
Abstract
Purpose
Self-reported health-related quality of life (HRQoL) represents one central indicator for the need of prevention or intervention with gaining importance for public health monitoring. As part of this framework, the present study aims to identify potentially supportive factors of HRQoL and to determine age-related differences.
Methods
In a sample of young to older adults (18–79 years; M = 52.71, SD = 16.06) from the German Health Interview and Examination Survey for Adults (DEGS1 subsample, n = 3667, 52% female), we investigated interrelations between individual (e.g., chronic condition), social (e.g., social support), and lifestyle factors (e.g., healthy eating) and executive functioning with the physical composite scale (PCS) and the mental composite scale (MCS) of HRQoL with the help of path analyses. Secondly, we performed multiple regression analyses to determine age interactions.
Results
Results suggest direct and indirect paths on PCS, respectively, MCS from various lifestyle factors and executive functioning in addition to individual and social factors with a good model fit (PCS: CD = .63, SRMR = .001; MCS: CD = .64, SRMR = .003). Furthermore, results suggest physical activity and healthy eating to become particularly relevant with advancing age (age group × physical activity on PCS, β = .09, p < .05; age group × healthy eating on MCS, β > .50, p < .01).
Conclusions
Several lifestyle factors and executive functioning offer the potential to promote HRQoL in the everyday life of individuals at various ages, independent of individual or social determinants. Public health action might want to foster behavioral multicomponent approaches supporting healthy aging.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Across the lifespan, at some points individuals have to face losses in their physical or mental health, such as when experiencing adverse life events, or acute or chronic diseases. As a consequence, individuals frequently show short- and long-term decreases in their health-related quality of live (HRQoL). More precisely, mobility and productivity constraints [1], frailty [2], feelings of loneliness or isolation, and the rise of mental disorders [3] were identified as negative consequences related to a reduced HRQoL. Hence, the question arises on how to meet this kind of life challenges in order to avoid the reduction or consolidation of constraints of HRQoL as well as everyday consequences in the long run. One central aim of current public health research is to identify risk and supportive factors for the prevention or intervention of health problems [4]. In this context, subjective reports on the current physical and mental health status play a key role for indicating disease severity and the need, or success of interventions [4]. Beyond somatic indication, the concept of HRQoL comprises how individuals physically and mentally feel, how they manage with others and cope with their everyday lives [5]. Thus, investigations on how HRQoL is related to the way individuals shape their everyday lives represent one crucial element for the derivation of public health recommendations. In line with these assumptions and with recent research perspectives, emphasizing the meaning of an early awareness and pursuit of a healthy lifestyle throughout adulthood, the present study aims to identify lifestyle factors promoting HRQoL from young to older adulthood rather than just focusing on the extension of the life span [6, 7].
HRQoL associations with individual and social factors
Previous research indicates that HRQoL is determined by certain individual and social characteristics. For example, low HRQoL was associated with chronic conditions such as arthrosis or Parkinson’s diseases [8]. Older age was also associated with lower physical HRQoL (as often caused by chronic conditions) [9, 10], while the majority of research points toward an age-related increase in mental HRQoL [11,12,13]. Furthermore, findings suggest that being female is associated with lower physical and mental HRQoL possibly due to a higher educational level as well as a lower prevalence of living alone among men as compared to women [13, 14]. This assumption stems from indications of individuals with low socio-economic status (SES) having lower levels of both physical and mental health, in general [15, 16]. In addition, living alone and the absence of a solid partnership was associated with lower HRQoL levels substantiating the meaning of social resources [17, 18]. Particularly, the perceived level of security and availability of help from persons of trust, neighbors, or society were associated with HRQoL [19, 20] which moreover showed systematic variation in the population such as with differing age, sex, and SES [21].
HRQoL associations with lifestyle factors and executive functioning
Beyond individual and social factors, previous research identified several lifestyle factors as possible resources for maintaining a healthy and satisfied life. To date, evidence on positive effects from physical activity and healthy eating on diverse physical and mental health-related outcomes is accumulating [22,23,24,25,26,27]. Taken together, physical activity is supposed to affect both physical and mental HRQoL by stimulating weight loss, the cardiovascular system, mobility, self-esteem and improving cognitive functioning and positive affect [28, 29]. Again, physical activity and healthy eating scores varied by age and SES, demonstrating how the utilization of sports as well as the quality of diet is largely determined by social and environmental variables [30]. Negative consequences of an insufficient level of physical activity as well as obesity are a loss of mobility, an increased dependency in daily life, and lower social activity, which in turn constitutes the risk of lower HRQoL [18, 20]. In conclusion, the ability to maintain an active and independent lifestyle characterizes one central goal for HRQoL interventions, gaining relevance particularly with advancing age [31, 32].
Another important factor for maintaining an independent and active lifestyle is represented by cognitive abilities. Although evidence is relatively rare, few studies show that physical activity can buffer age-related cognitive decline and that especially a combined training of executive functioning and physical activity can compensate functional losses and HRQoL perceptions [33, 34]. Moreover, insufficient sleep is associated with a variety of adverse health behaviors and a reduced HRQoL and thus represents one central public health concern [35, 36]. In sum, results point toward the interrelation of several lifestyle factors and executive functioning such as short sleep duration and lower cognitive functioning [37] or long sleep duration and inadequate food intake [38].
Rationale and hypotheses
To date, results on effects of lifestyle factors on HRQoL in a representative population sample covering a broad age-range are fragmentary and await further evidence. Thus, the present study aimed to (1) examine interrelations between lifestyle factors and executive functioning with HRQoL in a representative sample from young to old adulthood and while controlling for relevant individual and social factors and (2) determine age-related differences. The overarching aim was to identify factors positively related to HRQoL to derive recommendations for public health actions and the promotion of HRQoL in the everyday life of individuals from varying ages.
