomes. Journal of Personality and Social Psychology, 102, 1271–1288. https://doi.org/10.1037/a0025558.
Trzesniewski, K. H., Donnellan, M. B., Moffitt, T. E., et al. (2006). Low self-esteem during adolescence predicts poor health, criminal behavior, and limited economic prospects during adulthood. Developmental Psychology, 42, 381–390.
Thoits, P. A. (1995). Stress, coping, and social support processes: Where are we? What next? Journal of Health and Social Behavior, 35, 53. https://doi.org/10.2307/2626957.
Cohen, S., & Williamson, G. M. (1991). Stress and infectious disease in humans. Psychological Bulletin, 109, 5–24. https://doi.org/10.1037//0033-2909.109.1.5.
McEwen, B. S. (1993). Stress and the individual: Mechanisms leading to disease. Archives of Internal Medicine, 153, 2093–2101. https://doi.org/10.1001/archinte.1993.00410180039004.
Moksnes, U. K. (2011). Stress and health in adolescents: The role of potential protective factors. Trondheim: Norwegian University of Science and Technology.
Byrne, D. G., Davenport, S. C., & Mazanov, J. (2007). Profiles of adolescent stress: The development of the adolescent stress questionnaire (ASQ). Journal of Adolescence, 30, 393–416. https://doi.org/10.1016/j.adolescence.2006.04.004.
Fuligni, A. J., Telzer, E. H., Bower, J., et al. (2009). A preliminary study of daily interpersonal stress and C-reactive protein levels among adolescents from Latin American and European backgrounds. Psychosomatic Medicine, 71, 329–333. https://doi.org/10.1097/PSY.0b013e3181921b1f.
van Jaarsveld, C. H. M., Fidler, J., Steptoe, A., et al. (2009). Perceived stress and weight gain in adolescence: A longitudinal analysis. Obesity, 17, 2155–2161. https://doi.org/10.1038/oby.2009.183.
Kim, K. J., Conger, R. D., Elder, G. H., & Lorenz, F. O. (2003). Reciprocal influences between stressful life events and adolescent internalizing and externalizing problems. Child Development, 74, 127–143. https://doi.org/10.1111/1467-8624.00525.
Boynton-Jarrett, R., Hair, E., & Zuckerman, B. (2013). Turbulent times: Effects of turbulence and violence exposure in adolescence on high school completion, health risk behavior, and mental health in young adulthood. Social Science & Medicine, 95, 77–86. https://doi.org/10.1016/j.socscimed.2012.09.007.
Fairbank, J. A., & Fairbank, D. W. (2009). Epidemiology of child traumatic stress. Current Psychiatry Reports, 11, 289–295. https://doi.org/10.1007/s11920-009-0042-9.
Turner, R. J., & Lloyd, D. A. (2004). Stress burden and the lifetime incidence of psychiatric disorder inyoung adults. Archives of General Psychiatry, 61, 481. https://doi.org/10.1001/archpsyc.61.5.481.
Boardman, J. D. (2006). Self-rated health among U.S. adolescents. Journal of Adolescent Health, 38, 401–408. https://doi.org/10.1016/j.jadohealth.2005.01.006.
TREE (ed.). (2013). TREE project documentation 2000–2012. Basel: TREE.
Sacchi, S. (2011). Construction of TREE panel weights: Documentation for the panel waves from 2000 to 2010. Basel: TREE.
Abel, T., Hofmann, K., & Schori, D. (2013). Social and regional variations in health status and health behaviours among Swiss young adults. Swiss Medical Weekly. https://doi.org/10.4414/smw.2013.13901.
Rosenberg, M. (1979). Conceiving the self. New York: Basic Books.
Robins, R. W., Hendin, H. M., & Trzesniewski, K. H. (2001). Measuring global self-esteem: Construct validation of a single-item measure and the Rosenberg Self-Esteem Scale. Personality and Social Psychology Bulletin, 27, 151–161. https://doi.org/10.1177/0146167201272002.
StataCorp, L. P. (2011). Stata statistical software: Release 12. 2011. https://doi.org/10.2307/2234838.
Nolen-Hoeksema, S. (2001). Gender differences in depression. Current Directions in Psychological Science, 10, 173–176. https://doi.org/10.2307/20182732.
Hankin, B. L., Mermelstein, R., & Roesch, L. (2007). Sex differences in adolescent depression: Stress exposure and reactivity models. Child Development, 78, 279–295. https://doi.org/10.1111/j.1467-8624.2007.00997.x.
Wilburn, V. R., & Smith, D. E. (2005). Stress, self-esteem, and suicidal ideation in late adolescents. Adolescence, 40, 33–45.
Compas, B. E., Davis, G. E., Forsythe, C. J., & Wagner, B. M. (1987). Assessment of major and daily stressful events during adolescence: The Adolescent Perceived Events Scale. Journal of Consulting and Clinical Psychology, 55, 534–541. https://doi.org/10.1037/0022-006X.55.4.534.
Seiffge-Krenke, I. (2000). Causal links between stressful events, coping style, and adolescent symptomatology. Journal of Adolescence, 23, 675–691. https://doi.org/10.1006/jado.2000.0352.
Chandra, A., & Batada, A. (2006). Exploring stress and coping among urban African American adolescents: The Shifting the Lens study. Preventing Chronic Disease, 3, A40.
Acknowledgements
The authors would like to thank the following individuals for their contributions to this article: The TREE (Transition from Education to Employment) project team especially Dr. Sandra Hupka-Brunner and Thomas Meyer, as well as Prof. Dr. Thomas Abel for comments and suggestions. Constanze Pfeiffer was funded by a Marie Heim-Vögtlin (MHV) fellowship of the Swiss National Science Foundation (SNSF). The SNSF was not involved in the research for and preparation of this article. We would also like to thank the Editorial Offices at Social Science and Medicine and Quality Life Research and four anonymous reviewers for very helpful feedback on earlier drafts of this paper. We presented an earlier version of the research reported in this article in Lucerne, Switzerland on January 29, 2015 at Promotion Santé Suisse’s 16th annual conference: “16e Conférence nationale sur la promotion de la santé: Promouvoir notre santé tout au long de la vie.” We confirm that all people who contributed significantly to this work are listed here.
Funding
Constanze Pfeiffer was funded by a Marie Heim-Vögtlin (MHV) fellowship from the Swiss National Science Foundation (SNSF) (Grant Number PMPDP1-173902).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
As a social science survey with no medical component, this study is not subject to institutional review in Switzerland. All procedures performed in studies involving human participants were in accordance with the ethical standards of the 1964 Helsinki declaration and its later amendments.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Jafflin, K., Pfeiffer, C. & Bergman, M.M. Effects of self-esteem and stress on self-assessed health: a Swiss study from adolescence to early adulthood. Qual Life Res 28, 915–924 (2019). https://doi.org/10.1007/s11136-018-2059-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-018-2059-1