
Abstract
Purpose
To quantify the relationship between the change in exercise dose and health-related quality of life (HRQoL) in a cohort of patients participating in a community-based phase-3 cardiac rehabilitation (CR) program.
Methods
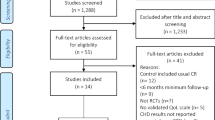
A retrospective, pre-experimental (no control group) design of 58 participants that completed a phase-3, 12-week exercise-based CR program was used to test the current hypothesis. Self-reported HRQoL (36-Item Short Form Health Survey Version 2, SF-36v2) was assessed prior and after completing the CR program. The change in exercise dose was estimated from the assigned training load in weeks 1 and 12 of the CR program. A series of regression models were fitted to ascertain the relationship between the change in exercise dose and changes in the SF-36v2.
Results
There was a strong quadratic trend between the change in exercise dose and the mean change in SF-36 Mental and Physical Health Summary Scores. Analysis of covariance showed that the mean changes in the SF-36 Summary Scores statistically fluctuate across quartiles of exercise dose. The data show that there is a threshold amount of increase in exercise (Q2; 350–510 kcal week− 1) needed to HRQoL and that greater amounts of exercise dose (Q3; 511–687 and Q4 ≥ 688 kcal week− 1) did not improve HRQoL further.
Conclusions
The current findings suggest that physical and mental health-related quality of life are improved with a phase-3 CR program. The dose–response relationship observed indicates that a threshold exercise dose is required to improve HRQoL, and that larger doses of exercise do not confer further improvements in HRQoL.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cardiovascular disease (CVD) is the leading cause of mortality among adults in developed countries. In 2013, an estimated 17 million adult deaths resulted from CVD and it is predicted that CVD will contribute to over 23 million deaths annually by 2030. In the United States alone, more than 85 million adults (1 in 3) have one or more forms of CVD. Each year approximately 660,000 American adults will experience their first ischemic heart disease-related hospitalization or death, while over 300,000 adults will suffer a recurrent hospitalization or death, highlighting the progressive and chronic nature of CVD [1, 2].
It is widely believed that the risk of developing CVD is reduced in those who do not smoke, regularly engage in physical activity and follow healthy dietary practices. For those with established CVD, management is centred on the optimization of pharmacological treatment and modification of lifestyle behaviours. Cardiac rehabilitation (CR) is recognized as an effective approach for tertiary prevention and management of CVD [3]. CR programs begin prior to hospital discharge (phase-1) and assist patients with the transition toward greater self-management during CR phases-2, -3 and -4. Phases-3 and -4 CR are usually delivered via outpatient or community-based programs that are multidimensional in their approach in that they often include supervised exercise training and behavioural change counselling sessions aimed at reducing CVD risk and improving overall functional capacity and health-related quality of life (HRQoL) [4].
The exercise training received during CR is known to reduce systolic blood pressure and systemic inflammation while improving endothelial dysfunction and aerobic exercise capacity [5]. The amount of improvement in maximal exercise capacity [6] and more conventional CVD risk factors such as blood lipids and glucose [2] is related to the exercise dose received (i.e. the product of frequency, duration and intensity) in that greater improvement is gained with larger doses of exercise. In addition to improvements in physiologic health, CR also significantly enhances the psychological health of those completing CR [7]. Surprisingly, despite a large number of reports indicating the positive effect of regular physical activity and/or exercise on HRQoL in those with CVD [8, 9], the relationship between the exercise dose performed and changes in the HRQoL has rarely been examined in CVD patients attending CR.
Evangelista et al. [10] reported a positive relationship between exercise dose and changes in the HRQoL in patients with advanced heart failure that completed a 6-month home-based CR program. While these findings are encouraging, we are unaware of any studies that have directly examined a dose–response relationship between the amount of exercise performed and changes in HRQoL within a standardized 12-week exercise-based phase-3 CR program. Establishing a dose–response relationship between exercise amount and changes in HRQoL would provide important information to health-service providers responsible for developing and implementing community-based outpatient CR programs [9, 11].
