
Abstract
Purpose
The Patient-Reported Outcomes Measurement Information System® (PROMIS®) was designed to develop, validate, and standardize item banks to measure key domains of physical, mental, and social health in chronic conditions. This paper reports the calibration and validation testing of the PROMIS Self-Efficacy for Managing Chronic Conditions measures.
Methods
PROMIS Self-Efficacy for Managing Chronic Conditions item banks comprise five domains, Self-Efficacy for Managing: Daily Activities, Symptoms, Medications and Treatments, Emotions, and Social Interactions. Banks were calibrated in 1087 subjects from two data sources: 837 patients with chronic neurologic conditions (epilepsy, multiple sclerosis, neuropathy, Parkinson disease, and stroke) and 250 subjects from an online Internet sample of adults with general chronic conditions. Scores were compared with one legacy scale: Self-Efficacy for Managing Chronic Disease 6-Item scale (SEMCD6) and five PROMIS short forms: Global Health (Physical and Mental), Physical Function, Fatigue, Depression, and Anxiety.
Results
The sample was 57% female, mean age = 53.8 (SD = 14.7), 76% white, 21% African American, 6% Hispanic, and 76% with greater than high school education. Full-item banks were created for each domain. All measures had good internal consistency and correlated well with SEMCD6 (r = 0.56–0.75). Significant correlations were seen between the Self-Efficacy measures and other PROMIS short forms (r > 0.38).
Conclusions
The newly developed PROMIS Self-Efficacy for Managing Chronic Conditions measures include five domains of self-efficacy that were calibrated across diverse chronic conditions and show good internal consistency and cross-sectional validity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
The National Institutes of Health (NIH) Patient-Reported Outcomes Measurement Information System® (PROMIS®) was designed to develop, validate, and standardize item banks that measure key patient-reported outcomes including, symptoms of chronic conditions, functioning, and health-related quality of life [1]. The goal was to develop item banks, short forms, and Computerized Adaptive Tests (CAT) to enable comparison across disease conditions and be openly available to researchers. As such, most PROMIS measures are not disease-specific but, instead, global measures of patient-reported outcomes. PROMIS created an initial domain framework [1] that included self-efficacy as a desired bank to be developed under the mental health/positive psychological health domain. Funding provided by the NIH for the second wave of PROMIS included our grant to develop the self-efficacy domain.
Self-efficacy is the belief that one can carry out a behavior necessary to reach a desired goal, even when a situation contains unpredictable and stressful elements [2, 3]. For many intervention studies [4, 5], self-efficacy is a primary or secondary patient-reported outcome, or it may be an important mediator variable. Self-efficacy is a major determinant of behavior and behavioral change, and acts as a key mediator of the acquisition of self-management skills in chronic disease [3, 6, 7]. Bandura theorized that an individual’s perception of capabilities may be more predictive of function than the actual level of impairment [8]. Both cross-sectional and longitudinal studies across a range of disease conditions have shown greater self-efficacy to be associated with better health outcomes and a greater sense of well-being [9–18]. Furthermore, self-efficacy has been shown to be a modifiable [6, 7] and an important mediator between self-management skills and other patient outcomes, including depression, pain, emergency department visits, and increased physical activity [12, 19–23].
Previously validated self-efficacy scales reflect a range of subdomains of self-management skills in chronic disease, including self-efficacy for daily activities, for effectively working with the clinician, and for managing the condition [24–26]. Most self-efficacy scales were developed to measure disease-specific self-efficacy [9, 27]. Only one scale, the Self-Efficacy for Managing Chronic Disease 6-Item Scale (SEMCD6 [28]), is widely used to measure self-efficacy for managing chronic conditions across multiple health conditions [7, 29]. While the SEMCD6 includes items related to important domains of chronic conditions, including fatigue, pain, emotional stress, symptoms, activity, and medication, it does not provide subscale scores nor is it calibrated for CAT applications.
