
Abstract
Background
Chordoma is a rare refractory neoplasm that arises from the embryological remnants of the notochord, which is incurable using any multimodality therapy. Vascular endothelial growth factor (VEGF) is a potent activator of angiogenesis that is strongly associated with the tumor-immune microenvironment. These factors have not been elucidated for chordomas.
Methods
To evaluate the characteristics of vascular and tumor cells in chordoma, we first analyzed the expression of VEGF receptor (VEGFR) 1, VEGFR2, CD34, and Brachyury in a cell line and 54 tumor tissues. Patients with primary skull base chordomas were divided into the following two groups as per the tumor growth rate: patients with slow progression (SP: < 3 mm/year) and those with rapid progression (RP: ≥ 3 mm/year). Thus, the expressions of VEGF-A, VEGFR 1, and VEGFR2 on tumor cells; tumor infiltrative immune cells, including regulatory T cells (Tregs) and tumor-associated macrophages (TAMs); and immune-checkpoint molecules (PD-1/PD-L1) were analyzed with the clinical courses, especially in a comparison between the two groups.
Results
In chordomas, both VEGFR1 and VEGFR2 were strongly expressed not only on vascular endothelial cells, but also on tumor cells. The recurrent cases showed significantly higher VEGFR1 expressions on tumor cells than the primary cases. The expression of VEGF-A was significantly higher in RP than that in SP group. The numbers of CD163+ TAMs and Foxp3+ Tregs were higher in RP than that in SP group.
Conclusions
Expression of VEGFR1 and VEGFR2 on tumor cells and immunosuppressive tumor-microenvironment were related to tumor growth in patients with chordomas.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chordoma is a rare clinically aggressive neoplasm that arises from the embryological remnants of the notochord along the spinal axis [1,2,3]. Although chordomas tend to grow slowly, patients develop severe symptoms such as cranial nerve palsies and brain stem compression, that make successful surgical treatment difficult, and become resistant to radio-chemotherapy. Recently, irradiation with high-energy particles, such as proton beams (Bragg peak), has proven effective for chordomas [3,4,5,6]. Therefore, palliative debulking followed by radiation therapy is the standard treatment. However, patients experience multiple local recurrences, and > 90% of patients die within 10 years [7].
Some studies have suggested clinical prognostic factors for chordomas. Although larger tumor size, non-total resection, older patient age, Ki-67 > 3% were generally used as adverse prognostic factors [8,9,10,11,12], these parameters did not lead to the development of a new treatment strategy. A better understanding of the molecular and genetic basis of chordoma pathogenesis is required to predict the prognosis and develop new targeted therapies.
Vascular endothelial growth factor (VEGF) is a potent activator of angiogenesis that is known to correlate with the progressive course of central nervous tumors [13, 14]. Although limited reliable data are available, some reports have demonstrated that VEGF plays a role in the development and recurrence of chordomas [15, 16]. Therefore, anti-angiogenic therapy, using bevacizumab and sorafinib, has shown efficacy in regulating the growth of chordomas [17, 18].
Tumor-immune microenvironment is also critical for tumor growth [19]. Tumor-associated macrophages (TAMs) and regulatory T cells (Tregs) are major components of immune-suppressive cells [19]. The immune microenvironment is strongly associated with VEGF-A exposure. VEGF-A suppresses antitumor immunity by inhibiting the maturation of dendritic cells and stimulating the proliferation of Tregs [20, 21]. Furthermore, vascular structure is known to be changed following VEGF-A exposure, leading to a leak of the immune-competent cells into the tumor—microenvironment through damaged blood vessels with increased permeability [22]. Recently, some reports have demonstrated that the clinical course of chordomas might be associated with immune-microenvironment [23]. Zou et al. demonstrated that the density of programmed cell death-1 (PD-1)+ tumor infiltrating lymphocytes (TILs), CD4+ TILs, and CD3+ TILs was significantly associated with local recurrence-free survival and overall survival. In addition, the density of Foxp3+ TILs and CD8+ TILs correlated with overall survival [23]. Immunotherapy was regarded as a potential treatment for chordomas [19, 24, 25]. In a phase II clinical trial, adult patients with unresectable localized chordoma who are scheduled to undergo radiation therapy received the yeast-Brachyury vaccine targeting Brachyury, a transcription factor of the T-box family that is typically expressed in notochord and chordoma [26].