Based on the findings reviewed above, it can be assumed that lifestyle factors and executive functioning are supportive for maintaining independence in, and a better quality of, daily life. More precisely, we hypothesized in Hypothesis 1 (H1) that a high level of healthy eating, physical activity, executive functioning, and moderate sleep duration show positive associations with HRQoL across the adult life span, while controlling for relevant individual and social factors. In Hypothesis 2 (H2), we expected certain lifestyle factors and executive functioning becoming particularly important with advancing age for maintaining a healthy and satisfied life, as indicated by enhanced HRQoL levels.
Methods
Sample and procedure
The underlying sample is a subsample from the German Health Interview and Examination Survey for Adults (DEGS1; performed from 2008 to 2011) which participated in the additional Mental Health Module (DEGS1-MH; performed with an average time lag of 6 weeks) containing n = 3667 individuals (52% female) ranging in age from young to old adulthood (18–79 years; M = 52.71, SD = 16.06). The original DEGS1 sample contained a nationally representative sample of n = 8152 randomly chosen individuals from local population registries covering 180 study sample points across Germany (see details in [39, 40]). Participants of this subsample completed both assessment parts (DEGS1 and DEGS1-MH) containing a face-to-face medical as well as a clinical interview, physical and laboratory examinations, and standardized self-report scales of approximately 3 h (DEGS1) plus 1 h (DEGS1-MH) in total at home or in community-owned facilities that were rented for the purpose of the survey. Present analyses include information from the standardized socio-demographic questionnaire (DEGS1), the food frequency questionnaire, the computer-assisted clinical interview (DEGS1), and the neuropsychological test battery (DEGS1-MH), only. Sample statistics for individual, social, and lifestyle factors and executive functioning are displayed in Tables 1 and 2. Informed consent was obtained from all participants. The research was approved by the Medical Ethics Review Committee of the Charité Berlin, Germany and by the Ethics Board of the Technische Universität Dresden, Germany.
Measures
Health-related quality of life
Health-related quality of life was assessed with the German version of the short form health survey SF-36.2 [41]. Psychometric validation of the German version of the SF-36 questionnaire yields comparable results for data reliability and construct validity with several non-German translations and samples [42,43,44]. The questionnaire consists of 36 items from eight multi-item scales subsuming general health concepts which can be summarized to one PCS including physical functioning, role limitations due to physical health problems, bodily pain, general health, and one MCS including vitality, social functioning, role limitations due to emotional problems, mental health (see Table S1, Supplementary material). Raw scores are summarized and transformed into z-standardized values ranging from 0 (min) to 100 (max) for each of the eight subscales as well as for the physical (PCS) and mental (MCS) composite scores, respectively.
Chronic diseases
Participants answered the Mini European Health Module [45] and we used the item “Do you suffer from any long-standing illness or condition?” (no = 0, yes = 1) as an indication of chronic diseases.
Partnership status
Participants were asked to indicate whether they were currently married or in a solid partnership (no = 0, yes = 1). Both answers were combined to one indicator for the current partnership status.
Social support
Perceived social support was assessed via the three-item Oslo social support scale [46, 47] regarding the number of close persons (from 1 = none to 4 = six or more persons), the sense of concern or interest from others (from 1 = none to 5 = a lot concern/interest), and the easiness to get help from neighbors (1 = very difficult to 5 = very easy). Answers were summarized to a total score and thereafter categorized into three categories from low (< 9) to moderate (9–11) and high (> 11) perceived social support.
Socio-economic status
The socio-economic status (SES) is represented by an index score on the basis of the individual dimensions of education, occupation, and income [48]. The SES Index is used as a categorical variable, allowing a categorization of three groups (low, medium, high) to enable comparisons between the bottom and top 20% of the population and a broadly defined middle group which comprises 60% of the population [48].
Healthy eating
Participants completed a self-administered food frequency questionnaire containing consumption frequencies and portion sizes of a total of 53 food groups (e.g., vegetables, cereals, juices) consumed during the last 4 weeks [49]. A healthy eating index was constructed by comparing calculated daily amounts of particular food intakes against age-specific recommendations of the German Nutrition Society [50]. For several food groups, consumption scores in relation to meeting the recommendations were assigned and summarized, resulting in an overall healthy eating index ranging from 0 (min) to 100 (max) [50].
Physical activity
Participants’ regular physical activity during the last 3 months was assessed via the item “How often do you do sports?”. Answers were categorized as never (0), up to 2 h a week (1) and more than 2 h a week (2).
Sleep duration
The self-reported average number of hours slept during the last 4 weeks was used as an indicator for sleep duration. In line with recent sleep literature, we used the sleep duration as a categorical variable indicating rather short (< 7 h), moderate (7–8 h), and long (> 8 h) sleep [51, 52].
Executive functioning
As part of a larger neuropsychological testing battery (mean duration of 21 min), participants’ executive functioning was assessed via four standardized tests including verbal fluency, trail making, digit span backwards, and letter digit substitution as described in Wagner et al. [53]. For the analyses, a composite measure of global executive functioning was created by converting and averaging each of the three test performances into a z-standardized score (adjusted by age and SES), as suggested by the results from a factorial analyses of all cognitive performance data [53].
Statistical analyses
The analyses were carried out in Stata 14 [54] and with a weighting factor which adjusts deviations of the present sample from the German population structure (as at 2010) in terms of age, sex, region, and nationality as well as municipality type and education [40, 55].