The development of the PROMIS Self-efficacy for Managing Chronic Conditions domain and item banks followed standard PROMIS guidelines [1, 30, 31], including development of definition, identification of domains, patient focus groups, and qualitative item review based on cognitive interviews. The final definition was: “Self-efficacy for Managing Chronic Conditions is defined as an individual’s confidence in his/her ability to successfully perform specific tasks or behaviors related to one’s health in a variety of situations.” This definition was determined by an online Delphi panel of 23 international experts who have published on self-efficacy for chronic conditions [32]. The Delphi panel also prioritized the domains of interest, resulting in the development of five item banks (Self-Efficacy for Managing: Daily Activities, Medications and Treatments, Symptoms, Emotions, and Social Interactions). These domains were further reviewed and confirmed by 78 patient participants in 12 focus groups, where additional content areas were identified. Over 1000 potential questionnaire items drawn from the literature and focus groups were reviewed by the investigative team, which including binning of similar items and then winnowing of redundant items by teams of two investigators. Items mentioned by more than one participant in the focus groups were created and added if not found in existing literature. The final items selected were reviewed by the full research team and then subjected to cognitive interviews with 30 patients. PROMIS reviewers also examined the items before calibration testing in a representative sample that is described here.
The goal of this paper is to report initial validity testing of the PROMIS Self-efficacy for Managing Chronic Conditions final calibrated item banks.
The specific aims are
-
1.
to validate five item banks of self-efficacy for managing chronic conditions across a range of chronic health conditions; and
-
2.
to investigate the characteristics of the five measures of Self-Efficacy for Managing Chronic Conditions by demographic characteristics, disease severity, disability, and mental health.
Methods
Sample
A total of 1,087 subjects completed the PROMIS Self-Efficacy for Managing Chronic Conditions measures. All forms were self-completed. Two sets of participants were included, those with (1) chronic neurologic conditions and (2) general medical conditions.
Patients with chronic neurologic conditions recruited from the University of Maryland Neurology Ambulatory Center (n = 837) were 18 years or older and had one of the following five neurologic conditions: epilepsy (n = 171), multiple sclerosis (MS, n = 166), neuropathy (n = 163), Parkinson’s disease (PD, n = 170), or stroke (n = 167). The original sampling goal was 150 participants per condition. Data in this part of the sample were collected from April 2013 to April 2014.
To improve generalizability to a wider range of general medical conditions, 250 participants were recruited from a national Internet panel maintained by Op4G, a private research community with approximately 250,000 members who participate in Internet-based surveys using home computers. Op4G participants are volunteers, and although they are spread across the USA, the panel is not nationally representative (see Op4G.com for more detail). To be eligible for this part of the sample, participants had to be 18 year or older and have at least one of the follow 20 chronic conditions: angina, arthritis, asthma, cancer, coronary artery disease, epilepsy, diabetes, myocardial infarction, chronic obstructive pulmonary disease, congestive heart failure, HIV or AIDS, kidney disease, liver disease, migraines, MS, neuropathy, PD, spinal cord injury, or stroke. Pre-specified target demographic distributions were identified that were representative of the age, gender, race, ethnic, and educational distributions of the U.S. general population [33]. Due to the low number of Hispanic participants in Baltimore, a target of 20% was included in this part of the sample to increase the overall Hispanic representation. The Internet data were collected August 25 to September 5, 2013.
Measures
PROMIS Self-efficacy for Managing Chronic Conditions banks and scales included the following five domains:
-
1.
Self-Efficacy for Managing Daily Activities The 36 items included assessment of the subject’s confidence in performing various activities of daily living (ADLs) without assistance. Items also assessed exercise, sexual activities, and managing activities in challenging situations (traveling, bad weather).
-
2.
Self-Efficacy for Managing Medications and Treatments The 26 items (27 initially, 1 dropped) included assessment of the subject’s confidence in managing medication schedules of different complexities. Items also assessed managing medication and other treatments in challenging situations such as when traveling, when running out of medication, and when adverse effects are encountered.
-
3.
Self-Efficacy for Managing Symptoms The 28 items included assessment of the subject’s level of confidence to manage/control their symptoms, to manage their symptoms in different settings (home, public place, an unfamiliar place), and to keep their symptoms from interfering with work, sleep, relationships, or recreational activities.
-
4.
Self-Efficacy for Managing Emotions The 27 items (28 initially, 1 dropped) included assessment of the subject’s level of confidence to manage/control symptoms of anxiety, depression, helplessness, discouragement, frustration, disappointment, and anger. Items also explored the presence of strategies to manage stress and loss.
-
3.
Self-Efficacy for Managing Social Interactions The 23 items (24 initially, 1 dropped) included assessment of the subject’s confidence in participating in social activities and getting help when necessary. Items also assessed managing communication with others about their medical condition, including communication with health professionals.
