
Abstract
Most young adults with mental health symptoms do not receive treatment or access services. It remains important to identify barriers to service utilization to improve access to care. The current study was a prospective analysis examining predictors of (a) mental health service utilization and (b) perceived unmet need for mental health services. Barriers to service utilization were examined by prior depression severity status and college student status. Participants included a subsample of young adults ages 18–23 at time of recruitment who were participating in a longitudinal monthly study who completed both baseline and a 15-month follow-up assessment (N = 622, 80% of larger study). At month 15, 23% of young adults reported receiving mental health services in the past 12 months; 26% of young adults reported a perceived unmet need for mental health services at some point in the past 12 months. There were differences in demographic and mental health predictors of service utilization and perceived unmet need for services. Women, sexual minorities, those with moderate depression, those with more impairment from depression, and perceived past year poor mental health were associated with greater likelihood of receiving services. Similar demographic characteristics were associated with greater likelihood of perceiving unmet need for services. Barriers to service utilization differed by severity of depression symptoms and student status. Young adults have distinct reasons for not accessing mental health services; addressing these to improve accessibility to care remains critical.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Late adolescence and young adulthood is a critical time for the development and manifestation of mental health disorders as a total of 75% of all lifetime disorders present by the age of 24 (Kessler et al. 2005). Prevalence rates for the majority of mental health disorders are higher among adolescents and young adults than in any other age group, with the most common being anxiety disorders (14%) and depressive disorders (17%) (Grant et al. 2004; Kessler et al. 2005; Merikangas et al. 2010). Despite a significant body of research identifying empirically-supported, efficacious treatment for mental illness (APA 2006) many young adults do not receive services. It has been estimated 7.6 million American young adults (22%) meet criteria for a mental health disorder each year and one-third (estimates ranging from 32 to 41%) received mental health services within the past year (Eisenberg et al. 2007; Eisenberg et al. 2011; SAMSHA 2014; Wang et al. 2005).
Depression and Service Utilization
Prevalence rates of a past year Major Depressive Disorder (MDD) are highest among young adults compared to any other age cohort (APA 2013; SAMSHA 2014). In 2015, a total of 3.6 million American young adults (10.3% of young adults) had a major depressive episode in the past year and 1.7 million (46.8%) of those individuals received mental health services for depression (SAMSHA 2014). In a study of over 70 college campuses, less than half of all students who reported seriously considering attempting suicide in the past year received services (Drum et al. 2009). Given that depression is associated with increased risk of suicide and significant impairment in social, occupational, and emotional functioning, service utilization is essential (Brent et al. 1993; Brown et al. 2000; SAMSHA 2014).
Student Status and Service Utilization
There are important distinctions between young adults attending college and same-aged non-college peers with regard to mental health service utilization. Although full-time college students and same-aged non-college peers report a similar prevalence of psychiatric disorders and serious thoughts of suicide (8.0 and 8.7%, respectively), college students are less likely than non-college peers to attempt suicide (Blanco et al. 2008; SAMSHA 2014). Among young adults with a past year mood disorder, 34.1% of college students and 34.8% of non-college young adults received mental health treatment (Blanco et al. 2008).
Mental Health Attitudes and Barriers to Service Utilization
Given the prevalence of mental health disorders and low endorsement of mental health service utilization, it remains critical to identify and understand attitudes and barriers to service utilization to improve access to care. In the general US adult population, reasons for not receiving services were assessed among 5.1 million adults with a past year mental illness who perceived a need for treatment but did not receive it (SAMSHA 2014). Over half of adults (55%) were not able to afford the cost, 26% did not know where to go for services, 25% thought they could handle the problem without treatment, 11% thought treatment would not help, 11% had a fear of being committed or having to take medicine, 10% reported their health insurance did not cover enough treatment, and 9% thought receiving services may have a negative effect on their job (SAMSHA 2014). Other frequently endorsed barriers to mental health service utilization among young adults include perceived stigma, fear of negative effect on career and academic record, not recognizing symptoms, and general lack of knowledge about mental health services (Eisenberg et al. 2012; Gulliver et al. 2010). Many college students do not receive services because they do not perceive a need and prefer to handle their problems on their own (Eisenberg et al. 2011).
Although rates of mental health service utilization are similar between college and non-college age young adults (Blanco et al. 2008), less is known about how barriers to service utilization differ between these groups. Differences in access to resources (i.e., many college students have access to a centralized student health service building which could deliver interventions for free or reduced cost) may contribute to differences in service utilization (Blanco et al. 2008). Understanding barriers to accessing services among subgroups of young adults will help clinicians and researchers identify targeted approaches to address young adult service needs.
