
Abstract
Spiritual bypafssing is a term coined in 1984 by the psychologist and Buddhist practitioner John Welwood to define the use of spiritual practices and beliefs as a way of avoiding dealing with unresolved psychological issues. Despite the popular appeal of spirituality, little research exists about spiritual bypass. The purpose of this study was to explore the perspectives of experts with a background in working with spiritual bypass in clinical settings by conducing 10 semi-structured interviews. The results of the conventional content analysis yielded 63 codes that the authors clustered into 10 categories: (a) Exploring Client’s Spirituality, (b) Definition, (c) Symptoms, (d) Personality Traits and Life Experiences, (e) Causes, (f) Negative Consequences, (g) When Spiritual Bypass Is Not Unhealthy, (h) Ways to Treat, (i) Healthy Spirituality, and (j) Longevity. The study’s findings offer future researchers a broader view of the phenomenon of spiritual bypass, including its main symptoms, causes, and consequences and methods of treatment.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
The pleasure principle states that, as humans, we seek the immediate gratification of desire; in other words, we tend to seek pleasure and avoid pain (Freud 1952). The motivation to seek pleasure and avoid pain is well documented throughout history, extending back to the ancient Greeks and their philosophy of hedonism. The ways to avoid pain are of course diverse; they include alcoholic, narcotic, erotic, intellectual, material, selfish, or spiritual means (Masters 2010). Though they may be common ways to create an anesthetic or analgesic effect, they end up catalyzing even more pain (Masters 2010).
Over the past several decades, spirituality has been studied as an important aspect of human development (Beutler and Clarkin 1990; Fowler 1981), and a considerable body of research has consistently demonstrated that there is a positive association between spirituality and health (e.g., Koenig 2012; Larson and Milano 1995; Pargament et al. 1998). Because of this upward trend, scholars have focused on ways spirituality can be incorporated in counseling. Examples of this are the publications of Cashwell and Young (2011), Maher and Hunt (1993), Miller (2003), Parker (2011), Pargament (2007), and Richards and Bergin (2005).
Although counselors consider their clients’ spiritual practices and beliefs as potential resources for improving their physical and mental health, the shadow side of spirituality is often overlooked (Welwood 2000). In this regard, an area that has still received limited attention within the clinical and psychological literature is the issue of spiritual bypass (Cashwell et al. 2004), which is defined as the use of spiritual practices and beliefs to avoid dealing with painful feelings, unresolved wounds, or uncomfortable issues (Welwood 2000).
Although the term spiritual bypassing was first used in the 1980s, few scientific studies have explored this phenomenon. Among published works, there is a shortage of research focused on analyzing the perspective of counselors on how to identify and treat spiritual bypass with clients. To address the lack of existing literature, the current study focused on exploring the perspectives of experts with a background in working with spiritual bypass in clinical settings in order to describe spiritual bypass and its main symptoms, causes, and consequences and methods of treatment. First, a description of spiritual bypass is presented, followed by the study itself based on a conventional content analysis of 10 semi-structured individual interviews. A thorough understanding of how experts with a background in working with spiritual bypass in clinical settings explore the phenomenon of spiritual bypass and work with their clients can provide scholars a solid foundation for designing studies that will assist in the creation of assessment tools for spiritual bypass, measuring its main negative consequences, and establishing parameters of treatment.
Spiritual bypass
The term spiritual bypassing was coined by the psychologist and Buddhist practitioner John Welwood in 1984 to address the use of spiritual practices and beliefs to avoid dealing with unresolved personal or emotional issues. Later, Charles Whitfield (1987, 1995, 2003), a medical doctor and psychotherapist who specialized in trauma, addiction recovery, and co-dependence, also used the term. According to Whitfield (2003), spiritual bypass refers to a condition in which an individual tries to avoid or bypass necessary work on the psychological plane by jumping directly to the spiritual plane. The concept of spiritual bypass was also referred to by Harris (1994) as “premature transcendence” and “high level of negation” as a way of denoting this common way in which clients attempt to skip over necessary steps in their spiritual development.
Spiritual bypass usually occurs when a person adopts the polarized thinking that “human” issues are unimportant, eventually neglecting relationships and other day-to-day aspects of life as a result of spiritual bypass (Sovatsky 1998). Consequently, spiritual exercises and disciplines may be compartmentalized, creating a gap between the sophistication of the spiritual practice and the individual’s level of personal development (Welwood 2000). In short, spiritual bypass serves an avoidance function; it allows the individual to avoid the often difficult and painful psychological work of healing old wounds (Cashwell et al. 2010). The main symptoms of spiritual bypass listed in the literature are emotional alienation and repression; excessive detachment; too much emphasis on the positive side of development; blind or overly tolerant compassion; minimization or negation of one’s own shadow; illusions about one’s own awakening; viewing everything, including suffering, as illusory as a way to escape from suffering; disregarding the personal or mundane; and exaggerating certain aspects of development (Cashwell et al. 2004; Masters 2010). Because it is a form of escape, spiritual bypass eventually makes possible the manifestation of a series of negative consequences such as an exaggerated need to control others and the self, shame, fear, dichotomous thinking, emotional confusion, high tolerance of inappropriate behaviors, co-dependency, and pain (Welwood 1984, 2000). Other negative consequences of spiritual bypass would be obsession or addiction, a blind belief in charismatic teachers, spiritual materialism (the use of spiritual practice for material gain), and abdication of personal responsibility (Cashwell et al. 2004). Finally, spiritual bypass compromises long-term spiritual well-being because it leaves the process of spiritual development incomplete (Cashwell et al. 2007).
