
Abstract
Background There has been no in depth published study to date reporting on community pharmacists’ current experiences and their future practice needs relating to providing culturally competent pharmaceutical care to Australian culturally and linguistically diverse patients with low English proficiency. Objective To explore community pharmacists’ experiences serving culturally and linguistically diverse patients who have low English proficiency. Setting Community pharmacists in Australia. Method Focus group discussions with practising community pharmacists were conducted. Participants were recruited from metropolitan Sydney. Discussion centred around their current experiences and practice changes needed to enhance the provision of culturally competent pharmaceutical care. Thematic analysis using the constant comparison method within a grounded theory approach was performed on the data collected. Main outcome measure Participants’ experiences in providing culturally competent care to culturally and linguistically diverse patients with low English proficiency. Results Thirty community pharmacists participated in six focus group discussions. Inadequate provision of culturally competent care was found to be primarily due to the issue of language incongruence between pharmacist and patient. Participants proposed various means with which such care may be provided to ensure patient safety. Conclusion Pharmacist participants expressed being inadequately equipped to provide culturally competent care in the community setting and identified potential means by which such care may be delivered. Addressing identified barriers that hinder community pharmacists’ capacity to engage in culturally competent practice can potentially improve provision of pharmaceutical care to culturally and linguistically diverse patients with low English proficiency.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Impacts on practice
-
Findings highlight the unmet practice needs of community pharmacists in feeling adequately supported to provide culturally competent care to culturally and linguistically diverse patients with low English proficiency.
-
Pharmacy professional organisations and coursework providers may need to re(consider) the focus of training and continuing professional development activities with respect to culturally competent practice.
-
There is a need for increased awareness of existing support resources and for pharmacy practice research focused on the development of tailored resources that may support culturally competent community pharmacist practice.
Introduction
Over the last decade, the importance of healthcare professionals’ cultural competency in ensuring patient safety and optimal medicines use in diverse patient populations has been increasingly recognised [1,2,3]. Cultural competence is an adaption of care to ensure effective delivery of services to culturally and linguistically diverse (CALD) patient populations [3].
Multiple definitions exist of the concept [4,5,6]; the common thread in all of them being an awareness of the health beliefs/practices and cultural background of the patient and possession of skills and attitudes that facilitate delivery of effective patient care.
The Purnell model of cultural competence is widely used to understand the influence of culture, of both the patient and healthcare provider, in the provision of healthcare [3, 7,8,9]. This model suggests that one must first understand ‘culture’ as something that is unique but interactive at various macro levels e.g., personal, family unit, community and global levels. At a micro level, there are 12 domains that uniquely characterise a culture; some of which are family roles, communication determinants and healthcare practices. In this context of knowledge about culture, health professionals may be thought of as being in one of four classes, as depicted in Table 1 [7].
One integral component of the “set of skills” that allows a healthcare professional to be equipped to deliver effective healthcare to CALD patients with low English proficiency (CALD LEP), ultimately ensuring quality care and a step towards professional cultural competency, is effective communication [7].
Pharmacists, referred to as the ‘gate-keepers’ of medicines and usually the last healthcare professional any patient consults prior to medicine consumption [10], are integrally placed to ensure quality use of medicines and hence, for whom the issue of effective patient communication is important [11,12,13]. Community pharmacies in particular are the main outlet for distribution of all medicines. Thus, for community pharmacists, the issue of cultural competence and effective communication is critical [3]. This is particularly relevant as patient populations around the world, such as in Europe, the United States of America (US) and Australia have become increasingly ethnically diverse.
A recent 2016 National Australian Census highlighted that Australia was amongst the most multi-ethnic nations in the world, with a multitude of CALD population groups [14] and over 300 languages spoken, despite the national language being English [15]. Thus, LEP may be a key issue in the communication with and health literacy of patients within Australia, as well as in other multicultural countries in which English is the official language of communication such as the United Kingdom (UK), US and New Zealand (NZ) [16].
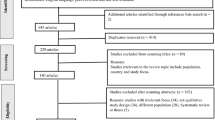
Several studies have sought ways to enhance health professionals’ cultural competency [2, 17,18,19]. There are also various exploratory studies in the literature pertaining to community pharmacies and provision of health/medicine-related information to patients with a CALD background with/without LEP. Explorations have been made from the patient [20,21,22,23] and pharmacist/pharmacy perspective [10, 24,25,26,27,28,29,30,31,32,33]. However, the majority of the studies have been conducted in relation to Spanish-speaking or Latino patients in the US [20, 21, 24, 29, 30, 33], with some in relation to patients with LEP in general [10, 25, 27, 28, 31, 32, 34]. There is a paucity of studies outside of the US though; with a few in Scotland [26], Australia [27, 35] and NZ [28].
