
Abstract
Using the 2008 and 2009 Rural–Urban Migration in China (RUMiC) survey data, two waves of a nationally representative survey dataset, this study examined the “healthy migrant phenomenon” with regard to mental health in China. The results show that migrants exhibited better mental health than urban residents did after controlling for variables of socioeconomic status in a regression analysis. The study confirms that the “healthy migrant phenomenon” does exist under the setting of internal rural to urban migration in China, and the socioeconomic status disparities between migrants and urban natives plays a vital role in the phenomenon. Taking advantage of the unique framework of the RUMiC survey data, we were able to use not only the samples of migrants and urban residents but also those of rural residents to assess the potential channels further. Our results provide some suggestive evidence that self-selection effect and “salmon effect” are possible mechanisms causing this phenomenon.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The rapid economic growth of China has resulted in a historically unprecedented surge in urbanization. Increasing numbers of rural inhabitants have joined this exodus to the cities in search of an improved quality of life. According to the National Bureau of Statistics, in 2015, rural–urban migration in China involved approximately 278 million people (including migrant workers, who numbered 169 million), which may constitute the most massive migration in the history of humankind (Meng et al. 2010).
Chinese rural–urban migrants are usually engaged in 3D (i.e., dirty, dangerous, and demanding) work that urban residents are seldom willing to perform. They often work more extended hours at a high intensity and with less protection than native residents do, while they frequently live in worse conditions and have less support from their families (Meng et al. 2010). These factors significantly increase the risk of rural–urban migrants becoming sick while living in cities. Moreover, due to the discrimination involved in the “hukou” household registration system, rural–urban migrants are often systematically excluded from urban public resources, one of which is access to healthcare. Consequently, rural–urban migrants receive less coverage under formal medical schemes and encounter more barriers when applying for reimbursement of treatment expenses, even if they have specific insurance (Hu et al. 2008).
Although migrant workers face a higher risk of poor health and lower chance of accessing and affording treatment, studies face challenges when asserting that the health status of the migrant workers is worse than that of urban residents. Indeed, most studies have found that migrants exhibit better health than urban natives because young, healthy individuals having a higher capability and propensity to migrate. The “healthy immigrant effect” (henceforth referred to as the HIE) is a well-established phenomenon in the field of international migration, which describes the observation that immigrants are generally healthier than natives (Antecol and Bedard 2015).Footnote 1 A more nuanced definition includes a second aspect: after immigrants move to their new country of residence, the health advantage gradually deteriorates (Aglipay et al. 2013) in what referred to as the years since migration (henceforth referred to as the YSM) effect (McDonald and Kennedy 2004).
Numerous empirical studies have investigated the effects of HIE and YSM in the international migration context. Most of them inevitably come from developed countries, since they are the countries receiving the most immigrants. For developing countries, especially for the vast countries such as China, internal migration is often from rural to urban areas rather than the immigration patterns. Accordingly, some researchers have sought to determine whether internal migrant workers are healthier than urban residents and whether this health advantage deteriorates over time in ChinaFootnote 2. However, most studies have mainly focused on self-reported health or physical health indicators, such as diseases and disability (Tong and Piotrowski 2012), while the mental health status of migrant workers has been paid less attention.
Intuitively, it may be predictable that the healthy migrant effect is evident among Chinese rural–urban migrants according to measures of self-evaluated or physical health. After all, in most cases, people who choose to migrate have better health or exhibit a positive outlook about their health. However, in the context of mental health, the scenario may differ substantially. Migrant workers who work in unfamiliar environments without the company of family members may feel lonely and anxious. Moreover, rural to urban migrant workers who perform low-skilled tasks may commonly be discriminated against by native residents. Therefore, they may tend to have more anxiety disorders, depression, and low self-esteem than urban native residents, although they are physically healthier. Hence, the evidence of the healthy migrant phenomenon regarding physical health in China may not apply to mental health. This association needs to be empirically tested, preferably using national-representative survey data; therefore, the original motivation of this research was to focus on the mental health of rural to urban migrants in China.
Furthermore, China is undergoing a period of epidemiologic transition: the reason for most deaths in recent decades is noncommunicable instead of infectious disease, and with the rapid development of industrialization, some health problems have emerged, for instance, mental health disorders (Lu et al. 2012). The mental health problem of migrant workers is a crucial issue of immediate significance.
Therefore, in this study, we first contribute to the literature by using more representative nationwide survey data focused on rural–urban migrants in China, the Rural–Urban Migrants in China (RUMiC) database, to explore the HIE in regard to mental health in China.Footnote 3 Our results show that the mental health level of migrant workers is better than that of native urban residents based on the regression analysis controlled for individual characteristics. This is consistent with the stylized facts of the HIE, as we mentioned.
Second, due to the unique data framework of the RUMiC database, we were able to use not only the samples from the Rural-to-Urban Migrants Survey (UMS) and the Urban Household Survey (UHS) but also that from the Rural Household Survey (RHS), which allowed us to assess potential channels of the healthy migrant phenomenon. Concretely, we classified rural samples in the RHS into three categories: (1) people who have never migrated, (2) people who have returned to their hometown, and (3) people who had jobs in urban cities but were temporarily living in a rural area during the survey fieldwork period. Consequently, we were able to discuss the mechanisms of self-selection by migrants and the “salmon effect”, as well as the measurement of the healthy migrant phenomenon itself. We found a substantial, significant self-selection effect and a weaker, insignificant “salmon effect” as possible mechanisms causing this phenomenon.
Finally, we determine that the socioeconomic status (SES) disparity between migrants and urban natives plays a crucial role in whether a healthy migrant effect on mental health exists in China. For the segmentation of the hukou household registration system in China, migrant workers possessed relatively lower SES as measured by household income, educational attainment, and job characteristics than their urban counterparts, which drastically impaired their health status.
