
Abstract
Fun For Wellness (FFW) is a self-efficacy theory-based online behavioral intervention that aims to promote growth in physical activity and well-being. The FFW conceptual model for the promotion of subjective well-being posits that FFW exerts both a positive direct effect, and a positive indirect effect through well-being self-efficacy, on subjective well-being. Subjective well-being is defined in FFW as an individual’s satisfaction with their status in seven key domains of their life. Well-being self-efficacy is defined in FFW as the degree to which an individual perceives that they have the capability to attain a positive status in seven key domains of their life. The objective of this study was to use baseline target moderation to assess variation in the impact of FFW on subjective well-being dimensions in adults with obesity. Data (N = 667) from the Well-Being and Physical Activity Study (ClinicalTrials.gov, identifier: NCT03194854) were reanalyzed. There was evidence that well-being self-efficacy at baseline moderated the direct effect of FFW on well-being self-efficacy at 30 days post-baseline for the occupational and psychological dimensions. Both of these findings suggest a “compensatory” effect. Similarly, there was evidence that well-being self-efficacy at baseline moderated the indirect effect of FFW on subjective well-being at 60 days post-baseline through well-being self-efficacy at 30 days post-baseline for the occupational and psychological dimensions. Both of these findings suggest a “compensatory” effect. Finally, there was evidence that well-being self-efficacy at baseline moderated the direct effect of FFW on subjective well-being at 60 days post-baseline for the community, occupational, and physical dimensions. Each of these three findings suggests some version of a “rich-get-richer” effect. In summary, results provide both supportive and unsupportive (i.e., interpersonal, economic, and overall dimensions) evidence regarding variation in the impact of the FFW intervention and should impact the design of future FFW trials.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The current study is intended to contribute to the special issue entitled: When is it time to revise or adapt our prevention programs? Using baseline target moderation (BTM) to assess variation in prevention impact (Howe & Leijten, 2020). Specifically, the current study considers whether it is necessary to revise or adapt the Fun For Wellness intervention program (FFW; Myers et al., 2017a, b). The first aim is to introduce BTM as a means of exploring theory-driven moderation of malleable targets specified within the FFW conceptual model for the promotion of subjective well-being (Myers et al., 2021). The second aim is to present findings of BTM statistical models by reanalyzing data from the 2018 Well-Being and Physical Activity study (Myers et al., 2019), highlighting the range of different patterns of heterogeneous impact for the FFW intervention. The third aim is to discuss how the findings from the second aim can inform successful adaptation of the FFW intervention to increase its impact and guide the design of its future trials. Prior to addressing these aims, we first provide an overview of the most recently completed FFW trial.
The 2018 WBPA Study
The 2018 Well-Being and Physical Activity (WBPA) study (Myers et al., 2019) is the most recently completed FFW trial. The objective of the WBPA study was to provide the first investigation of the effectiveness of FFW to increase well-being and physical activity in adults with obesity in the United States of America (USA). There were three main outcomes in the WBPA study: subjective well-being, well-being actions, and physical activity. A separate conceptual model was constructed for each of these outcomes, that is, the FFW conceptual model for the promotion of (1) subjective well-being (Myers et al., 2021), (2) well-being actions (Lee et al., 2021), and (3) physical activity (Myers, et al., 2020). Within each of the FFW conceptual models, a self-efficacy construct (i.e., well-being self-efficacy, well-being actions self-efficacy, and physical activity self-efficacy) was targeted as a theory-driven malleable mediator of the concordant main outcome (i.e., subjective well-being, well-being actions, and physical activity, respectively). Data collection details relevant to the current study will be reported in the “Methods” section. Readers are referred to Lee et al. (2021) for the well-being actions results and Myers et al. (2020) for the physical activity results. Given that the focus of the current manuscript is on subjective well-being, results (under a non-BTM approach) reported in Myers et al. (2021) will be reviewed below. Before doing so, however, we provide a brief review of the target population, theoretical framework, and intervention in the WBPA study.
Target Population in the WPBA Study: Adults with Obesity
Billions of adults are with overweight (World Health Organization [WHO], 2018). Furthermore, roughly one-third of adults with overweight (i.e., body mass index [BMI] is greater than or equal to 25.00 kg/m2 and less than or equal to 29.99 kg/m2) can more accurately be categorized as adults with obesity (i.e., BMI greater than or equal to 30.00 kg/m2) and the magnitude of observations within this category has increased threefold over the past few decades (WHO, 2018). The trend toward an increasing number of adults with obesity is problematic from a public health perspective because obesity is a risk factor for major non-communicable chronic diseases such as cardiovascular disease, type II diabetes, musculoskeletal disorders, and some cancers (United States Department of Health and Human Services [USDHHS], 2013). To reduce the prevalence of adults with obesity, the WHO (2018) recommends that individuals engage in regular physical activity (e.g., at least 2.5 h at a moderate intensity each week). There is evidence, however, that a very large percentage (e.g., ~ 95%) of adults with obesity do not meet public health guidelines for physical activity (Tudor-Locke et al., 2010). Fortunately, there is also evidence that cognitive-behavioral interventions can successfully promote physical activity in adults with obesity (Gourlan et al., 2011). To encourage sustained engagement with physical activity promoting interventions, the potential for experiencing health benefits across a broader array of health dimensions (e.g., subjective well-being) may be targeted and emphasized (United States Department of Health and Human Services, 2013). More generally, broadly focused interventions for populations at-risk for a narrower health or social problem is an established practice in prevention (e.g., United States Preventive Services Task Force [USPSTF], 2018).