In the present study, molecular and histopathological characterizations regarding angiogenic factors, vascular structure, and tumor-immune microenvironment were examined for skull base chordomas. Novel biomarkers strongly associated with poor prognosis were identified that helped achieve an understanding about the clinical course and develop effective treatment strategies.
Materials and methods
This research was approved by the Institutional Review Board at our institutes (Reference number: 20,050,002). Written consent was obtained from all patients.
Study population
In the present study, 27 primary skull base chordomas and 27 recurrent ones (a total of 54 tumors from 42 patients) from December 1999 to March 2018 were analyzed. Twenty-four out of the 54 tumors were paired primary and recurrent tumors obtained from 12 patients. Other 15 primary tumors and 15 recurrent tumors (not paired samples) were also included in the study. Of the 27 recurrent tumors, only three were radiation-naïve, recurrent tumors. All the patients underwent neurosurgical procedures for mass reduction or diagnostic biopsy.
Immunohistochemical analysis
Histopathological analyses were performed on 3-μm sections of formalin-fixed, paraffin-embedded tissue of 54 skull base chordomas (27 primary and 27 recurrent tumors). Histological characteristics were assessed using hematoxylin and eosin (H&E) staining. All the samples were diagnosed by a neuropathologist.
Standard immunohistochemistry was performed. Sections were deparaffinized and rehydrated. The antigen retrieval was performed in citrate buffer (Ki-67, VEGFR1, CD34, Foxp3, CD163, CD3, CD4, and PD-1), or in Tris buffer (pH 9 for VEGF-A, VEGFR2, CD8, and programmed cell death ligand-1 [PD-L1]) using microwave irradiation or autoclave (PD-L1). The sections were blocked for 60 min in 2.5% horse serum (ImmPRESSTM Detection Systems, Vectorlabs). The sections were incubated overnight at 4 °C with anti-Ki-67 antibody (1:200, M7249, DAKO), anti-VEGF-A antibody (1:200, JH121, Merck Millipore), anti-VEGFR1 antibody (1:200, AF321, R&D SYSTEMS), anti-VEGFR2 antibody (1:600, 55B11, Cell Signaling Technology), anti-CD34 antibody (1:100, F1604, Nichirei Biosciences Inc.), anti-Foxp3 antibody (1:100, ab54501, Abcam), anti-CD163 antibody (1:100, ab87099, Abcam), anti-CD3 antibody (1:100, ab5690, Abcam), anti-CD4 antibody (1:200, 1F6, Nichirei Bioscience Inc.), anti-CD8 antibody (1:50, ab17147, Abcam), anti-PD-1 antibody (1:50, NAT105, Abcam), and anti-PD-L1 antibody (1:500, 28-8, Abcam); thereafter, they were incubated with anti-mouse, rabbit, or goat Ig secondary antibody (ImmPRESSTM Detection Systems, Vectorlabs) for 60 min at room temperature. The products were visualized with peroxidase-diaminobenzidine reaction.