First, we performed two sets of path analyses to quantify multiple significant interrelations as well as direct and indirect paths from individual (age group, sex, chronic diseases), social (partnership, social support, SES), and lifestyle factors (healthy eating, physical activity, sleep duration) and executive functioning on MCS and PCS, respectively, with the help of structural equation modeling (SEM) based on maximum-likelihood (ML) estimation and with the weighted survey data estimation function (linearized SE).
Next, we conducted two multiple linear regression analyses for survey data on PCS and MCS, respectively, in order to investigate potential age-related differences in the significance of the lifestyle factors included in path analyses. Besides the individual, social, and lifestyle factors, and executive functioning, we therefore included age group × lifestyle factors and age group × executive functioning interactions as predictors in the same models.Footnote 1
Results
Interrelations: results from path analyses
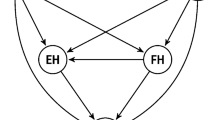
Results from path analyses showed several significant direct paths between individual, social, and lifestyle factors and executive functioning. Individuals with chronic diseases and at older age showed higher healthy eating scores (chronic disease: β = .06, p < .05; age group: β = .31, p < .01), lower physical activity (chronic disease: β = − .08, p < .01; age group: β = − .14, p < .01), and lower executive functioning (chronic disease: β = − .10, p < .05; age group: β = .53, p < .01), while women showed higher healthy eating scores (β = .21, p < .01) and sleep duration than men (β = .07, p < .05; see Figs. 1, 2 and Table S2 from the Supplementary material for more detailed information). Higher social support was related to higher physical activity (β = .09, p < .01) and executive functioning (β = .06, p < .01) and a higher SES was related to higher healthy eating scores (β = 11, p < .01), physical activity (β = .18, p < .01) , and executive functioning (β = .26, p < .01). Being in a solid partnership was neither related to lifestyle factors nor to executive functioning. Results also revealed various significant direct paths between lifestyle factors and executive functioning: Higher healthy eating scores were associated with higher physical activity (β = .14, p < .01), sleep duration (β = .06, p < .01); higher physical activity was associated with higher healthy eating scores (β = .11, p < .01) and executive functioning (β= .09, p < .01); higher sleep duration was related to higher healthy eating scores (β= .05, p < .05) ; and higher executive functioning was related to higher healthy eating scores (β= .05, p < .01) and physical activity (β= .06, p < .01) (see Figs. 1, 2, Table S2 in Supplementary information).

Significant direct paths from individual (age group, sex, chronic diseases), social (partnership status, social support, SES), and lifestyle factors (healthy eating, physical activity, sleep duration) and executive functioning on the PCS of HRQoL are marked with solid lines. Indirect effects on PCS are marked with dashed lines. Model fit statistics for survey data: coefficient of determination (CD) = .63, standardized root mean-squared residual (SRMR) = .001

Significant direct paths from individual (age group, sex, chronic diseases), social (partnership status, social support, SES), and lifestyle factors (healthy eating, physical activity, sleep duration) and executive functioning on the MCS of HRQoL are marked with solid lines. Indirect effects on PCS are marked with dashed lines. Model fit statistics for survey data: coefficient of determination (CD) = .64, standardized root mean-squared residual (SRMR) = .003
Moreover, a series of factors was related to HRQoL. PCS was lower in individuals with chronic diseases (β = − .31, p < .01), at older age (β = − .21, p < .01), female sex (β = − .06, p < .01) and higher in individuals with high social support (β = .05, p < .05), SES (β = .11, p < .01), physical activity (β= .10, p < .01), sleep duration (β = .05, p < .05), and executive functioning (β = .11, p < .01; Fig. 1). Besides, healthy eating showed an indirect path on PCS (β = .08, p < .01) mediated by physical activity. Chronic diseases (β = − .02, p < .01), age (β = − .03, p < .01) , and SES (β = .06, p < .01) also showed indirect paths through physical activity on PCS. MCS was lower among individuals with chronic diseases (β = − .11, p < .01), female sex (β = − .16, p < .01) and higher among individuals at older age (β = .21, p < .01), with a solid partnership (β = .10, p < .01), high social support (β = .17, p < .01), high healthy eating scores (β = .04, p < .05), long sleep duration (β = .08, p < .01) , and high executive functioning (β = .07, p < .05; Fig. 2). Healthy eating also showed an indirect path on MCS (β = .06, p < .01), mediated by executive functioning. In addition, MCS was indirectly related to SES (β = .09, p < .01),, and social support (β = .04, p < .01), through executive functioning.
Age-related differences: results from regression analyses
In general, results from multiple regression analyses replicate findings from path analyses: PCS but not MCS is lower with older age; men as well as individuals without chronic conditions or with medium or high social support showed higher PCS and MCS, on average; being in a solid partnership was positively related to MCS, while low SES was negatively related to PCS, only (Table 3). Several lifestyle factors as well as executive functioning showed positive relations with both PCS and MCS: physical activity, medium sleep duration, and higher levels of executive functioning were related to higher PCS; healthy eating, medium sleep duration as well as higher executive functioning were related to higher MCS. The relation between healthy eating and PCS as well as between sleep duration and MCS was marginally significant, only (Table 3). Results revealed a significant interaction of age group × physical activity on PCS, indicating a higher increase in older as compared to younger adults with regular physical activity (Fig. 3a; Table 3). Moreover, age group × physical activity as well as age group × healthy eating interactions were significantly related to MCS. While MCS increased with more than 2 h physical activity per week in younger and middle-aged adults, it remained constantly high for older adults (Fig. 3b; Table 3). On the contrary, higher healthy eating scores were related to higher MCS in older adults, only (Fig. 3c).Footnote 2

Interaction effects between age group (18–39 years, 40–59 years, 60–79 years) and a physical activity (none, less than 2 h per week, more than 2 h per week) on the PCS of HRQoL, b physical activity on the MCS of HRQoL, c healthy eating (low = M − 1 SD, medium = M, high = M + 1 SD) on the MCS of HRQoL
Discussion
The present study provides new insights into interrelations and the age relevance of several factors that have been identified as potentially supportive for HRQoL across adulthood. In addition to social and individual characteristics such as chronic conditions or age, we identified positive associations with lifestyle factors and executive functioning that can be addressed by public health measures. Taken together, results suggest that certain factors are essential for the promotion of both physical and mental HRQoL (e.g., moderate sleep duration, executive functioning) during adulthood in general, while others seem to be of particular relevance for physical or mental HRQoL and gain importance with advancing age (e.g., healthy eating, physical activity).