A small-scale study conducted in Australia (2015) presented preliminary findings focused on the community pharmacist-low English proficient patient dyad from 5 pharmacies [27]. Study findings were informed from interviews with five community pharmacists in Queensland, Australia. Hindrances to pharmacists’ ability to provide care were reported illustrating a gap in provision of care to such patients; however, the need for more research with larger sample size was also highlighted [27]. More recently, in 2020, an Australian exploratory study of pharmacists’ experiences of asthma management in CALD patients highlighted the need for culturally appropriate pharmaceutical care models to be developed for the management of chronic conditions such as asthma [35].
Some examples of resources available in Australia that address the issue of language hinderances between healthcare professional and patient are the National Translation and Interpreting Service (NTIS) [36] and various online resources with translated health information online[37] and from the National Prescribing Service [38]. The NTIS is a free interpreting service that pharmacists may use to facilitate verbal communication with patients who have LEP when used “for the purpose of dispensing the Pharmaceutical Benefits Scheme medicationsFootnote 1” [39].
Despite Australia’s highly CALD population, there remains a paucity of published studies relating to current pharmacists’ practices regarding provision of services to such community members.
Aim of the study
This study aimed to examine experiences of community pharmacists providing professional services to this population within Australia in-depth. The specific objective was to explore and describe the current practice/s of community pharmacists serving CALD community members who have LEP and report on factors affecting their ability to provide culturally competent care to such patients.
Ethics approval
Ethics approval was granted by the University of Sydney Human Research Ethics Committee (HREC Protocol Number 2014/466).
Method
Design
This research study was mainly qualitative in nature and employed focus group discussions (FGDs) as a principal method of data collection. This approach was judged to be appropriate since diverse practice experiences would allow constructive discussion and foster participants’ reflections on their own practice [40,41,42]. Consenting participants were also requested to complete a short, de-identified study questionnaire (Appendix A) which allowed the recording of participants’ baseline characteristics including some details about their work experiences.
The FGD guide (Appendix B) was developed through a review of the available literature and designed to explore the objectives of the study [10, 22, 25, 43]. The research team members (experienced researchers in the field of pharmacy practice and practising community pharmacists themselves in areas with a diverse patient population) iteratively revised topic items for clarity and relevance to the aims. Key topics included:
-
(1)
Pharmacists’ current experience in providing pharmaceutical care to CALD LEP patients and
-
(2)
Future practice needs i.e., pharmacists’ recommendations regarding practice advances needed to enhance delivery of culturally competent care in a community pharmacy setting.
The FGD guide was pilot tested with three registered pharmacists who worked in an area known to have cultural and linguistic diversity as per Australian Bureau of Statistics (ABS) data [44, 45]. Additional questions suggested by the pilot pharmacists were incorporated in the final version. The FGD guide comprised key discussion points layered with prompts to allow deeper exploration of issues and probing into pharmacists’ experiences.
Participant recruitment
This study was carried out in the City of Sydney, New South Wales, Australia.
Data from the 2011 ABS census revealed the Sydney metropolitan area to be more culturally diverse than the Australian population as a whole, according to three aspects of diversity: country of origin, language spoken and religion [46]. Three areas with high diversity levels were selected for pharmacist recruitment: South-Western, Western and Inner-City Sydney. These areas were the least culturally homogenous relative to other areas of Sydney, such as the Northern and Southern suburbs, according to ABS parameters: language spoken at home, self-reported LEP and country of origin [46]. The recruitment strategy adopted is detailed in Table 2 [47, 48].
Exact number of focus groups that were necessary to be conducted was determined by the point at which thematic saturation was deemed to have been reached, in line with qualitative research methods [49,50,51,52], as explained below.
Data collection and qualitative analysis
Prior to conducting the focus groups, consent for participation as well as the completed study questionnaire was obtained from all participants.
The primary researcher facilitated all FGDs after receiving comprehensive training about facilitation (e.g. use of open ended questioning, probing leads, providing equal opportunities to all to speak, not allowing a dominant speaker to sabotage discussions, drawing participants back to the topic on hand if the discussion strayed) [40,41,42]. The other more experienced research team members were in attendance in all FGDs. FGDs were carried out in professional meeting spaces within the council areas that pharmacies were located.
FGDs were digitally audio-recorded, de-identified then transcribed verbatim. Field notes taken by the research team at the meeting were appended to transcripts where appropriate for completeness. The text files were then analysed independently by the primary researcher using QSR International’s NVivo 10 (version 10, 2012) qualitative data analysis software. Analysis was conducted according to the constant comparison method [53, 54], whereby issues were iteratively explored by carrying out the analysis concurrently with data collection. Data-driven inductive coding techniques, using a grounded theory approach, were then incorporated to identify themes [53, 55].