Items were scored on a 5-point Likert scale: 1 (I am not at all confident); 2 (I am a little confident); 3 (I am somewhat confident); 4 (I am quite confident); and 5 (I am very confident). Full-item banks, as well as 8-item and 4-item short forms, were created for the 5 domains. For all self-efficacy scales, a higher score meant more self-efficacy.
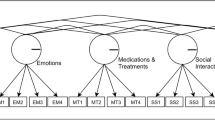
Testing and calibration of the banks followed the PROMIS standards for bank creation [1, 30, 31, 34]. Confirmatory factor analyses (CFA) were used to investigate the underlying structure (dimensionality) of the item bank using Mplus version 7.11 [35]. Because the data were treated as ordered categorical, all model parameters were estimated using the weighted least square mean-and-variance adjusted (WLSMV) estimator and a one-factor solution [36]. Dimensionality was investigated using model fit indices, including comparative fit index (CFI), Tucker–Lewis Index (TLI), and root mean square error of approximation (RMSEA) [30]. The residual correlation matrix from the single-factor CFA was used to evaluate local independence of the item bank. The criterion for the violation of the local independence was defined as a residual correlation greater than 0.2 with any of the remaining test items [30]. Item-total correlation and Cronbach’s coefficient alpha were used to evaluate internal consistency of the test items. The IRT analyses were conducted using IRTPRO version 2.1 [37]. A 2-parameter Graded Response Model was used to estimate item difficulty and item discrimination. Only 3 items were eliminated for violating local independence (1 in Managing Medications and Treatment, 1 in Managing Emotions, 1 in Managing Social Interactions).
The detailed psychometric results for one of the banks (Managing Daily Activities) have been previously published [34], but an overview of the findings from all the banks is presented here. Internal consistency of the five PROMIS Self-efficacy banks and short forms was high, with Cronbach’s alphas ranging from 0.96 to 0.97 for the full bank, 0.90–0.95 for the 8-item short forms, and 0.85–0.92 for the 4-item short forms. All measures demonstrated good item-total correlations (>0.55). The CFA model fit indices were moderate to high; observed CFIs were: 0.952 Daily Activities, 0.959 Emotions, 0.967 Medications and Treatments, 0.923 Symptoms, and 0.917 Social Interactions (where CFI > 0.95 is a good fit); TLI were: 0.949 Daily Activities, 0.955 Emotions, 0.953 Medications and Treatments, 0.917 Symptoms, and 0.909 Social Interactions (where TLI > 0.95 is a good fit); and RMSEA were: 0.090 Daily Activities, 0.127 Emotions, 0.089 Medication and Treatments, 0.127 Symptoms, and 0.118 Social Interactions (where RMSEA < 0.08 adequate fit). Factor loadings were all greater than 0.50. All short forms correlated highly with the full-item banks (r > 0.90 for 8-item short forms, r > 0.0.85 for 4-item short forms). All measures demonstrated good item-total correlations (r > 0.55 8-item short forms, r > 0.85 for 4-item short forms). None of the items across the five banks demonstrated differential item functioning (McFadden’s pseudo R2 > 10%) for age (18–55 years vs. 56+), sex (male vs. female), race (white vs. other), or data source (chronic neurologic conditions vs. general medical conditions).
Legacy self-efficacy measure
The Self-Efficacy for Managing Chronic Disease 6-Item scale (SEMCD6) was developed as part of the Stanford Patient Education Center [28]. Items were rated from 0 = not at all confident to 10 = totally confident and scores are averaged across items (final score 0–10). The SEMCD6 contains 6 items related to managing (1) fatigue, (2) physical discomfort/pain, (3) emotional distress, (4) other symptoms/health problems, (5) tasks/activities needed to manage health conditions, and (6) things other than just taking medication.
PROMIS version 1.0 short forms
Data were collected on six previously validated PROMIS version 1.0 short forms (SF, with the number afterwards stating the number of items, and the letter indicating the version) [1, 30, 31]: Physical Function SF12a, Anxiety SF8a, Depression SF8a, Fatigue SF8a, and Global Health 10a (which includes scales on Global Mental Health, 4 items, and Global Physical Health, 4 items). These are all normed to the U.S population as T-scores with a mean of 50 and standard deviation of 10. Higher scores on depression, anxiety, and fatigue indicate worse health (e.g., greater depression), while higher scores on the other scales indicate better health (e.g., greater physical functioning).