Results underline previous findings on varying HRQoL levels among individuals with differing individual and social factors such as age or SES [12, 16, 55]. For example, chronic diseases and high age was indicative of low physical activity and physical HRQoL. Possible explanations for an age-related decrease in physical HRQoL are a higher risk of chronic diseases and related consequences such as less physical ability. At the same time, older age was associated with high healthy eating scores and mental HRQoL. Thus, apart from the negative effects that older age and chronic conditions might have on physical HRQoL, mental HRQoL is not necessarily affected in the same way and the negative effects might even be initiative for promoting lifestyle factors that can be modified such as healthy eating. This interpretation corresponds with other findings on relatively high coping and emotion regulation abilities in older adults, allowing adjustments to changes of physical health or other adverse life events [11, 33, 57].
In the past, SES differences have been explained by a higher exposure to stress and anxiety, a lack of proper medical services, and also by certain unhealthy lifestyle behaviors such as the consumption of unhealthy food or less physical activity [17, 58]. In line with these explanations, the present results indicate besides lower healthy eating scores, physical activity, and executive functioning also lower physical HRQoL with lower SES. Noticeably, the strength of association between SES and mental HRQoL attenuated when entering lifestyle factors and executive functioning into the same model suggesting a potential to buffer negative effects from SES by, for example, promoting executive functioning (as suggested by the found indirect effects). Furthermore, the relatively low proportion of explained variance in mental HRQoL indicates how other so far unconsidered factors can additionally contribute to the enhancement of mental HRQoL and compensate certain individual and social risk factors. Additionally, present findings underpin previous assumptions on salutary effects from social support on well-being and health. One possible explanation is related to (interpersonal) coping abilities helping to buffer adverse life circumstances [21, 59]. A lack of perceived social support on the contrary seems to be related to lower mental HRQoL as well as lower cognitive functioning, as already discussed before [59, 60].
As expected in H1, lifestyle factors and executive functioning showed positive relations with HRQoL in addition to individual and social factors. Individuals with above-average executive functioning, healthy eating, regularly conducting sport more than 2 h per week, and average sleep duration of 7–8 h showed higher physical and mental HRQoL as compared to individuals not fulfilling the aforementioned criteria. Present findings also underpin the central role of physical activity, being related to almost all of the included factors as well as to mental and physical HRQoL. Thus, findings are in line with the success rates of physical activity interventions on different health-related outcomes [46] and with previous assumptions on the benefits of physical exercise mediating or even surpassing modifications in eating behavior [26]. Correspondingly, in the present study, the relation between healthy eating and physical HRQoL was only marginally significant but showed a significant indirect relation through physical activity. Hence, it is to be assumed that individuals who eat healthy also do regularly sports and thereby promote several healthy lifestyles at the same time.
Similar to the high relevance of physical activity especially on physical HRQoL, executive functioning can be interpreted as a particularly relevant resource contributing to the enhancement of mental HRQoL. The present findings are in favor of interpretations of executive functioning as one central aspect for mental HRQoL and as a prerequisite for the ability to cope with everyday life demands [47, 61]. Social support as well as healthy eating showed indirect relations through executive functioning on mental HRQoL, underpinning previous results on interdependencies between executive functioning and relevant coping resources for mental health [62, 63]. In conclusion, results substantiate current suggestions of multimodal training approaches for the successful and comprehensive promotion of lifelong physical and mental health [47, 64].
In line with H2, present findings indicate that certain factors gain importance especially with advancing age. Physical HRQoL increased stronger with higher physical activity and mental HRQoL increased stronger with higher healthy eating scores among older individuals. These findings correspond with previous research suggesting a high risk of (a) insufficient physical activity for chronic conditions and (b) poor diet for reduced immunity, muscle strength, or depression in turn also leading to frailty and functional limitations, especially in older ages [27, 63, 65]. Results also suggest that physical activity seems to be less important to mental HRQoL in older as compared to younger or middle-aged adults. It is to be assumed that older adults accept having less physical capacity and thus focus on other modifiable opportunities [57]. In conclusion, the active pursuit of a healthy lifestyle might become particularly apparent in eating behaviors among older adults, but awaits further investigations. This refers specifically to the healthy eating index as a general summary score of an individual’s compliance with meeting several recommendations. Some of these recommendations may be more relevant than others in relation to HRQoL which does not become apparent in the present study. Further differentiations of healthy food recommendation specificity and quality with regard to age-related physiological fitness might add insights to the observed conflicting associations with mental and physical HRQoL in older age [46].
Limitations
The cross-sectional design of the present study represents a limitation as it does not allow drawing conclusions on causality or within-person change. Future research should investigate changes in HRQoL associated with lifestyle by following individuals over time as they age.