Demographic variables are known to be associated with greater likelihood of service utilization. Rates of mental health service utilization have been found to be higher for women, sexual minorities, individuals 21 or older, and those with lower religiosity (Burgess et al. 2008; Dunbar et al. 2017; Pottick et al. 2008). We examined these variables in models predicting service utilization and perceived unmet service need.
Current Study
Although a significant body of research has examined college student mental health and barriers to service utilization among 4-year college students (e.g., Eisenberg et al. 2011; Zivin et al. 2009), with some attention on 2-year community college students (e.g., Katz and Davison 2014), little attention has been placed on examining community samples of young adults. Further, less is known regarding how barriers to service utilization differ among those with and without depression symptoms and among college students (both community college and 4-year students) and same-aged non- college peers. Therefore, the current study examines mental health service utilization and barriers to service utilization among 622 young adults (ages 18–23 at recruitment) who completed a baseline assessment and a follow-up assessment 15 months later. We examined baseline demographic characteristics and mental health symptoms to prospectively identify predictors of mental health service utilization and barriers to service utilization over a year later. The following research questions were examined: (1) What demographic characteristics and baseline mental health symptoms predict: a) receiving mental health services (service utilization) assessed 15 months later and b) perceiving a need for mental health services but not receiving it (i.e., perceived unmet service need) assessed 15 months later, (2) How do service utilization and attitudes about service utilization differ by depression symptom status, and (3) Among young adults who report a perceived unmet service need, how do barriers differ between (a) those with baseline depression and those without and (b) college students and same-aged non-students? We hypothesized mental health symptoms would predict perceived unmet service need and specific demographic variables (i.e., women, sexual minority, age 21 or older) would predict receiving services. We also hypothesized barriers of perceived need and cost of mental health care would differ by depression subgroup and student subgroup.
Method
Participants and Procedures
Participants were 622 young adults (ages 18–23 at recruitment) who were participating in a longitudinal monthly study of young adult transitions and alcohol use and completed a 15 month assessment. Young adults were recruited from a large metropolitan area in the Pacific Northwest United States. Recruitment methods included online, social media, and print advertisements, and community outreach. Those interested were asked to contact the study and complete a brief screening survey to determine eligibility. Eligibility criteria included being 18–23 years old at recruitment, residing within 60 miles of the research site, having a valid email address, drinking alcohol at least once in the last year, and being willing to come to the study office for an initial appointment. At the appointment, age was verified by driver’s license or photo ID, and informed consent was obtained from all participants in the study. All procedures were approved by the University Institutional Review Board, a federal Certificate of Confidentiality was obtained, and no adverse consequences were reported.
In total, 779 young adults met eligibility criteria, came to the study offices and completed the baseline survey. The longitudinal commitment for the larger project included completing 24 consecutive months of online surveys plus a final survey at 30 months. Data for the present analyses include measures from the baseline assessment and month 15 assessment. Participants received $20 in Amazon gift cards for completed surveys in Year 1, $25 in Year 2 and a $20 bonus if they completed all monthly surveys in a 6-month period.
Of the subset of participants who completed both baseline and month 15 assessments (n = 622, 79.8% of the total sample), the majority were women (59.5%), Caucasian (58.9%), and heterosexual (80.8%), 19.8% were Asian or South Asian, 4.7% were Black or African American, 1.3% Arab, Middle Eastern, or Northern African, 0.5% American Indian or Alaskan Native, and 0.6% Native Hawaiian or other Pacific Islander. A total of 11.5% reported more than one race and 7.8% across races were Hispanic/Latino/a ethnicity.
Using this subset of participants (n = 622), at baseline most of the participants were students (74.1%). Among the students, 1.9% were high school students, 0.3% were working toward a General Education Development (GED), 1.1% were trade or vocational school students, 18.3% were 2-year community college students, 47.2% were 4-year college or university students, and 5.3% were graduate or professional school students. Approximately, one-fourth of the sample was not currently students (25.8%). A total of 39.6% of participants were not working, 44.3% were working part-time, and 16.2% were working fulltime. Over half of all participants were age 21 or older (54.4%) and the average age of the sample was 20.68 years old (SD = 1.726). A third of participants (33.4%) reported they had no current influential religious beliefs. A total of 7.4% of participants reported they had been homeless at some point in their lives. When asked about their current health insurance, 71.1% were covered on their parent’s plan, 12.4% were on Medicaid, 9.8% were covered at work or school, 3.4% did not currently have insurance, 2.6% reported other, and 0.8% stated they pay out of pocket.
