
Abstract
This study (a) examined changes in marijuana and cigarette initiation sequencing and (b) considered implications of such changes for prevention efforts by examining associations between initiation sequencing and current adolescent substance use. Analyses used 2000–2019 cross-sectional data from the national Monitoring the Future (MTF) study (78,252 U.S. 12th grade students). Models examined trends in six distinct patterns of initiation order, and multivariable associations between order of initiation and 30-day cigarette and marijuana use prevalence, cigarette and marijuana use frequency among users, and nicotine and marijuana vaping prevalence. While the percentage of students initiating neither cigarettes nor marijuana increased, increases also were observed in marijuana-only initiation (the fastest-growing pattern) and initiation of marijuana before cigarettes; these increases were accompanied by a significant decrease in cigarette-only initiation. Cigarette use prevalence and frequency were highest among students initiating cigarettes before marijuana; marijuana use prevalence and frequency were highest among students initiating marijuana before cigarettes. Cigarette and marijuana prevalence, as well as marijuana frequency, were lowest among students initiating only a single substance. Nicotine vaping was less prevalent among students initiating a single substance versus both substances, but no significant differences were observed in nicotine vaping prevalence between those initiating only cigarettes versus only marijuana. Implications of these findings for prevention efforts are discussed in the frameworks of both the common liability model and route of administration model.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Adolescent cigarette and marijuana use are associated with a range of negative outcomes (American College of Pediatricians 2018; U.S. Department of Health and Human Services 2012). Several theoretical models have been developed to explain if and how the order in which adolescents initiate substance use may have implications for prevention effort focus and timing, e.g., the gateway, common liability, and route of administration models. The gateway model (Kandel and Kandel 2015) posits that initiation order is important because tobacco use—particularly cigarette use—is causal of later marijuana use. The gateway model indicates prevention efforts should focus strongly on tobacco at early ages in order to prevent later marijuana uptake. The common liability model (van Leeuwen et al. 2011; Vanyukov et al. 2012) posits that cigarette and marijuana use both arise from common biological and social liability factors associated with substance use in general. The common liability model suggests prevention efforts should focus on delaying/preventing initiation of both behaviors from early childhood onwards, given that adolescents who use one substance may be likely to initiate the other given adequate consumption opportunities. The route of administration model (Agrawal and Lynskey 2009) hypothesizes the shared administration route of inhalation connects cigarette and marijuana use. Thus, prevention efforts might focus on preventing early inhalation behaviors (i.e., considering a combined risk group who smoke combustible tobacco or marijuana, or report any vaping behaviors) versus focusing on preventing cigarette or marijuana use initiation separately without regard to administration method.
Until recently, cigarette and marijuana initiation order appeared relatively stable across time. International data generally have been consistent in finding adolescents initiate cigarette use prior to marijuana use (Baumeister and Tossmann 2005; Degenhardt et al. 2008; Leatherdale et al. 2008). Yet, recent research indicates cigarette initiation age has increased among U.S. youth (Cantrell et al. 2018; Keyes et al. 2019) while marijuana initiation age has remained stable (Keyes et al. 2019). Changes in initiation order may be associated with public acceptance decreasing for cigarettes while increasing for marijuana as reflected in changing policy and perceived risk (Bretteville-Jensen and Williams 2011; Fairman et al. 2019; McBride et al. 2016; Miech et al. 2020; Wen et al. 2019). Cigarette and marijuana initiation order change also may be associated with modern vaping technology. A growing number of adolescents initiate nicotine vaping before cigarette smoking (Evans-Polce et al. 2020). Marijuana initiation likelihood may be increasing due to perceptions that vaping (versus smoking) cannabis is safer and allows use in more locations (Budney et al. 2015). Patterns of cigarette and marijuana initiation order include initiating (1) neither, (2) cigarettes only, (3) marijuana only, (4) cigarettes before marijuana, (5) cigarettes and marijuana at the same time, or (6) marijuana before cigarettes. Among adolescents who have initiated both, the likelihood of initiating marijuana prior to cigarettes is growing (Fairman et al. 2019; Keyes et al. 2019; Livingston et al. 2020). Little data are available that examine the degree to which changes over time are occurring in initiating cigarettes only or marijuana only, or initiating both substances at the same time.
Based on gateway, common liability, and/or route of administration models, initiation order change impacts later adolescent cigarette, nicotine vaping, and marijuana use. According to the gateway model, the observed decreases in cigarette initiation (Cantrell et al. 2018; Keyes et al. 2019) should lead to decreasing adolescent cigarette and marijuana prevalence, but national data show decreased cigarette prevalence but stable marijuana prevalence (Miech et al. 2020). While not consistent with the gateway model, current trends are consistent with the common liability model as it does not hypothesize an a priori substance initiation sequence.
Based on the common liability model, cigarette and/or marijuana use prevalence likelihood may not vary based on changing percentages of adolescents initiating one substance prior to the other. Fairman et al. (2019) found initiating marijuana prior to other substances was associated with higher heavy marijuana use and use disorder, but nicotine dependence was not associated with marijuana and cigarette initiation order. Co-use of tobacco and marijuana is associated with increased dependence and withdrawal difficulty for both substances (Agrawal et al. 2012; Hindocha et al. 2015; Peters et al. 2012; Weinberger et al. 2018). Frequent marijuana use is associated with higher nicotine addiction among adolescents (Rubinstein et al. 2015), possibly due to connections between marijuana’s primary psychoactive component (THC) and later nicotine addiction (Panlilio et al. 2013). Marijuana’s associations with decreased motivation also may reduce motivation to quit smoking cigarettes (Humfleet and Hass 2004).