Method
The purpose of this study was to better understand the perspectives of experts with a background in working with spiritual bypass in clinical settings regarding the characterization of spiritual bypass and to identify how they usually treat clients who are experiencing this phenomenon. To accomplish the aims of this study, five central research questions were developed. Each research question is listed here, followed by sample interview questions in parentheses:
-
How do experts with a background in working with spiritual bypass in clinical settings explore the beliefs and spiritual practices of their clients? (How do you explore the spiritual beliefs and practices of your clients?)
-
How do experts define the phenomenon of spiritual bypass? (How would you define spiritual bypass? What are usually the main symptoms of spiritual bypass? Do you believe there are any personality traits, characteristics, or life experiences that make people more likely to have a predisposition for spiritual bypass?)
-
In the experts’ view, what are the main causes and consequences of spiritual bypass? (What are the possible causes of spiritual bypass?)
-
How do experts treat spiritual bypass, and what would they consider a definition of healthy spirituality? (What approaches do you usually use to treat clients who are experiencing spiritual bypass? In your view, what is the path to healthy spiritual development and practice?)
-
What is the origin of spiritual bypass and its historical evolution? (Do you believe spiritual bypassing has always been present in society? Do you notice any evolution of the phenomenon in recent decades? If so, for what reasons?)
Sample
This study used a sample of 10 experts. The identification of these experts was based on articles, chapters, and books focused on the phenomenon of spiritual bypass. First, all authors who had written scientific articles, chapters, or books, and those who had been mentioned in other authors’ publications as experts in the subject, were selected. Finally, 13 experts with a background in working with spiritual bypass in clinical settings were identified and invited to participate in the study. Out of the sample of 13 experts contacted, 10 agreed to participate in the study (N = 10; 8 males and 2 females). All 10 interviewees currently reside and work professionally in the United States.
Data collection and analysis
Ten semi-structured interviews were conducted with the experts. Each interview was conducted by videoconference, lasted approximately one hour, and was recorded in video and audio and later transcribed. The interviews were analyzed using conventional content analysis (CCA; Hsieh and Shannon 2005). CCA is usually used in studies that focus on exploring a phenomenon when the existence of theoretical literature or research on the phenomenon is limited. In this way, researchers use inductive logic, avoiding imposing any categorical system of data interpretation (Hsieh and Shannon 2005). In addition, the CCA offers researchers the ability to give their findings theoretical cohesion, which may potentially inform the direction of future research and substantiate future findings (Fox et al. 2015).
The analysis of the data began with the principal investigator (Picciotto) reading each of the transcribed interviews to immerse herself in the experience of the experts and to get a sense of the whole phenomenon. Next, the principal investigator read each of the interviews again, taking notes on her first impressions, thoughts, and initial analyses, and then developed codes for each unit of meaning identified. Definitions were developed for each of the codes that were later grouped into clusters of related meanings to develop categories. The categories were also defined to clarity their meaning. A peer debriefer (Fox) audited the process by reviewing the research methodology, the coding process, and the proposed revisions to the codes or categories.
Threats to validity and verification strategies
According to Hsieh and Shannon (2005), a potential weakness of CCA is that it can fail to provide adequate context for the phenomenon investigated and therefore overlook key categories. To ameliorate this potential threat to validity, we followed Creswell’s (2013) recommendation that all qualitative research should incorporate at least two forms of verification into its methodology. In the present investigation, we included positionality, investigator triangulation, data triangulation, peer debriefing, and thick, rich description.
Findings
The CCA analysis yielded 63 codes, all of which are defined in Table 1. Each code was reanalyzed in context, and all codes were grouped into ten categories. The ten categories are (a) Exploring Client’s Spirituality, (b) Definition, (c) Symptoms, (d) Personality Traits and Life Experiences, (e) Causes, (f) Negative Consequences, (g) When Spiritual Bypass Is Not Unhealthy, (h) Ways to Treat, (i) Healthy Spirituality, and (j) Longevity. Each of the categories is described below and provided with thick, rich descriptions, using examples from the transcripts to clarify their meaning.
Exploring Client’s Spirituality
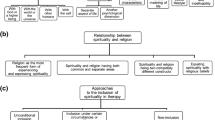
The first category, Exploring Client’s Spirituality, is defined as “ways used by counselors to understand client’s spirituality.” The category captures the ways in which experts usually explore their clients’ spiritual practices and beliefs during therapy. Two distinct ways of exploration were identified. The first, used by most of the experts interviewed, is asking questions during the intake, which consists of the counselor asking questions related to spirituality during the intake in order to have an overview of the role of spiritual beliefs and practices in the life of the client. According to the answers and degree of interest of the client in the subject, the counselor might follow up with more in-depth questions. One of the participants said: “Well, in the intake on the first session, I ask clients about their spiritual worldview, and about their family background, if their family has a particular religion or orientation, if there was a particular spiritual lineage they were brought up in. ..”