Measures
Demographic characteristics, substance use, and mental health symptoms were assessed at baseline. Mental health services, attitudes, and barriers were assessed at month 15.
Demographic characteristics included: biological sex (0 = male; 1 = female), age (0 = less than 21; 1 = 21 or older), sexual orientation (0 = heterosexual; 1 = sexual minority), ever been homeless (0 = never homeless; 1 = ever homeless), religious beliefs (0 = no current influential religious beliefs; 1 = currently have influential religious beliefs), student status (0 = not a student; 1 = student), and employment status (0 = not employed; 1 = employed part-time or full-time).
Substance Use
Alcohol use was assessed with the Alcohol Use Disorders Identification Test (AUDIT; Babor et al. 2001), a 10-item self-report measure used to assess hazardous alcohol consumption and alcohol dependence. Some response options in the current study (i.e., “2 to 3 times per week”, “4 or more times were week”) were worded slightly differently than in the original AUDIT (i.e., “weekly”, “daily or almost daily”).
Alcohol-related problems were assessed with The Brief Young Adult Alcohol Consequences Questionnaire (BYAACQ; Kahler et al. 2005). The BYAACQ consists of 24 dichotomous items used to assess alcohol-related problems during the past month. The internal consistency estimate for the measure was .86. Marijuana use was assessed with the Cannabis Use Disorder Identification Test (CUDIT-R; Adamson et al. 2010), an 8-item self-report measure to identify individuals with harmful cannabis use. Substance use treatment was assessed with the item “Have you ever received treatment or counseling for your use of alcohol or any drug use as a client or patient?” (0 = no; 1 = yes).
Mental Health
Depressive symptoms were assessed using the Patient Health Questionnaire (PHQ-9; Spitzer et al. 1999). The PHQ-9 is a widely used self-report measure for assessing depression symptoms (Kroenke et al. 2001). Participants are presented with nine symptoms of depression and instructed to indicate “Over the last month, how often have you been bothered by any of the following problems?” on a scale from “0-Not at all”, “1-Several days”, “2-More than half the days”, to “3-Nearly every day”. Total scores range from 0 to 27. PHQ-9 scores of 10 or greater are recommended as a cutpoint for Major Depression, with a sensitivity of 88% and specificity of 88% (Kroenke and Spitzer 2002). Consistent with the guidelines of the recommended clinical cutpoint, individuals were coded as having “no depression symptoms at baseline” if their total PHQ-9 score was less than 10 and coded as having “depression symptoms at baseline” if their total PHQ-9 score was 10 or greater. Additionally, scores of 5, 10, 15, and 20 were used as the cutpoints for mild, moderate, moderately severe and severe depression, respectively (Kroenke et al. 2001). The internal consistency estimate for the measure was .88. Item-9 was used to assess suicidality. Anxiety symptoms were assessed using a modified version of the Generalized Anxiety Disorder-7 (GAD-7; Spitzer et al. 2006). The GAD-7 has shown excellent sensitivity (89%) and specificity (82%) in detecting generalized anxiety disorder. Participants are presented with various problems and indicate “Over the last month, how often have you been bothered by any of the following problems?” on a scale from “Not at all,” “Several days,” “More than half the days,” to “Nearly every day.” In the current study, five items from the GAD-7 were used as an indicator of anxiety (α = .85): “Feeling nervous, anxious, or on edge,” “Worrying too much about different things,” “Trouble relaxing,” “Being so restless that it is hard to sit still,” and “Becoming easily annoyed or irritable.” Perceived stress was assessed using the Perceived Stress Scale (PSS; Cohen et al. 1983), a 14-item self-report measure where participants indicate how often in the past month they felt various levels of stress (α = .85).
General mental health was assessed with the items “In general, how would you say your mental health was in the past 12 months?” and “In general, how would you say your mental health was in the previous month?” [response options ranged from: Excellent (1) to Poor (5)] which were adapted from the Centers for Disease Control and Prevention (CDC 2013).
Mental health service utilization was assessed with the item “During the past 12 months, have you received counseling or outpatient treatment for any problem you were having with your emotions, nerves, or mental health? Please do not include counseling for alcohol or drug use” (0 = no; 1 = yes) (SAMSHA 2014).