Behavioral Change Theory in the WBPA Study: Self-efficacy Theory
Self-efficacy theory (Bandura, 1997) resides within social cognitive theory and views an individual as a proactive agent in the regulation of their emotions, cognitions, and behaviors. Self-efficacy beliefs play a primary role in self-efficacy theory and are defined as domain-specific judgments held by an individual about their ability to successfully execute differing levels of performance given certain situational demands. Self-efficacy beliefs rely upon the cognitive processing of several potential sources of efficacy information: enactive mastery experiences, vicarious experiences, verbal persuasion, and physiological and/or emotional states. Two proposed omnibus outcomes of self-efficacy beliefs are an individual’s thought patterns (e.g., subjective well-being) and behaviors (e.g., physical activity). A necessary condition for valid testing of self-efficacy theory is a high degree of concordance between the domain specific self-efficacy beliefs (e.g., well-being self-efficacy) and the domains of the proposed outcomes (e.g., subjective well-being) of interest (Bandura, 1997). Targeting domain specific self-efficacy beliefs as a potentially modifiable mediating variable via intervention is an established practice in prevention science (e.g., Beauchamp et al., 2019; Mihelic et al., 2016).
The Intervention in the WBPA Study: Fun For Wellness
Fun For Wellness is a self-efficacy theory-based online behavioral intervention developed to promote growth in well-being and physical activity by providing capability-enhancing opportunities to participants (Myers et al., 2019). The capability-enhancing learning opportunities provided to FFW participants come in the form of 152 interactive and scenario-based challenges organized in the on-line environment by the BET I CAN acronym (Myers et al., 2017a, b). “B” challenges are designed to focus on behaviors (e.g., setting a goal). “E” challenges are designed to focus on emotions (e.g., coping with negative feelings). “T” challenges are designed to focus on thoughts (e.g., challenging negative assumptions). “I” challenges are designed to focus on interactions (e.g., communicating with other people). “C” challenges are designed to focus on contexts (e.g., reading cues in the environment). “A” challenges are designed to focus on awareness (e.g., knowing yourself). “N” challenges are designed to focus on next steps (e.g., making a plan). Readers are referred to Myers et al. (2019) for a review of the scientific literature for each type of BET I CAN challenge.
The FFW Conceptual Model in the WBPA Study
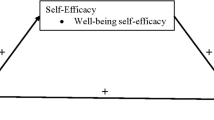
The FFW conceptual model for the promotion of subjective well-being posits that FFW exerts both a positive direct effect, and a positive indirect effect through well-being self-efficacy, on subjective well-being (Myers et al., 2021). Subjective well-being is defined as an individual’s satisfaction with their status in key domains of their life: interpersonal, community, occupational, physical, psychological, economic, and overall (I COPPE; Myers et al., 2017a, b). Well-being self-efficacy is defined as the degree to which an individual perceives that they have the capability to attain a positive status in key (i.e., I COPPE) domains of their life (Myers et al., 2017a, b). Figure 1 illustrates the FFW conceptual model for the promotion of subjective well-being.

The Fun For Wellness conceptual model for the promotion of multidimensional subjective well-being under a baseline target moderation (BTM) approach. Note. A dashed line indicates a path not estimated in Myers et al. (2020). The expression — baseline target moderated mediation (BTMM) — may be used when focusing on the product: a path × b path, conditioned on the targeted mediator at baseline
Four construct-level hypotheses were investigated in the WBPA study based on the conceptual model (ignoring paths with a dashed line) illustrated in Fig. 1. In Myers et al. (2021), an a priori hypothesis approach, and not a more exploratory research question approach, was taken based on relevant findings from the 2015 FFW efficacy trial. The first hypothesis focused on the “a path” in Fig. 1. Partial support for this hypothesis was observed in the form of FFW exerting a statistically significant positive direct effect on both occupational and psychological well-being self-efficacy at 30 days post-baseline. The second hypothesis focused on the “b path” in Fig. 1. Full support for this hypothesis was observed in the form of well-being self-efficacy at 30 days post-baseline exerting a statistically significant positive direct effect on subjective well-being at 60 days post-baseline for each of the seven I COPPE dimensions. The third hypothesis focused on the “c’ path” in Fig. 1. Partial support for this hypothesis was observed in the form of FFW exerting a statistically significant positive direct effect on both community and physical subjective well-being at 60 days post-baseline. The fourth hypothesis focused on the indirect effect, operationalized as the product of “a path” and the “b path” in Fig. 1. Partial support for this hypothesis was observed in the form of FFW exerting an indirect effect on subjective well-being at 60 days post-baseline through well-being self-efficacy at 30 days post-baseline for both the occupational and psychological dimensions. These prior findings from Myers et al. (2021) were based on a model that did not account for the potential moderating role of well-being self-efficacy at baseline.
New Research Questions Under a BTM Approach
BTM designs test whether intervention effects, direct and indirect, vary by baseline level of theoretically relevant intervention targets for the purpose of informing the design of future trials (Howe & Leijten, 2020). Recall that the first aim of this paper is to introduce BTM as a means of exploring theory-driven moderation of malleable targets specified within the FFW conceptual model for the promotion of subjective well-being. Accordingly, this manuscript explores three new construct-level research questions based on the dashed paths within the FFW conceptual model for the promotion of multidimensional subjective well-being in Fig. 1.
Research Question 1
Did well-being self-efficacy at baseline moderate the direct effect of the FFW intervention on well-being self-efficacy at 30 days post-baseline (i.e., the “a path”)?
Research Question 2
Did well-being self-efficacy at baseline moderate the indirect effect of the FFW intervention on subjective well-being at 60 days post-baseline through well-being self-efficacy at 30 days post-baseline (i.e., the “a path” x “b path”)?