Accordingly, the primary aim of this study was to quantify the relationship between the change in exercise dose and HRQoL in a cohort of CVD patients participating in a community-based phase-3 CR program. We hypothesize that there is a positive dose–response relationship between changes in exercise dose over 12 weeks and the magnitude of change in HRQoL.
Methods
Study design, setting and participants
This current study was a pre-experimental (no control group) research design involving a convenience sample of participants enrolled in an outpatient CR program. All participants were diagnosed with CVD including but not limited to coronary artery bypass graft (CABG) surgery, percutaneous transluminal coronary angioplasty or another transcatheter procedure, myocardial infarction or valve surgery. Participants were excluded if they had a recent documented change in resting ECG, uncontrolled resting hypertension (systolic BP > 180 mmHg and/or diastolic BP > 110 mmHg) or had any orthopaedic limitations that would significantly limit exercise participation. All participants provided informed consent and all research protocols were approved by the Human Ethics Committee of the University of Auckland.
Phase-3 cardiac rehabilitation (CR) program
All participants completed 12 weeks of phase-3 CR exercise programming in a community-based setting. Standard anthropometric (i.e. height, total body mass and waist circumference) and cardiovascular indices (i.e. resting heart rate and blood pressure) were collected according to procedures established by the Canadian Society for Exercise Physiology [12] prior to beginning the exercise programme.
The CR program was developed according to evidence-based guidelines, which have been detailed elsewhere [13]. Participants were encouraged to perform 3 × 60 min exercise sessions weekly. The exercise program was supervised and individualized to match participant ability by an experienced American College of Sports Medicine or equivalent registered clinical exercise physiologists. For each session, the target exercise intensity was an effort that would elicit a rating of perceived exertion (RPE) score of 11–13 on a 6–20 scale. The exercise prescription was designed to incorporate the patient’s preference for mode of exercise, but usually involved a mixture of walking, cycling and rowing. Participant safety and exercise effort were monitored during each session via pulse oximetry, blood pressure and RPE.
Quality of life (HRQoL)
The 36-Item Short Form Health Survey version 2 (SF-36v2) [14], which covers the domains of physical function, bodily pain, general health, vitality, social functioning, emotional and mental health, was used to assess HRQoL in weeks 1 and 12 of CR. Individual subscale scores and two summary scores, defined as a physical component score (PCS) and a mental component score (MCS), were computed. All subscales and components were graded from 0 (worst condition) to 100 (best condition).
Estimation of exercise dose
The dose of exercise received by each participant was estimated for the first and last three exercise sessions (i.e. weeks 1 and 12) of the 12 week programme. To calculate the exercise dose, the activity intensity for each exercise modality was estimated using the appropriate ACSM metabolic Equation [15] and this was multiplied by the activity duration. All activity performed for the week was summed to represent the weekly activity dose. All data are expressed in units of metabolic equivalents (METs) or kilocalories (kcal) by assuming that 1 L of oxygen consumed per minute is equal to 3.5 and that 1 L of oxygen yields 5.0 kcal of energy.
Statistical analysis
All analyses were performed using SPSS statistical software, version 17.0 (SPSS Inc., Chicago, IL, USA). The Kolmogorov–Smirnov test was used to confirm the parametric distribution for all outcome variables. Descriptive baseline characteristics are presented as a mean and standard deviation or as a percentage. The Mahalanobis distance analysis was used to detect potential outliers in the datasets for the change in mental health and physical health summary scores. Eight (≈ 14% of the sample) of the 58 participants were considered outliers for one or both variables and were removed from the final dataset. Thus, all subsequent analysis was based on a sample size of 50 participants. Differences in study outcomes between weeks 1 and 12 were determined using paired t test. In addition to the p values, detailed statistics including the mean and 95% confidence interval were calculated to provide a better interpretation of changes that occurred during the course of the study. The exercise dose examined as either the relative energy expenditure (kcal/kg) or exercise intensity (METs) was distributed into quartiles. The relationship between exercise dose and the mean change in SF-36 Mental and Physical Summary Scores was determined using linear and quadratic regression analysis for trends. An analysis of covariance (ANCOVA) was used to identify statistically significant differences between quartile groups. The p value was set at 0.05 for all analyses and adjusted using a Bonferroni correction to compensate for multiple comparisons between groups.