Perceived unmet need for mental health service was assessed with the item “During the past 12 months was there any time when you needed mental health treatment or counseling for yourself but did not get it?” (0 = no; 1 = yes).
Attitudes toward service utilization was assessed with the items “If you had a serious emotional problem, how likely would you go for professional help?” [response options ranged from: Definitely Go (1) to Definitely Not Go (4)], “How comfortable would you feel talking about personal problems with a professional?” [response options ranged from: Very Comfortable (1) to Not At All Comfortable (4)], “How embarrassed would you be if your friends knew you were getting professional help for an emotional problem?” [response options ranged from: Very Embarrassed (1) to Not At All Embarrassed (4)], (Gonzalez et al. 2005).
Barriers to service utilization
Individuals who responded “yes” to perceived unmet need for mental health services were then asked “Which of these statements explain why you did not get the mental health treatment or counseling you needed?” and asked to check all that apply from a list of 15 items (see Table 3 for list, SAMSHA 2014).
Analytic Procedure
First, logistic regression was used to examine baseline predictors of receiving mental health services in the past 12 months and predictors of perceived unmet need for services in the past 12 months (as measured in month 15). A stepwise model was used with demographic variables on step 1, substance use variables on step 2, and mental health variables on step 3. In the final step (step 3), all significant predictors were also significant in all previous steps, therefore for the sake of parsimony, only the final step is shown. Second, chi-square tests, t tests, and nonparametric Mann-Whitney U tests were used to assess differences in mental health attitudes and service utilization by baseline depression symptom status. Third, among those who reported a perceived unmet need for mental health services, chi-square tests were used to examine barriers to service utilization as a function of baseline depression symptom status and school status.
Results
Descriptive Information
At baseline, the average AUDIT score was 6.26 (SD = 4.87; range: 0–28), average BYAACQ score was 3.23 (SD = 3.76; range: 0–21), and average CUDIT-R score was 4.33 (SD = 5.42; range: 0–29). A total of 28.1% (n = 174) screened positive for depression symptoms. The average depression score on the PHQ-9 was 7.26 (SD =5.33; range: 0–27), average anxiety scores was 4.80 (SD =3.52; range: 0–15), and the average perceived stress score was 22.32 (SD = 9.03; range: 0–56).
Predictors of Mental Health Service Utilization
At month 15, a total of 22.7% (n = 141) of young adults reported they had received mental health services in the past 12 months. Sex and sexual orientation status were significantly associated with the likelihood of receiving mental health services at month 15 (Table 1), such that women and sexual minorities had greater odds of receiving services. Depression severity status was associated with the likelihood of receiving services, such that individuals with moderate depression (i.e., PHQ-9 scores of 10–14) had greater odds of receiving services. Depression impairment was associated with the likelihood of receiving services, as those with “very difficult” impairment had greater odds of receiving services. Individuals with a perceived past year mental health as “fair” or “poor” had a significantly greater likelihood of receiving services. No other significant associations were found.
Predictors of Perceived Unmet Need for Mental Health Services
At month 15, a total of 26.1% (n = 161) of young adults identified a perceived unmet need for mental health services at some point in the past 12 months. Sex and sexual orientation status were significantly associated with the likelihood of perceiving a need for mental health services at month 15 but not receiving it (Table 1), such that women and sexual minorities had greater odds of endorsing an unmet need. Young adults who perceived their past year mental health as “fair,” or “poor” had a significantly greater likelihood of endorsing a perceived need for services but not receiving it. No other significant associations were found.
Mental Health Attitudes and Service Utilization by Depression Symptoms
Differences in mental health attitudes and service utilization by baseline depression symptom status are shown in Table 2. Young adults with baseline depression symptoms perceived their past year and past month mental health as significantly worse than individuals without depression symptoms. There were no differences in the likelihood of going to a professional for help, feeling comfortable talking about problems with a professional, or feeling embarrassed if friends knew they were getting professional help for an emotional problem between young adults with depression symptoms and those without. Young adults with depression symptoms were more likely to receive services, and also to report a perceived unmet need for mental health services, compared to those who were not depressed.
Barriers to Service Utilization
At month 15, young adults who reported a perceived unmet need for mental health services in the past 12 months (n = 161), were asked to select all reasons why they did not get the mental health services they needed (Table 3). The most common responses were: thought could handle the problem without treatment (60.6%), did not have time because of job, childcare, or other commitments (51.3%), could not afford the cost (39.4%), did not think treatment would help (36.3%), and did not know where to go to get services (33.1%).