Research Question 3
Did well-being self-efficacy at baseline moderate the direct effect of the FFW intervention on subjective well-being at 60 days post-baseline (i.e., the “c’ path”)?
In the current study, an exploratory research question approach was taken based on a lack of previous BTM research on FFW trials. Addressing this gap in the literature is important because it may increase understanding of for whom (e.g., subgroups of adults with obesity) and how (e.g., directly and/or indirectly via well-being self-efficacy) the FFW intervention is effective.
Method
The data described in this manuscript were collected in the WBPA study (see Myers et al., 2019 for protocol and Myers et al., 2020 for a populated CONSORT-EHEALTH checklist). The data analyzed in this manuscript were analyzed by Myers et al. (2021) under a non-BTM approach. These data were reanalyzed under a BTM approach in the current manuscript to investigate three new research questions. Some of the text that will describe the methods used in WBPA study is similar to the text in Myers et al. (2021). We provide this text so that the reader does not need to consult a previously published paper in order to understand methods used in the WBPA study that are important to understand the data used in the present study (American Psychological Association, 2020).
Research Design
The WBPA study was a large-scale, prospective, double-blind (i.e., investigators, outcome assessor were masked), parallel group randomized controlled trial (RCT). Recruiting, screening, random assignment, and collection of data were conducted online from August 2018 through November 2018. Data collection occurred at three time points: baseline, 30 days post-baseline, and 60 days post-baseline. Eligibility criteria were (a) ability to access the online intervention, (b) living in the USA, (c) 18 years old ≤ age ≤ 64 years old, (d) BMI ≥ 25.00 kg/m2, and (e) absence of simultaneous enrollment in another intervention program promoting either well-being or physical activity. Participants were recruited through the general population panel of the SurveyHealth (http://www.surveyhealthcare.com/) recruitment company.
Random assignment of each eligible participant occurred after a unique and secure login credential was created, informed consent was obtained, a medical disclaimer was agreed to, and the baseline survey battery was completed. Eligible participants were randomly assigned to the intervention (i.e., FFW) or the usual care (i.e., UC) group via a software code that was written to accomplish equal allocations to the FFW and UC groups. Participants assigned to the FFW group were given immediate 24-h access to the 152 BET I CAN challenges for 30 days (i.e., from baseline to 30 days post-baseline). Participants assigned to the UC group were asked to conduct their lives as usual and were put on a waitlist for access to the intervention.
Survey Battery
Instruments designed to measure demographic information, well-being self-efficacy, and subjective well-being were included in the survey battery. Proposed demographic covariates of subjective well-being were collected via self-report at baseline and included participant gender, race/ethnicity, highest level of education completed, marital status, employment status, age, and household annual income (Rubenstein et al., 2016). This set of demographic variables is collectively referred to as the demographic covariates from this point forward.
Subjective well-being was measured at each time point with the established I COPPE Scale (Prilleltensky et al., 2015). Each of the seven dimensions of subjective well-being purported to be assessed by the I COPPE Scale — interpersonal, community, occupational, physical, psychological, economic, and overall — was measured with an exclusive item stem that referenced three unique periods of time: past (i.e., 30 days ago), present (i.e., right now), and future (i.e., 30 days from now). Responses to each item were organized within an eleven-category rating scale structure that ranged from 0 (worst your life can be) to 10 (best your life can be). Internal consistency for subjective well-being scores ranged from 0.86 (interpersonal) to 0.92 (occupational) at baseline and from 0.76 (economic) to 0.89 (occupational) at 60 days post-baseline. An average score for each dimension of subjective well-being was computed based on relevant scoring guidelines (Myers et al., 2014).
Well-being self-efficacy was measured at each time point with the recently developed well-being self-efficacy (WBSE) Scale (Myers et al., 2021). The WBSE Scale was designed to be concordant with subjective well-being as conceptualized in the FFW context. Specifically, the seven dimensions of well-being self-efficacy purported to be measured by the WBSE Scale — interpersonal, community, occupational, physical, psychological, economic, and overall — match the seven dimensions of subjective well-being measured by the I COPPE Scale (Myers et al., 2019). Each of the seven dimensions of well-being self-efficacy purported to be measured by the WBSE Scale has an exclusive item stem that referenced three unique periods of time: past (i.e., 30 days ago), present (i.e., right now), and future (i.e., 30 days from now). Responses to each item were organized within a five-category rating scale structure: 0 = no, 1 = low, 2 = moderate, 3 = high, and 4 = complete confidence. Evidence for the validity and the reliability of scores derived from responses to the WBSE Scale has been provided in the WBPA study (Myers et al., 2021). Internal consistency for scores derived from the WBSE scale ranged from 0.79 (physical) to 0.85 (interpersonal) at baseline and from 0.76 (physical) to 0.84 (occupational) at 30 days post-baseline. An average score for each dimension of well-being self-efficacy was computed based on relevant scoring guidelines (Bandura, 2006).
Data Analytic Approach
Seven statistical models were fit in Mplus 8.4 with maximum-likelihood (ML) estimation with robust standard errors (Muthén & Muthén, 1998–2017). Specifically, a saturated (df = 0) model was fit for each of the seven concordant pairs of dimensions of well-being self-efficacy and subjective well-being (e.g., interpersonal) depicted in Fig. 1. In each model, there were two continuous observed outcome variables: well-being self-efficacy at 30 days post-baseline and subjective well-being at 60 days post-baseline. Well-being self-efficacy at 30 days post-baseline was regressed on demographic covariates, subjective well-being at baseline, FFW (i.e., 0 = UC, 1 = FFW), well-being self-efficacy at baseline, and FFW × well-being self-efficacy at baseline. Subjective well-being at 60 days post-baseline was regressed on demographic covariates, subjective well-being at baseline, well-being self-efficacy at 30 days post-baseline, FFW, well-being self-efficacy at baseline, and FFW × well-being self-efficacy at baseline. Missing data were addressed with full information ML estimation using the observed information matrix under the assumption of missing at random (Schafer & Graham, 2002).