The second way is by using incomplete sentences through which the counselor initiates a sentence directed to a particular subject, in this specific case directly related to spirituality, and asks the client to finish the sentence. As one participant said,
I like to use incomplete sentences . . . so I’m working with someone else and wait for them to finish my sentences. Those might be like: “What right now I’m feeling . . .”, “What I wish is . . .,” and after a number of sentences I get fairly deep and they might say something like: “What my spiritual beliefs are . . .” or “What I hold to be sacred is . . .” and related things, like “What I assume happens when I die is . . .” or “I feel most connected to the source of things when . . .” I just make them up for each person! And I see if that is in their way, if it supports the work and what I want to know.
Definition
The next category identified is called Definition, and it represents an “explanation of the meaning of spiritual bypass.” That is, all the meanings that the experts interviewed gave for spiritual bypass were codified here. Five different codes were found to define this phenomenon. Regarding the first, using spirituality to avoid something, the participants described spiritual bypass as the use of spiritual beliefs and practices to avoid dealing with psychological issues or trauma, relationship difficulties, emotional hassles, and developmental tasks. One participant said: “It’s the use of spiritual beliefs and practices to avoid, it’s the big word, it’s ‘avoid!’ to avoid dealing with relationship difficulties, emotional hassles, challenges, developmental tasks. .. so basically it’s ‘avoidance in spiritual robes.’”
The second code in this category is called self-defense and justification and captures the meaning of spiritual bypass as the use of spiritual ideas and beliefs in self-defense and as justification for acting on impulses. As one of the experts said,
I think spiritual bypass is using spiritual ideas and beliefs into as self-defense . . . sort of the old super ego substitutes the “old shoulds” for “new spiritual shoulds”! It’s the same basic process . . . it’s still holding down impulses that want to come up and so it’s a defensive process . . . It can also be used, I think, as a way to justify . . . But rather than holding vessels, it can be a justification for releasing impulses! For example, Islamic terrorism uses a system to justify murder and terrorism.
The third code is overall preference for or privileging of spiritual realities, which defines spiritual bypass as the polarization of spiritual practices as superior and psychological or physical work as inferior. One of the participants said,
The way that I would define spiritual bypass is kind of an overall preference for spiritual privileges or basic realities and so it’s more about how people tend to take on that kind of unconscious presupposition of how reality works in relation to what they call spiritual.
The fourth identified code was spiritual development illusion in which spiritual bypass is defined by the fact that the person believes they are at a level of spiritual development superior to their actual level. As one expert reported:
It’s the personal experience of someone that believes he or she is in a particular spiritual stage of development that he or she isn’t! So the perception, the meaning of certain experiences are kind of dyed by the experience or belief that they are in a certain stage and . . . being blind, basically to their own reality, you know, it’s just too based on self-assessment. And there’s ego inflation that happens because of that.
Finally, the last code, spiritual bypass as a four-category definition, subdivides spiritual bypass into four facets: (1) normal bypass, (2) states-driven bypass, (3) problematic bypass, and (4) narcissistic bypass. Normal bypass is related to developmental models and posits that we all go through some kind of bypass during our spiritual development. Thus, this form of spiritual bypass may not be problematic but just an expression of where we are:
One of them is more influenced by developmental models. . . So my understanding of the stages is that the stages have only certain capacities, and one of those capacities is the ability to let go of what we might call certain kinds of wishful thinking or self-deception or beliefs which are not grounded in experience but that those beliefs naturally arise during stages, so sometimes when people that sound like a spiritual bypass it’s really not a problem, it’s just an expression of where they are in their development, and it may not be something that one would need to challenge.
States-driven bypass involves the experience of spiritual states and the mental and functional disturbances that these can cause in the life of an individual, which one of the participants described as follows:
This is very specific for when people are going through periods of very intense either spiritual opening or spiritual emergency, whatever you want to call it . . . and they’re so what I would call neurologically overwhelmed, just by the states coming, and they’re so compelling that everything else gets put on the side. So when somebody’s going through that kind of thing, they typically push other things aside, but that actually needs to happen so it’s not a problem, it’s only a problem if people stay past the point and that can be, you know, months, it could be a couple of years, it could be longer in theory.
A problematic bypass, in turn, would correspond to the previous code using spirituality to avoid something. One of the experts said,
I’d call problematic bypass, and this is more when people have a lot of spiritual beliefs, they are really using those to push away serious psychological issues, it’s not because they’re going into super high states all the time and are compelled by that, they have to set up their life . . . either consciously or unconsciously to avoid.
On the other hand, in narcissistic bypass there is a melding within the person of strong narcissistic tendencies with spiritual ideas, beliefs, or experiences, as stated by one of the participants:
People with narcissistic personality disorder or features do have basically moved into the spiritual world as a way to communicate their narcissism. . . . Some of them may have authentic spiritual experiences; some of them may just be speaking about it in a convincing way . . . I’ve seen both! But in either case, the problem is more that the structure of their personality is very out of touch with the whole set of basic core emotions and feelings so it’s almost like a separation, like there are two layers of them and they cannot see that lower layer, so that’s a harder situation.
Symptoms
The category of Symptoms encompasses “the main symptoms of spiritual bypass.” This category possesses more unique codes than any other category: 16 in total. One of the symptoms frequently identified by the participants was emotional dissociation, described as the disconnection of the individual from their emotional life or great difficulty getting in touch with their own emotions. Relatedly, another identified symptom was anger phobia, which is the fear of becoming angry. The third code identified in this category was intellectual dissociation, in which there is a transition to reason and the person avoids uncomfortable emotions by focusing on facts and logic. One participant described this as “intellectual dissociation, with the cognitive intelligence often being far ahead of moral and emotional intelligence.” Another symptom described was minimizing or denying our shadow side and negativity, which would be a superficial acceptance or nonacceptance of the shadow or the negative side of humanity. The fifth code, closely aligned with the previously reported symptom, was of overemphasis of the positive, in which an unrealistic emphasis of the positive side of situations occurs.