To test the reliability and consistency of the themes created, the two other researchers read a proportion of the transcripts and coded them independently. All three coded transcript sets were then compared, any differences arbitrated and themes clarified with discussion until consensus was reached [55].
Data collection continued until further FGDs did not reveal new findings and thematic saturation [52] was deemed to have been reached. Findings were summarised and quotes presented representative of each theme.
Results
A total of six FGDs were conducted between July 2014 and February 2015 with an average of five participants in each, and a total of 30 participants. FGDs ranged between 25 and 45 min in duration. After five focus groups no new distinct themes or ideas emerged from the data, indicating data saturation had been achieved. One more focus group was conducted subsequently to confirm saturation of themes. There were no invited participants who refused to participate or did not participate. The investigators had no professional relationships, or otherwise, with any of the participants. Consolidated criteria for reporting qualitative research was followed to report study findings [56].
The issue of language proficiency between pharmacist and patient was identified as the major hindrance to culturally competent care within the community pharmacy setting.
Participants were aware that with gender-specific health issues, CALD LEP patients, particularly of certain cultural backgrounds or with certain religious affiliations, may feel more comfortable speaking to a same-gendered pharmacist or trained pharmacy team member. They reported always being mindful of this and ensuring this was achieved wherever possible. “From my experience, I know men and women in the area I work in, would prefer to have a pharmacist of the same gender speak to them if they had to, at length about any gender-specific health concerns or medicines- it is not a discriminatory feel- it is just what they feel comfortable with because of the norms in their culture. We are mindful of this and try to be accommodating that way. “(P3, FGD3).
Participants were also aware of the issue of CALD patients’ dietary restrictions, such as the choice to consume medicinal products deemed or accredited as “vegan” or “halal,” and reported this to be the only pervasive “health practice or beliefs” related issue, within the context of cultural competency that they encountered. “The only predominant belief- related query I’ve seen in relation to any pharmaceutical product is whether it is vegan compliant or if it is halal- the latter being an issue of relevance to those of the Islamic faith.” (P4, FGD4).
Data from study questionnaire
Demographic data of the participant sample and their practice experiences with CALD community members are highlighted in Table 3 and Appendix C, respectively, indicating a good diversity of various characteristics.
Most of the participants were bilingual (n = 27); some even trilingual (n = 2). Participants reported encountering CALD LEP patients frequently and majority also reported working alongside multilingual staff members (80%).
Many participants indicated they were aware of some resource/s that may be of assistance when interacting with CALD LEP patients (Table 4 and Appendix C).
Majority of participants were not aware of any dispensing software functionalities such as capacity to print multilingual labels that may assist in communication.
Two participants indicated they had received training about effective engagement of CALD LEP patients. They described this training to be a “seminar attended in their intern year”, and “part of the undergraduate (B. Pharm) degree some years ago”.
Themes derived from FGDs
Data analysis revealed themes pertaining to the current practice of pharmacists in relation to the provision of pharmaceutical care to CALD LEP patients.
Figure 1 is a thematic map depicting the overarching themes and sub-themes that emerged from the FGDs. Supporting quotations for each theme can be found in Table 5.

Thematic map: Pharmacists’ concerns relating to the inadequate provision of culturally competent care and proposed means with which such care may be ensured
Theme 1: Concerns relating to the inadequate provision of culturally competent care
Issues with professional satisfaction
Pharmacists reported that CALD LEP patients had limited access to services and health information provided by them due to existing language barriers. This manifested as a concern for fulfilling pharmacist professional duties relating to providing good care and working with patients [57]. “When I think of what we do for the minority CALD patients I don’t feel that I’m doing my job like I ought to be as a health professional.” (P1, FGD 5).
Participants were ‘uneasy’ when such patients came to their pharmacy as they felt they would not be able to optimally serve them. They lacked confidence in dealing with them and this was one reason why they did not feel satisfied with the care they were providing.
Pharmacists reported resorting to use of unaccredited interpreters to augment their dialogue with CALD LEP patients, despite viewing it as unreliable. These included family members, nearby shop staff, customers and multilingual pharmacy staff members. Similarly, some mentioned the use of ‘google translate’ as useful, due to its accessibility but expressed concern about it not being accredited from a health professional body. Resources such as officially accredited translators were not deemed suitable due to perceived inconvenience in a busy community pharmacy. “It is professionally troubling to rely on a non-accredited interpreter.” (P1, FGD 6).
Concern for patient safety
Pharmacists also expressed a concern for patient safety due to the issue of language incongruence when interacting with CALD LEP patients. This concern meant pharmacists were reluctant to serve such patients, highlighting the need for more structured support for dealing with this patient population. Patient understanding of health information was seldom confirmed. “I don’t actively ask about confirmation…not what I tend to do in my normal practice I am ashamed to say which potentially is very dangerous.” (P2, FGD 6).