We considered results from two statistical approaches to evaluate Research Question 1: if well-being self-efficacy at baseline moderated the direct effect of FFW on well-being self-efficacy at 30 days post-baseline (i.e., the “a path” in Fig. 1). First, we evaluated the statistical significance of the “a path” moderated by well-being self-efficacy at baseline (i.e., β1). This approach focused on the statistical significance of the interaction term (i.e., the difference in the magnitude of the effect across levels of the moderator). Second, we used the Johnson and Neyman (1936) technique to probe for a region of significance for the estimate of the “a path” across the range of observed values of well-being self-efficacy at baseline (Preacher et al., 2006). This approach focused on whether the 95% CI for the effect included 0.00 across the range of values of the moderator via the plot produced by an online utility provided by Preacher et al. (2006).
We considered results from one statistical approach to evaluate Research Question 2: if well-being self-efficacy at baseline moderated the indirect effect of FFW on subjective well-being at 60 days post-baseline through well-being self-efficacy at 30 days post-baseline (i.e., the “a path” × “b path” in Fig. 1). Specifically, we used only the J-N technique to probe for a region of significance for the estimate of this indirect effect (i.e., β2) across the range of observed values of well-being self-efficacy at baseline. We used only this approach because the estimate of β2 and its 95% CI varied across levels of the moderator variable (MacKinnon, 2008). The online utility provided by Preacher et al. (2006) does not currently produce plots for conditional indirect effects so the relevant plot provided by Mplus was used instead.
We considered results from two statistical approaches to evaluate Research Question 3: if well-being self-efficacy at baseline moderated the direct effect of FFW on subjective well-being at 60 days post-baseline (i.e., the “c’ path” in Fig. 1). First, we evaluated the statistical significance of the “c’ path” moderated by well-being self-efficacy at baseline (i.e., β3). Second, we used the J-N technique to probe for a region of significance for the estimate of the “c’ path” across the range of observed values of well-being self-efficacy at baseline via the plot produced by an online utility provided by Preacher et al. (2006).
Type I Error
The probability of falsely rejecting a true null hypothesis (i.e., α) was set to equal 0.05. This approach was consistent with a majority of RCTs with multiple outcomes, where a downward adjustment to α generally has not been applied to maximize statistical power (and minimize type II error) in the event that a null hypothesis is truly false (Vickerstaff et al., 2015). To address, however, a reasonable concern with the possibility of an inflated α, in the event that a null hypothesis is truly true, we note that caution should be exercised with regard to observed statistical significance of a focal parameter until confirmatory studies become available.
Results
Readers are referred to Myers et al. (2021) for a figure depicting participant flow from screening to randomization to retention over the three measurement occasions for the subjective well-being data. In summary, 667 participants (nFFW = 331, nUC = 336) provided subjective well-being data at baseline; 548 participants (nFFW = 249, nUC = 299) provided subjective well-being data at 30 days post-baseline; and 570 participants (nFFW = 267, nUC = 303) provided subjective well-being data at 60 days post-baseline. A majority of the participants identified as female (67.2%), White, non-Hispanic (74.1%), having completed at least a 4-year college degree (60.1%), married (65.2%), a full-time employee (62.6%), at least 40-years old (55.6%), and as residing in a household with an annual income of at least $70,000 (51.6%). There were no statistically significant differences in the observed proportions of demographic characteristics or the mean well-being self-efficacy scores or the mean subjective well-being scores at baseline by randomization group. A majority (81.9%) of the participants who were assigned to the FFW group were classified as engaged with the FFW intervention. Univariate descriptive statistics for well-being self-efficacy and subjective well-being scores at baseline by I COPPE dimension are available in Table 1s of the supplementary material.
Path Model
There was evidence of a considerable amount of variance accounted for in both well-being self-efficacy at 30 days post-baseline (i.e., R2 ranged from 32.9% for physical to 51.4% for occupational) and subjective well-being at 60 days post-baseline (i.e., R2 ranged from 41.3% for psychological to 51.1% for economic). Table 1 provides the unstandardized estimate of key parameters from the path model. The paragraphs below briefly interpret key estimates regarding the new research questions under a BTM approach. Estimates of covariates at 30 days post-baseline and 60 days post-baseline for each concordant pair of dimensions of well-being self-efficacy and subjective well-being are available in Table 2s of the supplementary material.