Conceptual Background and Literature Review
HIE Framework: From International Immigration to Internal Migration
As mentioned earlier, the health immigration effect (HIE) describes a phenomenon in which immigrants are generally healthier than natives. Two concepts of defining the HIE are commonly found in the literature. One involves directly comparing the mean of the health outcomes between natives and immigrants, which is also called the “unconditional” HIE (e.g., Gotsens et al. 2015; Kwak and Rudmin 2014). The other is based on multiple regression analysis and expresses the HIE as “immigrants are healthier than their native counterparts” (e.g., Antecol and Bedard 2015). The word “counterparts” reminds us that the latter definition requires controlling for covariates, such as demographic variables, work, income, and education.
There is a large body of literature about the HIE in immigration studies. Researchers often compare the health of immigrants to that of natives at the destination in terms of various indicators of health status for most developed countries, including the US, Canada, Australia, the UK, Germany, Sweden, and others, which are often the most major immigrant-receiving countries.Footnote 4 Moreover, most studies, whether unconditionally comparing or conditionally comparing the mean of health outcomes, provide some evidence that HIE does exist, which means that immigrants are both conditionally and unconditionally healthier than native residents.
However, only a few studies have been performed concerning internal migration; most are conditional comparisons. For example, examining the economically motivated movement from rural to urban areas in Indonesia, Lu (2008) applied the HIE to internal migration and determined that the migration process is complex and diverse while the healthy migrant phenomenon does exist in Indonesia. Subsequently, Lu (2010) used the Indonesian Longitudinal Data for 1997 and 2000 to examine the YSM effect of rural–urban migration on physical and mental health. She concluded that migration has little impact on physical health for several years but that the YSM effect does apply to mental health among migrant workers in Indonesia.
Some scholars have also used the HIE to explore the problems faced by rural to urban migrants in China. For instance, using the data from CHNS (China Health and Nutrition Survey), Tong and Piotrowski (2012) suggested that, in terms of self-reported health, high blood pressure, heart disease, and ADLs (activities of daily living), migrants are generally healthier than native residents. Niu (2013) also analyzed aspects such as self-reported health, chronic diseases and disability and identified the health advantage of migrant workers over native urban residents in China by using data from the third issue of the Chinese Women’s Social Status Survey. In other words, she confirmed the existence of HIE in China as well. Meanwhile, she found that migrants who eventually returned to their hometown had worse health conditions than the rural residents who never migrated, which supports the theory of the YSM effect. Using data from the eight district migrant workers survey in Beijing, Yuan (2009) revealed the diminishing health situation of migrant workers after their immigration and the formation of the vicious cycle of decreasing health status and decreasing income, both of which support the existence of the YSM effect. Utilizing the 16-province tracking data from the ministry of agriculture fixed observation points of China, Qin et al. (2015) also showed similar results. Furthermore, Zhou and Lu (2016) demonstrated that the YSM effect exists among manufacturing and construction workers more often than it does among those in white-collar jobs, such as administrative, technical, management and service jobs.
In summary, numerous studies on the healthy migrant phenomenon in China have investigated self-reported health and physical health, whereas evidence concerning mental health is relatively limited.
Mechanisms of the Healthy Migrant Effect
Many previous studies have provided three potential channels to explain why the HIE exists in China (Chen 2011).
Health Care Access and Health Behaviors
Studies have indicated that barriers to health service access result in immigrants obtaining relatively less information concerning diseases that they have, thereby causing them to provide relatively high ratings of their health condition, which can result in overestimation of subjective health indicators of the HIE (McDonald and Kennedy 2004). However, empirical conclusions regarding this mechanism are unclear because some studies have reported that increasing health care access can effectively improve health levels. Immigrants commonly have less access to public medical care systems, which may impair health and reduce HIE further. Hence, the influence of medical factors on HIE is hard to determine (Antecol and Bedard 2015). In addition to the healthcare mechanism, health behaviors may play another potential role in explaining HIE (Kennedy et al. 2015). For example, a healthy premigration lifestyle may have involved high levels of physical activity and low-calorie diets. These health behaviors are more conducive to a better health status.
Selective Migration Effect
In most cases, migrants tend to be healthier people. Therefore, new immigrants enjoy a health advantage over native residents. This mechanism can account for the HIE among domestic migrant workers in China: healthy rural residents tend to migrate for work (Tong and Piotrowski 2012; Zhou and Lu 2016). In international migration, another mechanism affects potential migrants, namely, the immigration screening processes of host countries can reject applicants with relatively inferior health. Although this mechanism does not exist for internal migrants in China, strict household registration policies can be considered a form of migration screening and allow only relatively privileged migrant workers being permitted to settle; these strict registration policies are enforced in megacities such as Beijing and Shanghai and force unhealthy migrant workers to return to rural areas. This strict household registration policy can also explain the third HIE mechanism, namely, the “salmon effect”.
Salmon Effect
The term is used to describe the patters that immigrants who are relatively less healthy are more likely to return to their country of origin; consequently, the average health condition of immigrants in the host country is superior. However, the empirical results are mixed. Fong (2008) reported that Chinese sojourners in the United Kingdom and Ireland returned to China because of personal or familial health crises. Van Hook and Zhang (2011) determined that immigration was less strongly associated with health in the United States. Nevertheless, we contend that the “salmon effect” can explain the healthy migrant phenomenon in China. For example, Niu (2013) reported that migrant workers who returned to rural areas were less healthy than those who did not. Moreover, Zhou and Lu (2016) stated that “migrant workers devoted themselves to the development of the city, but when they become less healthy, the city was unwilling to accept them and pushed them back to rural areas.”
