
Abstract
Coping Power is an evidence-based preventive intervention for youth with aggressive behavior problems that has traditionally been delivered in small group formats, but because of concerns about potentially diminished effects secondary to aggregation of high-risk youth, an individual format of Coping Power has been developed. The current study examined whether physiological characteristics of the child may provide information about which intervention delivery format works best for that individual. Indicators of sympathetic and parasympathetic nervous system functioning were examined in 360 fourth-grade children (65% male; 76.4% self-reported African-American) who were randomly assigned to Group Coping Power (GCP) or Individual Coping Power (ICP) (Lochman et al. 2015). Longitudinal assessments of teacher- and parent-reported proactive and reactive aggression were collected through a 1-year follow-up. For children with higher initial levels of aggression, those with lower parasympathetic functioning at pre-intervention showed greater reductions in teacher-rated proactive aggression in the ICP condition than the GCP condition. For children with high parasympathetic functioning, there was no differential effect of intervention format. Regardless of intervention format, youth with lower levels of sympathetic functioning at pre-intervention demonstrated greater reductions in teacher-rated proactive aggression. These findings suggest that physiological indicators may be worth considering in future studies examining which youth respond best to specific types of interventions.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Recently, there has been interest in developing personalized approaches to healthcare that take into consideration biological, environmental, and lifestyle factors of the individual. This may lead to more cost-effective interventions that target individuals most in need and their specific deficits. In this study, we assessed biological factors that may influence how youth respond to different types of interventions for aggression, as emerging research suggests that individual characteristics of youth likely influence “what works for whom” (Albert et al. 2015).
Several intervention programs focus on preventing behavior problems in youth (Dodge 2009). However, for most of these programs, effect sizes are modest; although some youth respond well to the interventions, others remain at risk. One factor that may reduce effectiveness for some youth is the group format of the interventions. There are potentially negative effects of aggregating high-risk children into groups because of the opportunity for increased affiliation with deviant peers (Dishion and Tipsord 2011). Involvement with deviant peers increases the risk for adolescent problem behaviors (Dodge et al. 2006). However, delivering interventions in individual sessions is significantly more time-intensive and costly. With limited resources, intervention programs may not be provided to as many youth if delivered individually. Also, some youth do well in group-based interventions and may not need an individual format.
To move toward a precision prevention approach, which involves targeting “precise” groups, we examined biological factors that may predict which children do well in a group intervention and which may benefit more from the individual format. Coping Power is the intervention used in the present study and is a rigorously tested school-based program to address behavior problems in at-risk youth (Lochman and Wells 2002, 2003, 2004). It involves group sessions that take place in schools, separate group sessions for parents, and supports to teachers. Coping Power results in lower rates of substance use and delinquency (Lochman and Wells 2003, 2004), reductions in proactive (i.e., planned, instrumental) aggression, improved social competence, and greater teacher-rated behavioral improvement (Lochman and Wells 2002).
Despite positive effects of Coping Power, it is likely that the group-based format is not effective for all youth. Thus, Lochman et al. (2015) conducted a controlled trial in which youth were randomized to either the group-based Coping Power (GCP) or a version with individually administered sessions (ICP). Although all children showed reductions in teacher- and parent-reported behavior problems at the end of a 1-year follow-up, improvement on teacher-reported outcomes was greater for children receiving the individual version of the program. Furthermore, children in the group condition with lower pre-intervention levels of parent-rated inhibitory control showed less improvement over the course of the intervention (Lochman et al. 2015).
Characteristics of the individual, such as levels of inhibitory control, may help predict which type of intervention would be best for a particular child, thus maximizing the cost-benefit ratio. To date, most studies examining predictors of treatment response have examined family level variables such as maternal depression or behavioral comorbidities. However, numerous lines of research indicate that autonomic nervous system (ANS) functioning is associated with processes that may be key to successful intervention responses, such as self-control, sensitivity to reward and punishment, and responses during peer interactions (Beauchaine 2001, 2015; Erath et al. 2012). Skin conductance level (SCL) and respiratory sinus arrhythmia (RSA) are two indicators of ANS functioning associated with these processes and that may influence responsiveness to the Coping Power intervention. Measurement of SCL and RSA may help determine which intervention format (group or individual) may be most suitable for a child.
SCL assesses sweat gland activity, which is an indication of physiological arousal. Resting SCL is considered a marker of the activity of the sympathetic nervous system (SNS), which mobilizes an individual for “fight or flight” behavior (Beauchaine 2001). Externalizing behavior has been associated with lower levels of SCL (Gatzke-Kopp et al. 2002), particularly when assessed at rest (Lorber 2004).
Low SNS functioning may result in fearlessness, increased sensation seeking (Raine 1993), low levels of inhibition, and low punishment sensitivity (Beauchaine 2001; Matthys et al. 2013), each of which may influence intervention response. Low SNS functioning may particularly predict responses to group-based interventions, as several studies have shown that SNS activity moderates the effects of peer experiences on externalizing behaviors (Gregson et al. 2014; Rudolph et al. 2010). Gregson et al. (2014) found that negative peer experiences were associated with increased rates of parent- and teacher-reported externalizing behaviors only among youth who exhibited lower SCL reactivity. They suggest that lower SNS functioning may reflect fearlessness, which may potentiate retaliatory responses to negative peer experiences and may reflect weaker self-control that could otherwise facilitate more benign interpretations of stressful peer situations. They also suggest that lower SNS functioning may indicate a lack of awareness with peer stress experiences, limiting their ability to learn from problem situations or develop skills to avoid escalating conflicts in the future. Consistent with the idea that SNS functioning may predict responding to group-based interventions, Beauchaine et al. (2015) recently found that lower baseline skin conductance predicted poorer treatment responses to the Incredible Years intervention in preschool children with ADHD. Although the age range is younger than Coping Power, it involved group sessions that included many of the same elements, such as following group rules, identifying/expressing feelings, problem solving, teamwork, and developing social skills. Thus, SNS functioning may be useful in predicting whether an individual will respond well to a group-based intervention or whether an individual format would be more effective.