Following this, a series of symptoms related to interpersonal competencies was identified. As a sixth code, relationship problems was described by the respondents as difficulty in engaging in relationships, not being open, available, or believing that they can engage in a relationship, or idealizing a relationship as possible only with an ideal spiritual partner. Another symptom described was sexuality dysfunction in which the person exerts their sexuality in an unhealthy way by practicing forms of polyamory or completely avoiding any type of sexual relationships. The eighth code identified was avoidance of toxic people, in which the individual avoids contact with people whom they judge to be nonspiritual or toxic or with whom they have painful or strained relationships. Next, the category of narcissism and grandiosity in the spiritual domain describes a person who acts as if they are spiritually superior to others, the owner of reason, and the holder of all the answers; the only one who knows and who sees beyond. As a tenth code, the experts reported that blind following is based on the creation of a blind belief in charismatic or cult-like leaders. The next symptom, blind compassion, denoted an exaggerated tolerance or undiscriminating attempt at caring through which the individual ends up being overly permissive. Much in line with this code is the fear of confrontation, in which a person attempts to not disappoint others; the person is afraid to put up a barrier, to challenge, to disagree, or to confront.
The thirteenth category code was the avoidance of responsibilities, which was defined as the individual’s tendency to avoid responsibility (such as dealing with work or money) by not taking their career seriously or making long-term financial plans. The next code, magical thinking, describes a mixture of superstition, perception of illusory connections, conflation of correlation with causation, wishful thinking, and awaiting divine intervention instead of taking personal responsibility. One participant said:
That’s the type of thinking that’s common to young children! Where they literally assume that they’re walking along and the sun seem to be always over their left shoulder, the sun’s following them! We know it’s not true, but for them it seems true! And a lot of adults will engage in magical thinking when they’re in severe pain, crisis, a dear one has died—they start to think magically, like, if I only place the shoes in the right part of the house, maybe my dead partner will return!
Finally, in the last code of this category, disconnection from the body, the person loses intimacy with their own body, including a certain disdain for the physical body and lacks grounding in the body.
Personality Traits and Life Experiences
The category of Personality Traits and Life Experiences refers to those codes that are clustered under the definition “some personality traits and life experiences that can increase the predisposition for spiritual bypass.” Seven codes were identified in this category; five are related to personality traits and two to life experiences. The first code identified was the attachment person, which refers to individuals with an unhealthy attachment pattern (i.e., children who had breaks from their primary caregiver resulting in unmitigated pain, abuse, neglect, or other ways in which they did not have their needs met that subsequently impaired their ability to develop healthy emotional attachments). These individuals tend to be more prone to engage in spiritual bypass. In this category, co-dependency was identified to illustrate that individuals with an excessive reliance on other people for approval and a sense of identity tend to be more prone to engage in spiritual bypass. As one participant said:
I think co-dependency can be a factor, so again if we’re talking about recovery if somebody doesn’t really have a sense of self and they’re coming into a 12-steps program, and someone says to them “You’re just being selfish and self-centered and you need to pray about it,” they are going to take that direction on wholesale and not really be able to unpack some of the subtleties and what it means to both have all of their feelings and have a spiritual practice. When I’ve seen it be pretty devastating is when people don’t have a solid sense of themselves.
The third code in this category is neuroticism, which means that people who score high on neuroticism (who are more emotionally reactive and vulnerable to stress) in the Big Five personality traits tend to have a higher predisposition to spiritually bypass. In relation to the fourth code, openness (which is also a reference to the Big Five), there was some divergence of opinion among the interviewees. Some reported a higher incidence of spiritual bypass among people who score both high and low in openness (appreciation for art, emotion, adventure, unusual ideas, curiosity, and variety of experience). The last code related to personality traits is obsessive compulsive personality disorder (OCD), which implies that people with personality features consistent with OCD may be more predisposed to spiritual bypass. One of the participants said:
People who have the tendency to OCD where the perfection is so important, you know, I always talk to my clients about the realm of the gods and that we all are human beings, so that we all love the gods, it’s perfect, right? Everything makes sense, it’s meaningful, it’s organized, you know? There are like several of them taking care of things. . . . So I always ask them, like, “What you’re talking about is from the realm of the gods or the human beings?” If you’re aiming at becoming one, you know, that’s . . . your choice. . . . And most likely, you know, you’re going to still be a human being, welcome to that realm of messiness, you know? So the idealistic mind, the one who just, like, looks into perfection, is the one that suffers.”
Regarding life experiences, the first code identified was trauma survivors, which implies a greater tendency to engage in spiritual bypass among people who have experienced very difficult situations with a high level of pain or trauma during their life journey. The seventh code, growing up in a non-conducive environment, can increase the tendency to spiritual bypass, as described in the following example by one of the participants:
. . . people who grow up in non-conducive environments either from low socioeconomic status or parents who might be addicted or . . . you know, something like that, I think there’s a possibility that they might learn, you know, how to engage in spiritual bypass.