The route of administration model supports the possibility that changing cigarette and marijuana initiation patterns may affect vaping behaviors. Prospective research found significant bi-directional links between nicotine vaping and marijuana initiation (Ksinan et al. 2020). Overall nicotine vaping may be just as prevalent among adolescents who initiate marijuana only as among those who initiate cigarettes only due to common inhalation experience.
Examining associations (even at descriptive cross-sectional levels) between cigarette and marijuana initiation patterns and adolescent cigarette smoking, nicotine vaping, and marijuana use would be informative when considering the potential implications of initiation order change for prevention efforts. Analyses would need to consider the extent to which observed cross-sectional associations may be confounded by other measures. Research has identified key covariates that significantly correlate with, or act as moderators of, cigarette smoking and marijuana use initiation and/or current use. Such covariates include sex, race/ethnicity, parental education, individual education, and truancy (Evans-Polce et al. 2020; Fairman 2015; Green et al. 2016; Henry and Thornberry 2010; Kennedy et al. 2016; Miech et al. 2020; Vanyukov et al. 2012; Weinberger et al. 2018). Further, marijuana (or cigarette) initiation may lead to exposure to social mechanisms such as perceived norms and peer groups that then lead to cigarette use (or marijuana use) (Keyes et al. 2019). If so, controlling for factors such as perceived risk and friends’ substance use may help isolate independent associations between initiation order and current use. Analyses also should control for alcohol use (the other primary substance used by adolescents) and age of initiation (Reidpath et al. 2014; Richmond-Rakerd et al. 2017).
The current study used cross-sectional, nationally representative data from U.S. 12th grade students collected from 2000 to 2019 to examine (1) change in cigarette and marijuana initiation order, as well as (2) associations between initiation order patterns and past 30-day adolescent cigarette and marijuana use, and (in recent years) nicotine and marijuana vaping. Based on the common liability and route of administration models, as well as recent changes in policy and perceived risk, it was hypothesized that (a) growing percentages of adolescents would report initiation of marijuana only, or initiation of marijuana before cigarettes; (b) current cigarette and marijuana use likelihood each would be highest among students reporting initiating that substance before the other, and least likely among students initiating only that substance; and (c) vaping nicotine would be most likely among students initiating both cigarettes and marijuana, followed by those initiating only one or the other, followed by those initiating neither.
Methods
Participants and Procedure
Analyses used data from the Monitoring the Future (MTF) study; detailed methodology is available elsewhere (Bachman et al., 2015; Miech et al., 2020). MTF annually surveys nationally representative cross-sectional samples of 12th grade students in the coterminous U.S.A., resulting in approximately 15,000 students from 130 high schools surveyed per year. Informed consent was obtained; a University of Michigan Institutional Review Board approved the study. Surveys were administered in classrooms by University of Michigan personnel; students self-completed surveys during a normal class period. From 2000 to 2019, student response rates averaged 82%; absenteeism was the primary reason for nonresponse (Miech et al. 2020).
MTF uses six questionnaire forms (randomly distributed within classrooms); grade of first use items are asked on two forms yielding a random one third of the full sample. A total of 94,496 students responded to forms containing grade of first use questions from 2000 to 2019. Of the 94,496, 14,965 (15.8%) did not provide valid data for items on grade of first use of cigarettes and/or marijuana; an additional 863 (0.9%) were excluded due to reporting “grade 6 or below” for both substances, resulting in our inability to determine which was initiated first. An additional 416 cases (0.4%) were excluded due to missing outcome data (past 30-day cigarette use, marijuana use, nicotine vaping, and marijuana vaping), or inconsistencies between reported initiation history and past 30-day use. Thus, the analytic sample included 78,252 cases (82.8% of the 94,496 possible). Sensitivity analyses indicated retained (vs. total sample) cases were more likely to be female (vs. male), be white (vs. non-white), and report high parental education.
Measures
Independent Variables
Respondents were asked: “When (if ever) did you FIRST do each of the following things? …Smoke your first cigarette. …Try marijuana or hashish.” Answer categories were as follows: grade 6 or below, grade 7, grade 8, grade 9 (freshman), grade 10 (sophomore), grade 11 (junior), grade 12 (senior), and never. Order of initiation was coded as a multi-categorical variable indicating (1) initiating neither cigarette nor marijuana use (non-initiation); (2) cigarette-only initiation (i.e., did not initiate marijuana use); (3) marijuana-only initiation; (4) initiating cigarettes before marijuana (cigarette-first initiation); (5) initiating both cigarettes and marijuana in the same grade (same-grade initiation); and (6) initiating marijuana before cigarettes (marijuana-first initiation). To help provide context for changes over time in specific order of initiation patterns, two additional dichotomous indicators were coded indicating any cigarette initiation and any marijuana initiation.