RSA is an index of parasympathetic nervous system functioning that is considered a valid and reliable peripheral marker of self-regulation (Beauchaine 2015). RSA refers to the ebbing and flowing of heart rate across the respiratory cycle. When measured at rest, higher scores are thought to reflect physiological flexibility and the ability to adapt to environmental stressors (Fabes and Eisenberg 1997). Higher baseline RSA is generally considered adaptive and associated with better emotion regulation (Beauchaine 2001), although excessive RSA reactivity has also been linked with social maladjustment and anxiety (e.g., Gazelle and Druhen 2009). Fabes and Eisenberg (1997) found that higher baseline RSA was associated with less negative emotional arousal in response to stressors and better coping. In preschool children, higher baseline RSA has been associated with better attention regulation in response to angry emotion, higher levels of prosocial behavior (Clark et al. 2016), and better social functioning (Eisenberg et al. 1995). Higher RSA may support calm attentional focus and social engagement (Porges 2007b), which are compatible with sensitive conversational interaction and prosocial problem-solving. In contrast, lower RSA during social interaction is thought to reflect emotional arousal that is less compatible with positive social engagement and more compatible with social disengagement or defensiveness (Erath et al. 2012; Hastings et al. 2008).
Thus, RSA may be an indicator of how youth fare in group-based interventions for several reasons. First, children’s poor self-regulation might augment peer contagion effects that could occur in group interventions (e.g., avoiding situations in which it may be challenging to say “no” is a self-regulation strategy; Dishion and Tipsord 2011). Second, youth with poor self-regulation may be more susceptible to distractions from their peers, which may impede learning in the group. Finally, youth who are less able to cope with negative arousal may be more sensitive to potential provocations from peers, which may affect their ability to positively engage with peers in the group. Thus, RSA may be a biomarker for socioemotional competence that may be useful in determining whether youth would do well in a group-based intervention or not.
One study examined RSA as a moderator of responsiveness to a 22-week school-based intervention for kindergarteners with aggressive behavior (Gatzke-Kopp et al. 2015). RSA reactivity in response to angry and happy film clips was associated with behavioral change over 18 months. The researchers suggest that RSA reactivity can illuminate important individual differences in how children respond under specific emotional conditions that may provide insight into factors that make some children more or less vulnerable. No associations were observed for resting RSA; however, the authors note that associations with resting RSA are less consistent in younger children and that resting RSA may be an emergent property of development (Fortunato et al. 2013).
The goal of the present study was to examine whether pre-intervention levels of SCL and baseline RSA predict responsiveness to Coping Power in the group compared to individual format. Although we recognize the importance of assessing reactivity, only baseline data was available at this time. Given the number relevant relationships with resting measures, we believe these variables are worthy of examination. Based on the findings discussed above, we hypothesized that lower baseline SCL and RSA would be associated with poorer intervention responses, particularly in the group format.
Method
Sample
Children included in the analyses were drawn from a randomized controlled trial (RCT) examining the relative effectiveness of group and individual formats of Coping Power. The RCT involved 360 children recruited from 20 elementary schools. Recruitment involved screening by teachers and parents for eligibility; because teacher screenings have been found to be more predictive of later externalizing problems (Hill et al. 2004), they were considered the primary screening and were more stringent, whereas the parent screening was used to exclude children who showed few signs of aggression in the home setting. Fourth grade teachers completed the Reactive and Proactive Aggression Questionnaire (RPQ; Dodge et al. 1997) on each student in their classrooms. Ratings were compiled across all 20 schools, and a cutoff score corresponding to the 25th percentile was determined, indicating moderate to high levels of aggressive behavior.
A randomized list of eligible children was created for each school, and families were contacted according to their placement on the list. Study procedures were described to families over the phone, and face-to-face assessments were scheduled for interested families. The Behavior Assessment System for Children, Second Edition (BASC-II; Reynolds and Kamphaus 1992) Aggression scale (parent-rated) was the second screening. Children whose parents rated them within the average range or above on the BASC Aggression scale were invited to enroll in the study. Families were contacted and assessed until six children were enrolled at each school. Of the 1131 students eligible from the teacher screening, 499 were successfully contacted. Of those, 139 were excluded because they did not schedule or missed the initial appointment (45), did not pass the parent screening (41), declined to participate (32), moved (15), were a sibling of another participant (three), or had cognitive limitations (three).
Three annual cohorts were recruited, resulting in a total sample of 360 participants. Of those, 94.4% (n = 340) completed the physiological measurements prior to the intervention. Of those, three had data that was unusable due to noise and 87 recording errors that prevented determination of the baseline period. The final sample included 250 participants (125 in GCP, 125 in ICP). Assignment to condition was made at the school level. Schools were paired on demographic factors (percent receiving free or reduced price lunch and percent minority) and, within the pairs, one school was randomly assigned to each condition. There were no differences in proportion of gender, χ2 = 0.01, p = .90, race, χ2 = 0.04, p = .85, or pre-intervention scores on the teacher-rated RPQ screening measure, t(358) = .09, p = .92, between individuals who had usable physiological data and those who did not.