Results
None of the participants reported any adverse health effects during the exercise program. Nearly half (48%) of the participants did not complete at least 80% of the exercise sessions offered in the program; however, there were no significant differences in physical or Mental Health Summary Scores at 12-weeks between those participants completing greater or less than 80% of the available sessions.
Baseline characteristics are shown in Table 1. The majority of the current cohort were late-middle aged and older men (84% M, mean 61.6 years), who were overweight but not obese (BMI 28.97 ± 4.51 kg m− 2). Almost 60% of participants were taking a beta-adrenergic receptor blocker; 80% were taking lipid-lowering medication and 12% were taking glycemic control medication.
Changes in exercise energy expenditure over the 12-week program are presented in Table 2. Absolute and relative levels of energy expenditure and mean exercise session intensity were increased at 12 weeks (all p < 0.001). The SF-36 Mental Health Summary Score (p = 0.001) and the SF-36 Physical Health Summary Score were also increased after 12 weeks (p < 0.001).
Table 3 displays the quartile-based distribution values of the change in absolute and relative energy expenditure and average exercise session intensity over 12 weeks of exercise training. Although a statistically significant linear trend was not observed (i.e. p > 0.05), there was a strong quadratic trend between the mean change in SF-36 Mental (p = 0.058) and Physical (p = 0.051) Summary Scores and the relative energy expenditure (Table 4). The analysis of covariance showed that SF-36 Mental and Physical Summary Scores mean changes statistically fluctuate across the relative energy expenditure quartiles (Table 5). These data suggest there is a dose effect on the mean change in SF-36 Mental and Physical Summary Scores in that quartile 1 had little change in SF-36 score outcomes while those in quartile 2 had the greatest change in summary score values. The summary score values of quartile 3 and 4 were higher than quartile 1, but did not elicit further improvement in summary scores compared to that obtained in quartile 2.
Discussion
Improvement in health-related quality of life is a valuable and beneficial outcome for participants engaging in CR. It is worthwhile to better understand how this outcome can be used to optimize CR interventions. In this study we examined HRQoL data obtained from patients completing 12 weeks of phase-3 CR exercise training in order to test the hypothesis that there is a positive dose–response relationship between the change in exercise dose and the magnitude of change in HRQoL achieved after participation in a CR program. The novel finding of this study is that there appears to be a minimum or threshold dose of exercise required before there is an improvement in HRQoL. Surprisingly, the threshold dose of exercise found in this study was 3.9–5.7 kcal/kg/week (i.e. quartile 2) and higher doses of exercise (i.e. quartiles 3 and 4) resulted in progressively less improvement in HRQoL (see Table 5). Thus, our data suggest that while some exercise is certainly required to improve HRQoL, greater amounts of exercise does not necessarily result in greater outcomes.
The improvement on the SF-36 physical and Mental Health Summary Scores reported by our participants is consistent with previous reports [8, 9]. A recent meta-analysis of randomized controlled trials [16] reported an overall mean change of 6.9 on health-related quality of life as assessed by the Minnesota living with heart failure questionnaire (MLHFQ). A comparable effect size and mean change was observed in the current study in health-related quality of life as assessed by means of the Physical Summary Scores (effect size 0.625 and mean change 8.9) and the Mental Summary Scores (effect size 0.49 and mean change 5.2). These current findings are supported by previous works that also used the SF-36 for the assessment of health-related quality of life. For example, Meyer and Laederach-Hofmann [17] reported a mean change of 6.4 with an estimated effect size of 0.40 on the Mental Summary Scores after a CR program using a similar research design and sample size to the current study. While Meyer and coworkers did not observe a positive change in the Physical Summary Scores component, a significant improvement of the physical component when assessed by a disease-specific instrument (i.e. MLHFQ) was reported, which supports the contention of a positive impact of exercise on physical and mental components of health.
