
Abstract
To date, mechanistic modeling of oral drug absorption has been achieved via the use of physiologically based pharmacokinetic (PBPK) modeling, and more specifically, physiologically based biopharmaceutics model (PBBM). The concept of finite absorption time (FAT) has been developed recently and the application of the relevant physiologically based finite time pharmacokinetic (PBFTPK) models to experimental data provides explicit evidence that drug absorption terminates at a specific time point. In this manuscript, we explored how PBBM and PBFTPK models compare when applied to the same dataset. A set of six compounds with clinical data from immediate-release formulation were selected. Both models resulted in absorption time estimates within the small intestinal transit time, with PBFTPK models generally providing shorter time estimates. A clear relationship between the absorption rate and the product of permeability and luminal concentration was observed, in concurrence with the fundamental assumptions of PBFTPK models. We propose that future research on the synergy between the two modeling approaches can lead to both improvements in the initial parameterization of PBPK/PBBM models but to also expand mechanistic oral absorption concepts to more traditional pharmacometrics applications.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The physiologically based pharmacokinetic (PBPK)Footnote 1 modeling work relies on detailed mechanistic representations, which reduce the complex drug processes of the biological systems. In this context, the PBPK models integrate both drug-dependent parameters (physicochemical properties) and drug-independent (species-specific anatomy, physiology, and biochemistry) as well as combined, such as parameters related to biotransformation and excretion [1,2,3].
One of the most important applications of PBPK modeling is in oral drug absorption. Thus, hot themes in oral drug absorption such as specific patient populations, regional differences in the gastrointestinal tract, advanced formulations, and food-drug interactions have been reviewed recently [4]. In parallel, the concept of finite absorption time (FAT) has been developed recently and the application of the relevant physiologically based finite time pharmacokinetic (PBFTPK) models to experimental data provides explicit evidence that drug absorption terminates at a specific time point, τ [5,6,7,8,9]. In fact this is true because drug absorption takes place under sink conditions for physicochemical and physiological reasons. Thus, for BCS class II, III and IV drugs with low solubility and/or low permeability drug concentration in the GI tract remains essentially constant; in parallel, high blood flow in the vena cava, 20–40 cm/s [10] imposes sink conditions for the drug transfer rate. For class I drugs with high solubility and high permeability, absorption is very rapid and is completed in very short time. For one-compartment model drugs with a one-input rate, the value of τ coincides with tmax (the time corresponding to the maximum concentration, Cmax) [9]. In all other cases, simulations show that τ can be equal to or higher than tmax [9].
PBPK models of oral drug absorption utilize specific transit times in the compartments of the gastrointestinal tract and often rely on the passive drug diffusion mechanism under sink conditions since the blood on the basolateral side of the membrane is regarded as an ideal sink [2]. The PBFTPK models [5, 7,8,9] rely on the same principles: i) finite absorption time, τ for drug absorption processes and ii) zero-order drug input (single or multiple) or first-order [11,12,13] as a result of the passive drug absorption under sink conditions. This resemblance in the fundamental characteristics (transit and rate of drug input) prompted us to couple the simulated drug absorption profile derived from the PBPK models with the analysis of the in vivo data based on PBFTPK models to get a better understanding of the kinetics of drug absorption. Furthermore, we explore the relationships, if any, between physicochemical and pharmacokinetic parameters, e.g., rate of drug input.
Materials and Methods
Compounds
Six compounds, including etoricoxib, gaboxadol, dipryridamole, pioglitazone, compound C and losartan, were selected in this study to explore the relationship between biopharmaceutics and pharmacokinetic (PK) parameters. The key physicochemical and PK parameters are included in Table I. The selected compounds range from BCS I–III and are considered with a moderate to high fraction of absorption (Fa) for oral formulations [14,15,16,17]; the compounds were selected based on the availability of PO/IV data and PBPK models that were needed for this analysis.