The mean age of the children was 9.72 (SD = 0.62), 64.8% were boys, 76.4% identified as African American, 20% as Caucasian, and 3.6% identified as Hispanic or “Other.” Regarding yearly family income, 12.2% of parents reported none, 21.7% less than $15,000, 30.6% between $15,000 and $29,999, 19.4% between $30,000 and $49,999, and 16.1% greater than $50,000.
Intervention
Coping Power is an evidenced-based manualized intervention (Lochman et al. 2008) designed to target key social-cognitive deficits in children with aggression. It addresses social information-processing distortions (e.g., hostile attributional biases) and deficiencies (e.g., dominance and revenge-oriented social goals; problem solving that relies on direct action strategies rather than verbal assertion or help seeking). It also addresses tendencies to become overaroused, especially when angry, when social problems are perceived. Using cognitive-behavioral strategies, children are taught to use social problem-solving, goal-setting, and emotional regulation skills. The full curriculum includes a parenting component, but it was not implemented in this study. For both ICP and GCP conditions, students attended 32 weekly meetings at school, beginning in the fall of fourth grade and continuing through fifth grade.
Group Coping Power (GCP)
GCP groups included the six children enrolled in the project at each GCP school. Sessions were scheduled for 50–60 min and were co-led by a Coping Power staff member and another clinician (e.g., graduate student, school counselor). Group leaders remained the same throughout children’s involvement in the program. The majority of the groups were mixed gender; two of the 30 groups consisted of all boys. The GCP and ICP curricula covered the same content, though specific activities were tailored for each condition (e.g., children in GCP had opportunities to practice specific skills through role plays with their peers and received feedback from their peers at the end of each session). Children in GCP also participated in monthly individual meetings (approximately nine individual sessions total, lasting 15–30 min each), consistent with the standard Coping Power curriculum, which were included to build rapport, assess comprehension of material, and address individual issues.
Individual Coping Power (ICP)
Children in the ICP condition met one-to-one with a Coping Power staff member for 32 30-min sessions, which included interactive activities (e.g., role plays) between the student and the Coping Power leader, rather than with peers (as in GCP).
Twenty Coping Power leaders were responsible for delivering content, plus several co-leaders. All Coping Power leaders were involved in the delivery of both conditions. Leaders participated in a 6-h initial training and then met weekly for group supervision meetings.
Procedure
Questionnaire Data
Pre-intervention (time 1) measures were completed with children and parents at the time of enrollment. Students and parents completed mid-intervention assessments (time 2) in the summer after fourth grade. Post-intervention assessments (time 3) were completed in the summer after fifth grade. One-year follow-up assessments (time 4) were completed after sixth grade. Most assessments took place in participants’ homes. Children and parents were interviewed separately by research staff members blind to the children’s condition assignment. Parents received $50 for each assessment interview and children received $10. Teachers provided data for times 1, 3, and 4. Teachers received $10 for each student assessed.
Physiological Measures
Physiological measures were collected at pre-intervention (time 1). A BioLog™ recorder was administered to measure heart rate and skin conductance. It was attached to participants through bioelectric and transducer input assemblies. To measure heart rate and interbeat intervals (collected to determine RSA), one electrode was placed above the right collarbone, another behind the left knee, and a reference electrode was placed on the right side of the neck. To measure SCL, electrodes were placed on the volar surface of the distal phalanx of the first and third fingers on the participant’s non-dominant hand.
Following the placement of the electrodes, each participant watched a 3-minute video. The video depicted scenery and was meant to be neutral and unlikely to elicit an emotional reaction. We elected to have participants watch a video rather than sitting quietly because it gave them something to watch and attend to, thus minimizing the likelihood that they would fidget or talk. Baseline RSA and SCL were calculated using data collected during the last 60 s of the video, giving them time to acclimate to the testing equipment.
RSA was derived from techniques in the manual Inter-Beat-Interval Editing for Heart Period Variability Analysis: An Integrated Training Program with Standards for Student Reliability Assessment (Porges 2007a). This manual was designed for use alongside the CardioEdit and CardioBatch computer programs. Porges’ vagal tone method of calculating RSA is empirically supported (Denver et al. 2007; Grossman et al. 1990; Porges 2007b). For a detailed description of the Porges-Bohrer Method, see Lewis et al. (2012). The first procedure involved cleaning interbeat interval data collected using the Biolog. As per procedures outlined in the manual, each participant’s heart rate data was hand edited using the CardioEdit program in order to remove any unwanted artifacts. Artifacts are errors in the interbeat interval data that are likely due to the digitizing process of the data or to physiological anomalies. After data cleaning, RSA was extracted from one of the predominant rhythms exhibited in the data via computations of the participant’s heart period series using the CardioBatch computer software. Mean RSA was quantified for the 60-s baseline period. SCL data was processed using Ledalab. Artifacts were removed and the average SCL over the 60-s period was calculated.