Clinical scales
Three clinician-reported scales were completed for the participants from the neurologic ambulatory center (n = 837); all disease-specific ratings were done for the index neurologic condition. Physicians rated severity of disease as 0 = none, 1 = mild, and 2 = moderate or severe. Two disability scales were completed: the modified Rankin Scale [38], which rates overall disability from 0 = no disability to 6 = dead, and the Barthel Index,[39–41] which ranges from 0 to 100, with lower score indicating better functioning. In addition, duration of disease (number of years since diagnosis) was also completed by the physician.
Analyses
Description of derived banks
Descriptive statistics were used to describe the demographic characteristics of the sample. Scores for PROMIS scales are presented based on T-score units, with a mean of 50 and a standard deviation of ten. For the PROMIS Self-efficacy banks and scales, the T clin designation is provided, as our sample is a clinical sample (by definition, as the bank refers to managing a chronic disease condition). Differences in the means of the PROMIS Self-efficacy scales and the SEMCD6 legacy measure by the demographic groups were tested using Analysis of Variance (ANOVA) models.
Concurrent validity
Pearson product moment correlations of the five PROMIS Self-efficacy scales with each other and with the SEMCD6 legacy measure were computed. Correlations were also compared with the PROMIS short forms, as well as the clinical measures within the neurologic sample to examine convergent validity.
Results
Descriptive statistics
Table 1 presents sample demographics and the distributions of the PROMIS Self-efficacy scales by these demographics. The sample was 57% female, mean age = 53.8 (SD = 14.7, range 18–89), 76% white, 21% African American, 3% other race, with 6% Hispanic. Education level was above high school for 80% of the sample and income over $60,000 a year for 54%. The majority were currently married (59%) and not employed (59%). All subjects (by definition) had at least one chronic condition, with 45% having 4 or more. Most data came from the neurologic data source (77%).
PROMIS Self-efficacy measures differed by most demographic characteristics. Younger age was significantly associated with better Self-efficacy for Managing Daily Activities, but worse Self-efficacy for Managing Emotions and Managing Social Interactions. Females scored higher on Managing Medications and Treatments, but did not differ for other measures. Those of non-white race and Hispanic ethnicity scored lower on all the PROMIS Self-efficacy domains. Married participants scored higher on all the PROMIS Self-efficacy banks, except for Managing Symptoms. Those who were employed and had higher incomes had higher scores on all PROMIS Self-efficacy domains. Those with more chronic conditions scored lower on all PROMIS Self-efficacy banks. Finally, the chronic neurologic sample scored higher than those with general medical conditions completing questionnaires on the Internet (although not significant for Managing Daily Activities).
Most observed differences by the demographics were less than 5 Tclin units (0.5 standard deviation), a less than medium effect size difference. The differences by Hispanic ethnicity were larger than 0.5 standard deviation for all the PROMIS self-efficacy banks (ranging from 7.9 to 10.4 Tclin units). Differences of around 5 Tclin units were seen for Self-efficacy for Managing Daily activities by income and by comorbidity (1 vs. 6+ conditions) and for Self-efficacy for Managing Symptoms by comorbidity. Self-efficacy for managing Emotions and Social Interactions also differed by more than 5 Tclin units by source of data, with higher scores for the general medical conditions sample.
For the SEMCD6 legacy measure, self-efficacy was higher among those with higher age, higher education, white race, non-Hispanic, being married, currently employed, greater income, and fewer comorbidities. The chronic neurologic sample also scored higher on the SEMCD6 than those with general medical conditions completing questionnaires on the Internet. Again, most comparisons were less than 0.5 standard deviations (about 1 point on the SEMCD6), with the exception of Hispanic ethnicity (1.1 points) and comorbidity (1.5 points difference between 1 and 6+ comorbidities).
Concurrent validity
Table 2 presents the intercorrelations among the PROMIS Self-efficacy banks and correlation with the legacy scale. All correlations within the PROMIS Self-efficacy banks were significant (r < .001) with r = 0.59 or higher. The highest correlation within the PROMIS Self-efficacy banks was between Managing Symptoms and Managing Social Interactions (r = 0.76), and lowest between Managing Daily Activities and Managing Social Interactions (r = 0.59). Correlations of the PROMIS Self-efficacy banks with the SEMCD6 legacy measure were all positive and ranged from r = 0.57 (Managing Medications and Treatments) to r = 0.76 (Managing Symptoms).