Conclusions
Present finding underpins the need to improve lifestyle conditions, behavior, and social supply offers and thereby reduce the risk of health problems for individuals with low social support and low SES, also because possibilities on how to reach such high-risk groups through lifestyle interventions are not fully explored, yet [15]. However, another central finding of the present research lies in the interrelation and potential of other factors to promote HRQoL beyond environment and disposition. As a consequence, health intervention might want to foster behavioral multicomponent approaches addressing simultaneously several potentially supportive factors for the promotion and maintenance of an independent and satisfied life, such as physical activity and cognitive functioning. Few preventive lifestyle recommendations have already been formulated for older individuals [22] but should be extended to younger ages for an early habitualization of salutary behavior and the consolidation of a healthy lifestyle. From a perspective of health education, an early awareness of potentially buffering effects might be beneficial to actively implement supportive factors in the daily lives of high-risk groups such as persons with chronic conditions.
Notes
We tested multicollinearity by taking the correlation between indicators and the variance inflation factor (VIF) of all indicators of the regression model into account. All values were below the conventional limits of r < .70 and VIF < 10 (e.g., [56]).
We furthermore tested for HRQoL differences between the three physical activity (none, < 2 h, > 2 h) and healthy eating categories (low, medium, high) for each age group, separately. PCS scores differed significantly regarding physical activity for young (none vs. < 2 h B = − 0.14, SE = 0.75, p = .85; none vs. > 2 h B = 1.67, SE = 0.70, p = .02), middle-aged (none vs. < 2 h B = 0.41, SE = 0.73, p = .58; none vs. > 2 h B = 2.71, SE = 0.72, p < .01) as well as older adults (none vs. < 2 h B = 2.85, SE = 0.83, p < .01; none vs. > 2 h B = 5.21, SE = 0.94, p < .01), while MCS scores did not differ significantly regarding physical activity for young (none vs. < 2 h B = 1.47, SE = 1.24, p = .24; none vs. > 2 h B = 1.96, SE = 1.30, p = .14), middle-aged (none vs. < 2 h B = 0.31, SE = 0.82, p = .71; none vs. > 2 h B = 1.49, SE = 0.85, p = .08) , and older adults (none vs. < 2 h B = − 0.36, SE = 0.85, p = .67; none vs. > 2 h B = − 0.08, SE = 0.98, p = .94). MCS scores differed significantly regarding healthy eating for older (low vs. medium B = 4.04, SE = 1.86, p = .03; low vs. high B = 6.43, SE = 1.96, p < .01) but not for young (low vs. medium B = − 0.49, SE = 1.14, p = .67; low vs. high B = − 2.61, SE = 2.21, p = .24) or middle-aged adults (low vs. medium B = − 0.46, SE = 1.34, p = .73; low vs. high B = − 0.73, SE = 1.88, p = .64)
References
Fagerström, C., & Borglin, G. (2013). Mobility, functional ability and health-related quality of life among people of 60 years or older. Aging Clinical and Experimental Research, 22(5–6), 387–394. https://doi.org/10.1007/bf03324941.
Mulasso, A., Roppolo, M., & Rabaglietti, E. (2014). The role of individual characteristics and physical frailty on health related quality of life (HRQOL): A cross sectional study of Italian community-dwelling older adults. Archives of Gerontology and Geriatrics, 59(3), 542–548. https://doi.org/10.1016/j.archger.2014.08.012.
Saarni, S. I., Suvisaari, J., Sintonen, H., Pirkola, S., Koskinen, S., Aromaa, A., et al. (2007). Impact of psychiatric disorders on health-related quality of life: General population survey. British Journal of Psychiatry, 190(4), 326–332. https://doi.org/10.1192/bjp.bp.106.025106.
Hennessy, C. H., Moriarty, D. G., Zack, M. M., Scherr, P. A., & Brackbill, R. (1994). Measuring health-related quality of life for public health surveillance. Public Health Reports, 109(5), 665–672.
WHO. (1995). The World Health Organization quality of life assessment (WHOQOL): Position paper from the World Health Organization. Social Science & Medicine, 41(10), 1403–1409. https://doi.org/10.1016/0277-9536(95)00112-k.
US Department of Health and Human Services. (2010). Healthy people 2020. Washington, DC: Office of the Assistant Secretary for Health. Retrieved from http://www.healthypeople.gov/2020/about/DOHAbout.aspx.
Parekh, A. K., Goodman, R. A., Gordon, C., Koh, H. K., & HHS Interagency Workgroup on Multiple Chronic Conditions (2011). Managing multiple chronic conditions: A strategic framework for improving health outcomes and quality of life. Public Health Reports 126(4), 460–471, https://doi.org/10.1177/003335491112600403.
Saarni, S. I., Härkänen, T., Sintonen, H., Suvisaari, J., Koskinen, S., Aromaa, A., et al. (2006). The impact of 29 chronic conditions on health-related quality of life: A general population survey in Finland using 15D and EQ-5D. Quality of Life Research, 15(8), 1403–1414. https://doi.org/10.1007/s11136-006-0020-1.
Lubetkin, E. I., Jia, H., Franks, P., & Gold, M. R. (2005). Relationship among sociodemographic factors, clinical conditions, and health-related quality of life: Examining the EQ-5D in the US general population. Quality of Life Research, 14(10), 2187–2196. https://doi.org/10.1007/s11136-005-8028-5.