PBPK Modeling Development
PBPK models for six selected compounds were developed as previously described [14,15,16,17]. The key physicochemical and pharmacokinetic parameters used as model input for each compound are summarized in Table I. When dissolution data were used, dissolution profile input was either entered as is or used a z-factor dissolution model [18] as input. Particle size based simulations used the Hintz-Johnson model [19]. Given that many of the compounds in this work are highly soluble in the stomach, the simulations are not very sensitive to the dissolution model selected. For compounds where precipitation was not observed in vitro, precipitation time (i.e. reciprocal of precipitation rate) was set to a high value as not to impact the simulation. Most models estimated human effective permeability from in vitro data which is a common practice [20]. Pharmacokinetic parameters for systemic disposition were obtained from previous publications where they were estimated by fitting intravenous PK data using either Phoenix WinNonlin (Certara, Princeton, NJ) or with the build-in PK-Plus module in GastroPlus™ (Simulations Plus, Lancaster, CA). Specific model settings or optimized parameters for model development were included in Table I. Since the purpose of this study is to use the estimates of in vivo absorption for comparison to the PBFTPK models, and the published models were within desired model acceptance criteria in terms of describing the clinical data, no further parameter optimization or change in the model setting was conducted in this manuscript; Table I indicates whether the original model was a bottom-up or middle-out approach, sources of parameters and fitted parameters when applicable.
All simulations were conducted using GastroPlus® software v9.8. The PBPK models used default fasted human physiology settings unless otherwise stated in the Table I. Opt logD model SA/V 6.1 was used as the absorption scale factor (ASF) model.
PBFTPK Model Fittings
The model equations [9] were fitted to experimental PK data [14,15,16,17]. The PBFTPK software used in all model fittings relies on user-defined functions in Igor programming environment. In this implementation, we adapted its versatile built-in least-squares algorithm which allows, among other features, restrictions to parameter values, the use of statistical weights and data sub-sets, calculation of parameter covariance matrix, and easy graphical representation of results. Due to the complex form of the model equations and the convoluted shape of the resulting χ2 hypersurface in parameter space with numerous local minima, the determination of initial trial parameter values was crucial and required manual adjustments.
Exploring Relationships between Biopharmaceutics Properties and Pharmacokinetic Parameters
The absorption kinetics can be described by the rate of penetration [5, 7].
where Peff is the effective permeability of the drug expressed in velocity units (length/time), SA is the surface area of the membrane in (length)2 units, CGI is drug concentration in the gastrointestinal (GI) lumen, Fa is the fraction of dose (D) absorbed and τ is the duration of the absorption phase.
The relationship between biopharmaceutics properties (e.g., Peff and solubility) and (AUC)0-τ for one zero-order input rate was discussed previously [5, 7].
where F is the bioavailable fraction of dose D, Vd is the volume of distribution and kel is the elimination rate constant. Time τ denotes either the passage of the drug beyond the absorptive sites or the completion of the absorption process since no more dissolved drug is available for absorption. (AUC)0-τ is the area under the curve from time 0 to τ.
(AUC) 0-τ represents the exposure of the compound in a certain time period and is a combining consideration of absorption rate and elimination rate. By replacing the FD/τ assuming no first pass effect with Eq. 1, a relationship among (AUC)0-τ, Peff, gastrointestinal concentration, and elimination parameters is established. In this study, correlation analysis was conducted between physicochemical properties such as Peff, Clumen, and pharmacokinetics parameters such as τ, elimination rate, and (AUC)0-τ. For compounds, such as gaboxadol and pioglitazone, which require a second stage of zero-order kinetics, τ1 and corresponding (AUC)0-τ1 were used for analysis. In this manuscript, the term “(AUC)0-τ “and “τ” were used for all the compounds.
All the selected compounds in this study are dissolved in solution after dosing and remain supersaturated in the GI tract, thus duodenum and jejunum lumen drug concentrations, estimated from PBPK modeling [14,15,16,17], were used for correlation analysis. Relevant PK parameters and absorption parameters were generated from PBFTPK fitting including τ, (AUC)0-τ, and elimination rate constant (kel). Effective human permeability (Peff) values for tested compounds were gathered from previously published papers [14,15,16,17].
Results
PBPK Modeling
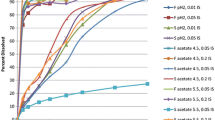
Detailed model development and validation can be found in previous publications [14,15,16,17]. Overall, the developed models can reasonably describe the observed pharmacokinetic profiles for the tested compounds. The percentage of prediction errors (%PE) for Cmax and AUC are within the typically acceptable criteria (%PE < 25%), as shown in Table II. Observed versus predicted plasma concentration-time profiles for each compound are presented in Fig. 1. Hence, the models are considered valid and robust, and suitable for further data analysis in this study.