Causes
Next, the category Causes was identified, which captures in the view of the interviewees “the possible reasons why people experience spiritual bypass.” Participants brought up five possible causes. First, the issue of avoidance of pain was addressed, which refers to a person’s low tolerance of facing, dealing with, and working through pain and things that hurt as a possible cause for spiritual bypass. One of the participants said:
Probably just, I think, a natural avoidance of things that hurt. That is totally natural, and to some extent normal. We have diagnostic labels for people who consistently do things to hurt themselves or hurt others. It is natural to avoid something painful, but when that avoidance is really stifling to one’s growth, the avoidance itself has to be addressed.
A second possible cause, a defensive structure, referred to ways in which a person’s defensive structure and the consequent use of defense mechanisms could cause the phenomenon of spiritual bypass. The third code, religious/spiritual leaders and communities, described the negative influence or lack of psychological knowledge of religious or spiritual leaders or communities as possible causes for spiritual bypass, as illustrated by the following quotation from one of the participants:
I do think that sometimes religious leaders in religious communities . . . I consider myself both religious and spiritual so I’m not “religion bashing” here, I think there are many, many good things that happen in religious communities, but I do think there are sometimes where it’s encouraged by leadership in religious communities . . . the example that I often give when I’m talking to students about it, for example, is you experience a death in your immediate family or some very close friend and sometimes the religious community will say, for example, in a Christian community, which is where I practice, will say, “Don’t be sad, he or she is going to a better place and they’re not suffering anymore.” And you know, my belief system tells me that that’s completely accurate, that that is true . . . but I’m not sad because they’re not here anymore, I’m sad because I miss them and I long for them and I’m grieving for that and so psychologically being sad is perfectly right!
Another identified cause was receiving “wrong” messages in which receiving strong messages around self-worth or psychological misinformation that it is not okay to feel anger, sadness, fear, or shame can cause spiritual bypass. The last code in this category is the lack of time or social context conditions for spiritual development, in which a possible cause of spiritual bypass would be that the individual does not live in an environment or social context that encourages their spiritual growth and therefore sabotages their spiritual development.
Negative Consequences
The next category, Negative Consequences, denoted “the possible negative effects or outcomes of spiritual bypass.” Eight negative consequences were coded. The first, getting stuck, happens when a person stays paralyzed, does not know what to do, feels lost, and ends up going in circles or not evolving. One of the participants said, “We stay stuck; we don’t evolve! We go in circles and we rise above that without ever having faced things! And we miss so much when we do that! We miss life, like we’re in a bubble!” In line with the first code, not growing spiritually captures cases when a person does not evolve and remains young and even immature in terms of their spiritual life. Connected to the first two negative consequences, blindness denotes when a person lacks the capacity for self-awareness and ends up losing contact and access to the self, which is illustrated in this quotation from one of the participants:
One of the negative consequences is that they sort of have these blinders on where they can’t see outside of “this is the route, this is where I have to do, this is how I get there,” and they lose access to everything to the left or the right of that, which means they also lose access to themselves.
The fourth code identified in this category, staying immature, is linked to the previously described symptom of magical thinking, the consequence in this case being that the person does not grow cognitively and stays stuck in childish illusions of magical thinking.
The final negative consequences identified are consequences that not only directly affect the person who is experiencing spiritual bypass but that also affect others in their social circle. The first, suffering and causing unnecessary suffering, captures instances of suffering caused by spiritual bypass, which can vary in intensity depending on how significant the issues are that are faced by the person. One participant said:
People continue to just suffer unnecessarily . . . and they cause unnecessary suffering, and that can be smaller or more intense, it depends on how significant the issues that they have are or how deep the problems are. . . . So yeah, that sounds like a simple answer, but it’s just the whole range, it can be the whole range! I mean, all the way to the point where . . . you know, I talked to a guy the other day who has done a lot of spiritual practice but he’s been suicidal for, you know, a couple of years.
Another consequence, not taking care of their relationships and families, refers to people who tend to devote so much time to their spiritual practices and beliefs that they end up not devoting enough quality time to their relationships and families. Similarly, disconnection describes a difficulty connecting with others, possibly negatively affecting their empathic attunement with other people. Finally, the last negative consequence is preying on other people’s indecision and avoidance, and this denotes instances where people or institutions take advantage of the vulnerability and stagnancy of people who spiritually bypass by selling products and services that often exacerbate their spiritual bypass.
When Spiritual Bypass is Not Unhealthy
In spite of the several negative consequences listed, the participants also identified times when spiritual bypass was not problematic or could even be necessary to coping or survival. The category When Spiritual Bypass Is Not Unhealthy was defined as “times when spiritual bypass has no negative consequences and can be useful or even necessary to someone’s development.” In this category, two distinct codes were identified. The first, natural step of spiritual development, captures the belief of some experts that spiritual bypass can manifest as a natural step in our spiritual development and that practically everyone who embraces a spiritual journey ends up experiencing some type of bypass. As one participant said:
I think that probably all of us have gone through spiritual bypass in our spiritual development and are still kind of . . . I imagine it can be part of a normal spiritual development to get fascinated for example with that particular belief and then just, you know, put all of you to make that . . .