Sun, S., Chen, J., Johannesson, M., Kind, P., Xu, L., Zhang, Y., et al. (2011). Population health status in China: EQ-5D results, by age, sex and socio-economic status, from the National Health Services Survey 2008. Quality of Life Research, 20(3), 309–320. https://doi.org/10.1007/s11136-010-9762-x.
Gana, K., Bailly, N., Saada, Y., Joulain, M., & Alaphilippe, D. (2013). Does life satisfaction change in old age: Results from an 8-year longitudinal study. Journal of Gerontology B Psychological Science and Social Science, 68(4), 540–552. https://doi.org/10.1093/geronb/gbs093.
Gunzelmann, T., Albani, C., Beutel, M., & Brahler, E. (2006). Subjective health of older people in view of the SF-36: Values from a large community-based sample. Zeitschrift Gerontologie Geriatrie, 39(2), 109–119. https://doi.org/10.1007/s00391-006-0352-z.
Costa, P. T. Jr., McCrae, R. R., & Zonderman, A. B. (1987). Environmental and dispositional influences on well-being: Longitudinal follow-up of an American national sample. British Journal of Psychology, 78(3), 299–306. https://doi.org/10.1111/j.2044-8295.1987.tb02248.x.
Cherepanov, D., Palta, M., Fryback, D. G., & Robert, S. A. (2010). Gender differences in health-related quality-of-life are partly explained by sociodemographic and socioeconomic variation between adult men and women in the US: Evidence from four US nationally representative data sets. Quality of Life Research, 19(8), 1115–1124. https://doi.org/10.1007/s11136-010-9673-x.
Bukman, A. J., Teuscher, D., Feskens, E. J., van Baak, M. A., Meershoek, A., & Renes, R. J. (2014). Perceptions on healthy eating, physical activity and lifestyle advice: Opportunities for adapting lifestyle interventions to individuals with low socioeconomic status. BMC Public Health. https://doi.org/10.1186/1471-2458-14-1036.
Stringhini, S., Sabia, S., Shipley, M., Brunner, E., Nabi, H., Kivimaki, M., et al. (2010). Association of socioeconomic position with health behaviors and mortality. JAMA, 303(12), 1159–1166. https://doi.org/10.1001/jama.2010.297.
Lallukka, T., Laaksonen, M., Rahkonen, O., Roos, E., & Lahelma, E. (2007). Multiple socio-economic circumstances and healthy food habits. European Journal of Clinical Nutrition, 61(6), 701–710. https://doi.org/10.1038/sj.ejcn.1602583.
Pinquart, M., & Sörensen, S. (2001). How effective are psychotherapeutic and other psychosocial interventions with older adults? A meta-analysis. Journal of Mental Health and Aging, 7(2), 207–243.
Enkvist, A., Ekstrom, H., & Elmstahl, S. (2012). Associations between functional ability and life satisfaction in the oldest old: Results from the longitudinal population study good aging in Skane. Clinical Interventions in Aging, 7, 313–320. https://doi.org/10.2147/CIA.S33610.
Fone, D., Dunstan, F., Lloyd, K., Williams, G., Watkins, J., & Palmer, S. (2007). Does social cohesion modify the association between area income deprivation and mental health? A multilevel analysis. International Journal of Epidemiology, 36(2), 338–345. https://doi.org/10.1093/ije/dym004.
Kawachi, I., & Berkman, L. F. (2001). Social ties and mental health. Journal of Urban Health, 78(3), 458–467. https://doi.org/10.1093/jurban/78.3.458.
Kahana, E., Kahana, B., & Lee, J. E. (2014). Proactive approaches to successful aging: One clear path through the forest. Gerontology, 60(5), 466–474. https://doi.org/10.1159/000360222.
Bize, R., Johnson, J. A., & Plotnikoff, R. C. (2007). Physical activity level and health-related quality of life in the general adult population: A systematic review. Preventive Medicine, 45(6), 401–415. https://doi.org/10.1016/j.ypmed.2007.07.017.
Fontaine, K. R., Barofsky, I., Andersen, R. E., Bartlett, S. J., Wiersema, L., Cheskin, L. J., et al. (1999). Impact of weight loss on health-related quality of life. Quality of Life Research, 8(3), 275–277. https://doi.org/10.1023/A:1008835602894.
Colcombe, S., & Kramer, A. F. (2003). Fitness effects on the cognitive function of older adults: A meta-analytic study. Psychology Science, 14(2), 125–130. https://doi.org/10.1111/1467-9280.t01-1-01430.
Penedo, F. J., & Dahn, J. R. (2005). Exercise and well-being: A review of mental and physical health benefits associated with physical activity. Current Opinion in Psychiatry, 18(2), 189–193.
Drewnowski, A., & Evans, W. J. (2001). Nutrition, physical activity, and quality of life in older adults: Summary. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 56(Supplement 2), 89–94. https://doi.org/10.1093/gerona/56.suppl_2.89.
Smith, P. J., Blumenthal, J. A., Hoffman, B. M., Cooper, H., Strauman, T. A., Welsh-Bohmer, K., et al. (2010). Aerobic exercise and neurocognitive performance: A meta-analytic review of randomized controlled trials. Psychosomatic Medicine, 72(3), 239–252. https://doi.org/10.1097/PSY.0b013e3181d14633.
Josefsson, T., Lindwall, M., & Archer, T. (2014). Physical exercise intervention in depressive disorders: Meta-analysis and systematic review. Scandinavian Journal of Medicine Science in Sports, 24(2), 259–272. https://doi.org/10.1111/sms.12050.
Kennedy, E., Ohls, J., Carlson, S., & Fleming, K. (1995). The healthy eating index: Design and applications. Journal of the Academy of Nutrition and Dietetics, 95(10), 1103–1108. https://doi.org/10.1016/S0002-8223(95)00300-2.