Fittings of PBFTPK Models to In Vivo Data
A variety of models [9] were tested on the experimental data of the six formulations. Fits were attempted with one or two zero-order input stages for one or two compartment disposition models. Figure 2 shows the best fit for each drug product. Details and parameter values are also given in Fig. 2 for each drug.

Model fits to pharmacokinetic data for 6 oral formulations. Losartan and Compound C formulations are best described by a one-compartment model with a single stage of zero-order input kinetics [Eqs. 29–30 in [9]]. Gaboxadol and pioglitazone require a second stage of zero-order kinetics [Eqs. 31–33 in [9]]. Etoricoxib and dipyridamole are best described by a two-compartment model with one stage of zero-order kinetics [Eqs. 38–40 in [9]]. Optimized parameters are shown in the insets of each graph along with χ2 and R2 for each fit. Note: Fits for gaboxadol and pioglitazone were restricted to reduce parameter correlations. A solid triangle marks the end of any absorption stage, which in the cases presented happens to coincide with Cmax.
Figure 3 shows a plot of the disposition parameters versus the finite time absorption time τ estimates for the six drugs studied. All of them, except the borderline losartan, belong to the very rapidly absorbed drug class [9].

Grouping of formulations based on ranges of elimination rate constants one-compartment model drugs (β rate constants for two-compartment drugs) and FATs. Open symbols refer to two-compartment models.
Exploring Relationships between Biopharmaceutical Properties and Pharmacokinetic Parameters
Physicochemical and PK parameters, including effective permeability (Peff), maximum drug lumen concentration in duodenum and jejunum, absorption termination time (τ), AUC0-τ, and elimination rate (kel or β), for data analysis, are included in Table III.
Given the limited dataset, fully exploring relationships between PBFTPK parameters and PBBM input/output is not practical. Exploratory plots (data not shown) on, e.g., AUC0-τ vs Peff or Cs did not result in specific trends. We explore two relationships below.
-
1)
D/τ vs Peff*max(Clumen)
D/τ which is used as a measure of absorption rate showed a positive correlation with Peff * Clumen using either the maximum luminal concentration in the jejunum or duodenum, as shown in Fig. 4.
-
2)
kel (β) vs. AUC0-τ

Correlation between D/τ and Peff * Clumen. Open circle: etoricoxib, open triangle: gaboxadol, open square: dipyridamole, open diamond: pioglitazone, closed circle: compound C, closed square: losartan. For compounds, such as gaboxadol and pioglitazone, which require a second stage of zero-order kinetics, τ1 was used for analysis.
Values for kel or β were generated from PBFTPK model fitting, as shown in Fig. 2. Based on Eq. 2, elimination parameters (kel, clearance, β) are expected to exhibit a negative relationship with AUC0-τ. As shown in Fig. 5, a negative correlation between kel (or β for etoricoxib) and AUC0-τ was observed.
Discussion
The two modeling approaches utilized in the present study were based on PBPK and PBFTPK models. This allows us, for the first time, to explore potential relationships between the biopharmaceutics properties, solubility, and permeability with the pharmacokinetic parameters. This is so since the drug’s passive absorption under sink conditions kinetics can be described by the rate of penetration (Eq. 1) [5].
To the best of our knowledge, this is the first attempt to explore PBPK (and more specifically PBBM) and PBFTPK models for the same clinical datasets. The two modeling approaches have currently distinct application and focus. PBBM primarily focuses on simulation/prediction of oral absorption for a diverse set of applications during discovery and CMC activities (e.g., formulation development, dissolution specifications) and during clinical development (e.g., pH-dependent drug-drug interaction prediction, food effect prediction) [21]. The outcome is dictated by the input parameters, while the observed data are used for model validation as demonstrated in Table II. PBFTPK models on the other hand focus on the characterization of oral absorption based on the fitting of observed data. This difference in focus is also reflected in the outcomes shown in the examples herein, where the PBBM models show some deviations from the clinical data and somewhat different estimations of, e.g., termination of absorption time compared to the PBFTPK model.