Outcome Variables
Respondents were asked, “How frequently have you smoked cigarettes during the past 30 days?” (not at all, less than 1 cigarette per day, 1–5 cigarettes per day, about ½ pack per day, about 1 pack per day, about 1 ½ packs per day, 2+ packs per day). Two measures were coded for analysis: cigarette use prevalence (0,1) and cigarette frequency among smokers (coded as 0.5, 3, 10, 20, 30, 40, based on the response categories listed above). Marijuana use was measured using the item, “On how many occasions (if any) have you used hashish/marijuana during the last 30 days?” (0 occasions, 1–2, 3–5, 6–9, 10–19, 20–39, and 40 or more). Two dichotomous marijuana measures were coded for analysis: any marijuana use prevalence (0,1) and frequent marijuana use among users (0 = 1–19 occasions; 1 = 20+ occasions). Nicotine and marijuana vaping prevalence items (available only for 2017–2019, and on only one of the two relevant questionnaire forms) were asked as, “On how many occasions (if any) have you vaped [specified substance] during the last 30 days?” and coded into dichotomies of any/none.Footnote 1
Covariates
All covariates other than year were self-reported, and included grade smoked first cigarette, grade first tried marijuana, and grade first drank alcohol (before 9th grade, 9th–12th grade, not initiated); past 30-dayalcohol use frequency (0, 1.5, 4, 7.5, 14.5, 29, 40 occasions); perceived risk of smoking 1+ cigarette packs/day, perceived risk of using marijuana regularly, and (in the model examining current nicotine vaping) perceived risk of vaping nicotine regularly (great risk vs. no/slight/moderate risk; perceived risk of vaping marijuana is not asked); how many friends smoke cigarettes and how many friends use marijuana (most/all vs. none/a few/some); gender (male vs. female); race/ethnicity (African American/Black, Hispanic, White, or other including multi-racial); parental education (used as a proxy for socioeconomic status, indicating if any parent completed college vs. not); average high school grades (B− or above vs. C+ or below); truancy (any whole days of school missed due to skipping/cutting in the last 4 weeks vs. none); and year of survey (coded as centered linear and quadratic terms for time trend models, and as four dichotomous 5-year indicators for multivariable models).
Statistical Analysis
Descriptive statistics and prevalence/mean frequency estimates utilized SURVEYFREQ and SURVEYMEANS procedures in SAS v.9.4 (SAS Institute, Inc., Cary, NC), accounting for the complex sample design and employing weights to account for unequal probabilities of selection. To examine change over time in patterns of cigarette and marijuana initiation (research question [RQ] 1), SURVEYLOGISTIC models were run regressing dichotomous indicators for each pattern type on centered linear and quadratic year terms.
To examine associations between the various initiation patterns and substance use outcomes (RQ2), Mplus v.7.4 (Muthén and Muthén, Los Angeles, CA) was used to fit logistic regression models for prevalence outcomes and OLS regression models for cigarette frequency among smokers. Order of initiation was modeled using dummy indicators. For cigarette outcomes, the referent category was cigarette-first initiation; non-initiators and marijuana-only initiators were excluded. For nicotine vaping, the referent category again was cigarette-first initiation, but all other initiation categories were included. For marijuana outcomes, marijuana-first initiation was the referent category; non-initiators and cigarette-only initiators were excluded. All models were run simultaneously including initiation order; grade of first use of cigarettes, marijuana, and alcohol (using dichotomies of before 9th grade vs. other); alcohol use frequency; perceived risk of cigarettes and marijuana, friends’ use of cigarettes and marijuana, gender; race/ethnicity; parental education; high school grades; truancy; and year (using 5-year-group indicators; 2015–2019 was omitted as the referent category). For nicotine and marijuana vaping models, year was excluded because only 3 years of data (2017–2019) were available for these outcomes. Cigarette outcome models also included past 30-day marijuana use frequency (no use, non-frequent use, frequent use); marijuana outcome models included past 30-day cigarette use frequency; the nicotine vaping model included past 30-day cigarette and marijuana use frequency and perceived risk of vaping nicotine. All Mplus models accounted for the complex sample design (specifying TYPE = COMPLEX), included sampling weights, and used maximum likelihood estimation with robust standard errors and Monte Carlo integration. Missing data on covariates were addressed by using full-information maximum-likelihood estimation in Mplus (Muthén and Muthén 1998-2017).
Results
Sample Descriptives
Descriptive statistics are shown in Table 1. Among all students from 2000 to 2019, 16.7% reported any 30-day cigarette use; mean frequency among smokers was 5.1 cigarettes per day. Any 30-day marijuana use was reported by 18.9% of students; 26.4% of users reported frequent use. From 2017 to 2019, any 30-day nicotine vaping was reported by 17.7% of students; any 30-day marijuana vaping was reported by 18.0%.
Order of Initiation Trends
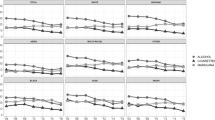
Table 2 provides the percentages of students reporting each pattern of cigarette and marijuana initiation over time; data are presented graphically in Fig. 1. All trends discussed below were significant at p < 0.01 or stronger. Any cigarette initiation decreased from 56.0% in 2000 to 18.2% in 2019; any marijuana initiation decreased from 44.1 to 37.3%. Among all respondents and averaging across years, 50.8% were non-initiators. Approximately one in five initiated only one of the two substances: 8.9% cigarette-only initiation and 13.0% marijuana-only initiation. Approximately one quarter of respondents initiated both substances: 14.4% cigarette-first initiation, 8.3% same-grade initiation, and 4.7% marijuana-first initiation.