Barriers as a Function of Depression Symptoms
Young adults with depression symptoms were more likely to not receive services due to concerns that treatment or counseling might have a negative effect on their job, concerns they might be committed to a psychiatric hospital or might have to take medicine, and logistical issues (i.e., lack of transportation, not convenient hours, did not know where to go to get services) than non-depressed individuals.
Barriers as a Function of Student Status
Young adults who were not students were more likely to report not receiving services because they could not afford the cost or because health insurance does not pay enough for mental health treatment. Students were more likely to report not receiving services because they did not think they needed treatment.
Discussion
Young adulthood is a developmental stage characterized by transitions in social roles, living situations, work status, relationships, and identity (Arnett 2007; Schulenberg and Maggs 2002) and is an acute time for the development of mental health disorders (Kessler et al. 2005). The current study found certain demographic characteristics and mental health symptoms assessed at baseline predicted mental health service utilization, in addition to predicting perceived unmet need for mental health services, over a year later. The study also extends research on attitudes of service utilization and barriers by examining differences among subgroups (i.e., college status; depression status) to further understand their unique needs.
Mental Health Service Utilization
In the general U.S. population of adults aged 18 and older, 14.6% receive mental health services in the past year (SAMSHA 2014). In our sample of young adults, 22.7% reported receiving mental health services in the past year. Consistent with previous research examining predictors of service utilization among college students (Eisenberg et al. 2007; Eisenberg et al. 2011; Zivin et al. 2009), we found females and sexual minorities to be more likely to receive services as assessed nearly fifteen months later. Individuals reporting their past year mental health (assessed at 15 month follow-up) was “fair” or “poor” were also more likely to have received services. Notably, we also found those with moderate depression (i.e., PHQ-9 scores between 10 and 14) and with “very difficult” impairment were more likely to receive services. This suggests young adults with some impairment (e.g., experiencing some depression symptoms impacting daily functioning) may be more motivated to utilize services than those with higher levels of impairment and risk for self-harm (e.g., severe, impairing, depression symptoms).
Rates of depressive symptoms were higher in the current study than among other young adults and college student samples. We found 28% of young adults screened positive for depression symptoms (i.e., PHQ-9 scores > 10), while other student samples have found 15% screened positive for depression symptoms (Eisenberg et al. 2007). Our finding that 49.3% of individuals with depression symptoms received services was similar to a finding that 45% of college students with MDD received services in the past year (Eisenberg et al. 2007).
Perceived Unmet Need for Mental Health Services
There is a substantial unmet need for mental health services among young adults, a vulnerable group for developing mental health disorders. For those with perceived past year mental health as “fair” or “poor,” the odds were 20 and 24 times higher, respectively, that they reported needing services but not receiving them compared to those with “excellent” past year mental health. This highlights that those with mental health difficulties were more likely to report an unmet service need. These findings are similar to cross-sectional analyses showing students with mental health problems report a need for services with many not receiving them (Eisenberg et al. 2007; Eisenberg et al. 2011).
Being female and identifying as a sexual minority were the only demographic factors to predict both 1) receiving mental health services and 2) perceived unmet need for services. Similarly, rates of service utilization are higher for women and sexual minorities (Burgess et al. 2008; Dunbar et al. 2017; Pottick et al. 2008). Consistent with our findings, sexual minority college students have been shown to report higher rates of psychological distress and are more likely to use mental health services than heterosexual students (Dunbar et al. 2017). Therefore, it is possible both women and sexual minority young adults are more likely to report an unmet need for services due to greater distress and are more likely to access services.
Barriers to Service Utilization
The most frequently endorsed barrier to mental health service utilization was believing one could handle the problem without treatment. This barrier, often referred to in the literature as “self-reliance,” has been frequently cited among young adults as a reason for not pursuing treatment (Gulliver et al. 2010). If young adults are steadfast about not accessing services, we recommend they have access to evidence-based self-help material (e.g., treatment workbooks, mobile apps, web-based resources). It is also important they be informed of accurate norms that they are not alone (e.g., in our study 1 in 4 students had depression symptoms) and that most young adults who do not believe they need services actually have elevated clinical symptoms and may benefit from brief interventions (Geisner et al. 2006).