Table 3 presents the correlations of the PROMIS Self-efficacy banks with the PROMIS short forms and with clinical measures, as well as the means for these comparison measures. As a whole, this sample scored close to the normed T-score of 50 for Fatigue, Depression, Anxiety, and Global Physical Health, but were about 5 T-score units lower than the national average on Physical Function and Global Mental Health. The PROMIS Self-efficacy banks correlated significantly (all r < .001) with all the PROMIS short forms. The highest correlations for Self-efficacy for Managing Daily Activities was with Physical Function (r = 0.78) and Global Physical Health (r = 0.75). The highest correlations for Self-efficacy for Managing Emotions was with Global Mental Health (r = 0.70) and Depression (r = −0.69). The highest correlation with Managing Medications and Treatments was with Global Mental Health (r = 0.52). The highest correlation with Managing Social Interactions and with Managing Symptoms (r = 0.63) was also with Global Mental Health. The highest correlation with Fatigue was with Self-efficacy for Managing Daily Activities (r = −0.54) and Self-efficacy for Managing Emotions (r = −0.54). The SEMCD6 legacy measure had higher correlations with Fatigue (r =−0.65) than the PROMIS Self-efficacy banks (r = −0.39 to −0.54).
Correlations of the PROMIS Self-efficacy banks with the clinical measures (physician-rated) were lower than the correlations among the patient-reported measures. Self-efficacy for Managing Daily Activities correlated significantly with disease severity (r = −0.43), modified Rankin (r = −0.47), and Barthel Index (r = 0.46) and had the highest correlations with disease severity and disability measures as compared to the other PROMIS Self-efficacy banks. Disease duration was only significantly correlated with Self-efficacy for Managing Medications and Treatments (r = −0.11), Managing Emotions (r = 0.09), and Managing Symptoms (r = 0.09), and these correlations were low. The SEMCD6 legacy measure had significantly lower correlations with disease severity, modified Rankin, and Barthel Index than the PROMIS Self-efficacy for Managing Daily Activities measure (differences between correlations p < .001).
Conclusions
The newly developed PROMIS Self-efficacy for Managing Chronic Conditions domains include five item banks (Self-efficacy for: Managing Daily Activities, Managing Emotions, Managing Medications and Treatments, Managing Social Interactions, and Managing Symptoms) that have been calibrated across diverse chronic conditions and show good internal consistency and cross-sectional validity. Short-form versions of these measures have also been created with 4 items and 8 items (scoring and calibration information can be freely obtained from the PROMIS website: http://www.healthmeasures.net/explore-measurement-systems/promis).
The PROMIS Self-efficacy for Managing Chronic Conditions banks differed in expected ways on a number of demographic characteristics, with higher self-efficacy scores seen among participants who were white, non-Hispanic, married, employed, had higher income, and with fewer chronic conditions. The differences between Hispanic and non-Hispanic and by level of comorbidity were the largest. Previous studies have shown greater difficulty in disease management among Hispanics, perhaps due to language and cultural barriers, lack of access to preventive services, lack of insurance, and greater medical comorbidity [42]. The mean SEMCD6 rating for the Hispanic sample in this study is similar to those reported in two randomized controlled trials of disease management among Hispanics [42].
Younger age was associated with better Self-efficacy for Managing Daily Activities, but worse Self-efficacy for Managing Emotions and Managing Social Interactions. This result is consistent with other findings in emotional health and social functioning supportive of the socio-emotional selectivity theory [43]. This theory builds upon the observation that older persons maintain higher levels of emotional health and quality of social interactions in the face of declining health through selective focus on more positive emotions and even positive cognitive stimuli. The SEMCD6 legacy measure also showed higher scores (higher self-efficacy) among those over age 65. The fact that Self-efficacy for Managing Daily Activities was higher in the youngest age group (as opposed to lower as for Emotions and Social Interactions) may be supportive of the need for domain-specific self-efficacy measures as proposed by Bandura [8].