Despite the currently different focus, we believe that synergies exist for their application in oral absorption modeling, derived from the common denominator that is the finite absorption time concept. As is evident from Figs. 1 and 2 for all the compounds studied, absorption is essentially complete within the small intestinal transit time as estimated by either model. The estimates of absorption time were generally shorter using the PBFTPK model compared to the PBBM model. This is perhaps not surprising as the PBBM models incorporate additional first-order processes to simulate gastrointestinal transit resulting in absorption curves that show curvature at ~80% of the maximum absorption point; for the earlier points, the absorption rate is very close to zero-order as assumed in the PBFTPK models.
Based on Eqs. 1 and 2, in this manuscript, we attempted to explore the relationship between PBFTPK estimated parameters and input parameters or outputs for PBBM models. For such analysis to result in actionable correlations to single physicochemical properties (e.g., Peff) it will require significantly larger datasets, most likely of compounds of similar class. Within the limited dataset explored, a clear relationship between D/τ and Peff*Clumen using either the maximum duodenum or jejunum concentrations was observed (Fig. 4). This relationship (Eq. 1) is fundamental and in accord with the basic principles of PBFTPK [5]. According to the drug’s biopharmaceutics properties, the rate-limiting property solubility or permeability will control the rate of drug penetration. However, the analysis of the data of this study demonstrates that the product Peff*Clumen is correlated with the rate of drug input. This finding is in accord with the fundamental principles of the absorption potential concept [22, 23] used prior to the introduction of BCS for the biopharmaceutics classification of drugs.
According to Eq. 2, \({\left( AUC\right)}_{0-{\tau }}\) is increasing when kel is decreasing. As shown in Fig. 5, this trend was indeed observable. It should also be emphasized that the partial area \({\left( AUC\right)}_{0-{\tau }}\) is used today as an early exposure metric [24]; however, what it represents, under the prism of the finite absorption time concept [7], is the fundamental extent of the absorption metric since it is linearly related (Eq. 2) with the dose (D) absorbed at time τ, namely, the end of the absorption processes.

Correlation between elimination parameter (kel or β) and AUC 0-τ. Open circle: etoricoxib, open triangle: gaboxadol, open square: dipyridamole, open diamond: pioglitazone, closed circle: compound C, closed square: losartan.
While the intent of this manuscript was to simply serve as a starting point for exploring the relationship of PBPK and PBFTPK models, we envision some broader areas for additional synergy of PBBM and PBFTPK models that could be considered as areas of future research.
-
PBFTPK models allow for the estimation of bioavailability-corrected disposition parameters without the need for IV data [7] at an individual level basis. Current PBBM models are often developed either without IV data being available or with IV data coming from an independent study, thus introducing between-study variability uncertainty. Especially for compounds where absorption is close to complete and thus the bioavailability correction only reflects first-pass metabolism, PBFTPK estimated disposition parameters could facilitate the development of PBBM models on an individual basis, allowing for better capturing of the variability of absorption processes, an important consideration, especially for virtual bioequivalence applications.
-
It has been reported in the literature that “default” parameters for colonic permeability in PBPK models may overestimate the contribution of colonic absorption [15]. Given the ability of PBFTPK models to readily estimate termination of absorption, this knowledge can help parameterization of regional dependent absorption for PBPK and IVIVC-PBPK models, especially for MR formulations. This could be accomplished by estimating τ from high dose arms of single ascending dose studies, where for BCS II/IV compounds, absorption is likely not to be complete.
-
Estimation of different absorption time periods (i.e. τ1 and τ2) may also provide insights into in vivo processes that are currently difficult to predict via in vitro data, e.g., precipitation. Recent workshops have discussed these challenges as well as the importance of the use of biopredictive dissolution methods for PBPK models [20, 25]. Thus, an early estimation of τ, based on FIH data could facilitate the development of such dissolution methods.
-
Currently, population pharmacokinetics (popPK) models generally rely on an empirical simulation of absorption using ka/tlag or transit compartment constructs without the necessary consideration of physiological constraints [26]. The potential of adoption of PBFTPK model structure for popPK applications may allow to better connect findings from popPK models to mechanistic simulation via PBPK/PBBM in related applications (e.g., characterization of DDI with acid-reducing agents).
Conclusion
For the first time we report the application of PBBM and PBFTPK models on the same clinical datasets. Both models support the concept of finite absorption time, which has been somewhat underappreciated in traditional pharmacokinetic/pharmacometrics applications. The estimates of luminal concentration from PBPK model were correlated to the absorption rate estimates from PBFTPK models. We propose that additional synergies should be explored moving forward to bring a more mechanistic modeling of the absorption process not only as part of core PBPK models, but incorporate these principles also in modeling applications that currently largely rely on compartmental models.