Healthy Migrant Effect and Mental Health
Relative to studies using physical health as the primary outcome variable, few have been conducted on the HIE and mental health. Alegria et al. (2008) and Cook et al. (2009) have assessed that Latino immigrants in the United States exhibit a lower risk of developing psychiatric disorders than do US-born Latino immigrants. Similarly, adopting psychiatric disorders and anxiety disorders as indicators to measure mental health, Menezes et al. (2011) and Aglipay et al. (2013), respectively, confirmed that the HIE is evident in Canada. Rivera et al. (2016) used the GHQ-12 questionnaire as an indicator of psychological well-being and revealed that a group who migrated to Spain less than 10 years prior exhibited better mental health. They also observed no HIE in the group who had migrated more than a decade prior, which supports the existence of the YSM effect. Bergeron et al. (2009) reported that immigrants in Canada suffered diminishing mental health because of cultural, language, and climate-related problems that had occurred following migration. Straiton et al. (2014) indicated that men from non-English speaking backgrounds were exposed to an increased risk of mental health problems, which also verified the action of the YSM effect on mental health.
Compared with the studies above, the mental health of Chinese rural to urban migrants has received less attention. To the best of our knowledge, only Wen et al. (2010) and Chen (2011) used data from Shanghai and Beijing, respectively, to study the healthy migrant phenomenon in relation to mental health in China. They presented mixed and inconsistent pieces of evidence. Wen et al. (2010) confirmed the healthy migrant phenomenon impact on mental health by using survey data that only covered Shanghai, whereas Chen (2011) reported the opposite results by using survey data solely from Beijing. The contradictory conclusions reflect not only a considerable heterogeneity between the two different regions of China but also unusually insufficient evidence of the phenomenon regarding mental health.
Data, Methods, and Variables
Rural–Urban Migration in China (RUMiC) Survey Data
This study used data from the RUMiC survey, which implemented a stratified sampling method using random mapping to conduct detailed investigations of five thousand rural–urban migrant families in fifteen large and medium-sized cities in China. The survey obtains individual and family characteristics, including occupation, income, consumption, and daily routine. In addition to information about the migrant families, it also obtains data from samples of five thousand urban residents in the fifteen cities above and eight thousand rural residents in ten provinces. Thus, the RUMiC survey data comprise three datasets: the “Rural-to-urban Migrants Survey (UMS)” dataset, the “Urban Household Survey (UHS)” dataset, and the “Rural Household Survey (RHS)” dataset.
We use the pooled cross-sectional data of the RUMiC 2008–2009 data, which covers the years 2007 and 2008. The advantages of the RUMiC survey are as follows: (1) It focuses on rural–urban migration issues, and its purpose corresponds to that of this study. (2) The data sampling method is distinct from those of previous surveys of migrants in that it applies both workplace and place of residence to determine the sampling frame. Therefore, we were able to include migrant workers who live at their workplace, who have typically been omitted from previous surveys. (3) More importantly, the data include native urban residents, migrant workers, and rural residents based on a nationally representative sample.
Methods
This study measured the healthy migration phenomenon by comparing migrant workers (from the UMS dataset) with urban residents (from the UHS dataset). We evaluated the healthy migrant effect through an ordinary least squares regression model. Our baseline estimating equation was as follows:
where mhidt represented the level of mental health of individual i in area d at year t. Migidt indicated whether the individual is a migrant worker (1 = migrant worker, 0 = urban resident). X′idt represented a series of control variables. Did and Tit represented the region fixed effect and the year fixed effect, respectively. μidt was the error term. In particular, β was the critical coefficient of concern, representing the coefficient of the healthy migrant effects.
Equation (1) was not only used for the basic framework but was also adapted for subsequent analysis of the mechanisms. To analyze the selective migration effect and the “salmon effect”, we classified samples in the RHS into three groups: (1) rural residents who never had any migratory experiences and continuously lived in rural areas; (2) migrant workers who had migration experiences but who returned to their rural hometowns in the relevant year; and (3) migrant workers who were temporarily living in the city during the period when the survey was conducted. These groups were referred to as nonmigration residentsR, return workersR, and migrant workersR, respectively. The superscript R represents that all three above are subsets among the RHS dataset.
Specifically, we used two different samples for the comparison in Eq. (1). The first was composed of migrant workers (from the UMS) and native urban residents (from the UHS) and was used to measure the healthy migrant phenomenon. Second, to assess the selective migration effect, we used the nonmigration residentsR, migrant workersR, and return workersR samples to determine the “salmon effect”. Therefore, the study not only analyzed the healthy migration phenomenon but also attempted to explore the mechanisms behind the phenomenon; it may provide a more comprehensive conclusion than many other studies regarding the HIE, particularly those focused on rural–urban migrants in China.
We used the RHS sample to evaluate selective migration effect and “salmon effect” rather than comparing migrant workers (from the UMS) and rural residents (from the RHS) for the following reasons: (1) Taking the mobility patterns of rural to urban migrants into account, the sampling design of the UMS and UHS in the RUMiC was different from that of RHS in RUMiC. The samples of the UMS and UHS were derived from fifteen cities located in more coastal areas and were intended to be representative of the host places of migrants. In contrast, the RHS was chosen from rural areas in ten provinces and was designed to be representative of the source places. (2) Migrant workers in the UMS dataset were surveyed in fifteen cities and originated from all regions of China, whereas the rural residents in the RHS dataset originated from only ten provinces as sources. Therefore, comparing the samples from the UMS and those from the RHS is inappropriate for discussing the selective migration effect and the “salmon effect”. Although the urban residents in the UHS dataset originated from only fifteen cities, we were still able to compare them with migrant workers in the UMS from the entire country because of the definition of the HIE. (3) We chose GHQ-12 as the proxy of mental health, which is a subjective index. However, Chinese people living in different circumstances (urban area vs. rural area) may use different criteria when assessing their subjective health conditions because they face different reference groups (Mu 2014). Therefore, compared migrant workers and urban residents to measure the healthy migrant effect because they were all investigated in the same urban cities at almost the same time. However, when we examined the selective migration and the salmon effects, samples that were all investigated in the rural areas were more suitable.Footnote 5
To illustrate the samples used in this paper more clearly, we present some details of the data in Table 1.