Measures
Reactive and Proactive Aggression Questionnaire (Dodge and Coie 1987; Dodge et al. 1997)
Parents and teachers completed a six-item measure of proactive and reactive behavior. Previous studies have found adequate internal consistency for the RPQ (Vitaro et al. 2006). In the current sample, parent-rated reactive and proactive aggression scales demonstrated Cronbach’s alphas of .71 and .80, respectively; alphas for teacher-rated reactive and proactive aggression were .84 and .88, respectively. The measure includes three items reflecting reactive aggression (e.g., “when this child has been teased or threatened, he or she gets angry easily and strikes back”) and three items reflecting proactive aggression (e.g., “this child threatens or bullies in order to get his or her own way”). Teachers and parents rated each item on a scale labeled “Never True,” “Rarely True,” “Sometimes True,” “Usually True,” and “Almost Always True.”
Analytic Strategy
For this study, a three-level linear growth curve model was constructed by using HLM 7.0 with full maximum likelihood (FML) estimation method (Raudenbush and Bryk 2002). The times of measurement was level 1, individual child characteristics were level 2, and nested within the intervention units (i.e., school) was level 3. The individual growth trajectories were fitted in the level 1 model. Each child’s outcome scores were modeled as a function of time. For teacher outcomes, the data collection dates at each wave were very close in time. Therefore, the time variable for teacher outcomes is 0 as baseline, 1 as post-intervention, and 2 as 1-year-follow-up. For parent outcomes, the data collected with each wave were spread across several months, so we took the actual time interval from baseline as the time variable, with setting baseline to 0. Each of the growth parameters in the level 1 model has a substantive meaning and was estimated in the level 1 model. The intercept was as initial status at baseline. Time slope was the linear change rate over time in each growth trajectory.
At level 2, the person level and child characteristic (gender, race, teacher-rated RPQ screening score, RSA, and SCL) were entered as control variables in the intercept, and child characteristic (gender, race, teacher-rated RPQ screening score, RSA, and SCL, and the interaction terms RSA, and SCL with teacher-rated RPQ screening score) was examined as a potential moderator of the child’s rate of change and effect of intervention on behavior outcomes over time at level 1 model. Child characteristics were group mean centered. The intercept and time slope were treated as random effects at level 2.
ICP and GCP intervention conditions (ICP = 1 and GCP = 0) were randomly assigned to schools, and the school received the same intervention condition in three successive years (cohorts). At level 3, we controlled intervention condition on intercept and detect effects of children’s characteristics on intervention (indicating interactions of intervention and child’s characteristic) on child’s behavior change rate. The intercept was random effect at level 3, and all interaction effects were fixed effects.
The three-level growth curve model captured children’s behavior outcome changes over time in two growth parameters (intercept, time slope), the variation in the growth parameters was partitioned, (a) the variation among children within intervention unit (school) was captured in the level 2 model, and (b) the variation among intervention units is represented in the level 3 model.
For models in which control variables (gender, race, teacher-rated RPQ screening score) were not significant, these variables were removed from final models.
Results
Table 1 provides the means and standard deviations from the behavioral outcome variables and from the physiological variables by intervention condition at each time point. Zero-order correlations between variables can be found in Table 2. Boys and girls did not differ significantly on baseline SCL (t = 1.3, p = .20) or RSA (t = − 1.3, p = .19). RSA values were similar to those found in previous studies using the same method of calculation (Porges et al. 2013; Sijtsema et al. 2011; Vaughan Van Hecke et al. 2009).
We first examined associations between aggression and RSA. RSA was not associated with levels of proactive or reactive aggression at time 1 or with changes in aggression in response to the intervention (with both formats combined) (Table S1). A quadratic relationship was also tested, but this was also not significant for teacher or parent reports (all ps > .29).
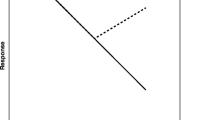
Contrary to hypotheses, we did not find an interaction between time 1 RSA and intervention format in predicting changes in teacher- or parent-rated proactive aggression or teacher-rated reactive aggression. However, RSA interacted with intervention format in predicting changes in parent-rated reactive aggression (Fig. 1). Follow-up growth-curve models were run separately for the individual and group conditions. In the individual condition, youth with lower RSA demonstrated greater reductions in parent-rated reactive aggression (p < .05); the effect size was small, d = 0.34 (median split for RSA). In the group condition, the effect of RSA was not significant, p = .31; however, the effect size was similar, d = − 0.40 but in the opposite direction (median split for RSA). We also ran follow-up models with the sample divided by high and low RSA (median split). The effect of intervention format was not significant for either high RSA, p = .30, or low RSA, p = .18. It should be noted that by arbitrarily dividing groups based on RSA for these analyses and running three-level models involving intervention group, we had less power to detect effects because most of the intervention groups were split (unlike the models divided by intervention format).

Changes in parent-rated reactive aggression from pre-intervention (time 1) to the 1-year follow-up (time 4) for youth receiving the group format (GCP) or individual format (ICP) of the Coping Power intervention. The interaction between intervention format and RSA was significant. The figure depicts individuals the 25th and 75th percentile for RSA
A three-way interaction was observed between time 1 RSA, teacher-rated RPQ screening score (i.e., initial levels of aggression), and intervention format on changes in teacher-rated proactive aggression, p = .021. As shown in Fig. 2, for individuals who had low RSA and high screening scores, those receiving the individual format showed reductions in teacher-rated proactive aggression, whereas those receiving the group format did not. For those with low RSA and low screening scores, there was little difference in responses to the group versus individual format. For youth with high RSA, the patterns of effects looked similar between those receiving the individual and group format. There was a trend toward a main effect of screening score, p = .10, with those who started with higher screening scores showing a greater reduction in teacher-rated proactive aggression than those with moderate screening scores, but there was no interaction between screening score and intervention format, p = .91.