Surprisingly, the chronic neurologic sample reported greater self-efficacy for managing conditions on all domains compared to those with general medical conditions completing the self-efficacy measures on the Internet. Findings describing the differences within the neurologic conditions will be published in another paper [44]. We explored whether this finding could be attributed to the higher prevalence of Hispanics in the Internet sample, but the difference was seen among non-Hispanics also. Higher scores from the chronic neurologic sample than the general medical sample Internet sample was also seen in the PROMIS short forms for Depression, Anxiety, Fatigue, and Global Mental Health (but not Global Physical Health or Physical Function, results not presented) in addition to the self-efficacy measures. We are unsure whether these differences may be due to location of administration (more reluctance to disclose mental health issues in-person versus the Internet, even though both sources self-completed the items) or to selection effects based on use of a self-nominating online survey population. Previous PROMIS findings did not show differences across settings for self-completed questionnaires (e.g., paper and pencil in a clinic versus Internet at home) for the PROMIS physical function, fatigue, and depression banks [45]. Neither our study nor previous PROMIS work has tested administration of forms by interviewers versus self-completion. Differences may also be explained by better quality of care in the chronic neurologic sample recruited from a neurology practice than the Internet survey population with self-reported chronic conditions. This finding warrants further exploration about the use of Internet surveys as samples for patient-reported outcomes.
All of the PROMIS self-efficacy measures correlated highly with the legacy measure and with the PROMIS short forms, supporting convergent validity. The SEMCD6 legacy measure correlated the most with Managing Symptoms, which is expected since many of the SEMCD6 items are symptoms. The SEMCD6 legacy measure showed greater correlation with Fatigue than the PROMIS self-efficacy measures—not surprising since fatigue is one of the six items. The SEMCD6 did correlate well across the PROMIS short forms (r > 0.5), although not as highly as the PROMIS Self-efficacy measures.
The highest correlations among the PROMIS self-efficacy measures and the PROMIS short forms were with PROMIS Self-efficacy for Managing Daily Activities and PROMIS Global Physical Health and Physical Function, which again was consistent with our expectations. Managing Daily Activities also showed the greatest correlations with the physician-rated disease and disability measures among all the PROMIS Self-efficacy banks. The high correlation between the Self-efficacy for Managing Daily Activities bank and the Physical Function short form (r = 0.78) raises questions about the difference between these domains. The self-efficacy questions ask about confidence in doing daily activities, while the Physical Function short form asks about the ability to perform daily activities. It is not surprising that these two measures are highly correlated, but it is in the cases where these measures do not agree that the most interesting information is found about the potential value of interventions to improve self-management skills. Patients who overestimate their self-management skills and abilities may engage in risky behaviors (e.g., walking in dangerous situations that may lead to falls) and those who underestimate their abilities may self-limit and underperform (e.g., fear of falling resulting in inactivity that leads to muscle wasting and weakness). Self-efficacy is an import independent predictor of health outcomes, and research has shown that self-efficacy can predict health outcomes better than actual change in health behaviors [20].
The chief limitation of this study is the cross-sectional nature of the assessment of validity. Further work is needed to examine whether these self-efficacy measures are independent predictors of outcomes while controlling for functional status. In addition, assessment of responsiveness to change and minimally important differences will be important to see if the PROMIS self-efficacy banks are sensitive to changes over time after interventions or other changes known to impact functioning or health-related quality of life. Validation in other samples of chronic conditions is also necessary.
In conclusion, the PROMIS self-efficacy measures provide a set of five item banks and short forms that have been psychometrically developed and tested using item-response theory. They allow for computerized adaptive testing and provide norms based on a large sample of patients with chronic medical conditions. The item banks (including CATs) and short forms are freely available to clinicians and researchers who want to evaluate patient confidence in performing important tasks and behaviors for managing chronic medical conditions.
References
Cella, D., et al. (2010). The Patient-Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005–2008. Journal of Clinical Epidemiology, 63(11), 1179–1194.
Bandura, A. (1989). Human agency in social cognitive theory. The American Psychologist, 44(9), 1175–1184.
Clark, N. M., & Dodge, J. A. (1999). Exploring self-efficacy as a predictor of disease management. Health Education & Behavior, 26(1), 72–89.
Ashford, S., Edmunds, J., & French, D. P. (2010). What is the best way to change self-efficacy to promote lifestyle and recreational physical activity? A systematic review with meta-analysis. British Journal of Health Psychology, 15(Pt 2), 265–288.
Bodenheimer, T., et al. (2002). Patient self-management of chronic disease in primary care. JAMA, 288(19), 2469–2475.
Holman, H. R., & Lorig, K. (1992). Perceived self-efficacy in self-management of chronic disease, in Self-efficacy: thought control of action. New York: Hemishperes Publications.
Lorig, K. R., et al. (2001). Effect of a self-management program on patients with chronic disease. Effective Clinical Practice, 4(6), 256–262.