The evaluation of immunohistochemistry was assessed as previously described [27,28,29]. The Ki-67 proliferation index was defined as the percentage of cells with positive nuclear Ki-67 immunostaining at high-power fields (HPF: × 20, 0.95 mm2). The positivity of VEGF-A staining in the tumor cytoplasm or stroma was assessed as the following: ++ , diffuse intense staining; + , diffuse faint staining; and − , negative staining. VEGFR1 and VEGFR2 were expressed on vascular endothelial cell and tumor cell. The expressions of VEGFR1 and VEGFR2 in the tumor cells were assessed as percentage of positive tumor cell analyzed from three areas. For the assessment of microvessel density (MVD), the tissue sections were screened in low-power fields (× 4), and the three most vascularized regions (hot spots) were selected for each region. The counting of microvessels was performed on these regions at high-power fields (HPF: × 20, 0.95 mm2). For the assessment of density of Foxp3, CD163, CD3, CD4, CD8, and PD-1 (+) cells, the tissue sections were screened using each immunohistochemistry at the low-power fields (× 4), and three hot spots were selected. The positive cells were counted in these areas at HPF (× 40, 0.47 mm2). The expression of PD-L1 in tumor cells was assessed as percentage of positive tumor cells analyzed from three areas. All the expressions were determined based on the consensus of four authors with blinded clinical information (YM, RT, KK, and KO).
Immunofluorescence analysis
Immunofluorescence triple staining for CD34, VEGFR1, and Brachyury; CD34, VEGFR2 and Brachyury; or VEGFR1, VEGFR2, and PDGFR-β expression was performed for all sections. Tissue sections were incubated with antibodies against CD34 (1:100 or 1:250, NU-4A1 or sc-18917, mouse polyclonal IgG or rat polyclonal IgG, Abcam or Santa Cruz Biotechnology), Brachyury (1:100, H-210, rabbit polyclonal IgG, Santa Cruz Biotechnology), VEGFR1 (1:100, AF321, goat polyclonal IgG, R&D Systems), VEGFR2 (1:100, EIC, mouse monoclonal IgG, Abcam), and PDGFR-β (1:50, Y92, rabbit monoclonal IgG, Abcam) overnight at 4 °C. Appropriate secondary antibodies, Alexa Fluor 488 donkey anti-mouse IgG, Alexa Fluor 488 donkey anti-rat IgG, Alexa Fluor 568 donkey anti-mouse IgG, Alexa Fluor 568 donkey anti-goat IgG, or Alexa Fluor 647 donkey anti-rabbit IgG were used (1:200). Finally, the sections were mounted with mounting medium for fluorescence with 4′,6′-diamidino-2-phenylindole (DAPI; Santa Cruz Biotechnology). Cell images were captured with fluorescence microscopy (Biorevo BZ-9000, KEYENCE).
Cell culture and immunocytochemistry
The human chordoma cell line JHC7 was obtained from the American Type Culture Collection. JHC7 cells were cultured in T-75 cell culture plastic flasks (Thermo Fisher Scientific) with DMEM (Sigma-Aldrich) containing 10% fetal bovine serum (FBS), 2 mM l-glutamine, 100 U/mL penicillin, and 100 μg/mL streptomycin. After four days, the medium was removed, and fresh media was added. When the cells were 90% confluent, the culture medium was removed, and 3 mL of 0.25% trypsin–EDTA solution (Thermo Fisher Scientific,) was added to the flask. The cells were resuspended in 10 mL fresh media before diluting into new culture flasks.
Immunocytochemistry was performed to clearly detect VEGFR1 and VEGFR2 expressions on the tumor cells. Chordoma cell line JHC7 was plated on 12-mm cover slips coated with poly-l-lysine-coated chamber slides. The cultured cells were fixed with 4% PFA and permeabilized with 0.5% Triton-X. The cells were stained with the following primary antibodies against Brachyury (1:100, H-210, rabbit polyclonal IgG, Santa Cruz Biotechnology), VEGFR1 (1:100, AF321, goat polyclonal IgG, R&D Systems), VEGFR2 (1:100, EIC, mouse monoclonal IgG, Abcam) overnight at 4 °C. Appropriate secondary antibodies, Alexa Fluor 488 donkey anti-rabbit IgG, Alexa Fluor 568 donkey anti-goat IgG, or Alexa Fluor 647 donkey anti-mouse IgG were used (1:200). Finally, the sections were mounted with mounting medium for fluorescence with 4′,6′-diamidino-2-phenylindole (DAPI; Santa Cruz Biotechnology, Texas, USA). Cell images were captured using fluorescence microscopy (Biorevo BZ-9000, KEYENCE).