Trends in order of cigarette and marijuana initiation of among U.S. 12th grade students, 2000–2019. Notes: n (unweighted) = 78,252, all 12th grade respondents; 21,406 among cigarette and marijuana initiates
The percentage of those not initiating either drug increased by more than half, from 38.6 to 59.2%. Cigarette-only initiation decreased by a factor of 5 (from 17.3 to 3.5%). As a percentage of all cigarette initiation, cigarette-only initiation decreased from 31% in 2000 (17.3/56.0) to 19% in 2019 (3.5/18.2). Marijuana-only initiation quadrupled (from 5.5 to 22.7%); as a percentage of all marijuana initiation, marijuana-only initiation increased from 12% in 2000 (5.5/44.1) to 61% (22.7/37.3) in 2019. There were significant decreases in cigarette-first initiation (down by almost a factor of 5 from 27.1 to 5.6%). For the remaining two patterns, non-linear changes were observed. Same-grade initiation increased from 8.9 to 10% in 2005, but then decreased, reaching 4.8% in 2019 (an overall decrease of approximately 50%). Marijuana-first initiation increased from 2.7 to 6.0% in 2013 and then decreased to approximately 4% in 2019 (an increase of roughly 50% overall).
Among the 27.4% of students who initiated both substances, 52.6% reported cigarette-first initiation, 30.3% same-grade initiation, and 17.1% marijuana-first initiation (Table 2, lower panel). Among initiates of both substances, cigarette-first initiation decreased by just under half (from 70.1 to 38.2%); same-grade initiation increased by approximately 40% (from 23.1 to 32.7%); and marijuana-first initiation more than quadrupled, rising from 6.9 to 29.0%.
Thus, over the 20 years examined, the strongest changes over time in initiation order for students overall occurred for cigarette-only, marijuana-only, and cigarette-first initiation. Among students initiating both substances, the strongest changes observed were for cigarette-first and marijuana-first initiation. In the regression models below, attention will be particularly focused on comparisons of these initiation patterns.
Associations Between Order of Initiation and Substance Use Outcomes
Table 3 presents prevalence or mean frequency estimates of all outcomes by initiation order, as well as multivariable regression estimates for the likelihood of each outcome based on initiation order. Supplement Tables 1–2 present full results including covariate associations.
Cigarette and Nicotine Vaping Outcomes
Cigarette Prevalence
Among cigarette-first initiators, 53.5% used cigarettes in the past 30 days. In comparison, cigarette prevalence was significantly lower among cigarette-only initiators (29.4%), same-grade initiators (48.5%), and marijuana-first initiators (47.2%). In additional models using cigarette-only initiation as the referent category (not shown), the likelihood of any cigarette use was significantly higher for both same-grade initiators (AOR 1.29 [95% CI 1.16, 1.43], p < 0.001) and marijuana-first initiators (AOR 1.22 [1.06, 1.39], p = 0.004).
Cigarette Frequency Among Smokers
Among cigarette users, mean daily cigarette frequency for cigarette-first initiators was 6.2/day, significantly higher than other initiation patterns: 3.5/day among cigarette-only initiators, 4.7/day among same-grade initiators, and 3.9/day among marijuana-first initiators. In additional models (not shown), no significant differences in cigarette frequency were observed between cigarette-only initiators and either same-grade (p = 0.412) or marijuana-first (p = 0.929) initiators.
Nicotine Vaping Prevalence
Thirty-day nicotine vaping was reported by 4.8% of non-initiators, 26.4% of marijuana-only initiators, 30.0% of cigarette-only initiators, 46.2% of marijuana-first initiators, 47.9% of same-grade initiators, and 51.2% of cigarette-first initiators. Nicotine vaping likelihood was significantly higher among cigarette-first initiators than non-initiators, cigarette-only initiators, marijuana-only initiators, and marijuana-first initiators. No significant differences in nicotine vaping were observed between cigarette-first initiators and same-grade initiators. In additional models (not shown), nicotine vaping likelihood was significantly lower among non-initiators than cigarette-only initiators (AOR 0.15 [0.09, 0.25], p < 0.001), but no significant differences were observed for cigarette-only initiators versus marijuana-only (p = 0.068), same-grade (p = 0.379), or marijuana-first (p = 0.937) initiators.
Marijuana Use Outcomes
Marijuana Use Prevalence
Past 30-day marijuana use was reported by 61.4% of marijuana-first initiators. All other initiation patterns reported significantly lower prevalence: 40.7% of marijuana-only initiators, 48.1% of cigarette-first initiators, and 48.4% of same-grade initiators. In additional models using marijuana-only initiators as the referent category (not shown), marijuana use likelihood was significantly higher among cigarette-first initiators (AOR 1.32 [1.19, 1.47], p < 0.001) and same-grade initiators (AOR 1.25 [1.14, 1.37], p < 0.001).
Frequent Use Among Marijuana Users
More than one third (35.9%) of past 30-day marijuana users reported frequent use among marijuana-first initiators, a significantly higher percentage than for other initiation patterns: 16.6% for marijuana-only initiators, 27.8% for cigarette-first initiators, and 29.8% for same-grade initiators. Compared to marijuana-only initiators, frequent use was significantly higher among cigarette-first (AOR 1.44 [1.19, 1.74], p < 0.001) and same-grade (AOR 1.59 [1.36, 1.86], p < 0.001) initiators (not shown).
Marijuana Vaping Prevalence
Past 30-day marijuana vaping was reported by 29.5% of marijuana-first initiators, 14.9% of marijuana-only initiators, 19.0% of cigarette-first initiators, and 20.9% of same-grade initiators. The likelihood of marijuana vaping was statistically similar between marijuana-first initiators and all other initiation patterns. No significant differences were observed between marijuana-only initiators versus cigarette-first (p = 0.451) or same-grade (p = 0.858) initiators (data not shown).