Changes in teacher-rated proactive aggression. There was a three-way interaction between RSA, intervention format, and screening score. For those with low RSA who had higher levels of proactive aggression at baseline (higher screening score), those receiving the individual format showed a reduction in teacher-rated proactive aggression over the course of the intervention whereas those in the group format did not. Although the analyses were conducted on continuous variables, the figure depicts the 25th/75th percentile for screening scores and a median split for RSA. Because all youth were selected for the study based on having high scores on the screening measure, the 25th and 75th percentiles are labeled “moderate” and “high,” respectively
As a follow-up, a direct examination of the effect of intervention format on change in teacher-rated proactive aggression for individuals with high screening scores revealed a significant effect of intervention format on time slope, p < .05. The effect size for the change in time slope (e.g., the change rate) was large, d = − .97. Using the procedures outlined in Preacher et al. (2006) for examining regions of significance in multilevel modeling, we found that for individuals with high RSA and high screening scores, the simple slope of the relationship between time and teacher-rated proactive aggression was significant for all screening scores except for those below the second percentile of the sample. For individual with low RSA and high screening scores, there was no region in which the simple slope of the relationship between time and teacher-rated proactive aggression was significant.
For analyses involving SCL, we found a trend-level association between time 1 SCL and lower levels of teacher-, but not parent-rated proactive aggression at time 1, p = .084 (Table S2). SCL was not associated with teacher- or parent-rated reactive aggression at time 1. Lower time 1 SCL was associated with a greater reduction in teacher-rated proactive aggression over the course of the intervention, p = .024. Time 1 SCL was not associated with changes in teacher-rated reactive aggression or parent-rated proactive or reactive aggression.
Consistent with our hypotheses, a trend-level interaction was observed between time 1 SCL and intervention condition, p = .099; SCL was not associated with response to the intervention in the individual condition, but in the group condition, those with higher pre-intervention SCL showed less of a reduction in teacher-rated proactive aggression. Contrary to hypotheses, there were no interactions between SCL and intervention condition in predicting changes in teacher-rated reactive aggression, or parent-rated proactive or reactive aggression.
Discussion
In this study, we examined pre-intervention RSA and SCL as predictors of response to two formats of an empirically supported intervention. Growth curve analyses indicated that pre-intervention RSA and SCL both were associated with changes in reactive and proactive aggression in response to intervention, but effects were not consistent across parent and teacher raters. For children who started out with particularly high levels aggression, RSA differentially predicted responding to the group versus individual format of the intervention. For children with low RSA, the children with high screening scores receiving the individual format of the intervention showed a significant reduction in teacher-rated proactive aggression, whereas the high-screener children receiving the group-based intervention showed no significant change. For those with high RSA, regardless of initial screening score, there was no differential effect of intervention format. This suggests that for youth with low RSA who are the most aggressive, the individual format of the intervention is more effective than the group format. For those with high RSA, intervention format does not appear to have a differential effect; for youth with high RSA and high initial aggression, a significant reduction in teacher-rated proactive aggression was observed in both formats of the intervention. As noted in the introduction, higher RSA has been associated with better self-regulation, emotion regulation, and better ability to cope with stressors (Beauchaine 2015). One possibility is that within our at-risk sample, children with relatively higher RSA may be less susceptible to peer provocations and/or distractions that occur in the group intervention and thus are able to benefit from the group-based intervention, whereas those with low RSA may have difficulty with distractions and provocations. For individuals with high screening scores and with low RSA, being in the individual format eliminates these challenges.
Another possibility is that for youth with low RSA, poor self-regulation might augment peer contagion effects in the group-based intervention, as individuals with poor self-regulation may have more difficulty resisting peer pressure (Dishion and Tipsord 2011). For example, Goodnight et al. (2006) found that the influence of a deviant friend was moderated by the individual’s ability to inhibit behavior in the context of rewards. In contrast, youth with high RSA may be better able to resist peer pressure in the group format and thus benefit.
Both of these possibilities are consistent with the previous finding that children in the group condition with lower pre-intervention levels of parent-rated inhibitory control showed less improvement over the course of the intervention (Lochman et al. 2015). With the current data, we are not able to determine the mechanism by which low RSA results in poorer performance in the group intervention; future studies examining mediators will be required to clarify this.
The involvement of initial aggression (screening score) in the three-way interaction was not predicted. The interactive effect of RSA and intervention format was only present for youth with high initial levels of aggression. For those with moderate screening scores, there was little change in teacher-rated proactive aggression, regardless of RSA or intervention format. There is some evidence that youth who are higher risk make greater gains in interventions, perhaps because they have larger room for change (Lipsey 2009). Thus, the effects of RSA and intervention format on responding were likely more influential for those with high initial aggression.
Intervention format and RSA also interacted to predict changes in parent-rated reactive aggression, but effects were small. For youth with low RSA, those receiving the individual format showed greater reductions in parent-rated reactive aggression than those receiving the group format. This is similar to the findings for teacher-rated proactive aggression (though not specific to those with high initial levels of aggression), and the same potential explanations listed above likely apply. For youth with high RSA, those receiving the group format showed greater reductions in parent-rated reactive aggression than those receiving the individual format. Although speculative, for youth who are able to better regulate emotions and resist peer pressure, the group-based intervention offers opportunities to practice social skills in a peer setting that may result in benefits that better translate to lasting reductions in aggressive behavior.