Reliance on the medical practitioner to facilitate communication was also common, as often these patients would see a doctor who was proficient in their native language. Pharmacists perceived this as not fulfilling their duty of care towards the patient. “There is no way of knowing whether it is safe and appropriate for them because you can’t effectively communicate.” (P2, FGD 5).
Theme 2: Means with which provision of culturally competent care may be ensured
Existing resources
Many participants indicated in the questionnaire that they were aware of a variety of resources that may be of use when interacting with such patients. However, when prompted about their experience with these resources within the FGDs the majority stated they had not used them in practice nor could they recall details such as the name of the resource or a method of accessing it. In the FGDs, it became apparent, that the majority of participants in fact perceived there were minimal suitable resources that could facilitate communication with CALD LEP patients. “I think an educational course informing of existing resources and what more can be done …would be beneficial.” (P9, FGD 3).
Development of tailored communication aids and resources
Participants suggested the development of communication aids and resources uniquely tailored to the community pharmacy space that could enhance their ability to provide culturally competent healthcare to CALD LEP patients.
The suggestions put forward were:
-
Centralisation of resources for easy accessibility
Participants expressed a need for developing a database or portal that summarised details of all resources available that may be utilised to enhance interaction with CALD LEP patients. “Available resources should be centralised at one point.” (P3, FGD 5).
-
Development of tailored communication aids
Participants suggested the development of communication aids uniquely tailored to the community pharmacy space, which can facilitate communication with CALD LEP patients such as dual-language medicine labels. “Having resources in other languages would be helpful- dispensing labels in a number of languages in the pharmacy would be very helpful.” (P3, FGD 1).
Another suggestion was an online or telephone-based consultation support dedicated for community pharmacy use for prescription and non-prescription item requests that allowed easy and accurate history taking and conveying of appropriate advice.
Participants stated any aid would need to be easy to use, reliable and efficient in achieving its purpose, given the dynamics of a community pharmacy setting, and have accreditation/approval by a representative health professional organisation. “Sometimes I know there is a function or resource I can use but because it takes too long, I would rather just go without it.” (P2, FGD6).
-
Training module
Participants also expressed a paucity of professional training received on how to optimally serve CALD LEP patients. There was limited awareness of health literacy principles in communicating with such patients and hence, participants suggested the development of a training model detailing such information. “We (pharmacists) aren’t really trained ….—so a lot of the time it’s just you using your problem-solving skills on the spot and improvising however you can.” (P1, FGD 4).
Discussion
This is the first Australian study that has qualitatively explored the professional interactions of community pharmacists with CALD LEP patients in depth [58, 59]. Study findings have highlighted the ongoing hindrances faced by community pharmacists to providing culturally competent care and various means by which these challenges may be overcome. This resonates with findings of a previous small-scale qualitative study involving five community pharmacists [27], which initially drew attention to the need for increased exploration of this area of professional practice.
In the context of Purnell’s cultural competence model [7], the participants in this study could be considered as ‘consciously incompetent’ as they did not display an unawareness of other cultures but rather were restricted in the culturally congruent care they could provide. Whilst this can be reassuring in terms of the study participants not displaying a blatant disregard or ignorance of the needs of such members of the community, the challenges community pharmacists experience is concerning due to the potential for compromised healthcare as well as duty of care that may ensue. This concern was relayed by study participants, indicating a high degree of self-reflection, despite being a relatively young cohort in terms of years of experience. It is thus necessary for these challenges to be addressed in a timely manner.
Study participants expressed the need for increased awareness of existing resources that can be used when interacting with CALD LEP patients. Increasing pharmacists’ awareness of the NTIS, for example, may potentially increase its utilisation in efforts to ameliorate communication challenges encountered in the community pharmacy space. Despite it being free of charge to patients and healthcare providers, it was clear that many participants in our study were not familiar with this service.
Studies indicate the use of professional interpreters or presence of bilingual healthcare professionals who are able to communicate in a patient’s primary language confers the most benefit in terms of patient safety and communication [60, 61]. Crossman KL, Wiener E, Roosevelt G, Bajaj L, Hampers LC, (2010) found both telephonic and in-person interpretation conferred greater benefit in understanding of discharge diagnosis in an urban paediatric emergency department compared with bilingual providers, highlighting the importance of such professional language assistance [62].
Many not-for-profit organisations focused on supporting patients with a specific disease also have patient information in different languages available online (e.g. Coeliac New South Wales [63]). This may be accessed and used as an aid by pharmacists when communicating specific health-related information. Again, participants in our sample appeared not to utilise these sources, possibly as these are not consolidated on a single site and due to a lack of awareness.