Discussion
Among this large, nationally representative sample of U.S. 12th grade students, significant changes from 2000 to 2019 were observed in all self-reported patterns of cigarette and marijuana initiation. As hypothesized, marijuana-only and marijuana before cigarette initiation increased, while cigarette-only initiation decreased. Also as hypothesized, cigarette prevalence and frequency were highest among students who initiated cigarettes before marijuana; marijuana use prevalence and frequency were highest among students who initiated marijuana before cigarettes. Cigarette and marijuana use prevalence, and marijuana frequency, were lowest among students initiating only that substance. Nicotine vaping was less prevalent among students who initiated only one versus both substances; no significant nicotine vaping differences were observed between cigarette-only and marijuana-only initiators.
Before considering the findings’ implications, several limitations should be recognized. Data were cross-sectional; results cannot be interpreted as causal. Findings may not generalize to non-U.S. settings or to individuals who drop out of high school; lower educational attainment is associated with higher substance use (Tice et al. 2017). Initiation order was based on retrospective self-reported grade of first use. However, self-reported age of onset has been found to be reasonably accurate in regard to substance use sequencing (LaBouvie et al. 1997). Self-report substance use data have been found to be reasonably reliable and valid under appropriate conditions (e.g., recognized, clearly protected confidentiality) which the MTF study has sought to provide (Bachman et al. 2015; Brener et al. 2003; Johnston and O’Malley, 1985; Miech et al. 2020; O’Malley et al. 1983). Some key covariates associated with cigarette and marijuana use initiation, such as family substance use disorder history, could not be included due to MTF data limitations but should be considered in future research. Longitudinal research is needed to model causal connections between cigarette and marijuana initiation patterns and later substance use through adulthood. Limitations notwithstanding, these findings have several implications for prevention efforts.
The current study’s results are not consistent with the gateway model, and thus do not support primary prevention effort focus on deterring cigarette use in order to deter later marijuana use. Findings are consistent with the common liability model’s position that common factors are associated with overall substance use likelihood. One such factor may be changing social norms. As noted previously public acceptance has dramatically decreased for cigarette use while notably increasing for marijuana use (Bretteville-Jensen and Williams 2011; Fairman et al. 2019; McBride et al. 2016; Miech et al. 2020; Wen et al. 2019). Primary prevention efforts may be strengthened by focusing on deterring specific behaviors (cigarette, nicotine, and marijuana use) with particular attention given to prevention messaging for the most common substances/use methods in each locale that are likely to be used first by adolescents (Degenhardt et al. 2010).
The dramatic reductions in any cigarette initiation observed in the current study reflect, in part, incredible efforts by the prevention community to utilize policy and regulatory mechanisms to lower adolescent and adult tobacco use. It is important to realize that increasing marijuana initiation carries risks for tobacco and nicotine use. Marijuana use (particularly frequent use) is associated with transitions to higher levels of cigarette smoking involvement (Agrawal et al. 2008), lower cigarette cessation rates (Swift et al. 2012), and relapse (Weinberger et al. 2018). Further, marijuana use increases cigarette initiation likelihood during adolescence and into adulthood (Agrawal et al. 2008; Nguyen et al. 2018; Swift et al. 212; Tullis et al. 2003; Weinberger et al. 2018). Tobacco control efforts may be strengthened by giving additional attention to growing marijuana use (Weinberger et al. 2018). Correspondingly, marijuana prevention efforts may be strengthened by learning from existing tobacco control policy and regulatory approaches (Keyes et al. 2019), particularly as state policy increasingly allows legalized recreational adult marijuana use.
The current study’s findings have several implications for prevention as expressed in intervention and treatment. First, the common liability model suggests adolescent screening and assessment tools should assess a range of behaviors including alcohol, tobacco, marijuana, and other substances (DuPont et al. 2018; for example screening tools, see National Institute on Drug Abuse 2019). Identification of problematic use of one substance may be considered an indicator of high risk for problematic use of other substances, regardless of initiation order. Second, decreasing cigarette-only initiation indicates a growing percentage of adolescents who ever initiate cigarette use also will have some degree of current or past marijuana experience, and thus a higher likelihood of current smoking prevalence with high frequency. Efforts to help nicotine/tobacco-using youth reduce use and/or quit are more likely now to also address current marijuana use and possible withdrawal to both substances. Third, a growing percentage of adolescent marijuana users do not have experience with cigarette smoking, but do have experience with nicotine vaping. Given that marijuana use increases cigarette use initiation likelihood (Agrawal et al. 2008; Nguyen et al. 2018; Swift et al. 212; Tullis et al. 2003; Weinberger et al. 2018), clinicians should be aware of the potential need to help adolescents who have initiated marijuana but not cigarette use avoid transitioning to cigarette smoking.
Finally, this study’s findings regarding current vaping behaviors have implications for all prevention levels. More marijuana-only initiates reported current nicotine vaping than marijuana vaping (26.4% vs. 14.9%); approximately half of those who initiated both cigarettes and marijuana reported current nicotine vaping. These results are consistent with the route of administration model, in which both (a) physiological adaptation to substance inhalation and (b) social/cultural norms and behavioral cues surrounding smoked versus smokeless forms of tobacco may influence the likelihood of co-occurring use (Agrawal et al. 2012; Agrawal and Lynskey 2009). Primary prevention may be strengthened by focusing risk messaging on inhalation behaviors in general versus targeting specific vaping behaviors. Policy actions limiting adolescent access to vaping devices may simultaneously help reduce nicotine and marijuana vaping, marijuana smoking (Ksinan et al. 2020), and lung injury that has been found to be associated with vaping behaviors (Christiani 2020). An awareness of risks associated with different vaping technologies may also assist prevention efforts; some types of vaping devices facilitate switching between cannabis and nicotine juices (Majmundar et al. 2019).