Key Variables
Different studies have used different indicators, such as psychiatric disorders (Cook et al. 2009; Menezes et al. 2011), anxiety disorders (Aglipay et al. 2013), and psychological distress (Chen 2011), to measure the status of mental health. Following the examples of Rivera et al. (2016) and Gotsens et al. (2015), we adopted the GHQ-12 questionnaire as a comprehensive indicator of mental health. GHQ-12 consists of 12 items with a 4-point Likert-type scale (ranging from 0 to 3). The score is used to generate a total score ranging from 0 (most healthy mental state) to 36 (least healthy), which is one of the most extensively used indexes for measuring common mental disorders. Its application in empirical research is well documented in various countries and various types of populations (Rivera et al. 2016). Therefore, we used the GHQ-12 questionnaire as the dependent variable to assess overall mental health level.
We also used other variables such as household incomes per capita, years of schooling, employment, ownership and contract type of employment, and occupation as control variables to evaluate the SES of the individuals. Additionally, demographic variables (gender, age, and ethnicity) were also controlled. We limited our migrant sample to individuals who were 18–60 years old, had a rural hukou and were engaged in “seeking a job and doing business” in cities. Table 2 provides the necessary information on these migrants as well as their counterparts in the cities and the native urban residents.
Table 2 shows that the mean GHQ-12 scores for migrant workers and native urban residents were 7.589 and 7.481, respectively. The mental health level of migrant workers was worse than that of native urban workers (significance level: 10%). This result appears to cast doubt on the existence of the HIE. However, when we compared the other variables in Table 2, we found that migrant workers were more likely to be male and younger (approximately 10 years) than the natives.
Moreover, migrants were also much lower than urban residents in terms of household income per capita, education level, shares of employment in the state sector and permanent contracts. Columns (5) and (6) in Table 2 present raw the differences and standard errors of these variables, respectively, by a t test of the mean differences between the two groups. Most values of the mean differences in these variables are significant at the 0.1% significance level. In other words, migrant workers and urban residents were, to some extent, two distinct groups competing in a segmented labor market. This indicates that we should control these significant covariates to make the comparison of migrants and urban residents comparable when studying the healthy migrant phenomenon in China.
Results
Main Findings of the Healthy Migrant Effect
Table 3 presents the multiple regression results according to Eq. (1). The baseline regression only included essential demographic characteristics, such as age, gender, and ethnicity, as well as the year and province dummy variables (Model 1). The result indicates that the migrant workers’ mental health was significantly worse than that of urban residents. This means that when we only matched on demographic characteristics, such as gender, age, and minority, plus a controlling year and region dummy variables, migrant workers’ mental health levels were significantly inferior to those of urban residentsFootnote 6.
Then, we gradually added some “conventional” controlling variables to the baseline regression (Model 1). At first, when the income variable was added, the key coefficient declined from 0.528 to 0.362, which reflects that migrants have much lower income than urban residents and income was positively associated with mental health (Model 2). Then, when we further controlled the education level, the result was reversed; the sign of the coefficient turned from positive to negative. This means that migrant workers’ mental health was significantly better than that of urban residents (Model 3).
In other words, when we matched the two groups and compared people with identical demographic characteristics, year, region, income level, and education level, the stylized fact of a healthy migrant effect appeared. In turn, when we did not control the income variable and education level, the migrant workers’ mental health was worse than that of urban residents because the income and education of the migrant workers were much lower than in urban residents.
To yield a deeper understanding of the healthy immigration effect, we gradually added more variables about employment, such as the status of employment and other job characteristics, if the respondent was employed. This specification allowed us to examine the effects of income, education, employment, and job characteristics separately so that we could understand the healthy migration effect better by pinpointing which aspect of SES was vital in explaining the mental health difference. As shown in Model 4, when employment status is added to the regression model as an control variable, the absolute value of the critical coefficient barely changed (from − 0.235 to − 0.232). That means that employment status could explain almost nothing. However, when we added detailed job characteristics, the critical coefficient turned from − 0.232 to − 0.342 (Model 5). This indicates that migrant workers engaged in different types of work than the urban residents, which tended to hurt the mental health of migrant workers. Additionally, from the changing magnitude of the critical coefficients between the five models, we can see that income and education played a relatively substantial role in explaining the reversal of the results.
In summary, the results reveal that migrant workers’ mental health is significantly superior to that of urban residents if we control the SES variables. Then, one may ask why the descriptive statistics showed that migrant workers’ mental health was worse. The results from the regression analyses suggest that it is because migrant workers and urban residents are two distinct groups with significant disparities in SES. The migrant workers possessed relatively inferior SES, which was negatively related to their mental health; thus, the stylized fact of healthy migrant effect—migrant workers exhibiting a better average mental health level—appeared only after equally controlling for SES.
Robustness Check
The Order of Inclusion of Controlling Variables
Our previous analysis is based on a stepwise regression method.Footnote 7 However, caution should be exercised in drawing inferences about the importance of particular covariates in relation to mental health based on the stepwise type of approach. In other words, the order of adding variables into the regression may matter for the result.
To test the robustness of our analysis in the last section, we tried five different orders of inclusion, which specifically changed the order of three important variables, education, income, and job information, and re-estimated the model to see if the results changed substantially. The results are shown in the Online Appendix Table 2. As we can see from the table, the basic pattern shown in Table 3 is relatively robust; both results present the fact that the sign of the coefficient was positive at first, then as we added more controlling variables, the sign eventually became negative, no matter which orders we chose.