The second code, short-term coping strategy, describes the use of spiritual bypass as something useful for coping with high stress or difficult situations for a short period of time. One of the experts said:
It is just like any other psychological defense mechanism; it serves an adaptive function. And so we don’t put psychological defense mechanisms in that category—they’re all bad! We actually put them in the category of “they are good for certain points of life.” But they all tend to outrun their usefulness and they become maladaptive. So I think the same is true for spiritual bypass in that it can serve in an adaptive function, especially when people are in trauma.
Ways to Treat
The category Ways to Treat is defined as “ways in which counselors work with clients experiencing spiritual bypass.” Eight codes were identified in this category. The first code, empowerment-base model, described a client autonomy-based model in which one explores the client’s goals for counseling and helps them perceive what is working so that they can develop the skills and capacity to gain control over their life. The second code, existential approach, views the tendency to avoid what is painful and the fact that suffering will not go away on its own as existential givens and is based on what the person wants to achieve. The third method of treatment is to stay sensitive to the purpose that spiritual bypass serves by understanding what purpose the bypass is serving in the client’s life. One of the participants said:
I try to stay sensible to what purpose it is serving in their life. So if it’s serving an adaptive function now they might be in too much pain to really be able to look at that coping skill. Is it outliving its usefulness? So I try to put it in the context of the relationship that I have with them.
The fourth code, empathetic approach, denotes putting yourself in the client’s shoes, being empathetic, connecting with them, and finding their language.
The fifth code, customized to each category, is related to the spiritual bypass code as a four-category definition identified under the Definition category above. Normal bypass does not need to be treated because it is an aspect of spiritual development that is to be expected. States-driven bypass is treated by talking about the psychological experiences of the client and using supportive interventions. Problematic bypass treatment is focused on helping the person realize that they are experiencing spiritual bypass and dealing with the psychological problems that lie beneath it. Lastly, narcissistic bypass should be treated as narcissism in general. The sixth code, customized to each client, captures the belief that each client should be treated with a unique and customized treatment plan. One participant said, “So it’s a unique journey for me with each person. I have a unique therapy for each person, each session; I make it up each time!” The seventh code, as other defenses, describes treating spiritual bypass in the same way other psychological defenses are treated in the therapeutic process. Finally, the eighth code, helping the client connect to the self, describes the use of various therapeutic techniques that support the client to have a deeper contact with their self.
Healthy Spirituality
The ninth category, Healthy Spirituality, represents all the codes clustered under “the path for healthy spiritual development and practice.” Seven codes were identified in this category. The first code, paying attention to different areas of life and dimensions of the self, denotes a path to healthy spiritual development that consists of seeking to be attentive and working the different areas of life and being, such as work, relationships, health, and emotions. One participant said, “Develop yourself in all the realms that you are! In all the dimensions, like, develop yourself physically, mentally, psychologically, intellectually.” The second code, possibility of connecting with their emotional world, posits that the path to a healthy spiritual life exists when a person’s spiritual practices and beliefs enable them to connect with their emotions. The third code is doing psychological work, in which the participants believed that the path to a healthy spirituality would be in the conjugation of spiritual practice with therapeutic work. One of the participants reported,
We have to put ourselves in therapeutic practices that address these issues and then we have to put ourselves maybe in spiritual practices . . . so people who only do psychology or therapy sometimes just get so caught up in trying to solve everything that way. . . . And then people who only do spirituality are much more likely to bypass, people who do both are going to get closer to the center! So I think it’s that cross.
The fourth code in this category is greater compassion and self-compassion, which defines healthy spirituality as a path that brings one to a place of compassion for oneself and others. The fifth identified code is called Dharma, Sangha, and Buddha and refers to the path of healthy spirituality as the conjunction of having a set of values, a group of people, or a community to become a part of and to serve as a standard. Similar to the previous code, the seventh code identified is community and guidance, which refers to the fact that the individual has a support group and environment or a person who plays the role of mentor, guide, or spiritual teacher. The final code in this category is involvement with the world, in which the path to a healthy spirituality would be spiritual practices that would help the individual to engage in the real world with real people.
Longevity
The last category identified was Longevity, which was defined as “how long spiritual bypass has been present in society.” In this category, the participants provided three different views expressed in the following three codes. The first, for centuries, captured the belief that spiritual bypass is something that has been present in the lives of human beings for centuries. As one of the participants said, “Ever since human beings gained self-awareness, their sentience along with that blossomed with the desire to avoid what’s painful and lie to ourselves for temporary relief. So this is as old as self-awareness. It goes with it.” The second code, more prevalent in the last 50 to 75 years, defined the belief that spiritual bypass has existed for a long time but has become more prevalent in the last 50 or 75 years. One of the interviewees said,
I mean, first of all, we weren’t talking about spiritual bypass 50 or 75 years ago at all! It just wasn’t out there. . . . And you know, there is kind of . . . I think we have the luxury in more modern society of more people doing more psychological work.
Finally, the third code, more recent, reflects the view of those who believe spiritual bypass is a more recent phenomenon, as the following quote from one of the experts illustrates:
I think that traditional society produced much more stable lives. . . . because the rules were so set and determined by class or sex or ethnicity or religion. So no one is really making a lot of choices and I think that . . . therefore there’s probably a lot of “expectable bypass” but probably not a lot of the complexity that leads to the “problematic bypass.” Also, there’s probably not as many people doing intense spiritual practice and living in the world, you know, they don’t have access to those teachings, they were often highly guarded, people didn’t read so you couldn’t pick up a card toll, you know, in your bookstore and learn some of the deepest teachings.