Taken together, these findings underscore the importance of monitoring change in initiation patterns and evaluating how such change may impact efforts to prevent, intervene in, and treat adolescent cigarette, nicotine, and marijuana use. Cigarette-only initiation has decreased dramatically; a growing percentage of current adolescent cigarette users has some level of current or past experience with marijuana use, increasing the likelihood of currently smoking cigarettes and doing so at high frequency. The quickly growing group of marijuana-only initiators evidences meaningful levels of nicotine vaping, and a growing percentage of adolescents who initiate both cigarette smoking and marijuana use report marijuana-first initiation, associated with a higher likelihood of any and frequent current marijuana use. Prevention efforts may be strengthened by (a) emphasizing the importance of no adolescent substance use (vs. focusing on preventing “gateway” substances); (b) tailoring prevention messaging to shared routes of administration (i.e., inhaled use of both combustible and vaped substances); (c) expanding policy and regulatory efforts that have proved successful with tobacco to include marijuana; (d) encouraging use of screening tools that assess a range of adolescent substance use behaviors; and (e) recognizing that adolescents presenting for either tobacco/nicotine or marijuana use treatment increasingly are likely to have established co-use patterns that may affect both dependence and cessation.
Notes
From 2017 to 2018, the items were worded as “On how many occasions…”, while in 2019, the wording was changed to “On how many DAYS…”.
References
Agrawal, A., Budney, A. J., & Lynskey, M. T. (2012). The co-occurring use and misuse of cannabis and tobacco: A review. Addiction, 107, 1221–1233. https://doi.org/10.1111/j.1360-0443.2012.03837.x.
Agrawal, A., & Lynskey, M. T. (2009). Tobacco and cannabis co-occurrence: Does route of administration matter? Drug and Alcohol Dependence, 99, 240–247. https://doi.org/10.1016/j.drugalcdep.2008.08.007.
Agrawal, A., Madden, P. A. F., Bucholz, K. K., Heath, A. C., & Lynskey, M. T. (2008). Transitions to regular smoking and to nicotine dependence in women using cannabis. Drug and Alcohol Dependence, 95, 107–114. https://doi.org/10.1016/j.drugalcdep.2007.12.017.
American College of Pediatricians. (2018). Marijuana use: detrimental to youth. https://www.acpeds.org/the-college-speaks/position-statements/effect-of-marijuana-legalization-on-risky-behavior/marijuana-use-detrimental-to-youth. Accessed 8 May 2020.
Bachman, J. G., Johnston, L. D., O’Malley, P. M., Schulenberg, J. E., & Miech, R. A. (2015). The Monitoring the Future project after four decades: design and procedures (Monitoring the Future Occasional Paper No. 82). Ann Arbor, MI: Institute for Social Research, University of Michigan.
Baumeister, S. E., & Tossmann, P. (2005). Association between early onset of cigarette, alcohol and cannabis use and later drug use patterns: An analysis of a survey in European metropolises. European Addiction Research, 11, 92–98.
Brener, N. D., Billy, J. O. G., & Grady, W. R. (2003). Assessment of factors affecting the validity of self-reported health-risk behavior among adolescents: Evidence from the scientific literature. Journal of Adolescent Health, 33, –P436, 457. https://doi.org/10.1016/S1054-139X(03)00052-1.
Bretteville-Jensen, A. L., & Williams, J. (2011). Decriminalization and initiation into cannabis use (Research Paper No. 1130). Parkville, VIC: Department of Economics, University of Melbourne.
Budney, A. J., Sargent, J. D., & Lee, D. C. (2015). Vaping cannabis (marijuana): Parallel concerns to e-cigs? Addiction, 110, 1699–1704. https://doi.org/10.1111/add.13036.
Cantrell, J., Bennett, M., Mowery, P., Xiao, H., Rath, J., Hair, E., et al. (2018). Patterns in first and daily cigarette initiation among youth and young adults from 2002 to 2015. PLoS One, 13, e0200827. https://doi.org/10.1371/journal.pone.0200827.
Christiani, D. C. (2020). Vaping-induced acute lung injury. New England Journal of Medicine, 382, 960–962. https://doi.org/10.1056/NEJMe1912032.
Degenhardt, L., Chiu, W.-T., Sampson, N., Kessler, R. C., Anthony, J. C., Angermeyer, M., et al. (2008). Toward a global view of alcohol, tobacco, cannabis, and cocaine use: Findings from the WHO World Mental Health Surveys. PLoS Medicine, 5, e141. https://doi.org/10.1371/journal.pmed.0050141.
Degenhardt, L., Dierker, L., Chiu, W. T., Medina-Mora, M. E., Neumark, Y., Sampson, N., et al. (2010). Evaluating the drug use “gateway” theory using cross-national data: Consistency and associations of the order of initiation of drug use among participants in the WHO World Mental Health Surveys. Drug and Alcohol Dependence, 108, 87–97. https://doi.org/10.1016/j.drugalcdep.2009.12.001.
DuPont, R. L., Han, B., Shea, C. L., & Madras, B. K. (2018). Drug use among youth: National survey data support a common liability of all drug use. Preventive Medicine, 113, 68–73. https://doi.org/10.1016/j.ypmed.2018.05.015.