The specificity of all procedures was checked using negative controls. For negative controls, sections and cells were incubated with non-immune mouse, rabbit, rat and goat IgG at the same concentration used for each antibody.
Radiographical analysis
The gadolinium (Gd)-enhanced T1-weighted magnetic resonance imaging (MRI) or T2-weighted image was used to evaluate tumor growth. The T2-weighted image was used to evaluate the tumor size in one patient because the patient exhibited an allergic reaction to Gd. The tumor growth rate for one year was quantitatively analyzed using the longest diameter [16, 23, 30, 31]. The growth rate was evaluated starting three months after the initial surgery because tumor sizes tended to change early after surgery. We deemed a growth ≧ 3 mm/year to indicate a progressive course. Slow progressive course (growth rate < 3 mm/year) was defined as SP and rapid progressive course (growth rate ≥ 3 mm/year) as RP. The use of 3 mm/year as a growth rate criterion was determined from the median growth speed in the present study, because no previous studies determined a quantitative growth rate for chordomas. Progression-free survival (PFS) was defined as the time that elapsed between treatment initiation and tumor progression.
Statistical analysis
Chi-squared test was used to evaluate the immunohistopathological expressions of patient sex, and distribution of VEGF-A. Student’s t-test was used to compare the recurrent rate; Ki-67 index; the number of CD3, CD4, CD8, CD34, CD163, or Foxp3 positive cells; and percentage of VEGFR1, VEGFR2 and PD-L1 positive tumor cell. Prognostic predictors were examined for tumor growth rate using a multiple linear regression analysis. Receiver operating characteristic (ROC) curves for postoperative recurrence were used to determine the cut-off points for VEGFR1 and VEGFR2 expressions on tumor cells. To evaluate the association with PFS, cut-offs greater than 46% for VEGFR1 and greater than 22% for VEGFR2 were used to include the highest true positive rates and the lowest false positive rates. Analyses were performed using IBM SPSS statistics (IBM Corp.). A p-value < 0.05 was considered statistically significant.
Results
Patients characteristics
Table 1 summarizes patients characteristics; 12 patients (male: 7, female: 5) in the SP group and 15 patients (male: 5, female: 10) in the RP group were analyzed. The age range of the study population was 17 to 79 y; the mean age of those in the SP group was 46.17 ± 21.6 y, while that of those in the RP group was 44.27 ± 20.2 y. There was no significant difference in general characteristics of the patients of the two groups. There was no significant difference in the Ki-67 index of the groups (SP: 4.23%, RP: 5.28%, p = 0.29).
VEGFR1 and VEGFR2 expressions on tumor cells
VEGFR1 and VEGFR2 expressions were detected on human chordoma tumor cells (JHC7) expressing Brachyury. Positive membranous staining of VEGFR1 and VEGFR2, with some faint cytoplasmic staining, was detected on tumor cells. VEGFR1 was more strongly stained on the tumor cells than VEGFR2 (Fig. 1a). Similarly, VEGFR1 and VEGFR2 expressions were clearly detected on endothelial cells with CD34 staining as well as tumor cells in human chordoma specimens (Fig. 1b). Vasculatures stained with VEGFR1 and VEGFR2 exhibited slight or negative PDGFR-β expression of a pericyte marker (Fig. 1b).