The Nonlinear Estimation Model
Another concern about our results is the specification of our estimation model. As we introduced, the dependent variable was the mental health measured in the GHQ-12, which consists of 12 items with a 4-point Likert-type scale (ranging from 0 to 3). The score range from 0 (most healthy mental state) to 36 (least healthy), for which the value is always a nonnegative and integral. This indicates that our linear estimation model may be overly restrictive.
Taking the possible nonlinear relationship between mental health and migration status into account, we also used a negative binomial regression model, which is often applied to count outcomes, to re-estimate the model as a robustness check. The results are shown in Online Appendix Table 3. The sign, magnitude, and significance of the estimate coefficients in the table are similar to those in Table 3, which proves that the specification of our model did not substantially change the results.
The Restriction of Recent Migrant Workers
Ideally, health status should be observed at the time of migration when measuring the healthy migration effect, since the time after movement could lead to possible health changes arising from migration. Namely, the YSM effect may confound the comparison between migrant workers and urban residents. Therefore, we restricted the sample of migrants to the recent migrants as a robustness check.
We generated a new variable, “YSM”, which we defined as the number of years since the migrant workers came to the city. Then, we repeated the same stepwise regressions as in Table 3 but restricted the migrant sample to YSM ≤ 3 years, YSM ≤ 2 years, and YSM ≤ 1 year separately. As shown in Table 4, the coefficients are only slightly higher than those in Table 3, which means that recent migrants suffered worse mental health than permanent migrants. In general, the results are consistent with the main findings in Table 3.
Potential Mechanisms of the Healthy Migration Effect
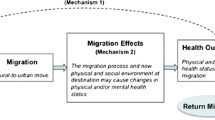
Since we have confirmed that the mental health level of migrant workers in China is consistent with the stylized facts in the HIE, after controlling the SES characteristics, the next question is what are the mechanisms behind the HIE phenomenon? As summarized in the literature review section, three channels behind the healthy migrant effect have been presented thus far: health care access and health behaviors, the self-selection effect, and the “salmon effect”.
Mechanism 1: Health Care Access and Health Behaviors
To identify the effect of health care access and health behaviors on HIE, we incrementally put more variables, which can be seen as the proxies of health care access and health behaviors, into the regression equation (presented in Model 5 of Table 3). The results are shown in Table 5.
First, we added the variables “health care expenditure over the last 3 months” and “whether you have health insurance” as proxies for health care access to assess this mechanism. We adhered to the concept that a newly added variable is the pathway variable for explaining the healthy migrant phenomenon if the magnitude and significance of the coefficient of the migrant worker’s variable declines after the new variable is added (Cutler and Lleras-Muney 2010). After the two variables were added, the coefficient of the migrant effect became − 0.299 (Model 6), which was not considerably different from the result presented in Model 5 of Table 3 (− 0.342). In other words, the health care factor only explained a small share, which is 14.4% ((0.299–0.342)/0.299 = − 14.4%), of the healthy migration phenomenon mechanism.
Considering that “whether you have health insurance” may be insufficient to describe the social benefits in the medical service gap between the two groups, we added the logarithmic reimbursement variable, which was the amount of medical treatment or expense covered by any social insurance in the last year. The results are presented in Model 7, which exhibit minimal change compared with Model 6. As stated, health care access has both positive and negative effects on individuals’ subjective health levels. Consequently, the effect of healthcare on HIE is challenging to determine (Antecol and Bedard 2015). In this study, we could not identify whether health care access had no effect at all or whether the positive and adverse effects offset each other.
Finally, we added smoking habits and the prevalence of obesity (body mass index, BMI ≥ 28) as a proxy for health behaviors (Kennedy et al. 2015).Footnote 8 As shown in Models 8 and 9, the key coefficients changed slightly. Interestingly, the coefficients of smoking and obesity were all negative, which means they were related to better mental health. The unexpected signs for smoking and obesity could indicate that smoking and obesity damage physical health; however, they may improve one’s mood, thereby enhancing mental health.
The health care expenditure over the past 3 months not only measures the supply of healthcare services to some extent but also undoubtedly reflects the demand for healthcare services; hence, it is going to be directly related to mental health status. To see if our results are robust, we dropped the health care expenditure variable and re-estimated the model. As shown in Model 10 and Model 11, the results were similar to the previous ones, which means that our results were immune to the potential endogeneity of health care expenditure.
In summary, our study does not yet indicate that health care access and health behaviors are potential mechanisms for explaining the role of mental health in the healthy migrant phenomenon in China. Nevertheless, we should note that the variable “health care expenditure over the last 3 months” contained only general medical information and that the RUMiC data lack more specialized psychological and medical information related to mental health, as well as the distant between the residence and the nearest the health care facilities, which may also affect the health status of migrant workers. Therefore, the relationship between health care access and the healthy migrant phenomenon requires further analysis.
Mechanism 2: Selective Migration Effect
This study also investigated the selective migration effect and “salmon effect”. First, we compared samples of migrant workersR and nonmigration residentsR to examine the selective migration effect; the regression results, presented in Column 1 of Table 6, indicate that migrant workersR had a lower risk of developing mental health problems than nonmigration residentsR did; this difference passed the 5% level of the significance test. Hence, the selective migration effect was supported.
As a supplementary statement, the coefficients of other controlling variables mostly adhered to our intuition: the young, employed individuals with higher incomes and higher education exhibited significantly superior mental health.