Evans-Polce, R. J., Veliz, P., Boyd, C. J., & McCabe, S. E. (2020). Initiation patterns and trends of e-cigarette and cigarette use among U.S. adolescents. Journal of Adolescent Health, 66, 27–33. https://doi.org/10.1016/j.jadohealth.2019.07.002.
Fairman, B. J. (2015). Cannabis problem experiences among users of the tobacco-cannabis combination known as blunts. Drug and Alcohol Dependence, 150, 77–84https://doi.org/10.1016/j.drugalcdep.2015.02.014.
Fairman, B. J., Furr-Holden, C. D., & Johnson, R. M. (2019). When marijuana is used before cigarettes or alcohol: Demographic predictors and associations with heavy use, cannabis use disorder, and other drug-related outcomes. Prevention Science, 20, 225–233. https://doi.org/10.1007/s11121-018-0908-3.
Green, K. M., Johnson, R. M., Milam, A. J., Furr-Holden, D., Ialongo, N. S., & Beboussin, B. A. (2016). Racial differences and the role of neighborhood in the sequencing of marijuana and tobacco initiation among urban youth. Substance Abuse, 37, 507–510. https://doi.org/10.1080/08897077.2016.1178680.
Henry, K. L., & Thornberry, T. P. (2010). Truancy and escalation of substance use during adolescence. Journal of Studies on Alcohol and Drugs, 71, 115–124. https://doi.org/10.15288/jsad.2010.71.115.
Hindocha, C., Shaban, N. D. C., Freeman, T. P., Das, R. K., Gale, G., Schafer, G., et al. (2015). Associations between cigarette smoking and cannabis dependence: A longitudinal study of young cannabis users in the United Kingdom. Drug and Alcohol Dependence, 148, 165–171. https://doi.org/10.1016/j.drugalcdep.2015.01.004.
Humfleet, G. L., & Hass, A. I. (2004). Is marijuana use becoming a ‘gateway’ to nicotine dependence? Addiction, 99, 5–6.
Johnston, L. D., & O’Malley, P. M. (1985). Issues of validity and population coverage in student surveys of drug use. In B. A. Rouse, N. J. Kozel, & L. G. Richards (Eds.), Self-report methods of estimating drug use: Meeting current challenges to validity (NIDA Research Monograph 57). National Institute on Drug Abuse: Washington, D.C.
Kandel, D., & Kandel, E. (2015). The gateway hypothesis of substance abuse: Developmental, biological and societal perspectives. Acta Pediatrica, 104, 130–137. https://doi.org/10.1111/apa.12851.
Kennedy, S. M., Patel, R. P., Cheh, P., Hsia, J., & Rolle, I. V. (2016). Tobacco and marijuana initiation among African American and white young adults. Nicotine and Tobacco Research, 18, S57–S64. https://doi.org/10.1093/ntr/ntv194.
Keyes, K. M., Rutherford, C., & Miech, R. (2019). Historical trends in the grade of onset and sequence of cigarette, alcohol, and marijuana use among adolescents from 1976-2016: Implications for “gateway” patterns in adolescence. Drug and Alcohol Dependence, 194, 51–58. https://doi.org/10.1016/j.drugalcdep.2018.09.015.
Ksinan, A. J., Spindle, T. R., Thomas, N. S., Eissenberg, T., Spit for Science Working Group, & Dick, D. M. (2020). E-cigarette use is prospectively associated with initiation of cannabis among college students. Addictive Behaviors, 106, 106312. https://doi.org/10.1016/j.addbeh.2020.106312.
LaBouvie, E., Bates, M. E., & Pandina, R. J. (1997). Age of first use: Its reliability and predictive utility. Journal of Studies on Alcohol, 58, 638–643.
Leatherdale, S. T., Hammond, D., & Ahmed, R. (2008). Alcohol, marijuana, and tobacco use patterns among youth in Canada. Cancer Causes and Control, 19, 361–369https://www.jstor.org/stable/40271873.
Livingston, M., Holmes, J., Oldham, M., Vashishtha, R., & Pennay, A. (2020). Trends in the sequence of fist alcohol, cannabis and cigarette use in Australia, 2001-2016. Drug and Alcohol Dependence, 207, 107821. https://doi.org/10.1016/j.drugalcdep.2019.107821.
Majmundar, A., Kirkpatrick, M., Cruz, T. B., Unger, J. B., & Allem, J. P. (2019). Characterising KandyPens-related posts to Instagram: Implications for nicotine and cannabis use. Tobacco Control.https://doi.org/10.1136/tobaccocontrol-2019-055006.
McBride, D. C., Terry-McElrath, Y. M., & VanderWaal, C. J. (2016). Illicit drug policy. In A. Eyler, J. Chriqui, S. M. Russell, & R. Brownson (Eds.), Prevention, policy, and public health (pp. 263–287). New York: Oxford University Press.
Miech, R. A., Johnston, L. D., O'Malley, P. M., Bachman, J. G., Schulenberg, J. E., & Patrick, M. E. (2020). Monitoring the future national survey results on drug use, 1975–2019: Volume I, secondary school students. Ann Arbor, MI: Institute for Social Research, The University of Michigan.
Muthén, L. K., & Muthén, B. O. (1998-2017). Mplus user’s guide (Eighth ed.). Los Angeles, CA: Muthén and Muthén.