VEGFR1 and VEGFR2 expressions on tumor and vascular endothelial cells in chordoma. a Immunofluorescence triple staining for Brachyury, VEGFR1, and VEGFR2 on a human chordoma cell line (JHC7) (original magnification, × 20; magnification bar, 100 μm) (NC, negative control). b Immunofluorescence triple staining for CD34, VEGFR1, and Brachyury; CD34, VEGFR2 and Brachyury; or VEGFR1, VEGFR2 and PDGFR-β on vascular endothelial cells and tumor cells in human chordoma tissue specimens (original magnification, × 20; magnification bar, 100 μm) (V, vascular endothelial cells)
The relationship between the percentage of VEGFR1- or VEGFR2-positive tumor cells and tumor growth (mm/year) was evaluated. Patients with a high percentage of VEGFR1- or VEGFR2-positive tumor cells showed higher tumor growth and a linear relationship (VEGFR1, p = 0.00029; VEGFR2, p = 0.0014) (Fig. 2a). PFS of the patients with a higher percentage of VEGFR1- or VEGFR2-positive tumor cells were significantly shorter than that in those with a lower percentage of positive tumor cells (VEGFR1: p = 3.21E-05, VEGFR2: p = 0.037) (Fig. 2b). The percentage of VEGFR1-positive tumor cells in recurrent cases was significantly higher than that in primary cases (33% vs. 53%, p = 0.0053) (Fig. 2c). The percentage of VEGFR2-positive tumor cells in the recurrent cases tended to be higher than that in the primary cases (26% vs. 37%, p = 0.107) (Fig. 2c). These findings were confirmed by comparing the paired initial and recurrent tumors from 12 patients.

Relationship between VEGFR1 or VEGFR2 expression on tumor cells and the clinical course in chordoma patients. a Relationship between the growth rate (mm/year) and percentage of VEGFR1- or VEGFR2-positive tumor cells. b Relationship between progression-free survival (PFS) and percentage of VEGFR1- or VEGFR2-positive tumor cells. Patients with a high percentage of VEGFR1-positive tumor cells ( ≥ 46%) or VEGFR2-positive tumor cells ( ≥ 22%) show significantly shorter PFS. c Percentage of VEGFR1-positive tumor cells in recurrent cases is significantly higher than that in primary cases (33% vs 53%, p = 0.0053). Percentage of VEGFR2-positive tumor cells in recurrent cases tends to be higher than that in primary cases (26% vs 37%, p = 0.107)
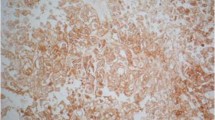
The percentage of VEGFR1-positive tumor cells was significantly higher in the RP group than in the SP group (60.11 vs 22.61%, p < 0.01) (Fig. 3a, b). The percentage of VEGFR2-positive tumor cells was also significantly higher in the RP group than in the SP group (45.45 vs 16.41%, p = 0.0067). Moreover, VEGF-A expression and MVD were also significantly higher in the RP group than in the SP group (VEGF-A: p = 0.03; MVD, 8.78 vs 15.81 /3 HPF: p = 0.013) (Fig. 3a, b).

Analyses of VEGF-A, VEGFR1, and VEGFR2 expressions on tumor cells. a VEGFR1, VEGFR2, and VEGF-A expression on tumor cells and CD34 expression in the SP and RP groups (SP, patient with growth rate < 3 mm/year; RP, patients with growth rate ≥ 3 mm/year, original magnification, × 40; magnification bar, 50 μm). b Percentage of VEGFR1- or VEGFR2-positive tumor cells is significantly higher in the RP group than that in the SP group. VEGF-A expression and MVD are also significantly higher in the RP group than in the SP group
Tumor-infiltrating immune cells
The number of CD3+ T cells was higher in the RP group than in the SP group (10.0 vs 4.97/3 HPF, p = 0.034) (Fig. 4a, c). The number of CD4 +, CD8+ and PD-1+ cells were not significantly difference between the RP and SP groups (CD4, 14.27 vs. 10.43/3HPF: p = 0.28; CD8, 9.96 vs. 12.72/3HPF: p = 0.30; PD-1,4.38 vs. 1.72/3HPF: p = 0.14) (4a–c). The percentage of PD-L1-positive tumor cells was higher in the RP group than in the SP group (38.47 vs 7.67%, p = 0.00064) (Fig. 4b, c). Immunosuppressive cells were also analyzed, and the numbers of Foxp3+ and CD163+ cells was significantly higher in the RP group than in the SP group (Fig. 5a, b).