Bowling, A., & Grundy, E. (1997). Activities of daily living: Changes in functional ability in three samples of elderly and very elderly people. Age and Ageing, 26(2), 107–114. https://doi.org/10.1093/ageing/26.2.107.
Borg, C., Fagerstrom, C., Balducci, C., Burholt, V., Ferring, D., Weber, G., et al. (2008). Life satisfaction in 6 European countries: The relationship to health, self-esteem, and social and financial resources among people (aged 65–89) with reduced functional capacity. Geriatric Nursing, 29(1), 48–57. https://doi.org/10.1016/j.gerinurse.2007.05.002.
Jonker, A. A., Comijs, H. C., Knipscheer, K. C., & Deeg, D. J. (2009). The role of coping resources on change in well-being during persistent health decline. Journal of Aging Health, 21(8), 1063–1082. https://doi.org/10.1177/0898264309344682.
Weuve, J., Kang, J. H., Manson, J. E., Breteler, M. M., Ware, J. H., & Grodstein, F. (2004). Physical activity, including walking, and cognitive function in older women. JAMA, 292(12), 1454–1461. https://doi.org/10.1001/jama.292.12.1454.
Ford, D. E., & Kamerow, D. B. (1989). Epidemiologic study of sleep disturbances and psychiatric disorders. An opportunity for prevention? JAMA, 262(11), 1479–1484.
Alhola, P., & Polo-Kantola, P. (2007). Sleep deprivation: Impact on cognitive performance. Neuropsychiatric Disease Treatment, 3(5), 553–567.
Lo, J. C., Loh, K. K., Zheng, H., Sim, S. K., & Chee, M. W. (2014). Sleep duration and age-related changes in brain structure and cognitive performance. Sleep, 37(7), 1171–1178. https://doi.org/10.5665/sleep.3832.
Kim, S., DeRoo, L. A., & Sandler, D. P. (2011). Eating patterns and nutritional characteristics associated with sleep duration. Public Health Nutrition, 14(5), 889–895. https://doi.org/10.1017/S136898001000296X.
Jacobi, F., Mack, S., Gerschler, A., Scholl, L., Hofler, M., Siegert, J., et al. (2013). The design and methods of the mental health module in the German Health Interview and Examination Survey for Adults (DEGS1-MH). International Journal of Methods in Psychiatric Research, 22(2), 83–99. https://doi.org/10.1002/mpr.1387.
Scheidt-Nave, C., Kamtsiuris, P., Gosswald, A., Holling, H., Lange, M., Busch, M. A., et al. (2012). German health interview and examination survey for adults (DEGS)—design, objectives and implementation of the first data collection wave. BMC Public Health, 12, 730. https://doi.org/10.1186/1471-2458-12-730.
Ware, J. E., Kosinski, M., Bjorner, J. B., Turner-Bowker, D. M., Gandek, B., & Maruish, M. E. (2008). User’s manual for the SF-36v2 health survey. Lincoln: Quality Metric Incorporated.
Bullinger, M. (1995). German translation and psychometric testing of the SF-36 Health Survey: Preliminary results from the IQOLA project. Social Science & Medicine, 41(10), 1359–1366. https://doi.org/10.1016/0277-9536(95)00115-N.
Ware, J. E., & Gandek, B. (1998). Overview of the SF-36 health survey and the International Quality of Life Assessment (IQOLA) Project. Journal of Clinical Epidemiology, 51(11), 903–912. https://doi.org/10.1016/S0895-4356(98)00081-X.
Ellert, U., & Kurth, B. M. (2004). Methodological views on the SF-36 summary scores based on the adult German population. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz, 47(11), 1027–1032. https://doi.org/10.1007/s00103-004-0933-1.
Cox, B., Oyen, H. V., Cambois, E., Jagger, C., Roy, S. l., Robine, J.-M., et al. (2009). The reliability of the Minimum European Health Module. International Journal of Public Health, 54(2), 55–60. https://doi.org/10.1007/s00038-009-7104-y.
Netz, Y., Wu, M. J., Becker, B. J., & Tenenbaum, G. (2005). Physical activity and psychological well-being in advanced age: A meta-analysis of intervention studies. Psychology and Aging, 20(2), 272–284. https://doi.org/10.1037/0882-7974.20.2.272.
Forte, R., Boreham, C. A., Leite, J. C., De Vito, G., Brennan, L., Gibney, E. R., et al. (2013). Enhancing cognitive functioning in the elderly: Multicomponent vs resistance training. Clinical Interventions in Aging, 8, 19–27. https://doi.org/10.2147/CIA.S36514.
Lampert, T., Kroll, L., Muters, S., & Stolzenberg, H. (2013). Measurement of socioeconomic status in the German Health Interview and Examination Survey for Adults (DEGS1). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz, 56(5–6), 631–636. https://doi.org/10.1007/s00103-012-1663-4.
Mensink, G. B., Truthmann, J., Rabenberg, M., Heidemann, C., Haftenberger, M., Schienkiewitz, A., et al. (2013). Fruit and vegetable intake in Germany: Results of the German Health Interview and Examination Survey for Adults (DEGS1). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz, 56(5–6), 779–785. https://doi.org/10.1007/s00103-012-1651-8.
Kuhn, D. A. (2017). Entwicklung eines Index zur Bewertung der Ernährungsqualität in der Studie zur Gesundheit Erwachsener in Deutschland (DEGS1) [The development of a healthy eating index to assess the quality of nutrition in the German Health Examination and Interview for Adults (DEGS1)] (master’s thesis). Berlin and Potsdam, Germany: Robert Koch Institute and German Institute of Human Nutrition.