Bandura, A., & Self-efficacy (1977). toward a unifying theory of behavioral change. Psychological Review, 84(2), 191–215.
Schwartz, C. E., et al. (1996). Measuring self-efficacy in people with multiple sclerosis: a validation study. Archives of Physical Medicine and Rehabilitation, 77(4), 394–398.
Wu, A. M., Tang, C. S., & Kwok, T. C. (2004). Self-efficacy, health locus of control, and psychological distress in elderly Chinese women with chronic illnesses. Aging & Mental Health, 8(1), 21–28.
Chlebowy, D. O., & Garvin, B. J. (2006). Social support, self-efficacy, and outcome expectations: impact on self-care behaviors and glycemic control in Caucasian and African American adults with type 2 diabetes. The Diabetes Educator, 32(5), 777–786.
Lorig, K., et al. (1985). Outcomes of self-help education for patients with arthritis. Arthritis and Rheumatism, 28(6), 680–685.
Beckham, J. C., et al. (1997). Self-efficacy and adjustment in cancer patients: A preliminary report. Behavioral Medicine, 23(3), 138–142.
Denison, E., Asenlof, P., & Lindberg, P. (2004). Self-efficacy, fear avoidance, and pain intensity as predictors of disability in subacute and chronic musculoskeletal pain patients in primary health care. Pain, 111(3), 245–252.
Kuijer, R. G., & D.T.D. De Ridder (2003). Discrepancy in illness-related goals and quality of life in chronically ill patients: The role of self-efficacy. Psychology & Health, 18(3), 313–330.
Riazi, A., Thompson, A. J., & Hobart, J. C. (2004). Self-efficacy predicts self-reported health status in multiple sclerosis. Multiple Sclerosis, 10(1), 61–66.
Hellstrom, K., et al. (2003). Self-efficacy in relation to impairments and activities of daily living disability in elderly patients with stroke: A prospective investigation. Journal of Rehabilitation Medicine, 35(5), 202–207.
Edwards, R., et al. (2001). Self-efficacy as a predictor of adult adjustment to sickle cell disease: One-year outcomes. Psychosomatic Medicine, 63(5), 850–858.
Holman, H., Mazonson, P., & Lorig, K. (1989). Health education for self-management has significant early and sustained benefits in chronic arthritis. Transactions of the Association of American Physicians, 102, 204–208.
Lenker, S. L., Lorig, K., & Gallagher, D. (1984). Reasons for the lack of association between changes in health behavior and improved health status: An exploratory study. Patient Education and Counseling, 6(2), 69–72.
Lorig, K., et al. (1989). The beneficial outcomes of the arthritis self-management course are not adequately explained by behavior change. Arthritis and Rheumatism, 32(1), 91–95.
Howorka, K., et al. (2000). Empowering diabetes out-patients with structured education: Short-term and long-term effects of functional insulin treatment on perceived control over diabetes. Journal of Psychosomatic Research, 48(1), 37–44.
Rigby, S. A., Thornton, E. W., & Young, C. A. (2008). A randomized group intervention trial to enhance mood and self-efficacy in people with multiple sclerosis. British Journal of Health Psychology, 13(Pt 4), 619–631.
Lev, E. L., & Owen, S.V. (1996). A measure of self-care self-efficacy. Research in Nursing & Health, 19(5), 421–429.
Fernandez, S., et al. (2008). Revision and validation of the medication adherence self-efficacy scale (MASES) in hypertensive African Americans. Journal of Behavioral Medicine, 31(6), 453–462.
Rodgers, W. M., et al. (2008). Evidence for a multidimensional self-efficacy for exercise scale. Research Quarterly for Exercise and Sport, 79(2), 222–234.
Frei, A., et al. (2009). Self-efficacy instruments for patients with chronic diseases suffer from methodological limitations—A systematic review. Health and Quality of Life Outcomes, 7, 86.
Lorig, K. S. A., Ritter, P., González, V. (1996). Outcome measures for health education and other health care interventions. Thousand Oaks: Sage Publications, Inc.
Lorig, K., Chastain, R. L., Ung, E., Shoors, S., & Holman, H. R. (1989). Development and evaluation of a scale to measure perceived self-efficacy in people with arthritis. Arthritis & Rhuematology, 32(1), 37–44.