Web applications such as UniversalDoctor [64], a medical translation software application tailored for healthcare professionals to facilitate communication with foreign patients speaking different languages, could also be considered for implementation in a community pharmacy setting and its utility explored. Direction may be taken from such applications to develop an aid more tailored to a community pharmacy setting that may assist in consultations between the pharmacist and low- English proficient patient. Further research documenting the practicalities, applicability, usefulness and logistics of the available resources in the context of the community pharmacy setting is needed.
Prescription labels were also highlighted by participants as integral for appropriate medicine taking. Research investigating improved prescription medicine labelling has been a focus of inquiry [65, 66] to improve CALD patients’ understanding of medicines use. In the US, the Institute of Medicine’s Preventing Medication Error [67] and Standardizing Medication Labels [68] reports, specifically cite ‘poor understanding of medicine labelling as one root cause of a large proportion of medicine errors’ that occur. Research regarding the development and use of multilingual labels [69, 70] and other language concordant medicines information [71] in ethnic minorities in the US has been promising in terms of increasing patient understanding of medicines use [69, 72, 73]. This warrants exploration of the development and use of customised multilingual labels that can be affixed by pharmacists, when dispensing prescription medicines for CALD LEP patients in Australia. Whilst plans are in place for medicine labels in Australia to be changed over the next few years to improve legibility [74], specific requirements of CALD LEP patients are not catered for in the proposed changes [74]. Furthermore, a futuristic concept may be to consider the use of media rich labels, e.g. speaking labels that can produce an audio translated version of the label in the users own language [75].
Thus, an increased awareness of existing resources and development of new resources that may be used in community pharmacy could positively influence CALD LEP patient safety outcomes and pharmacists’ sense of professional satisfaction in regards to duty of care towards such patients.
Moreover, given the rich ethnic diversity throughout Australia, an awareness of the cultural norms of various cultural groups in relation to interaction with healthcare professionals and belief-related issues relating to consumption of medicinal products, as was found in our study, would also be beneficial to ensuring a more understanding and accommodating pharmacist workforce. Given the increasing cultural diversity globally, our findings may be worthwhile to healthcare workforces internationally as well, despite the structural differences between healthcare contexts.
As with all research, this study had limitations. The majority of participants in our sample had fewer than ten years of experience as registered pharmacists. It is likely that a different demography of pharmacists from the same region may have yielded slightly varied results. It is possible that the perspectives of our study participants may also differ from pharmacists in other regions in Australia. The focus group data may have been influenced by selection bias as the pharmacists who agreed to participate possibly could have had an interest in the research topic. However, our random sampling strategy attempted to avoid such bias and given thematic saturation was reached, data is likely to be similar across other community pharmacies in CALD areas because pharmacy workflow and practice patterns would be similar. Self-reported data from the participants meant there was no means to confirm the accuracy of their responses. Future studies could use an observational narrative or observation by simulated patients to document interactions of pharmacists with CALD LEP patients allowing subjective findings to be triangulated with objective measurements.
Despite these limitations, this study has provided insights into the current practice and experiences of community pharmacists when rendering their professional services to CALD LEP patients as well as direction for future research so that pharmacists may optimally engage in culturally competent practice.
Conclusion
Community pharmacists reported communicating across language divides as the main challenge in providing culturally competent care to CALD LEP patients. The present study calls for increased awareness amongst pharmacists of existing resources that are available which may enhance their interaction with such patients. There appears to also be a need for further exploration of tailored resources such as multilingual prescription labels or tools for use in the unique community pharmacy space. Schools of pharmacy and pharmacist professional organisations may wish to also include more formal training in this area.
Pharmacists may better meet their professional obligations towards CALD LEP patients by an increase in awareness and understanding of existing resources that may facilitate their interaction. There is also need for further research into the development of a novel aid that mitigates the unique challenges faced by pharmacists in the Australian community pharmacy setting relating to prescription and non-prescription item requests by such patients. Addressing the identified gaps can facilitate progression towards community pharmacists being able to provide consciously competent care or even reaching a stage of being unconsciously competent as defined by Purnell’s model of cultural competence [7].
Data Availability
Not applicable.
Code availability
Not applicable.
Notes
The Pharmaceutical Benefits Scheme is an Australian Government program that benefits all Australians by subsidising medicines to make them more affordable. More info: http://www.pbs.gov.au/pbs/home.
References
Horvat L, Horey D, Romios P, Kis-Rigo J. Cultural competence education for health professionals. Cochrane Database Syst Rev. 2014;5:CD009405.
Lie DA, Lee-Rey E, Gomez A, Bereknyei S, Braddock CH 3rd. Does cultural competency training of health professionals improve patient outcomes? A systematic review and proposed algorithm for future research. J Gen Intern Med. 2011;26(3):317–25.