Mixed results were observed for Research Question 1. For five of the seven dimensions (i.e., interpersonal, community, physical, economic, and overall), well-being self-efficacy at baseline did not moderate the direct effect of FFW on well-being self-efficacy at 30 days post-baseline per the interaction term approach. Furthermore, for each of these five dimensions, the 95% CI for the direct effect of FFW on well-being self-efficacy at 30 days post-baseline included 0.00 across the entire range of observed values of well-being self-efficacy at baseline. For the two remaining dimensions, however, there was some evidence that well-being self-efficacy at baseline moderated the direct effect of FFW on well-being self-efficacy at 30 days post-baseline as per the interaction term approach: occupational, \({\widehat{\beta }}_{1}\) = −0.13, p = 0.061, and psychological, \({\widehat{\beta }}_{1}\) = 0.17, p = 0.017. Furthermore, for both of these dimensions, the 95% CI for the direct effect of FFW on well-being self-efficacy at 30 days post-baseline did not include 0.00 across the lower range of observed values of well-being self-efficacy at baseline. The region of significance for the direct effect of FFW on occupational well-being self-efficacy at 30 days post-baseline ranged from observed values of −2.38 to 0.27 (see top panel in Fig. 2). More specifically, the decreasingly positive “a path” estimate (i.e.,\({\widehat{\beta }}_{\mathrm{a} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\)) was strongest at the lowest observed value of occupational well-being self-efficacy at baseline, −2.38, where \({\widehat{\beta }}_{\mathrm{a} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\)= 0.48, and remained statistically significant through a value of 0.27 (i.e., just beyond the M) on occupational well-being self-efficacy at baseline, where \({\widehat{\beta }}_{\mathrm{a} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\) = 0.14. Similarly, the region of statistical significance for the direct effect of FFW on psychological well-being self-efficacy at 30 days post-baseline ranged from observed values of −2.44 to −0.06 (see bottom panel in Fig. 2). More precisely, the decreasingly positive “a path” estimate (i.e.,\({\widehat{\beta }}_{\mathrm{a} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\)) was strongest at the lowest observed value of psychological well-being self-efficacy at baseline, −2.44, where \({\widehat{\beta }}_{\mathrm{a} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\) = 0.53, and remained statistically significant through a value of −0.06 (i.e., just prior to the M) on psychological well-being self-efficacy at baseline, where \({\widehat{\beta }}_{\mathrm{a} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\) = 0.12.

Direct effect of the Fun For Wellness (FFW) intervention on occupational and psychological well-being self-efficacy (WBSE) at 30 days post-baseline across the range of observed values of occupational and psychological WBSE at baseline. Note. In each figure: (a) the band around the direct effect represents the 95% confidence interval and (b) the dashed vertical line demarcates regions of (non-)significance
Mixed results were observed for Research Question 2. For five dimensions — interpersonal, community, physical, economic, and overall — the 95% CI for the indirect effect of FFW on subjective well-being at 60 days post-baseline through well-being self-efficacy at 30 days post-baseline included 0.00 across the entire range of observed values of well-being self-efficacy at baseline. For the two remaining dimensions, however, the 95% CI for the indirect effect of FFW on subjective well-being at 60 days post-baseline through well-being self-efficacy at 30 days post-baseline did not include 0.00 across the lower range of observed values of well-being self-efficacy at baseline. The region of significance for the indirect effect of FFW on occupational subjective well-being at 60 days post-baseline through occupational well-being self-efficacy at 30 days post-baseline ranged from −2.38 to 0.16 (see top panel in Fig. 3). More specifically, the decreasingly positive “a path” × “b path” estimate (i.e., \({\widehat{\beta }}_{\mathrm{a} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\times {\widehat{\beta }}_{\mathrm{b} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\)) was strongest at the lowest observed value of occupational well-being self-efficacy at baseline, −2.38, where \({\widehat{\beta }}_{\mathrm{a} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\times {\widehat{\beta }}_{\mathrm{b} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\) = 0.25, and remained statistically significant through a value of 0.16 (i.e., just beyond the M) on occupational well-being self-efficacy at baseline, where \({\widehat{\beta }}_{\mathrm{a} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\times {\widehat{\beta }}_{\mathrm{b} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\) = 0.08. Similarly, the region of significance for the indirect effect of FFW on psychological subjective well-being at 60 days post-baseline through psychological well-being self-efficacy at 30 days post-baseline ranged from −2.44 to −0.12 (see bottom panel in Fig. 3). More exactly, the decreasingly positive “a path” × “b path” estimate (i.e., \({\widehat{\beta }}_{\mathrm{a} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\times {\widehat{\beta }}_{\mathrm{b} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\)) was strongest at the lowest observed value of psychological well-being self-efficacy at baseline, −2.44, where \({\widehat{\beta }}_{\mathrm{a} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\times {\widehat{\beta }}_{\mathrm{b} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\) = 0.32, and remained statistically significant through a value of −0.12 (i.e., just prior to the M) on psychological well-being self-efficacy at baseline, where \({\widehat{\beta }}_{\mathrm{a} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\times {\widehat{\beta }}_{\mathrm{b} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\) = 0.08.