Mechanism 3: “Salmon Effect”
To investigate the “salmon effect”, we ran a regression similar to the one in the previous subsection but only used the migrant workerR and return workerR samples at first. As shown in Column 2 of Table 6, migrant workersR exhibited insignificantly superior mental health levels compared to return workersR. This indicates that the “salmon effect” exerted a weak impact on the healthy migration phenomenon for migrant workers’ mental health in China. The result seems to correspond to some empirical evidence on international immigrants. That is, the effect of the salmon mechanism was relatively weaker than the effect of the selective migration effect (Van Hook and Zhang 2011). There are two opposite views to explain why migrant workers return to their hometown: worsening health conditions and familial reunion.
To estimate the selective migration effect and the “salmon effect” simultaneously, we also pooled all samples including the migrant sample, the nonmigrant sample, and the return migrant sample together and ran a new regression with two dummy variables that represented nonmigrant residents and return workers. The results are presented in column 3 of Table 6. We can see that the magnitude and significance of the two coefficients are very similar to the results from separate samples in the previous columns.Footnote 9
In summary, a selective migration effect and a relatively weaker “salmon effect” are found on the mental health of migrant workers in China. Our suggestive evidence derived from comparing urban residents and rural–urban migrants who have already self-selected to migrate to cities coincides with findings reported in the literature on the healthy migrant phenomenon. Therefore, we conducted a regression analysis under the control of individual characteristics, and we obtained results indicating that the mental health of migrant workers was better than that of urban residents. However, owing to the more inferior socioeconomic status of the migrant workers, their mental health status is worse than others when we did not control the SES.Footnote 10
Discussion and Conclusion
Using a nationwide representative dataset, RUMiC 2008 and 2009, this study examined the relation of the healthy migrant phenomenon with mental health in China. Our results confirmed that HIE does exist under the setting of internal rural to urban migrants in China and found that socioeconomic status disparities between migrants and urban natives plays a vital role in the phenomenon. In addition, we provide some suggestive evidence that self-selection and the “salmon effect” are potential mechanisms in explaining the healthy migrant phenomenon in China.
Our findings on mental health correspond to the evidence presented in the literature on the HIE. However, if SES factors are not controlled, migrant workers possessed inferior mental health conditions due to their inferior SES. The evidence reflects the severe disparity in social and economic characteristics between urban residents and rural residents; this can be attributed to the systematic discrimination involved in the “hukou” household registration system.
It is well known that the household registration system in China divides people into two distinctly different identities, “agriculture population” (rural hukou) and “non-agriculture population” (urban hukou). For a long time, people could not change their identities from one to another, except by several channels, such as going to college, joining the military, or having a marriage across the rural and urban divide. This meant that a person who had no “urban hukou”, even if he or she is living and working in a city, could not enjoy the social benefits in education, medical services, and social security that urban residents had.
Due to the discrimination involved in the “hukou” system, rural to urban migrants are often systematically excluded from urban public resources, one of which is access to healthcare (Gong et al. 2012). One reason is that the basic health insurance schemes used to be divided by “hukou”, Urban Resident Basic Medical Insurance (URBMI) for urban residents and the New Rural Cooperative Medical Scheme (NRMS) for rural residents, causing extensive fragmentation in the health insurance system. The identity-based schemes limit migrants’ access to healthcare services in their job locations because it is difficult for them to use a specific health insurance account across regions or schemes. In addition, the reimbursement levels and benefits packages differ among regions, and the separate operation mechanisms and different administrative institutions lead to weak interconnections within the system, thereby causing significant inequity issues for migrants (Shan et al. 2018). Migrants receive less coverage under formal medical schemes, and they encounter more barriers when applying for reimbursement of treatment expenses (Hesketh et al. 2008). As a result, they consistently underuse health services in their destination cities, causing potential short-term and long-term health problems (Mou et al. 2009). In this way, the migrant workers’ health advantage gradually deteriorates after migrants move to a new place of residence (Aglipay et al. 2013).
Several limitations of this study must be noted. First, the conclusions of our study are primarily descriptive and illustrative and do not represent canonical causal effects. Second, due to lacking detailed medical information and the data compatibility issue in RUMiC, our result about potential mechanisms for explaining the role of mental health in the healthy migrant phenomenon in China may be not conclusive. Finally, this study involves no panel data, so we could not examine mechanisms such as premature death (Antecol and Bedard 2015) and the dynamic YSM effect. Therefore, the mechanisms we proposed represent suggestive evidence rather than solid causal evidence. These limitations motivate us to address these shortcomings in our future research.
Notes
Because internal migrants are substantially different from immigrants, this paper references Chen (2011), who referred to the healthy immigrant effect as the healthy migrant effect/phenomenon. Some studies have used the term healthy migrant hypothesis (Tong and Piotrowski 2012). In our paper, we treat these as identical items and apply them according to the context.
We provide a detailed summary of the literature in “Conceptual background and literature review” section.
In this paper, we concentrate our discussion on the first aspect of the HIE based on the following reasons: First, we were concerned about distraction and divergence from the main points in our study if we added a more formal discussion about the YSM effect in the manuscript. Second, our data are cross-sectional and have some limitations in exploring the YSM effects; thus, cohort and YSM effects cannot be disentangled with a single cross-section of data. Last but not least, it is well known that assessing subjective mental health can be easily influenced by emotion, and when the respondents are interviewed, a study of the YSM effect of mental health needs a more sophisticated measure and delicate design.
For US evidence, see Hamilton and Hummer (2011), Huang et al. (2011), Hill et al. (2012). For Canadian evidence, see McDonald and Kennedy (2004), Newbold (2005), Kobayashi and Prus (2012), Aglipay et al. (2013), Kwak and Rudmin (2014). For Australian evidence, see Chiswick et al. (2008), Jatrana and Pasupuleti (2013). For UK evidence, see Averett et al. (2012). For Spanish evidence, see Gotsens et al. (2015), Rivera et al. (2016). For Irish evidence, see Nolan (2012). For US/UK/Canadian/Australian evidence, see Kennedy et al. (2015). For French, Italian, Spanish, and Belgian evidence, see Moullan and Jusot (2014).