Discussion
The purpose of this study was to explore the perspectives of experts with a background in working with spiritual bypass in clinical settings. In short, 63 codes in 10 categories describing spiritual bypass were identified. We will now discuss the findings in the context of the research questions before addressing the implications of the data. Then, some preliminary explanations and hypotheses related to the findings will be provided.
First, we asked the sample of participants, “How do experts with a background in spiritual bypass in clinical settings explore the beliefs and spiritual practices of their clients?” In general, the experts used the intake to begin the exploration of the topic through questions that allowed them to understand the role of spiritual practices and beliefs in the client’s life or to explore such practices and beliefs in their client’s spiritual journey. For example, some used incomplete sentence exercises to explore the process and functions of spirituality. According to the information obtained and the client’s interest in the subject, the counselor might or might not ask more in-depth questions.
Next, we posed the following question: “How do the experts characterize spiritual bypass?” From this line of questioning, we explored how the participants defined spiritual bypass and the main symptoms and personality traits or life experiences that would make a person more predisposed to experience the phenomenon. Some responses were very much in line with the existing literature, such as the view of spiritual bypass as the use of spiritual beliefs and practices to avoid dealing with psychological issues or trauma, relationship difficulties, emotional hassles, and developmental tasks (see Welwood 2000), privileging the spiritual over the psychological (see Whitfield 2003), and understanding that spiritual bypass could be defined as a state in which the person wrongly believes that they have attained a certain level of spiritual development (i.e., premature transcendence; Harris 1994). Adding to this body of knowledge, the most complex definition of spiritual bypass we discovered in our findings divided the phenomenon into four distinct categories. This definition incorporated the previous definitions but distinguished them according to causes and symptoms, which may help either in the identification of the phenomenon or in providing more appropriate forms of treatment. Another interesting aspect that emerged from our findings in this regard was that spiritual bypass is not always something problematic but can be seen as a natural phase of spiritual development or even as adaptive, as a coping strategy.
Regarding symptoms, the findings revealed 16 principle symptoms of the phenomenon, adding context and nuance to the existing literature not only in the quantity but also in the quality of the descriptions. Concerning personality traits and life experiences that predispose people to spiritual bypass, the experts identified five personality traits and two themes related to life experience, which offer interesting material for a better understanding of the phenomenon as it can help identify the predisposition for spiritual bypass and also understand its origin.
The third research question we posed was, “In the experts’ view, what are the main causes and consequences of spiritual bypass?” The causes experts discussed were in line with the existing literature (Welwood 2000). From their viewpoint, spiritual bypass arose from avoiding pain and the natural use of defense mechanisms. However, other causes were noted that are less common in the scholarly literature, including the influence of communities and religious leaders, receiving strong messages about self-worth that may encourage the development of low self-esteem, and living in environments or social contexts that are not conducive to spiritual development. Understanding such causes may help clinicians to more effectively address spiritual bypass. With respect to negative consequences, the findings would indicate that spiritual bypass, in general, can disrupt both the spiritual and psychological development of the individual and consequently negatively affect the individual as well as people in their social circles.
The fourth research question was, “How do experts treat spiritual bypass and what would they consider a definition of healthy spirituality?” Regarding treatment methods, experts noted several viable options. In general there is no definite strategy for treating all cases of spiritual bypass; rather, the therapeutic technique needs to be tailored to the individual client, echoing the wisdom of Gordon Paul’s (1967) question, “What treatment, by whom, is most effective for this individual with that specific problem, and under which set of circumstances?” (p. 111). Concerning the definition of healthy spirituality, the responses were multidimensional, including paying attention to all dimensions of one’s own being and areas of life, the possibility of contact with one’s emotions, doing psychological work in parallel with spiritual work, being in a place of compassion for yourself and for others, and being able to combine three things—a set of values, standards, and belonging to a community—to have the support of a guide or group and involvement in the real world. The answers to this topic are interesting in the way that they enable people to seek a balance in their spiritual lives and avoid spiritual bypassing.
Finally, the last question was, “What is the origin of spiritual bypass and its historical evolution?” The answers to this question were the most varied. Some of the experts believed that the phenomenon has been present for hundreds of years; others believed that although it has been present for many years, it has become more prevalent in the last 50 or 75 years. Some viewed it as a more recent phenomenon.
Clinical implications
As noted earlier, counselors should be able to assess the role that spiritual practices and beliefs have in relation to the therapeutic issues of their clients, which includes knowing how to identify, contextualize, and treat spiritual bypass. The current study has provided relevant information to help counselors understand in greater depth the phenomenon of spiritual bypass, to have a better understanding of its symptoms, causes, consequences, and forms of treatment, presenting results that add content to the previously published literature. The study showed that there are still no parameters for its treatment. In addition, the creation of assessment tools for spiritual bypass would help counselors to identify the phenomenon in their clients.
Limitations and implications for future research
The limitations of this study are threefold. All qualitative research is inherently limited by the fact that its findings cannot be generalized to people who were not included in the study sample. In addition, the sample was demographically homogeneous; it only included experts living in the United States. Thus, we do not know whether the experience of spiritual bypass is the same in the rest of the world. In addition, the study only examined the views of experts who treat patients and not those who have experienced spiritual bypass themselves. Although the study brings important content to the exploration of the phenomenon, it is still only a partial view.