Analyses of tumor-infiltrating lymphocytes and immune-checkpoint molecules. a Immunohistochemistry of CD3, CD4, CD8, PD-1, and PD-L1 expressions in the SP and RP groups (original magnification, × 40; magnification bar, 50 μm.). b The number of CD3+ T cells is higher in the RP group than in the SP group (10.0 vs 4.97/3 HPF, p = 0.034). No significant difference is present in the number of CD4+ , CD8+ , and PD-1+ cells between the RP and SP groups (CD4, 14.27 vs. 10.43/3HPF: p = 0.28; CD8, 9.96 vs. 12.72/3HPF: p = 0.30; PD-1,4.38 vs. 1.72 /3HPF: p = 0.14). Percentage of PD-L1-positive tumor cells is higher in the RP group than in the SP group (38.47 vs 7.67%, p = 0.00064)

Analyses of immunosuppressive cells and tumor growth. a Immunohistochemistry of Foxp3 and CD163 in the SP and RP groups (original magnification, × 40; magnification bar, 50 μm). b The numbers of Foxp3+ and CD163+ cells are higher in the RP group than that in the SP group
Multiple linear regression analysis revealed significant relationships between the tumor growth rate (mm/year) and VEGFR1, VEGFR2, or CD163 expression (Table 2).
There were no statistically significant differences in any parameters regarding angiogenesis or immune-related markers between the radiation-naïve tumors and the post-radiation tumors.
Discussion
VEGF promotes endothelial cell proliferation, and tumor growth. VEGF expression correlated with the prognosis in central nervous tumors, such as malignant gliomas [32]. For example, VEGF-A is strongly expressed in glioblastomas, with the expression being approximately 10 times higher than that in grade II gliomas [33]. Some reports demonstrated that VEGF plays a role in the development, and recurrence of chordoma through upregulated HIF-1α expression under hypoxia [15, 16, 18, 34]. HIF-1α directly regulates the VEGF expression [35]. In the present study, VEGF-A and MVD were associated with the growth rate of chordomas. Angiogenesis played a key role in chordoma growth, which was consistent with the previous study.
VEGF-VEGFRs signaling plays an important role in the development of notochord, which may be related to high expression of chordoma cells [36, 37]. This study showed that both VEGFR1 and VEGFR2 were co-expressed on tumor cells and vascular endothelial cells. It has been reported that not only VEGFR1, but also VEGFR2 was expressed on tumor cells and vascular endothelial cells in various types of tumors [38,39,40,41,42]. VEGFR1 and VEGFR2 expressions on tumor cells were observed in 25-50% of the patients with lung, breast, cervix, larynx, pancreas, and ovarian cancers, as well as melanoma [39,40,41,42]. Further, the expression of VEGFR1 or VEGFR2 on tumor cells was different in various types of tumors. In chordoma, the percentage of VEGFR1- or VEGFR2-positive tumor cells was higher than that in other malignant tumors, suggesting an autocrine regulatory process in tumor growth [41,42,43,44,45,46]. In particular, VEGFR2 is known to play an important role in tumor stem cells proliferation. Blocking VEGFR2 reduced the size of the tumor stem cell pool and stem cell self-renewal potential [47]. In the present study, VEGFR1 and VEGFR2 expression on tumor cells was strongly associated to chordoma growth.