Indirect effect of the Fun For Wellness (FFW) intervention on occupational and psychological subjective well-being (SWB) at 60 days post-baseline through occupational and psychological well-being self-efficacy (WBSE) at 30 days post-baseline moderated by occupational and psychological WBSE at baseline. Note. In each figure: (a) the band around the indirect effect represents the 95% confidence interval and (b) the thick dashed vertical line demarcates regions of (non-)significance
Mixed results were observed for Research Question 3. For all seven dimensions, well-being self-efficacy at baseline did not moderate the direct effect of FFW on subjective well-being at 60 days post-baseline per the interaction term approach. Furthermore, for four of these dimensions — interpersonal, psychological, economic, and overall — the 95% CI for the direct effect of FFW on subjective well-being at 60 days post-baseline included 0.00 across the entire range of observed values of well-being self-efficacy at baseline. For the remaining three dimensions, however, the 95% CI for the direct effect of FFW on subjective well-being at 60 days post-baseline did not include 0.00 across part of the range of observed values of well-being self-efficacy at baseline. The region of significance for the direct effect of FFW on community subjective well-being at 60 days post-baseline ranged from observed values of −0.72 to 1.28 (see top panel in Fig. 4). More specifically, the increasingly positive “c’ path” estimate (i.e.,\({\widehat{\beta }}_{\mathrm{c} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\)) began to be statistically significant at an observed value of community well-being self-efficacy at baseline of −0.72 (i.e., 0.71 of a SD below the M), where \(\hat{\beta }_{{{\text{c path}}}}\) = 0.31, and remained statistically significant through a value of 1.28 (i.e., 1.27 of a SD above the M) on community well-being self-efficacy at baseline, where \({\widehat{\beta }}_{\mathrm{c} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\) = 0.39. The region of significance for the direct effect of FFW on occupational subjective well-being at 60 days post-baseline ranged from observed values of 0.44 to 0.94 (see middle panel in Fig. 4). More precisely, the increasingly positive “c’ path” estimate (i.e.,\({\widehat{\beta }}_{\mathrm{c} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\)) began to be statistically significant at an observed value of occupational well-being self-efficacy at baseline of 0.44 (i.e., 0.40 of a SD above the M), where \({\widehat{\beta }}_{\mathrm{c} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\) = 0.26, and remained statistically significant through a value of 0.94 (i.e., 0.85 of a SD above the M) on occupational well-being self-efficacy at baseline, where \({\widehat{\beta }}_{\mathrm{c} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\) = 0.34. The region of significance for the direct effect of FFW on physical subjective well-being at 60 days post-baseline ranged from observed values of 0.11 to 1.16 (see bottom panel in Fig. 4). More exactly, the increasingly positive “c’ path” estimate (i.e.,\(\hat{\beta }_{{{\text{c path}}}}\)) began to be statistically significant at an observed value of physical well-being self-efficacy at baseline of 0.11 (i.e., 0.12 of a SD above the M), where \({\widehat{\beta }}_{\mathrm{c} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\) = 0.22, and remained statistically significant through a value of 1.16 (i.e., 1.20 of a SD above the M) on physical well-being self-efficacy at baseline, where \({\widehat{\beta }}_{\mathrm{c} \mathrm{p}\mathrm{a}\mathrm{t}\mathrm{h}}\) = 0.39.

Direct effect of the Fun For Wellness (FFW) intervention on community, occupational, and physical subjective well-being (SWB) at 60 days post-baseline across the range of observed values of community, occupational, and physical well-being self-efficacy (WBSE) at baseline. Note. In each figure: (a) the band around the direct effect represents the 95% confidence interval and (b) the dashed vertical lines demarcate regions of (non-)significance
Discussion
The objective of this study was to use BTM to assess variation in the impact of the FFW intervention on I COPPE dimensions of subjective well-being in adults with obesity. In general, the results from the current study provide both supportive and unsupportive evidence regarding this objective. Specific findings with respect to the three new research questions tested under a BTM approach within the FFW conceptual model for the promotion of subjective well-being (see dashed lines in Fig. 1) followed three distinct patterns. These patterns are discussed below with respect to (a) results from the WBPA study under a non-BTM approach (Myers et al., 2021) and (b) potential impact on the design of future FFW trials.
The first pattern is uniform evidence against variation in the impact of the FFW intervention on subjective well-being by baseline well-being self-efficacy. Three of the seven I COPPE dimensions followed this pattern: interpersonal, economic, and overall. For these dimensions, well-being self-efficacy at baseline did not moderate the direct effect of FFW on well-being self-efficacy at 30 days post-baseline (i.e., the “a path”), the indirect effect of FFW on subjective well-being at 60 days post-baseline through well-being self-efficacy at 30 days post-baseline (i.e., the “a path” × “b path”), nor the direct effect of FFW on subjective well-being at 60 days post-baseline (i.e., the “c’ path”). Moreover, the estimate for each of these effects also was statistically non-significant under a non-BTM approach for each of these dimensions (Myers et al., 2021). Future design of FFW trials may consider invoking the continual optimization principle within the multiphase optimization framework (MOST; Collins & Kugler, 2018) by returning to the preparation phase for the purpose of further tailoring BET I CAN challenges for adults with obesity regarding promoting subjective well-being in these dimensions. Taking this approach would be consistent with a recommendation for tailoring multicomponent behavioral interventions for this unique and at-risk population (United States Preventive Services Task Force, 2018).
The second pattern is evidence for variation in only the direct effect of the FFW intervention on subjective well-being at 60 days post-baseline (i.e., the “c’ path”) by baseline well-being self-efficacy. Two of the seven I COPPE dimensions followed this pattern: community and physical. Interestingly, the estimate for the “c’ path” also was statistically significant under a non-BTM approach for both of these dimensions (Myers et al., 2021). What the BTM approach suggests, however, is that there may be specific subgroups of adults with obesity for whom the FFW intervention most effectively directly promotes community and/or physical subjective well-being. The specific subgroup of adults with obesity for whom FFW most effectively directly promoted community subjective well-being in the WBPA study were those reporting “low” through “high” levels of community well-being self-efficacy at baseline (i.e., 66.6% of participants). More simply, this finding suggests a “lower middle to upper middle strata” effect. Similarly, the specific subgroup of adults with obesity for whom FFW most effectively directly promoted physical subjective well-being in the WBPA study were those reporting “moderate” through “high” levels of physical well-being self-efficacy at baseline (i.e., 28.6% of participants). Simply put, this finding suggests a “middle to upper middle strata” effect. Recognizing that in both cases this moderated “c’ path” was capturing all causal paths between intervention and outcome aside from the specified statistically insignificant indirect effect on well-being self-efficacy, future research could seek to identify alternate mechanisms through which FFW is influencing subjective well-being. The identification of an alternate mechanism that underlies the observed direct effect could allow for alterations to the FFW intervention that target this mechanism for community and physical subjective well-being.