We also discuss the selective migration effect and the “salmon effect” by using the migrant sample (from UMS) instead of the migrant workersR sample (from RHS). See Appendix A. This complementary discussion is only for reference.
We did not include marital status in the baseline regression because the variables capturing the basic demographic characteristics (such as age, gender, and ethnicity) were all exogenous. Marital status does not belong to this group of variables. When we included marital status in the demographic characteristics’ variables, the conclusions did not change.
We thank anonymous reviewers for suggesting valuable points in this section.
Unfortunately, a consistent measure of current or past heavy alcohol consumption and physical exercise habit information were not available.
Following the suggestion of an anonymous reviewer, we also performed an F-test to determine whether the two estimate coefficients are significantly different. It turns out that it failed to pass the test at any significant level (p value is 0.6314). Noting that the magnitudes of the t-statistics of the two coefficients are relatively close,(one is 2.05, and the other is 1.90), we could make a safe conclusion that the two effects were relatively close to each other; one passed the thresholds of the test of significance and the other failed to pass the test.
According to the definition of the healthy migrant phenomenon, the purpose of our study is to compare the urban residents and the migration workers who have already self-selected to migrate in cities. Therefore, the selective migration effect and the “salmon effect” are mechanisms that we should explain after measuring the healthy migration phenomenon rather than adjusting them before measuring. In fact, several researchers, such as Jatrana and Pasupuleti (2013), Qin et al. (2015), and Yuan (2009), have used a fixed-effect model or instrumental variables method to eliminate the self-selection problem. However, the purposes of these three studies differ significantly from ours. The three papers aimed to study the causal effect of migration on health; thus, they had to eliminate the self-selection problem to disentangle the endogenous problem, while ours focused on measuring the healthy migrant phenomenon itself.
References
Aglipay, M., Colman, I., & Chen, Y. (2013). Does the healthy immigrant effect extend to anxiety disorders? Evidence from a nationally representative study j immigrant minority health. Journal of Immigrant and Minority Health,15(5), 851–857.
Alegria, M., Canino, G., Shrout, P., Woo, M., Duan, N., Vila, D., et al. (2008). Prevalence of mental illness in immigrant and non-immigrant U.S. Latino Groups. American Journal of Psychiatry,165(3), 359–369.
Antecol, H., & Bedard, K. (2015). Immigrants and immigrant health. In B. Chiswick & P. W. Miller (Eds.), Handbook of the economics of international migration: The immigrants (pp. 271–315). Waltham, MA: North Holland.
Averett, S., Argys, L., & Kohn, J. (2012). Immigration, obesity and labor market outcomes in the UK. IZA Journal of Migration,1(1), 1–19.
Bergeron, P., Auger, N., & Hamel, D. (2009). Weight, general health and mental health: Status of diverse subgroups of immigrants in Canada. Canadian Journal of Public Health Review,100(100), 215–220.
Chen, J. (2011). Internal migration and health: Re-examining the healthy migrant phenomenon in China. Social Science and Medicine,72(8), 1294–1301.
Chiswick, B., Lee, Y., & Miller, P. (2008). Immigrant selection systems and immigrant health. Contemporary Economic Policy,26(4), 555–578.
Cook, B., Alegría, M., Lin, J., & Guo, J. (2009). Pathways and correlates connecting Latinos’ mental health with exposure to the United States. American Journal of Public Health,99(12), 2247–2254.
Cutler, D. M., & Lleras-Muney, A. (2010). Understanding differences in health behaviors by education. Journal of Health Economics,29(1), 1–28.
Fong, V. (2008). The other side of the healthy immigrant paradox: Chinese sojourners in Ireland and Britain who return to china due to personal and familial health crises. Culture, Medicine and Psychiatry,32(4), 627–641.
Gong, P., Liang, S., Carlton, E., Jiang, Q., Wu, J., Wang, L., et al. (2012). Urbanisation and health in China. The Lancet,379(9818), 843–852.
Gotsens, M., Malmusi, D., Villarroel, N., Vives-Cases, C., Garcia-Subirats, I., Hernando, C., et al. (2015). Health inequality between immigrants and natives in Spain: The loss of the healthy immigrant effect in times of economic crisis. European Journal of Public Health,25(6), 923–931.
Hamilton, T., & Hummer, R. (2011). Immigration and the health of U.S. Black adults: Does country of origin matter? Social Science and Medicine,73(10), 1551–1561.
Hesketh, T., Jun, Y., Lu, L., & Mei, W. (2008). Health status and access to health care of migrant workers in China. Public Health Reports,123(2), 189–197.
Hill, T., Angel, J., Balistreri, K., & Herrera, A. (2012). Immigrant status and cognitive functioning in late-life: An examination of gender variations in the healthy immigrant effect. Social Science and Medicine,75(12), 2076–2084.
Hu, X., Cook, S., & Salazar, M. A. (2008). Internal migration and health in China. The Lancet,372(9651), 1717–1719.
Huang, C., Mehta, N., Elo, I., Cunningham, S., & Stephenson, R. (2011). Region of birth and disability among recent U.S. Immigrants: Evidence from the 2000 census. Population Research and Policy Review,30(3), 399–418.
Jatrana, S., Pasupuleti, S., & Richardson K. (2013). Investigating the ‘healthy immigrant effect’ in Australia using fixed effects models: Findings from a Nationally-Representative Longitudinal Survey. HILDA_2013_Papers.
Kennedy, S., Kidd, M., Mcdonald, J., & Biddle, N. (2015). The healthy immigrant effect: Patterns and evidence from four countries. Journal of International Migration and Integration,16(2), 1–16.