O’connell M, Korner E, Rickles N, Sias J. Cultural competence in health care and its implications for pharmacy. Pharmacotherapy. 2007;27(7):1062–79.
Nelson A. Unequal treatment: confronting racial and ethnic disparities in health care. J Natl Med Assoc. 2002;94(8):666–8.
Betancourt JR, Green AR, Carrillo JE. Cultural competence in health care: emerging frameworks and practical approaches. New York, NY: The Commonwealth Fund; 2002.
Brach C, Fraser I. Can cultural competency reduce racial and ethnic health disparities? A review and conceptual model. Med Care Res Rev. 2000;57(Suppl 1):181–217.
Purnell L. The Purnell Model for Cultural Competence. J Transcult Nurs. 2002;13(3):193–6 (discussion 200-1).
Australian Institute of Family Studies, Sawrikar, P, Katz, I. Enhancing family and relationship service accessibility and delivery to culturally and linguistically diverse families in Australia. 2008. https://aifs.gov.au/cfca/publications/enhancing-family-and-relationship-service-accessibility-and/background. Cited 29 Jan 2021.
Purnell L. A description of the purnell model for cultural competence. J Transcult Nurs. 2000;11(1):40–6.
Westberg SM, Sorensen TD. Pharmacy-related health disparities experienced by non-English-speaking patients: impact of pharmaceutical care. J Am Pharm Assoc. 2005;45(1):48–54.
Carlisle A, Jacobson KL, Di Francesco L, Parker RM. Health literacy in the pharmacy practical strategies to improve communication with patients. P&T. 2011;36(9):576–80.
Davis TC, Federman AD, Bass PF, Jackson RH, Middlebrooks M, Parker RM, et al. Improving patient understanding of prescription drug label instructions. J Gen Intern Med. 2009;24(1):57–62.
Youmans SL, Schillinger D. Functional health literacy and medication use: the pharmacist’s role. Ann Pharmacother. 2003;37(11):1726–9.
Abouzeid M, Bhopal RS, Dunbar JA, Janus ED. The potential for measuring ethnicity and health in a multicultural milieu—the case of type 2 diabetes in Australia. Ethn Health. 2013;19(4):424–39.
Australian Bureau of Statistics. Media release: Census reveals a fast changing, culturally diverse nation. 2017. http://www.abs.gov.au/ausstats/abs@.nsf/lookup/Media%20Release3. Cited 29 Jan 2021.
Australian Bureau of Statistics. Adult literacy and life skills survey, summary of results. Canberra: Australian Bureau of Statistics; 2006. Contract No.: 4228.0.
Zeh P, Sandhu HK, Cannaby AM, Sturt JA. The impact of culturally competent diabetes care interventions for improving diabetes-related outcomes in ethnic minority groups: a systematic review. Diabet Med. 2012;29(10):1237–52.
Haack S. Engaging pharmacy students with diverse patient populations to improve cultural competence. Am J Pharm Educ. 2008;72(5):124.
Poirier TI, Butler LM, Devraj R, Gupchup GV, Santanello C, Lynch JC. A cultural competency course for pharmacy students. Am J Pharm Educ. 2009;73(5):81.
Olenik NL, Gonzalvo JD, Snyder ME, Nash CL, Smith CT. Perceptions of Spanish-speaking clientele of patient care services in a community pharmacy. Res Social Adm Pharm. 2015;11(2):241–52.
Sleath B, Blalock SJ, Bender DE, Murray M, Cerna A, Cohen MG. Latino patients’ preferences for medication information and pharmacy services. J Am Pharm Assoc. 2009;49(5):632–6.
Mohammad A, Saini B, Chaar BB. Exploring culturally and linguistically diverse consumer needs in relation to medicines use and health information within the pharmacy setting. Res Social Adm Pharm. 2015;11(4):545–59.
Hughes ML, John DN, Jones AT, Jones EH, Wilkins ML. Language issues in the community pharmacy: a perspective from Wales. Int J Pharm Pract. 2009;17(3):157–63.
Muzyk AJ, Muzyk TL, Barnett CW. Counseling Spanish-speaking patients: Atlanta pharmacists’ cultural sensitivity, use of language-assistance services, and attitudes. J Am Pharm Assoc. 2004;44(3):366–74.
Bradshaw M, Tomany-Korman S, Flores G. Language barriers to prescriptions for patients with limited English proficiency: a survey of pharmacies. Pediatrics. 2007;120(2):225–35.
Cleland JA, Watson MC, Walker L, Denison A, Vanes N, Moffat M. Community pharmacists’ perceptions of barriers to communication with migrants. Int J Pharm Pract. 2012;20(3):148–54.