Reeve, B. B., et al. (2007). Psychometric evaluation and calibration of health-related quality of life item banks: Plans for the Patient-Reported Outcomes Measurement Information System (PROMIS). Medical Care, 45(5 Suppl 1), S22–S31.
DeWalt, D.A., Rothrock, N., Yount S., Stone, A., on behalf of the PROMIS Cooperative Group. (2007). Evaluation of item candidates—The PROMIS qualitative item review. Medical Care, 45, S12–S21.
Sood, P., Romero, R., Velozo, C., Gruber-Baldini, A., Shulman L.(2015). Defining and prioritizing sub-domains of self-efficacy for managing chronic conditions: A web-based delphi technique. Archives of Physical Medicine and Rehabilitation, 96, 10, e4.
Rothrock, N. E., et al. (2010). Relative to the general US population, chronic diseases are associated with poorer health-related quality of life as measured by the Patient-Reported Outcomes Measurement Information System (PROMIS). Journal of Clinical Epidemiology, 63(11), 1195–1204.
Hong, I., et al. (2016) Assessment of the psychometrics of a PROMIS item bank: Self-efficacy for managing daily activities. Quality of Life Research. 25(9), 2221–2232.
Muthén, L. K., & Muthén, B. O. ( 2012) Mplus. Los Angeles: Muthén & Muthén.
Revicki, D. A., et al. (2014). Exploratory and confirmatory factor analysis of the PROMIS pain quality item bank. Quality of Life Research, 23(1), 245–255.
Cai, L., Thissen, D., & S.H.C. du Toit (2011). IRTPRO for Windows. Lincolnwood: Scientific Software International.
Bonita, R., & Beaglehole, R. (1988). Recovery of motor function after stroke. Stroke, 19(12), 1497–1500.
Collin, C., et al. (1988). The Barthel ADL Index: a reliability study. International Disability Studies, 10(2), 61–63.
Mahoney, F. I., & Barthel, D. W. (1965). Functional evaluation: The Barthel Index. Maryland State Medical Journal, 14, 61–65.
Wade, D. T., & Collin, C. (1988). The Barthel ADL Index: A standard measure of physical disability? International Disability Studies, 10(2), 64–67.
Melchior, M. A., et al. (2013). Intermediate outcomes of a chronic disease self-management program for spanish-speaking older adults in South Florida, 2008–2010. Preventing Chronic Disease, 10, E146.
Carstensen, L. L., Isaacowitz, D. M., & Charles, S. T. (1999). Taking time seriously. A theory of socioemotional selectivity. The American Psychologist, 54(3), 165–181.
Gruber-Baldini, A., Velozo, C., Romero, S., Barr, E., Armstrong, M., & Shulman, L. (2014). PROMIS physical and mental health measures across 5 neurologic disorders, platform, American neurologic association annual meeting. Annals of Neurology, 76, S36.
Bjorner, J. B., et al. (2014). Difference in method of administration did not significantly impact item response: an IRT-based analysis from the Patient-Reported Outcomes Measurement Information System (PROMIS) initiative. Quality of Life Research, 23(1), 217–227.
Acknowledgements
The study was funded by the National Institutes of Health, Grant 1U01AR057967-01, “Development and Validation of a Self-Efficacy Item Bank,” awarded to Lisa Shulman (Principal Investigator) and Ann Gruber-Baldini, Sergio Romero, and Craig Velozo (Co-Investigators). The results and conclusions presented in this paper are those of the authors and are independent from the funding source. The scales and item banks described in this paper are freely available at http://www.healthmeasures.net/explore-measurement-systems/promis. The authors would like to thank other members of the research team for their efforts, including Karen Anderson, MD, Barbara Resnick, RN, PhD, Melissa Armstrong, MD, Erik Barr, MS, Latasha Shoffner, BA, Katrina Schrader, BA, Rena Atayeva, BA, Yoo Jin Rhee, BA, Chih-Ying Li, Ickpyo Hong, and Maria Okafor, PhD.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics/IRB approvals
Informed consent was obtained from all individual participants included in the study. This study was approved by the Institutional review boards (IRB) of the University of Maryland (#HP-000432550), the Medical University of South Carolina (#Pro00033397), and the University of Florida (#261–2010). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Gruber-Baldini, A.L., Velozo, C., Romero, S. et al. Validation of the PROMIS® measures of self-efficacy for managing chronic conditions. Qual Life Res 26, 1915–1924 (2017). https://doi.org/10.1007/s11136-017-1527-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-017-1527-3