Although we observed interactions between RSA and intervention format for proactive and reactive aggression, this was not consistent across parent and teacher raters. Teachers and parents report on behaviors in different contexts. Future research is needed to better understand the different perspectives of teachers and parents in rating changes in their child’s aggression.
Contrary to hypothesis, SCL predicted responding regardless of intervention format. Lower pre-intervention SCL was associated with greater reductions in teacher-rated proactive aggression. SCL did not predict changes in the reactive aggression. Although there was a trend toward an interaction with intervention format for teacher-rated proactive aggression, it may be that SCL is a more general predictor of intervention responsiveness. Contrary to our prediction, youth with higher SCL at pre-intervention did not show as much reduction in teacher-rated proactive aggression as youth with lower SCL at pre-intervention. Although lower SCL is typically associated with higher levels of aggression (Gatzke-Kopp et al. 2002) and is thought to be associated with fearlessness and less sensitivity to punishment (Beauchaine 2001; Matthys et al. 2013), which would presumably diminish intervention responsiveness, research also suggests that overly high levels of SNS functioning are associated with vulnerability to adjustment problems, particularly in negative environments (Abaied 2016; Cummings et al. 2007). Abaied (2016) suggests that overarousal of the sympathetic fight or flight response may be overly taxing on the body, which may diminish available resources for regulating emotions and managing stress. Over the course of the intervention and in the 1-year follow-up, youth are transitioning from elementary to middle school, which is a stress-inducing period. Although speculative, one possibility is that youth with high SNS functioning may become depleted and less able to cope with stress. In contrast, youth with low SNS functioning may be able to disengage. As noted in the introduction, Gregson et al. (2014) suggest that lower SNS functioning may indicate a lack of awareness or engagement with peer stress experiences. Although this is typically thought to limit the ability of youth to learn from problem situations involving peers or to develop skills that help them avoid escalating conflicts with peers in the future, one alternative possibility is that a lack of awareness or engagement with peers may help some youth to avoid conflict and refrain from proactive aggression.
These results suggest that RSA interacted with intervention format, but SCL did not. One possibility is that RSA may predict responsiveness to the intervention format (e.g., sensitivity to the group context), whereas SCL may predict responsiveness to the intervention content.
There are a few limitations to the present study. First, we only examined baseline levels of RSA and SCL. Task-based measures of physiological reactivity may provide important information regarding which youth respond best to the two intervention formats. It is possible that that resting RSA may not be as informative as RSA reactivity in this age group (Gatzke-Kopp et al. 2015). Measuring RSA reactivity under specific conditions relevant to the social behavior (e.g., viewing anger scenes) may provide more information about how children react to specific types of cues. Second, our power for examining gender effects was limited. Although gender was entered into models, the smaller number of females in the sample may have limited our power to detect effects. Furthermore, we were not able to thoroughly examine how having mixed versus same gender groups may have influenced peer group contagion effects. Third, we were not able to examine the mechanisms by which physiological variables may affect responding to the intervention. For example, it is not clear if the lesser reductions in teacher-rated proactive aggression for youth with lower RSA are the result of distraction-related effects or of deviant peer-related effects. Fourth, there were four outcome variables of interest for each of the moderators. Although we did not think that this was enough to warrant correction for type 1 error rate, results should be interpreted with caution, particularly because findings were significant for some of the outcome variables but not others. Finally, although the focus of the present study was on physiological factors, there are other moderators (e.g., social skills) that could also affect intervention responsiveness that are worthy of examination. Future studies examining the relative strength of these factors as predictors will be helpful in determining the most important variables to consider when creating individualized interventions.
In sum, results from the present study provide preliminary evidence that information about RSA may be useful in determining whether group-based interventions would work well for a child—particularly children with higher levels of aggression prior to intervention. Identifying the characteristics of individuals for whom existing interventions are less effective and developing alternative versions that may be more effective for particular individuals is important for improving the overall effectiveness of interventions. Physiological data is relatively easy and inexpensive to collect and therefore may be a measure that can be implemented widely. However, much research, including replication of the current findings, remains to be done before conclusions can be drawn about the role of SCL and RSA in intervention responsiveness.
References
Abaied, J. L. (2016). Skin conductance level reactivity as a moderator of the link between parent depressive symptoms and psychosocial adjustment in emerging adults. Journal of Social and Personal Relationships, 33, 534–556. https://doi.org/10.1177/0265407515583170.
Albert, D., Belsky, D. W., Crowley, D. M., Latendresse, S. J., Aliev, F., Riley, B., et al. (2015). Can genetics predict response to complex behavioral interventions? Evidence from a genetic analysis of the fast track randomized control trial. Journal of Policy Analysis and Management, 34, 497–518. https://doi.org/10.1002/pam.21811.
Beauchaine, T. P. (2001). Vagal tone, development, and Gray's motivational theory: toward an integrated model of autonomic nervous system functioning in psychopathology. Development and Psychopathology, 13, 183–214.
Beauchaine, T. P. (2015). Respiratory sinus arrhythmia: a transdiagnostic biomarker of emotion dysregulation and psychopathology. Current Opinion in Psychology, 3, 43–47.
Beauchaine, T. P., Neuhaus, E., Gatzke-Kopp, L. M., Reid, M. J., Chipman, J., Brekke, A., et al. (2015). Electrodermal responding predicts responses to, and may be altered by, preschool intervention for ADHD. Journal of Consulting and Clinical Psychology, 83, 293–303. https://doi.org/10.1037/a0038405.