Arora DS, Mey A, Maganlal S, Khan S. Provision of pharmaceutical care in patients with limited English proficiency: preliminary findings. J Res Pharm Pract. 2015;4(3):123–8.
Chang E, Tsang B, Thornley S. Language barriers in the community pharmacy: a survey of northern and western Auckland. J Prim Health Care. 2011;3(2):102–6.
Devraj R, Young HN. Pharmacy language assistance resources and their association with pharmacists’ self-efficacy in communicating with Spanish-speaking patients. Res Social Adm Pharm. 2017;13(1):123–32.
Gonzalvo J, Schmelz A, Hudmon KS. Community pharmacist and technician communication with Spanish-speaking patients: needs assessment. J Am Pharm Assoc. 2012;52(3):363–6.
Weiss L, Gany F, Rosenfeld P, Carrasquillo O, Sharif I, Behar E, et al. Access to multilingual medication instructions at New York City pharmacies. J Urban Health. 2007;84(6):742–54.
Zargarzadeh AH, Law AV. Access to multilingual prescription labels and verbal translation services in California. Res Social Adm Pharm. 2011;7(4):338–46.
Young HN, Dilworth TJ, Mott DA, Cox ED, Moreno MA, Brown RL. Pharmacists’ provision of information to Spanish-speaking patients: a social cognitive approach. Res Social Adm Pharm. 2013;9(1):4–12.
Stevenson F. Achieving visibility? Use of non-verbal communication in interactions between patients and pharmacists who do not share a common language. Sociol Health Illn. 2014;36(5):756–71.
Alzayer R, Svedin E, Rizvi S, Basheti I, Chaar B, Saini B. Pharmacists’ experience of asthma management in culturally and linguistically diverse (CALD) patients. Res Social Adm Pharm. 2021;17:315–25.
Australian Government Department of Home Affairs. About the free interpreting service. 2021. https://www.tisnational.gov.au/en/Agencies/Charges-and-free-services/About-the-Free-Interpreting-Service. Cited 29 Jan 2021.
Victorian Government of Australia. Health Translations. https://www.healthtranslations.vic.gov.au/bhcv2/bhcht.nsf/pages/about_us. Cited 29 Jan 2021.
NPS MedicineWise. Translated health Information about medicines. 2017. https://www.nps.org.au/translated-info. Cited 29 Jan 2021.
Australian Government Department of Home Affairs. Pharmacies with access to the Free Interpreting Service—Listed by State and Suburb. 2021. https://www.tisnational.gov.au/~/media/Files/Registered%20pharmacies/PDF/Registered%20pharmacies.ashx. Cited 29 Jan 2021.
Freeman T. “Best practice” in focus group research: making sense of different views. J Adv Nurs. 2006;56:491–7.
Kitzinger J. Qualitative research: introducing focus groups. Br Med J. 1995;311:299–302.
Morgan DL. Focus groups as qualitative research. Thousand Oaks: Sage Publications; 1997.
Phokeo V, Hyman I. Provision of pharmaceutical care to patients with limited English proficiency. Am J Health Syst Pharm. 2007;64(4):423–9.
Public Health Information Development Unit (PHIDU). Social Health Atlas of Australia: New South Wales and Australian Capital Territory Data by Local Government Area. 2021. https://phidu.torrens.edu.au/current/maps/sha-aust/lga-single-map/nsw-act/atlas.html. Cited 29 Jan 2021.
Australian Bureau of Statistics. QuickStats. 2016. http://www.abs.gov.au/websitedbs/censushome.nsf/home/quickstats. Cited 29 Jan 2021.
SBS website. SBS census explorer. 2017. http://www.sbs.com.au/news/census-explorer. Cited 29 Jan 2021.
Pharmacy Council of NSW. Search the pharmacy register. 2021. https://search.pharmacycouncil.nsw.gov.au/. Cited 29 Jan 2021.
Martínez-Mesa J, González-Chica DA, Duquia RP, Bonamigo RR, Bastos JL. Sampling: how to select participants in my research study? An Bras Dermatol. 2016;91(3):326–30.
Bryman A. Social Research Methods. 4th ed. Oxford: Oxford University Press; 2012.
Guest G, Bunce A, Johnson L. How many interviews are enough?: An experiment with data saturation and variability. Field Methods. 2006;18(1):59–82.
Denzin NK, Lincoln YS. Designing funded qualitative research. In: Morse JM, editor. Handbook of qualitative research. 2nd ed. Thousand Oaks, CA: Sage; 1994. p. 220–35.
Ritchie J, Lewis J, Nicholls CM, Ormston R. Designing and selecting samples. Qualitative research practice. A guide for social science students and researchers. Thousands Oaks, CA: Sage; 2003. p. 77–108.