National Institute on Drug Abuse. (2019). Screening tools for adolescent substance use. https://www.drugabuse.gov/nidamed-medical-health-professionals/screening-tools-resources/screening-tools-for-adolescent-substance-use. Accessed 8 May 2020.
Nguyen, T. Q., Ebnesajjad, C., Stuart, E. A., Kennedy, R. D., & Johnson, R. M. (2018). Does marijuana use at ages 16–18 predict initiation of daily cigarette smoking in late adolescence and early adulthood? A propensity score analysis of Add Health Data. Prevention Science. https://doi.org/10.1007/s11121-018-0874-9.
O’Malley, P. M., Bachman, J. G., & Johnston, L. D. (1983). Reliability and consistency of self-reports of drug use. International Journal of the Addictions, 18, 805–824.
Panlilio, L. V., Zanettini, C., Barnes, C., Solinas, M., & Goldberg, S. R. (2013). Prior exposure to THC increases the addictive effects of nicotine in rats. Neuropsychopharmacology, 38, 1198–1208. https://doi.org/10.1038/npp.2013.16.
Peters, E. N., Budney, A. J., & Carroll, K. M. (2012). Clinical correlates of co-occurring cannabis and tobacco use: A systematic review. Addiction, 107, 1404–1417. https://doi.org/10.1111/j.1360-0443.2012.03843.x.
Reidpath, D. D., Davey, T. M., Kadirvelu, A., Soyiri, I., & Allotey, P. (2014). Does one cigarette make an adolescent smoker, and is it influenced by age and age of smoking initiation? Evidence of association from the U.S. Youth Risk Behavior Surveillance System (2011). Preventive Medicine, 59, 37–41. https://doi.org/10.1016/j.ypmed.2013.11.011.
Richmond-Rakerd, L. S., Slutske, W. S., & Wood, P. K. (2017). Age of initiation and substance use progression: A multivariate latent growth analysis. Psychology of Addictive Behaviors, 31, 664–675. https://doi.org/10.1037/adb0000304.
Rubinstein, M. L., Rait, M. A., & Prochaska, J. J. (2015). Frequent marijuana use is associated with greater nicotine addiction in adolescent smokers. Drug and Alcohol Dependence, 141, 159–162. https://doi.org/10.1016/j.drugalcdep.2014.05.015.
Swift, W., Coffey, C., Degenhardt, L., Carlin, J. B., Romaniuk, H., & Patton, G. C. (2012). Cannabis and progression to other substance use in young adults: Findings from a 13-year prospective population-based study. Journal of Epidemiology and Community Health, 66, e26. https://doi.org/10.1136/jech.2010.129056.
Tice, P., Lipari, R. N., & Van Horn, S. L. (2017). Substance use among 12thgrade aged youths, by dropout status. CBHSQ Report. Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality.
Tullis, L. M., DuPont, R., Frost-Pineda, K., & Gold, M. S. (2003). Marijuana and tobacco. Journal of Addictive Diseases, 22, 51–62. https://doi.org/10.1300/J069v22n03_05.
U.S. Department of Health and Human Services. (2012). Preventing tobacco use among youth and young adults: A report of the surgeon general. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
van Leeuwen, A. P., Verhulst, F. C., Reijneveld, S. A., Vollebergh, W. A. M., Ormel, J., & Huizink, A. C. (2011). Can the gateway hypothesis, the common liability nodel and/or, the route of administration model predict initiation of cannabis use during adolescence? A survival analysis—The TRAILS Study. Journal of Adolescent Health, 48, 73–78. https://doi.org/10.1016/j.jadohealth.2010.05.008.
Vanyukov, M. M., Tarter, R. E., Kirillova, G. P., Kirisci, L., Reynolds, M. D., Kreek, M. J., et al. (2012). Common liability to addiction and “gateway hypothesis”: Theoretical, empirical and evolutionary perspective. Drug and Alcohol Dependence, 123S, S3–S17. https://doi.org/10.1016/j.drugalcdep.2011.12.018.
Weinberger, A. H., Platt, J., Copeland, J., & Goodwin, R. D. (2018). Is cannabis use associated with increased risk of cigarette smoking initiation, persistence, and relapse? Longitudinal data from a representative sample of US adults. Journal of Clinical Psychiatry, 79, e1.
Wen, H., Hockenberry, J., & Druss, B. G. (2019). The effect of medical marijuana laws on marijuana-related attitude and perception among US adolescents and young adults. Prevention Science, 20, 215–223. https://doi.org/10.1007/s11121-018-0903-8.
Funding
This study was supported by the National Institute on Drug Abuse (R01DA001411). The study sponsor had no role in (a) study design; (b) the collection, analysis, and interpretation of data; (c) the writing of the report; or (4) the decision to submit the manuscript for publication. The views expressed in this article are those of the authors and do not necessarily reflect the views of the sponsor.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflicts of interest.
Ethical Approval
The study procedures were approved by the University of Michigan’s Health Sciences and Behavioral Sciences Institutional Review Board, and were performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed Consent
Appropriate consent procedures were used in accordance with federal, state, and school policies.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
ESM 1
(DOCX 48 kb)
Rights and permissions
About this article

Cite this article
Terry-McElrath, Y.M., O’Malley, P.M. & Johnston, L.D. Changes in the Order of Cigarette and Marijuana Initiation and Associations with Cigarette Use, Nicotine Vaping, and Marijuana Use: U.S. 12th Grade Students, 2000–2019. Prev Sci 21, 960–971 (2020). https://doi.org/10.1007/s11121-020-01150-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11121-020-01150-2