Furthermore, tumor-immune microenvironment was related to the progression of chordoma in the present study. Tumor-infiltrating immune cells, including Tregs, TAMs, and cytotoxic T lymphocytes, are known to be critical determinants of cancer outcome. VEGF-A promotes the immunosuppressive microenvironment [48]. Thus far, few studies have examined the relationship between chordomas and immune microenvironment [49]. Recently, Zou et al. [23, 31] demonstrated that immune cell infiltrates, such as Tregs, were observed in human chordoma specimens, which was associated with poor prognosis. The numbers of Tregs and TAMs were increased in the RP group compared with the SP group in the present study. The role of TAMs, known as immunoregulatory (M2) macrophages [50], has never examined for chordomas. Polarization of TAMs towards an M1 or M2 phenotype depends on the cytokine milieu and the local microenvironment [51]. Arginase I, interleukin (IL)-10, transforming growth factor (TGF)-β and prostaglandin E2 (PGE2) are produced by TAMs, resulting in the suppression of cytotoxic T cell [51]. Therefore, TAMs promote tumor growth, and correlate to tumor malignancy [51]. VEGF-A promotes the migration and differentiation of TAMs from immature myeloid cell [52], which was consistent with the present results.
Tregs also have been shown to play an important role in the regulation of immune responses via suppression of proliferation of other T cells present in the tumor—microenvironment [53]. Tregs produce immunosuppressive cytokines such as TGF-β, IL-10, and IL-35. Tregs induce the apoptosis of cytotoxic T cells by the action of granzyme B. Consuming IL-2 by Tregs inhibits effector T cell proliferation, resulting in impaired immune response [54]. Upregulation of VEGF-A promotes the recruitment of Tregs to the tumor microenvironment via over-expression of chemokine–chemokine ligand 28 (CCL28) by tumor cells and induces VEGFR-2-expressing Tregs [55]. Zou et al. [31] demonstrated CD8+ /Foxp3+ ratio to be an independent prognostic factor for overall survival of chordomas. This study also suggests that the presence of Tregs provides important prognostic information for chordomas. VEGF-A exposure increased the permeability of blood vessels with upregulated VEGFR1 and VEGFR2 expressions [22, 29, 56]. Immunocompetent cells can easily leak through the damaged vascular structures in the tumor—microenvironment [29, 56]. Permeability of blood vessels in chordoma was suggested to be high because high expressions of VEGF-A, VEGFR1, and VEGFR2 without strict coverage of PDGFR-β expressing pericytes were observed in tumor specimens.
The present results suggest that anti-angiogenic therapy, such as VEGF-targeting drugs (bevacizumab) can be effective for chordoma. In fact, bevacizumab induced durable stabilization for chordoma patients [57]. Furthermore, VEGFRs-targeting drugs (sorafenib, sunitinib and VEGFRs epitope peptide derived vaccine) may be more effective because chordoma cells expressed VEGFR1 and VEGFR2, and CD4+ CD25+ Foxp3+ Tregs that are known to express VEGFR2 [58, 59]. Sorafenib was used for advanced chordoma in phase II trial, leading to prolonged PFS [18]. However, we must pay attention for high PD-L1 expression in the RP group of chordoma. Previous studies have shown that high PD-L1 expression correlated with worse OS in patients with some central nervous tumors [60]. The relationship between PD-L1 expression and prognosis was controversial for chordoma [61]. Zou et al. [62] showed that the expression of PD-L1 is associated with favorable prognosis of spinal chordoma. In the present study, high PD-L1 expression was shown in the RP group of chordomas, which was related to poor prognosis. The expression of PD-L1 is induced by various proinflammatory molecules, such as interferon (IFN)-γ and VEGF-A, in the tumor—microenvironment [63,64,65]. Therefore, combinational therapy using anti-angiogenic therapy and checkpoint inhibitor can be more effective.
The present study evaluated VEGFR1 and VEGFR2 expression on tumor cells and found the expressions to be significantly correlated with an aggressive clinical course of chordomas. The percentage of VEGFR1- and VEGFR2-positive tumor cells might be helpful for predicting prognosis and for developing new targeted therapies. Furthermore, immunosuppressive cells, such as Tregs and TAMs, and immune checkpoint molecules were also associated with tumor growth. These tumor-microenvironments must be comprehensively regulated for the treatment of chordomas.