Notes
Abbreviations: AUC: area under the curve, BCS: biopharmaceutics classification system, CMC: chemistry, manufacturing and controls, FAT: finite absorption time, IVIVC: in vitro in vivo correlation, PBBM: physiologically based biopharmaceutics model, PBFTPK: physiologically based finite time pharmacokinetic, PBPK: physiologically based pharmacokinetic, PE: prediction error
References
Charalabidis A, Sfouni M, Bergström C, Macheras P. The biopharmaceutics classification system (BCS) and the biopharmaceutics drug disposition classification system (BDDCS): beyond guidelines. Int J Pharm. 2019;566:264–81.
Sjögren E, Westergren J, Grant I, Hanisch G, Lindfors L, Lennernäs H, et al. In silico predictions of gastrointestinal drug absorption in pharmaceutical product development: application of the mechanistic absorption model GI-Sim. Eur J Pharm Sci. 2013;49(4):679–98.
Sager JE, Yu J, Ragueneau-Majlessi I, Isoherranen N. Physiologically based pharmacokinetic (PBPK) modeling and simulation approaches: a systematic review of published models, applications, and model verification. Drug Metab Dispos. 2015;43(11):1823–37.
Vinarov Z, Abrahamsson B, Artursson P, Batchelor H, Berben P, Bernkop-Schnürch A, et al. Current challenges and future perspectives in oral absorption research: an opinion of the UNGAP network. Adv Drug Deliv Rev. 2021;171:289–331.
Macheras P, Chryssafidis P. Revising pharmacokinetics of oral drug absorption: I models based on biopharmaceutical/physiological and finite absorption time concepts Erratum/ Pharm Res 37, 206 (2020). Pharm Res. 2020;37(10):187.
Macheras P. On an unphysical hypothesis of Bateman equation and its implications for pharmacokinetics. Pharm Res. 2019;36(7):94.
Chryssafidis P, Tsekouras AA, Macheras P. Revising pharmacokinetics of oral drug absorption: II bioavailability-bioequivalence considerations. Pharm Res. 2021;38(8):1345–56.
Tsekouras AA, Macheras P. Re-examining digoxin bioavailability after half a century: time for changes in the bioavailability concepts. Pharm Res. 2021;38(10):1635–8.
Chryssafidis P, Tsekouras AA, Macheras P. Re-writing oral pharmacokinetics using physiologically based finite time pharmacokinetic (PBFTPK) models. Pharm Res. 2022;39(4):691–701.
Iranpour P, Lall C, Houshyar R, Helmy M, Yang A, Choi JI, et al. Altered Doppler flow patterns in cirrhosis patients: an overview. Ultrasonography. 2016;35(1):3–12.
Sugano K. Theoretical framework II: dissolution. In: Biopharmaceutics modeling and simulations; 2012. p. 33–63.
Sugano K. Lost in modelling and simulation? ADMET DMPK. 2021;9(2):75–109.
Lovering EG, McGilveray IJ, McMillan I, Tostowaryk W. Comparative bioavailabilities from truncated blood level curves. J Pharm Sci. 1975;64(9):1521–4.
Kesisoglou F, Mitra A. Application of absorption modeling in rational design of drug product under quality-by-design paradigm. AAPS J. 2015;17(5):1224–36.
Heimbach T, Kesisoglou F, Novakovic J, Tistaert C, Mueller-Zsigmondy M, Kollipara S. Establishing the bioequivalence safe space for immediate-release Oral dosage forms using physiologically based biopharmaceutics modeling (PBBM): case studies. J Pharm Sci. 2021;110(12):3896–906.
Kesisoglou F, Balakrishnan A, Manser K. Utility of PBPK absorption modeling to guide modified release formulation development of Gaboxadol, a highly soluble compound with region-dependent absorption. J Pharm Sci. 2016;105(2):722–8.
Patel S, Zhu W, Xia B, Sharma N, Hermans A, Ehrick JD, et al. Integration of precipitation kinetics from an in vitro, multicompartment transfer system and mechanistic oral absorption modeling for pharmacokinetic prediction of weakly basic drugs. J Pharm Sci. 2019;108(1):574–83.