Hirshkowitz, M., Whiton, K., Albert, S. M., Alessi, C., Bruni, O., DonCarlos, L., et al. (2015). National Sleep Foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health, 1(1), 40–43. https://doi.org/10.1016/j.sleh.2014.12.010.
Chen, X., Wang, R., Zee, P., Lutsey, P. L., Javaheri, S., Alcántara, C., et al. (2015). Racial/ethnic differences in sleep disturbances: The multi-ethnic study of atherosclerosis (MESA). Sleep, 38(6), 877–888. https://doi.org/10.5665/sleep.4732.
Wagner, M., Wolfsgruber, S., Gaertner, B., Kleineidam, L., Buttery, A. K., Jacobi, F., et al. (2017). Cognitive functioning in the general population: Factor structure and association with mental disorders-the neuropsychological test battery of the mental health module of the German Health Interview and Examination Survey for Adults (DEGS1-MH). International Journal of Methods Psychiatric in Research, 27(1), e1594. https://doi.org/10.1002/mpr.1594.
StataCorp LP (2015). STATA 14 [Computer software]. College Station: TX: StataCorp LP.
Ladwig, K. H., Marten-Mittag, B., Formanek, B., & Dammann, G. (2000). Gender differences of symptom reporting and medical health care utilization in the German population. European Journal of Epidemiology, 16(6), 511–518. https://doi.org/10.1023/A:1007629920752.
Dormann, C. F., Elith, J., Bacher, S., Buchmann, C., Carl, G., Carré, G., et al. (2013). Collinearity: A review of methods to deal with it and a simulation study evaluating their performance. Ecography, 36(1), 27–46. https://doi.org/10.1111/j.1600-0587.2012.07348.x. doi.
Kessler, E.-M., & Staudinger, U. M. (2010). Emotional resilience and beyond: A synthesis of findings from lifespan psychology and psychopathology. In P. S. Fry & C. L. M. Keyes (Eds.), New frontiers in resilient aging: Life-strengths and well-being in late life (pp. 258–282). Cambridge: Cambridge University Press.
Gidlow, C., Johnston, L. H., Crone, D., Ellis, N., & James, D. (2006). A systematic review of the relationship between socio-economic position and physical activity. Health Education Journal, 65(4), 338–367. https://doi.org/10.1177/0017896906069378.
Oxman, T. E., Berkman, L. F., Kasl, S., Freeman, D. H. Jr., & Barrett, J. (1992). Social support and depressive symptoms in the elderly. American Journal of Epidemiology, 135(4), 356–368. https://doi.org/10.1093/oxfordjournals.aje.a116297.
Bassuk, S. S., Glass, T. A., & Berkman, L. F. (1999). Social disengagement and incident cognitive decline in community-dwelling elderly persons. Annals of Internal Medicine, 131(3), 165–173. https://doi.org/10.7326/0003-4819-131-3-199908030-00002.
Wolinsky, F. D., Unverzagt, F. W., Smith, D. M., Jones, R., Wright, E., & Tennstedt, S. L. (2006). The effects of the ACTIVE cognitive training trial on clinically relevant declines in health-related quality of life. Journal of Gerontology B Psychological Science and Social Science, 61(5), 281–287. https://doi.org/10.1093/geronb/61.5.S281.
Singh, B., Parsaik, A. K., Mielke, M. M., Erwin, P. J., Knopman, D. S., Petersen, R. C., et al. (2014). Association of mediterranean diet with mild cognitive impairment and Alzheimer’s disease: A systematic review and meta-analysis. Journal of Alzheimer’s disease: JAD, 39(2), 271–282. https://doi.org/10.3233/JAD-130830.
Theodora, P., Psaltopoulou, T., Sergentanis, T. N., Panagiotakos, D. B., Sergentanis, I. N., Kosti, R., & Scarmeas, N. (2013). Mediterranean diet, stroke, cognitive impairment, and depression: A meta-analysis. Annals of Neurology, 74(4), 580–591. https://doi.org/10.1002/ana.23944.
Bamidis, P. D., Vivas, A. B., Styliadis, C., Frantzidis, C., Klados, M., Schlee, W., et al. (2014). A review of physical and cognitive interventions in aging. Neuroscience Biobehavioral Reviews, 44, 206–220. https://doi.org/10.1016/j.neubiorev.2014.03.019.
Payette, H., & Shatenstein, B. (2005). Determinants of healthy eating in community-dwelling elderly people. Canadian Journal of Public Health, 96, 27–31.
Acknowledgements
We are particularly grateful to all study participants and wish to acknowledge the assistance given by all collaborators in providing vigorous support and premises in the 180 study locations. Our grateful thanks are also extended to our colleagues from the Robert Koch Institute as well as from the Technische Universität Dresden for their excellent collaboration, high engagement, and valuable contribution to this project.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The present research was approved by the Medical Ethics Review Committee of the Charité Berlin and by the Ethics Board of the Technische Universität Dresden, Germany. Informed consent was obtained from all individual participants included in this research. The present research (DEGS1) is primary funded by the German Ministry of Health (BMG) and additionally by the German Association of Psychotherapy and Psychiatry (DGPPN) for implementing the module on mental health (DEGS1-MH).
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Cohrdes, C., Mensink, G.B.M. & Hölling, H. How you live is how you feel? Positive associations between different lifestyle factors, cognitive functioning, and health-related quality of life across adulthood. Qual Life Res 27, 3281–3292 (2018). https://doi.org/10.1007/s11136-018-1971-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-018-1971-8