Kobayashi, K., & Prus, S. (2012). Examining the gender, ethnicity, and age dimensions of the healthy immigrant effect: Factors in the development of equitable health policy. International Journal for Equity in Health,11(1), 1–6.
Kwak, K., & Rudmin, F. (2014). Adolescent health and adaptation in Canada: Examination of gender and age aspects of the healthy immigrant effect. International Journal for Equity in Health,13(1), 103–112.
Lu, Y. (2008). Test of the ‘healthy migrant hypothesis’: A longitudinal analysis of health selectivity of internal migration in Indonesia. Social Science and Medicine,67(8), 1331–1339.
Lu, Y. (2010). Rural-urban migration and health: Evidence from longitudinal data in Indonesia. Social Science and Medicine,70(3), 412–419.
Lu, Y., Hu, P., & Treiman, D. J. (2012). Migration and depressive symptoms in migrant-sending areas: Findings from the survey of internal migration and health in China. International Journal of Public Health,57(4), 691–698.
Mcdonald, J., & Kennedy, S. (2004). Insights into the ‘Healthy Immigrant Effect’: Health status and health service use of immigrants to Canada. Social Science and Medicine,59(8), 1613–1627.
Menezes, N., Georgiades, K., & Boyle, M. (2011). The influence of immigrant status and concentration on psychiatric disorder in canada: A multi-level analysis. Psychological Medicine,41(10), 2221–2231.
Meng, X., Manning, C., Li, S., & Effendi, T. N. (2010). The great migration: Rural-urban migration in China and Indonesia. Cheltenham: Edward Elgar Publishing.
Mou, J., Cheng, J., Zhang, D., Jiang, H., Lin, L., & Griffiths, S. (2009). Health care utilisation amongst Shenzhen migrant workers: Does being insured make a difference? BMC Health Services Research,9(1), 214.
Moullan, Y., & Jusot, F. (2014). Why is the ‘Healthy Immigrant Effect’ different between European countries? European Journal of Public Health,24(1), 80–86.
Mu, R. (2014). Regional disparities in self-reported health: Evidence from Chinese older adults. Health Economics,23(5), 529–549.
Newbold, K. (2005). Self-rated health within the Canadian immigrant population: Risk and the healthy immigrant effect. Social Science and Medicine,60(6), 1359–1370.
Niu, J. (2013). Migration and its impact on the differences in health between rural and urban residents in China. Social Science in China,2, 46–63. (in Chinese).
Nolan, A. (2012). The ‘healthy immigrant’ effect: Initial evidence for Ireland. Health Economics, Policy and Law,7(3), 343–362.
Qin, L., Chen, C., Liu, X., Wang, C., & Jiang, Z. (2015). Migration health status and earnings of migrant workers from rural China. China and World Economics,23(2), 84–99.
Rivera, B., Casal, B., & Currais, L. (2016). The healthy immigrant effect on mental health: Determinants and implications for Mental Health Policy in Spain. Administration and Policy in Mental Health and Mental Health Services Research,43(4), 616–627.
Salant, T., & Lauderdale, D. (2003). Measuring culture: A critical review of acculturation and health in Asian immigrant populations. Social Science and Medicine,57(1), 71–90.
Shan, L., Zhao, M., Ning, N., Hao, Y., Li, Y., Liang, L., et al. (2018). Dissatisfaction with current integration reforms of health insurance schemes in China: Are they a success and what matters? Health Policy and Planning,33(3), 345–354.
Straiton, M., Grant, J., Winefield, H., & Taylor, A. (2014). Mental health in immigrant men and women in Australia: The North West Adelaide health Study. BMC Public Health,14(1), 1–15.
Tong, Y., & Piotrowski, M. (2012). Migration and health selectivity in the context of internal migration in China, 1997–2009. Population Research and Policy Review,31(4), 497–543.
Van Hook, J., & Zhang, W. (2011). Who stays? Who goes? Selective emigration among the foreign-born. Population Research and Policy Review,30(1), 1–24.
Wen, M., Fan, J., Jin, L., & Wang, G. (2010). Neighborhood effects on health among migrants and natives in Shanghai. China. Health & Place,16(3), 452–460.
Yuan, H. (2009). Health and incomes of migrant workers: Based on Beijing migrant workers Survey. Management World,5, 56–66. (in Chinese).
Zhou, X., & Lu, M. (2016). The rural migrant workers’ health: China’s success or regret? China Journal of Economics,3, 79–98. (in Chinese).
Acknowledgements
We are grateful to the editor and the three reviewers for their considered and detailed comments on our manuscript, which have helped us to improve it significantly. We thank for Andrew Foster, Xi Chen, Hong Liu, Yanyan Xiong, Lingguo Cheng, Suqin Ge, and other participants in 2018 2nd Biennial Conference of CHPAMS (China Health Policy and Management Society) at Yale University, 2017 Conference on Health and Development at Institute of Economics, Academia Sinica, and seminars at Yale University, Shanghai University of Finance and Economics, Southeast University and Nanjing University for their helpful comments. Ling Zhou and Zuyu Wang provided excellent research assistance to this paper. We also thank for the financial support of the National Natural Science Foundation of China (Grant No. 71603046), the MOE Project of Key Research Institute of Humanities and Social Sciences at Universities (Grant No. 17JJD630002), National Social Science Foundation of China (Grant No. 13CJY091), and ZhiShan Young Scholar Program of Southeast University (Grant No. 001).
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Ma, C., Qu, Z. & Xu, Z. Internal Migration and Mental Health: An Examination of the Healthy Migration Phenomenon in China. Popul Res Policy Rev 39, 493–517 (2020). https://doi.org/10.1007/s11113-019-09552-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11113-019-09552-z