Takano R, Furumoto K, Shiraki K, Takata N, Hayashi Y, Aso Y, et al. Rate-limiting steps of oral absorption for poorly water-soluble drugs in dogs; prediction from a miniscale dissolution test and a physiologically-based computer simulation. Pharm Res. 2008;25(10):2334–44.
Hintz RJ, Johnsonm KC, Johnson KC. The effect of particle size distribution on dissolution rate and oral absorption. Int J Pharm. 1989;51(1):9–17.
Parrott N, Suarez-Sharp S, Kesisoglou F, Pathak SM, Good D, Wagner C, et al. Best practices in the development and validation of physiologically based biopharmaceutics modeling. A workshop summary report. J Pharm Sci. 2021;110(2):584–93.
Wu F, Shah H, Li M, Duan P, Zhao P, Suarez S. Biopharmaceutics applications of physiologically based pharmacokinetic absorption modeling and simulation in regulatory submissions to the US food and drug administration for new drugs. AAPS J. 2021;23(2):1–14.
Dressman JB, Amidon GL, Fleisher D. Absorption potential: estimating the fraction absorbed for orally administered compounds. J Pharm Sci. 1985;74(5):588–9.
Macheras PE, Symillides MY. Toward a quantitative approach for the prediction of the fraction of dose absorbed using the absorption potential concept. Biopharm Drug Dispos. 1989;10(1):43–53.
U.S. Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research (CDER) Bioavailability and Bioequivalence Studies Submitted in NDAs or INDs — General Considerations https://www.fda.gov/media/88254/download. 2014.
Pepin XJH, Dressman J, Parrott N, Delvadia P, Mitra A, Zhang X, et al. In vitro biopredictive methods: a workshop summary report. J Pharm Sci. 2021;110(2):567–83.
Samant TS, Dhuria S, Lu Y, Laisney M, Yang S, Grandeury A, et al. Ribociclib bioavailability is not affected by gastric pH changes or food intake: in silico and clinical evaluations. Clin Pharmacol Ther. 2018;104(2):374–83.
Mitra A, Kesisoglou F, Dogterom P. Application of absorption modeling to predict bioequivalence outcome of two batches of etoricoxib tablets. AAPS PharmSciTech. 2015;16(1):76–84.
Tosco P, Rolando B, Fruttero R, Henchoz Y, Martel S, Carrupt P-A, et al. Physicochemical profiling of sartans: a detailed study of ionization constants and distribution coefficients. Helv Chim Acta. 2008;91(3):468–82.
Ml B, Holm R, Tønsberg H, Frølund S, Ewon KB, Al N, et al. Function and expression of the proton-coupled amino acid transporter PAT1 along the rat gastrointestinal tract: implications for intestinal absorption of gaboxadol. Br J Pharmacol. 2012;167(3):654–65.
Agrawal NG, Porras AG, Matthews CZ, Rose MJ, Woolf EJ, Musser BJ, et al. Single- and multiple-dose pharmacokinetics of etoricoxib, a selective inhibitor of Cyclooxygenase-2, in man. J Clin Pharmacol. 2003;43(3):268–76.
Shadle C, Rainakrishnan R, Gargano C, Fu I, Luo R, Alexander R, et al. Assessment of dose proportionality, absolute bioavailability, and tolerability of gaboxadol in healthy young adults. Sleep. 2006;29:A40–1.
Bjornsson TD, Mahony C. Clinical pharmacokinetics of dipyridamole. Thromb Res. 1983;29:93–104.
Eckland DA, Danhof M. Clinical pharmacokinetics of pioglitazone. Exp Clin Endocrinol Diabetes. 2000;108(Sup. 2):234–42.
Sun L, Li H, Willson K, Breidinger S, Rizk ML, Wenning L, et al. Ultrasensitive liquid chromatography-tandem mass spectrometric methodologies for quantification of five HIV-1 integrase inhibitors in plasma for a microdose clinical trial. Anal Chem. 2012;84(20):8614–21.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests. Filippos Kesisoglou and Di Wu are employees of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA and may own stock or hold stock options in Merck & Co., Inc., Rahway, NJ, US.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Wu, D., Tsekouras, A.A., Macheras, P. et al. Physiologically based Pharmacokinetic Models under the Prism of the Finite Absorption Time Concept. Pharm Res 40, 419–429 (2023). https://doi.org/10.1007/s11095-022-03357-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11095-022-03357-0