To our knowledge, only one previous study has attempted to examine whether the change in HRQoL is related in a dose–response manner to the amount of exercise performed in CVD patients [10]. This work reported a positive dose–response relationship between the exercise amount measured by pedometer and the improvement in health-related quality of life assessed by the MLHFQ. We found a statistically significant quadratic trend between exercise amount and the mean Physical Summary Scores and the Mental Summary Scores. However, we did not identify significant pairwise differences across the increasing exercise dose groups. Therefore, an exercise dose-dependence relationship for changes in health-related quality of life was not supported in the present study.
In the present study, we did not observe a positive change in both the Mental and Physical Summary Scores in those participants in the first quartile (i.e. the lowest values) for exercise dose. Instead, the current findings suggest that the greatest improvement in the Physical and Mental Health Summary Scores was achieved with a moderate amount of exercise (quartiles 2 and 3). Supporting the current findings, a dose–response relationship between the amount of exercise and quality of life measures (SF-36 Mental Health Summary Score ) was reported in 430 previously sedentary postmenopausal women [18]. Similarly, it has been found that a moderate amount of exercise was more efficacious than higher amounts of exercise for improving HRQoL in women with breast cancer receiving adjuvant therapy [19].
Cross-sectional [20] and longitudinal [21] population-based epidemiological studies support the present findings of a quadratic relationship between health-related quality of life and exercise amount. For the highest amount of exercise (i.e. the fourth quartile), the mean change in the Mental Health Summary Score appears to plateau. Further, the Physical Health Mental Summary Score mean change decreased in those participants performing the highest amounts of exercise suggesting that there may be a limit to the amount HRQoL improvement attainable through exercise. These findings agree with a previous population-based study [20]. A plausible hypothesis to explain a decrease in the Physical Health Summary Score at the highest amounts of exercise is that participants might expect greater results when performing these levels of exercise. Nevertheless, it has been previously reported that potential health risks and sometimes pain is associated with high intensities of exercise, which in turn could limit the activities of daily life performance [22] impacting on the perception of HRQoL. An alternative explanation might be that those capable of undertaking higher volumes of exercise already enjoy high levels of HRQoL and thus have less room to improve [23]. Nonetheless, future large randomized controlled trials are necessary to confirm the present findings.
Implications
The current study shows that patients entering in a phase-3 CR programme may benefit more from doing a moderate dose of exercise compared to a low or high amount of exercise. The regression coefficients of the quadratic models performed in this study show an inverse U relationship between exercise dose and HRQoL. Thus, if improving HRQoL is deemed an important outcome of a CR intervention, a moderate dose of exercise appears to be optimal. However, this recommendation needs to be carefully considered as the correlative values established in the current study suggests that the association between exercise dose and HRQoL is rather weak.
Strengths and limitations
There are several limitations to the current study that should be acknowledged. First, the urban location, relatively small sample size and pre-experimental research design limits the generalizability of the current results. Despite these limitations, the current study provides novel findings, which could be considered as “proof of concept”, and thus should be examined in a larger cohort. The SF-36 has been reported to be a sensitive tool for detecting the improvement in health-related quality of life after CR in patients with recent myocardial infarction [4, 24]; however, it should be noted that a generic tool like the SF-36 may not be sensitive to disease-specific issues that impact patient HRQoL. Future large prospective randomized controlled trials overcoming these and other potential limitations are required to confirm the current findings.
Conclusions
In summary, the current findings suggest that a phase-3 CR program improves physical and mental health-related quality of life. The magnitude of improvement appears to be dependent on exercise dose, in that there is a minimum dose required to improve HRQoL scores but increasing the exercise dose above this level does not confer additional benefit.
References
Gersh, B. J., et al. (2010). Novel therapeutic concepts: The epidemic of cardiovascular disease in the developing world: Global implications. European Heart Journal, 31(6), 642–648.
Mozaffarian.(2016). Heart disease and stroke statistics-2016 update: A report from the American Heart Association. (vol. 133, p. 38, 2016). Circulation, 133(15), E599–E599.
Selig, S. E. et al. (2010). Exercise & sports science Australia position statement on exercise training and chronic heart failure. Journal of Science and Medicine in Sport, 13(3), 288–294.
Thompson, D. R., & Yu, C. M. (2003). Quality of life in patients with coronary heart disease-I: Assessment tools. Health Qual Life Outcomes, 1, 42.