Compared to non-depressed young adults, depressed young adults were more likely to report not receiving services due to logistical concerns (e.g., not knowing where to get treatment or how to get there) and concerns that treatment would negatively affect their job. Our finding show there were no differences in employment rates between depressed young adults and non-depressed young adults, suggesting that the implications of mental health services negatively impacting work is more salient for depressed individuals. This is consistent with findings from nationally representative data that 26% of US adults with service needs do not know where to go for services and 9% are concerned about treatment impacting their job (SAMSHA 2014).
Interventions aimed at increasing service utilization remain essential. Greater problem recognition has been associated with service utilization and students with active coping skills (i.e., knowing where to go for help; seeking alternative solutions to problems) are likely to use mental health services (Leaf et al. 1985; Sontag-Padilla et al. 2016). Therefore, clinicians and researchers could develop interventions targeting problem recognition skills (we found 26% of young adults with depression symptoms reported they did not think they needed treatment) and enhancing active coping and problem solving skills (we found 42% of young adults with depression symptoms did not know where to go to services and 26% had other logistical issues preventing them from accessing services) to improve service utilization.
Barriers to service utilization also differ between college students and non-college same aged peers. Increasing problem recognition could also be helpful for college students as they were more likely to report they did not need services. Many students have access to on-campus mental health resources for free or reduced cost which may minimize barriers related to cost and transportation (i.e., Blanco et al. 2008; Eisenberg et al. 2007). Some colleges have also adopted stigma-reducing campaigns on campuses (Hunt & Eisenberg 2010). Future research could examine where college students access mental health services (i.e., on- or off-campus) to further understand how students utilize services.
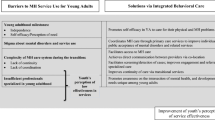
For all young adults, a model of screening, brief intervention, and referral to treatment (SBIRT) could be especially helpful in identifying those at risk (i.e., based on PHQ-9, GAD-7, substance use), followed by a warm handoff with a mental health service provider. Integrating mental health screening and providing some level of intervention based on an individual’s risk could enhance service utilization and increase dissemination of empirically-supported treatment. Compared to students, non-college young adults were more likely to report not receiving services due to cost/insurance. Providing a cost-effective screening and brief intervention option for non-college students, who have monetary concerns, is especially important.
Although there were no differences in attitudes about receiving services for young adults with and without depression, nearly 40% of both groups reported they would “probably not go” or “definitely not go” for professional help if they had a serious emotional problem. Further, 13% of the sample reported a barrier to service utilization was stigma concerns that mental health treatment might cause friends or family to have a negative opinion of them. It is possible these individuals are endorsing public stigma and not necessarily self-stigma, which is related to internalizing perceived negative beliefs about mental health which can lead to reduced self-worth, feelings of shame, and consequently less intention to seek mental health services (Sharp et al. 2015; Vogel et al. 2006). We encourage researchers to develop novel approaches to increase problem recognition, willingness to seek treatment, and reduce perceived self-stigma.
Limitations and Summary
Results and interpretations should be considered in light of several limitations. Although self-report measures used to assess mental health symptoms have strong psychometric properties and are frequently used, scores from the measures are not diagnostic. We did not assess the type of services received nor psychiatric medications. It is important to recognize ethnic and cultural values may impact what behavior or symptoms individuals view as problematic, affecting their decision to pursue services (Cauce et al. 2002). Cultural factors related to mental health utilization were not assessed. The sample was recruited from a single metropolitan area and included young adults who reported drinking at least once in the prior year, thus results may not generalize to other populations. Despite these limitations, the current study identified predictors of, and barriers to, mental health service utilization and perceived unmet need among emerging adults using a longitudinal dataset of diverse 18 to 23 year olds. We encourage future research to continue to address barriers to service utilization and improve access to care for those in need.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: DSM-5. Washington, D.C: American Psychiatric Association.
Adamson, S. J., Kay-Lambkin, F. J., Baker, A. L., Lewin, T. J., Thornton, L., Kelly, B. J., & Sellman, J. D. (2010). An improved brief measure of cannabis misuse: The cannabis use disorders identification test—revised (CUDIT-R). Drug and Alcohol Dependence, 110, 137–143.
APA Presidential Task Force on Evidence-Based Practice. (2006). Evidence-based practice in psychology. American Psychologist, 61, 271–285.
Arnett, J. J. (2007). Emerging adulthood: what is it, and what is it good for? Child Development Perspectives, 1, 68–73.
Babor, T. F., Higgins-Biddle, J. C., Saunders, J. B., Monteiro, M. G., & World Health Organization. (2001). AUDIT: The alcohol use disorders identification test: Guidelines for use in primary health care.