The third pattern is evidence for variation in both the direct effect of FFW on well-being self-efficacy at 30 days post-baseline (i.e., the “a path”) and the indirect effect of FFW on subjective well-being at 60 days post-baseline through well-being self-efficacy at 30 days post-baseline (i.e., the “a path” × “b path”) by baseline well-being self-efficacy. Two of the seven I COPPE dimensions followed this pattern: occupational and psychological. Interestingly, the estimate for both the “a path” and the “a path” × “b path” also was statistically significant under a non-BTM approach for both of these dimensions (Myers et al., 2021). What the BTM approach adds, however, is evidence that there may be a specific subgroup of adults with obesity for whom the FFW intervention most effectively indirectly promotes occupational and psychological subjective well-being through improvements in occupational and psychological well-being self-efficacy. The specific subgroup of adults with obesity for whom FFW most effectively indirectly promoted occupational subjective well-being at 60 days (through occupational well-being self-efficacy at 30 days) were those reporting “no” through “moderate” levels of occupational well-being self-efficacy at baseline (i.e., 54.7% of participants). Similarly, the specific subgroup of adults with obesity for whom FFW most effectively indirectly promoted psychological subjective well-being at 60 days (through psychological well-being self-efficacy at 30 days) were those reporting “no” through “moderate” levels of psychological well-being self-efficacy at baseline (i.e., 43% of participants). Both of these findings suggest a “compensatory” effect. That is, the subgroup of individuals who entered the WBPA study with low to moderate levels of occupational and psychological well-being self-efficacy had stronger FFW intervention effects on the mediator, and through the indirect effect, the outcome. Next generation FFW trials targeting these outcomes may consider using occupational and/or psychological well-being self-efficacy level as potential selection criteria for participant enrollment. This type of adaptation would align with “personalized prevention” that better targets intervention components to an individual’s specific pre-existing risk factors (e.g., August & Gewirtz, 2019; Collins et al., 2004). Furthermore, future research designed to yield better understanding of why some FFW effects may be “compensatory” (e.g., benefiting those with low baseline well-being self-efficacy) versus “rich get richer” (e.g., boosting those with more than low baseline well-being self-efficacy) is needed.
References
American Psychological Association. (2020). Publication manual of the American Psychological Association (7th ed.). American Psychological Association.
August, G. J., & Gewirtz, A. (2019). Moving toward a precision-based, personalized framework for prevention science: Introduction to the special issue. Prevention Science, 20, 1–9. https://doi.org/10.1007/s11121-018-0955-9
Bandura, A. (1997). Self-efficacy: The exercise of control. Freeman.
Bandura, A. (2006). Guide for constructing self-efficacy scales. In F. Pajares & T. C. Urdan (Eds.), Self-efficacy beliefs of adolescents (pp. 307–337). Information Age Publishing.
Beauchamp, M. R., Crawford, K. L., & Jackson, B. (2019). Social cognitive theory and physical activity: Mechanisms of behavior change, critique, and legacy. Psychology of Sport and Exercise, 42, 110–117. https://doi.org/10.1016/j.psychsport.2018.11.009
Collins, L. M., & Kugler, K. C. (2018). Optimization of behavioral, biobehavioral, and biomedical interventions: The multiphase optimization strategy (MOST). Springer.
Collins, L. M., Murphy, S. A., & Bierman, K. L. (2004). A conceptual framework for adaptive prevention interventions. Prevention Science, 5, 185–196. https://doi.org/10.1023/b:prev.0000037641.26017.00
Gourlan, M. J., Trouilloud, D. O., & Sarrazin, P. G. (2011). Interventions promoting physical activity among obese populations: A meta-analysis considering global effect, long-term maintenance, physical activity indicators and dose characteristics. Obesity Reviews, 12, e633–e645. https://doi.org/10.1111/j.1467-789X.2011.00874.x
Howe, G., & Leijten, P. (2020). When is it time to revise or adapt our prevention programs? Using baseline target moderation to assess variation in prevention impact. Manuscript in preparation.
Johnson, P. O., & Neyman, J. (1936). Tests of certain linear hypotheses and their applications to some educational problems. Statistical Research Memoirs, 1, 71–95.
Lee, S., McMahon, A., Prilleltensky, I., Myers, N. D., Dietz, S., Prilleltensky, O., Pfeiffer, K. A., Bateman, A. G., & Brincks, A. M. (2021). Effectiveness of the fun for wellness online behavioral intervention to promote well-being actions in adults with obesity: A randomized controlled trial. Journal of Sport & Exercise Psychology, 43, 83–96. https://doi.org/10.1123/jsep.2020-0049
MacKinnon, D. (2008). Introduction to statistical mediation analysis. Lawrence Erlbaum Associates.
Mihelic, M., Filus, A., & Morawaska, A. (2016). Correlates of prenatal parenting expectations in new mothers: Is self-efficacy a potential target for preventing postnatal adjustment difficulties? Prevention Science, 17, 949–959. https://doi.org/10.1007/s11121-016-0682-z
Muthén, L. K., & Muthén, B. O. (1998–2017). Mplus User’s Guide (8th ed.). Los Angeles, CA: Muthén & Muthén.