Strauss A, Corbin J. Basics of qualitative research techniques and procedures for developing grounded theory. 2nd ed. Thousand Oaks, CA: SAGE; 1998.
Ulin PRRE, Tolley EE. Qualitative methods in public health: a field guide for applied research. 1st ed. San Francisco, CA: Jossey-Bass; 2005.
Crabtree BFMW. Doing qualitative research. 2nd ed. Thousand Oaks, CA: Sage Publications; 1999.
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–57.
Pharmacy Board of Australia. Code of conduct for pharmacists. 2014. https://www.pharmacyboard.gov.au/Codes-Guidelines.aspx. Cited 29 Jan 2021.
Keleher H, Hagger V. Health literacy in primary health care. Aust J Prim Health. 2007;13(2):24–30.
Australian Commission on Safety and Quality in Health Care. Consumers, the health system and health literacy: taking action to improve safety and quality. Consultation Paper. 2013. https://www.safetyandquality.gov.au/sites/default/files/migrated/Consumers-the-health-system-and-health-literacy-Taking-action-to-improve-safety-and-quality3.pdf. Cited 29 Jan 2021.
Flores G. The impact of medical interpreter services on the quality of health care: a systematic review. Med Care Res Rev. 2005;62(3):255–99.
Meshreky W, Weekes L, Atkins L. Bilingual pharmacists delivering community education seminars to culturally and linguistically diverse (CALD) peoples. Res Social Adm Pharm. 2014;10(5):e11.
Crossman KL, Wiener E, Roosevelt G, Bajaj L, Hampers LC. Interpreters: telephonic, in-person interpretation and bilingual providers. Pediatrics. 2010;125(3):e631–8.
Coeliac Australia. Multilingual Fact Sheets. https://www.coeliac.org.au/s/coeliac-disease/multilingual-fact-sheets/. Cited 29 Jan 2021.
Universal Projects and Tools S.L. Universal Doctor. 2020. https://www.universaldoctor.com/. Cited 29 Jan 21.
Tarn DM, Heritage J, Paterniti DA, Hays RD, Kravitz RL, Wenger NS. Physician communication when prescribing new medications. Arch Intern Med. 2006;166(17):1855–62.
Davis TC, Wolf MS, Bass PF, Thompson JA, Tilson HH, Neuberger M, et al. Literacy and misunderstanding prescription drug labels. Ann Intern Med. 2006;145(12):887–94.
Institute of Medicine. Preventing medication errors. Washington, DC: Institute of Medicine; 2006.
Institute of Medicine. Standardizing medication labels: confusing patients less. Workshop summary. Washington, DC: National Academy Press; 2008.
Bailey SC, Hasnain-Wynia R, Chen AH, Sarkar U, Schoua-Glusberg A, Lindquist LA, et al. Developing multilingual prescription instructions for patients with limited English proficiency. J Health Care Poor Undersev. 2012;23(1):81–7.
Mohan A, Riley MB, Boyington D, Johnston P, Trochez K, Jennings C, et al. Development of a patient-centred bilingual prescription drug label. J Health Commun. 2013;8:49–61.
Sansgiry SS, Chanda S, Shringarpure GS. Impact of bilingual product information labels on Spanish-speaking adults’ ability to comprehend OTC information. Res Social Adm Pharm. 2007;3(4):410–25.
Babar Z, Pengelly K, Scahill S, Garg S, Shaw J. Migrant health in New Zealand: exploring issues concerning medicines access and use. J Pharm Health Serv Res. 2013;4:41–9.
Bailey SC, Agarwal N, Sleath B, Gumusoglu S, Wolf MS. Improving drug labeling and counseling for limited English proficient adults. J Health Care Poor Underserv. 2011;22(4):1131–43.
Therapeutic Goods Administration (TGA). Australia's medicine labels are becoming clearer. 2020. https://www.tga.gov.au/australias-medicine-labels-are-becoming-clearer. Cited 29 Jan 21.
Anonymous. Talking prescription labels available soon. J Dent Hyg.2001;75(2):112.
Acknowledgements
The authors would like to thank the community pharmacists who participated in this study which provided an insight into the experiences of community pharmacists providing healthcare to CALD LEP patients. They would like to also thank the Sydney Pharmacy School for infrastructure and research support.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. Annim Mohammad had secured the Australian Postgarduate Award from the Australian Government to support her Doctoral pursuits.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Mohammad, A., Saini, B. & Chaar, B.B. Pharmacists’ experiences serving culturally and linguistically diverse patients in the Australian community pharmacy setting. Int J Clin Pharm 43, 1563–1573 (2021). https://doi.org/10.1007/s11096-021-01284-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11096-021-01284-5