Blanco, C., Okuda, M., Wright, C., Hasin, D. S., Grant, B. F., Liu, S. M., & Olfson, M. (2008). Mental health of college students and their non–college-attending peers: results from the national epidemiologic study on alcohol and related conditions. Archives of General Psychiatry, 65, 1429–1437. https://doi.org/10.1001/archpsyc.65.12.1429
Brent, D. A., Perper, J. A., Moritz, G., Allman, C., Friend, A. M. Y., Roth, C., et al. (1993). Psychiatric risk factors for adolescent suicide: a case-control study. Journal of the American Academy of Child & Adolescent Psychiatry, 32, 521–529.
Brown, G. K., Beck, A. T., Steer, R. A., & Grisham, J. R. (2000). Risk factors for suicide in psychiatric outpatients: a 20-year prospective study. Journal of Consulting and Clinical Psychology, 68, 371–377.
Burgess, D., Lee, R., Tran, A., & Van Ryn, M. (2008). Effects of perceived discrimination on mental health and mental health services utilization among gay, lesbian, bisexual and transgender persons. Journal of LGBT Health Research, 3, 1–14. https://doi.org/10.1080/15574090802226626
Cauce, A. M., Domenech-Rodríguez, M., Paradise, M., Cochran, B. N., Shea, J. M., Srebnik, D., & Baydar, N. (2002). Cultural and contextual influences in mental health help seeking: a focus on ethnic minority youth. Journal of Consulting and Clinical Psychology, 70, 44–55.
Centers for Disease Control and Prevention (CDC). (2013). Behavioral Risk Factor Surveillance System Survey Questionnaire. Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. BRFSS. 2013 Behavioral Risk Factor Surveillance System Questionnaire.
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24, 385–396.
Drum, D. J., Brownson, C., Denmark, A. B., & Smith, S. E. (2009). New data on the nature of suicidal crises in college students: shifting the paradigm. Professional Psychology: Research and Practice, 40, 213–222. https://doi.org/10.1037/a0014465
Dunbar, M. S., Sontag-Padilla, L., Ramchand, R., Seelam, R., & Stein, B. D. (2017). Mental health service utilization among lesbian, gay, bisexual, and questioning or queer college students. Journal of Adolescent Health. https://doi.org/10.1016/j.jadohealth.2017.03.008
Eisenberg, D., Hunt, J., & Speer, N. (2012). Help seeking for mental health on college campuses: review of evidence and next steps for research and practice. Harvard Review of Psychiatry, 20, 222–232.
Eisenberg, D., Hunt, J., Speer, N., & Zivin, K. (2011). Mental health service utilization among college students in the United States. The Journal of Nervous and Mental Disease, 199, 301–308.
Eisenberg, D., Golberstein, E., & Gollust, S. E. (2007). Help-seeking and access to mental health care in a university student population. Medical Care, 45, 594–601.
Geisner, I. M., Neighbors, C., & Larimer, M. E. (2006). A randomized clinical trial of a brief, mailed intervention for symptoms of depression. Journal of Consulting and Clinical Psychology, 74, 393–399. https://doi.org/10.1037/0022-006X.74.2.393
Grant, B. F., Stinson, F. S., Dawson, D. A., Chou, S. P., Dufour, M. C., Compton, W., et al. (2004). Prevalence and co-occurrence of substance use disorders and independent mood and anxiety disorders: results from the national epidemiologic survey on alcohol and related conditions. Archives of General Psychiatry, 61, 807–816.
Gonzalez, J. M., Alegria, M., & Prihada, T. J. (2005). How do attitudes toward mental health treatment vary by age, gender, and ethnicity/race in young adults? Journal of Community Psychology, 33, 611–629. https://doi.org/10.1002/jcop.20071
Gulliver, A., Griffiths, K. M., & Christensen, H. (2010). Perceived barriers and facilitators to mental health help-seeking in young people: a systematic review. BMC Psychiatry, 10, 113. https://doi.org/10.1186/1471-244X-10-113
Hunt, J., & Eisenberg, D. (2010). Mental health problems and help-seeking behavior among college students. Journal of Adolescent Health, 46(1), 3–10.
Kahler, C. W., Strong, D. R., & Read, J. P. (2005). Toward efficient and comprehensive measurement of the alcohol problems continuum in college students: the brief young adult alcohol consequences questionnaire. Alcoholism: Clinical and Experimental Research, 29, 1180–1189. https://doi.org/10.1097/01.ALC.0000171940.95813.A5
Katz, D. S., & Davison, K. (2014). Community college student mental health: a comparative analysis. Community College Review, 42, 307–326.