Clark, C. A., Skowron, E. A., Giuliano, R. J., & Fisher, P. A. (2016). Intersections between cardiac physiology, emotion regulation and interpersonal warmth in preschoolers: implications for drug abuse prevention from translational neuroscience. Drug and Alcohol Dependence, 163, S60–S69. https://doi.org/10.1016/j.drugalcdep.2016.01.033.
Cummings, E. M., El-Sheikh, M., Kouros, C. D., & Keller, P. S. (2007). Children’s skin conductance reactivity as a mechanism of risk in the context of parental depressive symptoms. Journal of Child Psychology and Psychiatry, 48, 436–445. https://doi.org/10.1111/j.1469-7610.2006.01713.x.
Denver, J. W., Reed, S. F., & Porges, S. W. (2007). Methodological issues in the quantification of respiratory sinus arrhythmia. Biological Psychology, 74, 286–294. https://doi.org/10.1016/j.biopsycho.2005.09.005.
Dishion, T. J., & Tipsord, J. M. (2011). Peer contagion in child and adolescent social and emotional development. Annual Review of Psychology, 62, 189–214. https://doi.org/10.1146/annurev.psych.093008.100412.
Dodge, K. A. (2009). Community intervention and public policy in the prevention of antisocial behavior. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 50, 194–200.
Dodge, K. A., & Coie, J. D. (1987). Social-information processing factors in reactive and proactive aggression in children’s peer groups. Journal of Personality and Social Psychology, 53, 1146–1158.
Dodge, K. A., Lochman, J. E., Harnish, J. D., Bates, J. E., & Pettit, G. S. (1997). Reactive and proactive aggression in school children and psychiatrically impaired chronically assaultive youth. Journal of Abnormal Psychology, 106, 37–51. https://doi.org/10.1037/0021-843X.106.1.37.
Dodge, K. A., Dishion, T. J., & Landsford, J. E. (2006). Deviant peer influences in programs for youth: problems and solutions. New York: Guilford Press.
Eisenberg, N., Fabes, R. A., Murphy, B., Maszk, P., Smith, M., & Karbon, M. (1995). The role of emotionality and regulation in children’s social functioning: a longitudinal study. Child Development, 66, 1360–1384.
Erath, S. A., Tu, K. M., & El-Sheikh, M. (2012). Socially anxious and peer-victimized preadolescents: “doubly primed” for distress? Journal of Abnormal Child Psychology, 40, 837–848. https://doi.org/10.1007/s10802-011-9600-9.
Fabes, R. A., & Eisenberg, N. (1997). Regulatory control and adults’ stress-related responses to daily life events. Journal of Personality and Social Psychology, 73, 1107–1117.
Fortunato, C. K., Gatzke-Kopp, L. M., & Ram, N. (2013). Associations between respiratory sinus arrhythmia reactivity and internalizing and externalizing symptoms are emotion specific. Cognitive, Affective, & Behavioral Neuroscience, 13, 238–251. https://doi.org/10.3758/s13415-012-0136-4.
Gatzke-Kopp, L. M., Raine, A., Loeber, R., Stouthamer-Loeber, M., & Steinhauer, S. R. (2002). Serious delinquent behavior, sensation seeking, and electrodermal arousal. Journal of Abnormal Child Psychology, 30, 477–486. https://doi.org/10.1023/a:1019816930615.
Gatzke-Kopp, L. M., Greenberg, M., & Bierman, K. (2015). Children’s parasympathetic reactivity to specific emotions moderates response to intervention for early-onset aggression. Journal of Clinical Child and Adolescent Psychology, 44, 291–304. https://doi.org/10.1080/15374416.2013.862801.
Gazelle, H., & Druhen, M. J. (2009). Anxious solitude and peer exclusion predict social helplessness, upset affect, and vagal regulation in response to behavioral rejection by a friend. Developmental Psychololgy, 45, 1077–1096. https://doi.org/10.1037/a0016165.
Goodnight, J. A., Bates, J. E., Newman, J. P., Dodge, K. A., & Pettit, G. S. (2006). The interactive influences of friend deviance and reward dominance on the development of externalizing behavior during middle adolescence. Journal of Abnormal Child Psychology, 34, 573–583.
Gregson, K. D., Tu, K. M., & Erath, S. A. (2014). Sweating under pressure: skin conductance level reactivity moderates the association between peer victimization and externalizing behavior. Journal of Child Psychology and Psychiatry, 55, 22–30. https://doi.org/10.1111/jcpp.12086
Grossman, P., van Beek, J., & Wientjes, C. (1990). A comparison of three quantification methods for estimation of respiratory sinus arrhythmia. Psychophysiology, 27, 702–714.
Hastings, P. D., Nuselovici, J. N., Utendale, W. T., Coutya, J., McShane, K. E., & Sullivan, C. (2008). Applying the polyvagal theory to children's emotion regulation: social context, socialization, and adjustment. Biological Psychology, 79, 299–306.
Hill, L. G., Coie, J. D., Lochman, J. E., & Greenberg, M. T. (2004). Effectiveness of early screening for externalizing problems: Issues of screening accuracy and utility. Journal of Consulting and Clinical Psychology, 72, 809–820. https://doi.org/10.1037/0022-006X.72.5.809.