With regard to future research, we suggest that three types of studies be considered. The first of these would be to apply similar research but with a sample of experts with a background in working with spiritual bypass in clinical settings living in other countries to get a more global perspective of spiritual bypass. The second study could involve qualitatively analyzing the phenomenon of spiritual bypass based on firsthand experience. And finally, based upon the findings from these two lines of inquiry, it is suggested that quantitative research be conducted to investigate the psychological development of the individuals and the experience of spiritual bypass using variables such as symptoms, causes, personality traits, and negative consequences of spiritual bypass discovered in these investigations.
Conclusion
The research to date focused on the phenomenon of spiritual bypass using the methods of the social sciences is insufficient. This study examined the perspectives of experts with a background in working with spiritual bypass in clinical settings and provides a good description of its phenomenology from their perspectives. The findings obtained provided substantial answers to the five research questions, and the study’s findings can help counselors identify spiritual bypass in their clients, understand its implications, and develop treatment approaches. Lastly, this investigation provides new directions for the empirical research of spiritual bypass using qualitative and quantitative methodologies.
References
Beutler, L. E., & Clarkin, J. (1990). Systematic treatment selection: Toward targeted therapeutic interventions. New York: Brunner/Mazel.
Cashwell, C. S., & Young, J. S. (Eds.). (2011). Integrating spirituality and religion into counseling: A guide to competent practice. Alexandria: American Counseling Association.
Cashwell, C. S., Myers, J. E., & Shurts, M. (2004). Using the developmental counseling and therapy model to work with a client in spiritual bypass: Some preliminary considerations. Journal of Counseling & Development, 82, 403–409.
Cashwell, C. S., Bentley, P. B., & Yarborough, J. P. (2007). The only way out is through: The peril of spiritual bypass. Counseling and Values, 51, 139–148.
Cashwell, C. S., Glosoff, H. L., & Hammonds, C. (2010). Spiritual bypass: A preliminary investigation. Counseling and Values, 54, 162–174.
Creswell, J. W. (2013). Qualitative inquiry and research design: Choosing among five approaches. Los Angeles: SAGE Publications.
Fowler, J. (1981). Stages of faith: The psychology of human development and the quest for meaning. San Francisco: Jossey-Bass.
Fox, J., Gutierrez, D., Haas, J., Briganza, D., & Berger, C. (2015). A phenomenological investigation of centering prayer using conventional content analysis. Pastoral Psychology, 64(6), 803–825.
Freud, S. (1952). A general introduction to psychoanalysis. New York: Washington Square Press. (Original work published 1920).
Harris, B. (1994). Kundalini and healing in the west. Journal of Near-Death Studies, 13, 75–79.
Hsieh, H. F., & Shannon, S. E. (2005). Three approaches to qualitative content analysis. Qualitative Health Research, 15(9), 1277–1288.
Koenig, H. (2012). Overview of the research. In H. Koenig (Ed.), Spirituality and health research: Methods, measurement, statistics, and resources (pp. 13–27). West Conshohocken: John Templeton Press.
Larson, D. B., & Milano, M. A. (1995). Are religion and spirituality clinically relevant in health care? Mind/Body Medicine, 1(3), 147–157.
Maher, M., & Hunt, T. (1993). Spirituality reconsidered. Counseling and Values, 38, 21–28.
Masters, R. A. (2010). Spiritual bypassing: When spirituality disconnects us from what really matters. Berkeley: North Atlantic Books.
Miller, G. (2003). Incorporating spirituality in counseling and psychotherapy. Hoboken: Wiley.
Pargament, K. (2007). Spiritually integrated psychotherapy: Understanding and addressing the sacred. New York: Guilford Press.
Pargament, K. I., Smith, B. W., Koenig, H. G., & Perez, L. (1998). Patterns of positive and negative religious coping with major life stressors. Journal for the Scientific Study of Religion, 37, 710–724.
Parker, S. (2011). Spirituality in counseling: A faith development perspective. Journal of Counseling & Development, 89, 112–120.
Paul, G. L. (1967). Strategy of outcome research in psychotherapy. Journal of Consulting Psychology, 31, 109–118.
Richards, P., & Bergin, A. (2005). A spiritual strategy for counseling and psycho-therapy (2nd ed.). Washington, DC: American Psychological Association.
Sovatsky, S. (1998). Words from the soul: Time, east/west spirituality, and psychotherapeutic narrative. Albany: State University of New York Press.
Welwood, J. (1984). Principles of inner work: Psychological and spiritual. Journal of Transpersonal Psychology, 16, 63–73.
Welwood, J. (2000). Toward a psychology of awakening: Buddhism, psychotherapy, and the path of personal and spiritual transformation. Boston: Shambhala.
Whitfield, C. (1987). Healing the child within. Deerfield Beach: Health Communications.
Whitfield, C. (1995). Memory and Abuse: Remembering and Healing the Effects of Trauma. Deerfield Beach, FL: Health Communications.
Whitfield, C. (2003). My recovery: A personal plan for healing. Deerfield Beach: Health.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Picciotto, G., Fox, J. Exploring Experts’ Perspectives on Spiritual Bypass: a Conventional Content Analysis. Pastoral Psychol 67, 65–84 (2018). https://doi.org/10.1007/s11089-017-0796-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11089-017-0796-7