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62, 593–602. https://doi.org/10.1001/archpsyc.62.6.593
Kroenke, K., & Spitzer, R. L. (2002). The PHQ-9: a new depression diagnostic and severity measure. Psychiatric Annals, 32, 509–515.
Kroenke, K., Spitzer, R. L., & Williams, J. B. W. (2001). The PHQ9: validity of a brief depression severity measure. Journal of General Internal Medicine, 16, 606–616. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
Leaf, P. J., Livingston, M. M., Tischler, G. L., Weissman, M. M., Holzer III, C. E., & Myers, J. K. (1985). Contact with health professionals for the treatment of psychiatric and emotional problems. Medical Care, 23, 1322–1337.
Merikangas, K. R., He, J. P., Burstein, M., Swanson, S. A., Avenevoli, S., Cui, L., et al. (2010). Lifetime prevalence of mental disorders in US adolescents: results from the National Comorbidity Survey Replication–Adolescent Supplement (NCS-A). Journal of the American Academy of Child & Adolescent Psychiatry, 49, 980–989.
Pottick, K. J., Bilder, S., Vander Stoep, A., Warner, L. A., & Alvarez, M. F. (2008). US patterns of mental health service utilization for transition-age youth and young adults. The Journal of Behavioral Health Services and Research, 35, 373–389.
Schulenberg, J. E., & Maggs, J. L. (2002). A developmental perspective on alcohol use and heavy drinking during adolescence and the transition to young adulthood. Journal of Studies on Alcohol, Supplement, 54-70.doi: https://doi.org/10.15288/jsas.2002.s14.54.
Sharp, M. L., Fear, N. T., Rona, R. J., Wessely, S., Greenberg, N., Jones, N., & Goodwin, L. (2015). Stigma as a barrier to seeking health care among military personnel with mental health problems. Epidemiologic Reviews, 37, 144–162.
Sontag-Padilla, L., Woodbridge, M. W., Mendelsohn, J., D'Amico, E. J., Osilla, K. C., Jaycox, L. H., et al. (2016). Factors affecting mental health service utilization among California public college and university students. Psychiatric Services, 67, 890–897.
Spitzer, R. L., Kroenke, K., Williams, J. B., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: the GAD-7. Archives of Internal Medicine, 166, 1092–1097. https://doi.org/10.1001/archinte.166.10.1092
Spitzer, R. L., Kroenke, K., & Williams, J. B. W. (1999). Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. Journal of the American Medical Association, 282, 1737–1744.
Substance Abuse and Mental Health Services Administration (SAMSHA). (2014). Results from the 2013 National Survey on Drug Use and Health: Mental Health Findings, Rockville, MD. 2013 National Survey on Drug Use and Health: Mental Health Findings. NSDUH Series H-49, HHS Publication No. (SMA) 14–4887.
Vogel, D. L., Wade, N. G., & Haake, S. (2006). Measuring the self-stigma associated with seeking psychological help. Journal of Counseling Psychology, 53, 325–337.
Wang, P. S., Lane, M., Olfson, M., Pincus, H. A., Wells, K. B., & Kessler, R. C. (2005). Twelve-month use of mental health services in the United States: results from the National Comorbidity Survey Replication. Archives of General Psychiatry, 62, 629–640.
Zivin, K., Eisenberg, D., Gollust, S. E., & Golberstein, E. (2009). Persistence of mental health problems and needs in a college student population. Journal of Affective Disorders, 117, 180–185.
Funding
Data collection and manuscript preparation was supported by a grant from the National Institute on Alcohol Abuse and Alcoholism (NIAAA) (R01AA022087; PI: Lee). Manuscript preparation was also supported in part through NIAAA F32AA025263 (PI: Cadigan). The content of this manuscript is solely the responsibility of the author(s) and does not necessarily represent the official views of the National Institute on Alcohol Abuse and Alcoholism or the National Institutes of Health.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Cadigan, J.M., Lee, C.M. & Larimer, M.E. Young Adult Mental Health: a Prospective Examination of Service Utilization, Perceived Unmet Service Needs, Attitudes, and Barriers to Service Use. Prev Sci 20, 366–376 (2019). https://doi.org/10.1007/s11121-018-0875-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11121-018-0875-8