Lewis, G. F., Furman, S. A., McCool, M. F., & Porges, S. W. (2012). Statistical strategies to quantify respiratory sinus arrhythmia: are commonly used metrics equivalent? Biological Psychology, 89, 349–364. https://doi.org/10.1016/j.biopsycho.2011.11.009.
Lipsey, M. W. (2009). The primary factors that characterize effective interventions with juvenile offenders: a meta-analytic overview. Victims and Offenders, 4, 124–147.
Lochman, J. E., & Wells, K. C. (2002). Contextual social–cognitive mediators and child outcome: a test of the theoretical model in the Coping Power program. Development and Psychopathology, 14, 945–967. https://doi.org/10.1017/S0954579402004157.
Lochman, J. E., & Wells, K. C. (2003). Effectiveness study of Coping Power and classroom intervention with aggressive children: outcomes at a one-year follow-up. Behavior Therapy, 34, 493–515.
Lochman, J. E., & Wells, K. C. (2004). The coping power program for preadolescent aggressive boys and their parents: outcome effects at the 1-year follow-up. Journal of Consulting and Clinical Psychology, 72, 571–578. https://doi.org/10.1037/0022-006x.72.4.571.
Lochman, J. E., Wells, K., & Lenhart, L. (2008). Coping power: child group facilitator’s guide. New York: Oxford University Press.
Lochman, J. E., Dishion, T. J., Powell, N. P., Boxmeyer, C. L., Qu, L., & Sallee, M. (2015). Evidence-based preventive intervention for preadolescent aggressive children: one-year outcomes following randomization to group versus individual delivery. Journal of Consulting and Clinical Psychology, 83, 728–735. https://doi.org/10.1037/ccp0000030.
Lorber, M. F. (2004). Psychophysiology of aggression, psychopathy, and conduct problems: a meta-analysis. Pychological Bulletin, 130, 531–552.
Matthys, W., Vanderschuren, L. J., & Schutter, D. J. (2013). The neurobiology of oppositional defiant disorder and conduct disorder: altered functioning in three mental domains. Development and Psychopathology, 25, 193–207. https://doi.org/10.1017/s0954579412000272.
Porges, S. W. (2007a). Inter-beat interval editing for heart period variability analysis: an integrated training program with standards for student reliability assessment. Chicago: The Brain-Body Center at the University of Illinois at Chicago.
Porges, S. W. (2007b). The polyvagal perspective. Biological Psychology, 74, 116–143.
Porges, S. W., Macellaio, M., Stanfill, S. D., McCue, K., Lewis, G. F., Harden, E. R., et al. (2013). Respiratory sinus arrhythmia and auditory processing in autism: modifiable deficits of an integrated social engagement system? International Journal of Psychophysiology, 88, 261–270. https://doi.org/10.1016/j.ijpsycho.2012.11.009.
Preacher, K. J., Curran, P. J., & Bauer, D. J. (2006). Computational tools for probing interactions in multiple linear regression, multilevel modeling, and latent curve analysis. Journal of Educational and Behavioral Statistics, 31, 437–448. https://doi.org/10.3102/10769986031004437.
Raine, A. (1993). The psychopathology of crime: criminal behavior as a clinical disorder. San Diego: Academic Press.
Raudenbush, S. W., & Bryk, A. S. (2002). Hierarchical linear models: applications and data analysis methods (2nd ed.). Newbury Park: Sage.
Reynolds, C. R., & Kamphaus, R. W. (1992). Behavior assessment system for children (BASC). Circle Pines: American Guidance Service.
Rudolph, K. D., Troop-Gordon, W., & Granger, D. A. (2010). Peer victimization and aggression: moderation by individual differences in salivary cortisol and alpha-amylase. Journal of Abnormal Child Psychology, 38, 843–856. https://doi.org/10.1007/s10802-010-9412-3.
Sijtsema, J. J., Shoulberg, E. K., & Murray-Close, D. (2011). Physiological reactivity and different forms of aggression in girls: moderating roles of rejection sensitivity and peer rejection. Biological Psychology, 86, 181–192. https://doi.org/10.1016/j.biopsycho.2010.11.007.
Vaughan Van Hecke, A., Lebow, J., Bal, E., Lamb, D., Harden, E., Kramer, A., et al. (2009). Electroencephalogram and heart rate regulation to familiar and unfamiliar people in children with autism spectrum disorders. Child Development, 80, 1118–1133. https://doi.org/10.1111/j.1467-8624.2009.01320.x.
Vitaro, F., Barker, E. D., Boivin, M., Brendgen, M., & Tremblay, R. E. (2006). Do early difficult temperament and harsh parenting differentially predict reactive and proactive aggression? Journal of Abnormal Child Psychology, 34, 681–691. https://doi.org/10.1007/s10802-006-9055-6.
Funding
This research was supported by grants from NIDA (R01 DA023156) and the National Institute of Child Health & Human Development (R01 HD079273).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
None of the authors except for John Lochman has a conflict of interest. John Lochman is co-developer of the Coping Power program and receives royalties for the implementation guide published by Oxford University Press.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Electronic Supplementary Material
ESM 1
(DOCX 182 kb)
Rights and permissions
About this article

Cite this article
Glenn, A.L., Lochman, J.E., Dishion, T. et al. Toward Tailored Interventions: Sympathetic and Parasympathetic Functioning Predicts Responses to an Intervention for Conduct Problems Delivered in Two Formats. Prev Sci 20, 30–40 (2019). https://doi.org/10.1007/s11121-017-0859-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11121-017-0859-0