Williams, M. A., et al. (2006). Clinical evidence for a health benefit from cardiac rehabilitation: An update. American Heart Journal, 152(5), 835–841.
Berent, R., et al. (2011). Resistance training dose response in combined endurance-resistance training in patients with cardiovascular disease: A randomized trial. Archives of Physical Medicine and Rehabilitation, 92(10), 1527–1533.
Dalal, H. M., Doherty, P., & Taylor, R. S. (2015). Cardiac rehabilitation. BMJ, 351, h5000.
Clark, A. M., et al. (2005). Meta-analysis: Secondary prevention programs for patients with coronary artery disease. Annals of Internal Medicine, 143(9), 659–672.
Heran, B. S. et al. (2011). Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database of Systematic Reviews, 7, CD001800.
Evangelista, L. S., et al. (2010). Is exercise adherence associated with clinical outcomes in patients with advanced heart failure? The Physician and Sportsmedicine, 38(1), 28–36.
Vanhees, L., et al. (2012). Importance of characteristics and modalities of physical activity and exercise in the management of cardiovascular health in individuals with cardiovascular risk factors: Recommendations from the EACPR. Part II. European Journal of Preventive Cardiology, 19(5), 1005–1033.
CSEP. (2013). CSEP—PATH Physical Activity Training For Health 2013. Ottawa: Canadian Society For Exercise Physiology.
Dalleck, L. C., Schmidt, L. K., & Lueker, R. (2011). Cardiac rehabilitation outcomes in a conventional versus telemedicine-based programme. Journal of Telemedicine and Telecare, 17(5), 217–221.
Ware, J. E. Jr. (2000). SF-36 Health survey update. Spine , 25(24), 3130–3139.
Pescatello, L. S., et al. (2014). ACSM’s guidelines for exercise testing and prescription (9th ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins.
van der Meer, S., et al. (2012). Effect of outpatient exercise training programmes in patients with chronic heart failure: A systematic review. European Journal of Preventive Cardiology, 19(4), 795–803.
Meyer, K., & Laederach-Hofmann, K., (2003) Effects of a comprehensive rehabilitation program on quality of life in patients with chronic heart failure. Progress in Cardiovascular Nursing, 18(4), 169–176.
Martin, C. K., et al. (2009) Exercise dose and quality of life: A randomized controlled trial. Archives of Internal Medicine, 169(3), 269–278.
Carayol, M., et al. (2013). Psychological effect of exercise in women with breast cancer receiving adjuvant therapy: What is the optimal dose needed? Annals of Oncology, 24(2), 291–300.
Brown, D. W., et al. (2004). Associations between physical activity dose and health-related quality of life. Medicine and Science in Sports and Exercise, 36(5), 890–896.
Perales, F., Del Pozo-Cruz, J., & Del Pozo-Cruz, B. (2014). On the associations between physical activity and quality of life: Findings from an Australian nationally representative panel survey. Quality of Life Research, 23(7), 1921–1933.
Spirduso, W. W., & Cronin, D. L. (2001). Exercise dose-response effects on quality of life and independent living in older adults. Medicine and Science in Sports and Exercise, 33(6 Suppl), S598–S608. discussion S609–S610.
Saeidi, M., et al. (2013) Effects of a comprehensive cardiac rehabilitation program on quality of life in patients with coronary artery disease. ARYA Atherosclerosis, 9(3), 179–185.
Yu, C. M., et al. (2003). Long-term changes in exercise capacity, quality of life, body anthropometry, and lipid profiles after a cardiac rehabilitation program in obese patients with coronary heart disease. American Journal of Cardiology, 91(3), 321–325.
Acknowledgements
The Faculty of Science, University of Auckland, funded this study. We thank the participants in this study and all staff involved in the Health and Performance Clinics of the University of Auckland for all the support provided during the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
del Pozo-Cruz, B., Carrick-Ranson, G., Reading, S. et al. The relationship between exercise dose and health-related quality of life with a phase III cardiac rehabilitation program. Qual Life Res 27, 993–998 (2018). https://doi.org/10.1007/s11136-018-1784-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-018-1784-9