Myers, N. D., McMahon, A., Prilleltensky, I., Lee, S., Dietz, S., Prilleltensky, O., & Brincks, A. M. (2020). Effectiveness of the fun for wellness online behavioral intervention to promote physical activity in adults with obesity: A randomized controlled trial. Journal of Medical Internet Research Formative Research, 4, e15919. https://doi.org/10.2196/15919
Myers, N. D., Prilleltensky, I., Hill, C. R., & Feltz, D. L. (2017a). Well-being self-efficacy and complier average causal effect modeling: A substantive-methodological synergy. Psychology of Sport & Exercise, 30, 135–144. https://doi.org/10.1016/j.psychsport.2017.02.010
Myers, N. D., Prilleltensky, I., Jin, Y., Dietz, S., Rubenstein, C. L., Prilleltensky, O., & McMahon, A. (2014). Empirical contributions of the past in assessing multidimensional well-being. Journal of Community Psychology, 42, 789–798. https://doi.org/10.1002/jcop.21653
Myers, N. D., Prilleltensky, I., Lee, S., Dietz, S., Prilleltensky, O., McMahon, A., & Brincks, A. M. (2019). Effectiveness of the fun for wellness online behavioral intervention to promote well-being and physical activity: Protocol for a randomized controlled trial. BMC Public Health, 19, 737. https://doi.org/10.1186/s12889-019-7089-2
Myers, N. D., Prilleltensky, I., McMahon, A., Lee, S., Dietz, S., Prilleltensky, O., Pfeiffer, K. A., Bateman, A. G., & Brincks, A. M. (2021). Effectiveness of the fun for wellness online behavioral intervention to promote subjective well-being in adults with obesity: A randomized controlled trial. Journal of Happiness Studies, 22, 1905–1923. https://doi.org/10.1007/s10902-020-00301-0
Myers, N. D., Prilleltensky, I., Prilleltensky, O., McMahon, A., Dietz, S., & Rubenstein, C. L. (2017b). Efficacy of the fun for wellness online intervention to promote multidimensional well-being: A randomized controlled trial. Prevention Science, 18, 984–994. https://doi.org/10.1007/s11121-017-0779-z
Preacher, K. J., Curran, P. J., & Bauer, D. J. (2006). Computational tools for probing interactions in multiple linear regression, multilevel modeling, and latent curve analysis. Journal of Educational and Behavioral Statistics, 31, 437–448. https://doi.org/10.3102/10769986031004437
Prilleltensky, I., Dietz, S., Prilleltensky, O., Myers, N. D., Rubenstein, C. L., Jin, Y., & McMahon, A. (2015). Assessing multidimensional well-being: Development and validation of the I COPPE scale. Journal of Community Psychology, 43, 199–226. https://doi.org/10.1002/jcop.21674
Rubenstein, C. L., Duff, J., Prilleltensky, I., Jin, Y., Dietz, S., Myers, N. D., & Prilleltensky, O. (2016). Demographic group differences in domain-specific well-being. Journal of Community Psychology, 44, 499–515. https://doi.org/10.1002/jcop.21784
Schafer, J. L., & Graham, J. W. (2002). Missing data: Our view of the state of the art. Psychological Methods, 7, 147–177. https://doi.org/10.1037/1082-989X.7.2.147
Tudor-Locke, C., Brashear, M. M., Johnson, W. D., & Katzmarzyk, P. T. (2010). Accelerometer profiles of physical activity and inactivity in normal weight, overweight, and obese U.S. men and women. International Journal of Behavioral Nutrition and Physical Activity, 7, 60. https://doi.org/10.1186/1479-5868-7-60
United States Department of Health and Human Services. (2013). Managing overweight and obesity in adults: Systematic evidence review from the obesity expert panel. Retrieved from https://www.nhlbi.nih.gov/sites/default/files/media/docs/obesity-evidence-review.pdf
United States Preventive Services Task Force. (2018). Behavioral weight loss interventions to prevent obesity-related morbidity and mortality in adults: United States preventive services task force recommendations. Journal of the American Medical Association, 320, 1163–1171. https://doi.org/10.1001/jama.2018.13022
Vickerstaff, V., Ambler, G., King, M., Nazareth, I., & Omar, R. Z. (2015). Are multiple primary outcomes analysed appropriately in randomised controlled trials? A review. Contemporary Clinical Trials, 45, 8–12. https://doi.org/10.1016/j.cct.2015.07.016
World Health Organization. (2018). Obesity and overweight fact sheet. Retrieved from https://www.who.int/mediacentre/factsheets/fs311/en/
Funding
Funding for the study was provided by both the Erwin and Barbara Mautner Charitable Foundation through the Erwin and Barbara Mautner Endowed Chair in Community Well-Being at the University of Miami (Isaac Prilleltensky) and the National Institute on Drug Abuse (NIDA) grant # K01 DA046516 (Ahnalee Brincks, Principal Investigator).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
All procedures in the study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The institutional review board at the University of Miami provided necessary permission (IRB# 20,170,541) to conduct the WBPA study on July 11, 2017. The University of Miami and Michigan State University (STUDY00000979) established an Institutional Authorization Agreement on June 26, 2018 that provided permission for the University of Miami to serve as the designated IRB for the study.
Informed Consent
Informed consent was obtained from each participant included in the study. More specifically, immediately after being determined to be eligible for this study, each eligible individual was directed to a web-based IRB-approved informed consent form. Each individual who clicked “Consent to Participate” was enrolled as a participant in the study. Each individual who clicked “Decline to Consent” was denied access to the intervention.
Disclaimer
We do not perceive either funding body to exert any role in the design of the study and collection, analysis, and interpretation of data and in writing manuscripts.
Conflict of Interest
Two co-authors, Adam McMahon and Isaac Prilleltensky, are partners in Wellnuts LLC. Wellnuts LLC may commercialize the FFW intervention in the future.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Myers, N.D., Prilleltensky, I., McMahon, A. et al. Mechanisms by Which the Fun for Wellness Intervention May Promote Subjective Well-Being in Adults with Obesity: a Reanalysis Using Baseline Target Moderation. Prev Sci 24, 286–298 (2023). https://doi.org/10.1007/s11121-021-01274-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11121-021-01274-z