The prevalence of chordoma was reported as 0.5–0.8 per 1,000,000 [6, 66]. Reports on clival chordoma are more valuable because most examinations are performed using spinal chordomas [6, 66]. Limitation of the present study was the small number of paired primary and recurrent samples from the same patients. Some patients were initially operated at other hospitals, and came to our hospital at the time of recurrence. Ideally, studies using a larger number of paired samples should be conducted to confirm the findings of this study. Furthermore, the biology of chordomas has not been fully elucidated. To improve the patient clinical course, the tumor biology, including bone destruction, needs to be analyzed. For those analysis, in vitro and in vivo analyses using human chordoma cells are indispensable. Further analyses should be conducted using human chordoma cells to evaluate the relationship between VEGFR1 and VEGFR2 expression on tumor cells and the tumor biology, including bone destruction.
Conclusions
VEGFR1 and VEGFR2 that were strongly expressed on chordoma tumor cells. The percentage of VEGFR1- and VEGFR2-positive tumor cells significantly correlated with an aggressive clinical course. In addition, increased numbers of immunosuppressive cells, including that of Tregs and TAMs, and immune checkpoint molecule were also associated with the growth of chordomas.
References
Mundy GR (2002) Metastasis to bone: causes, consequences and therapeutic opportunities. Nat Rev Cancer 2:584–593
Otero JE, Stevens JW, Malandra AE, Fredericks DC, Odgren PR, Buckwalter JA, Morcuende J (2014) Osteoclast inhibition impairs chondrosarcoma growth and bone destruction. J Orthop Res 32:1562–1571
Takahashi S, Kawase T, Yoshida K, Hasegawa A, Mizoe JE (2009) Skull base chordomas: efficacy of surgery followed by carbon ion radiotherapy. Acta Neurochir (Wien) 151:759–769
Hug EB, Loredo LN, Slater JD, DeVries A, Grove RI, Schaefer RA, Rosenberg AE, Slater JM (1999) Proton radiation therapy for chordomas and chondrosarcomas of the skull base. J Neurosurg 91:432–439
Hug EB (2001) Review of skull base chordomas: prognostic factors and long-term results of proton-beam radiotherapy. Neurosurg Focus 10:E11
McMaster ML, Goldstein AM, Bromley CM, Ishibe N, Parry DM (2001) Chordoma: incidence and survival patterns in the United States, 1973–1995. Cancer Causes Control 12:1–11
Sundaresan N, Galicich JH, Chu FC, Huvos AG (1997) Spinal chordomas. J Neurosurg 50:312–319
Bakker SH, Jacobs WCH, Pondaag W, Gelderblom H, Nout RA, Dijkstra PDS, Peul WC, Vleggeert-Lankamp CLA (2018) Chordoma: a systematic review of the epidemiology and clinical prognostic factors predicting progression-free and overall survival. Eur Spine J 27:3043–3058
Bergh P, Kindblom LG, Gunterberg B, Remotti F, Ryd W, Meis-Kindblom JM (2000) Prognostic factors in chordoma of the sacrum and mobile spine: a study of 39 patients. Cancer 88:2122–2134
Leah P, Dower A, Vescovi C, Mulcahy M, Al Khawaja D (2018) Clinical experience of intracranial chordoma: a systematic review and meta-analysis of the literature. J Clin Neurosci 53:6–12
Zhou Y, Hu B, Wu Z, Cheng H, Dai M, Zhang B (2018) Clival chordoma: long-term clinical outcome in a single center. Medicine (Baltimore) 97:e12207
Zou MX, Lv GH, Zhang QS, Wang SF, Li J, Wang XB (2018) Prognostic factors in skull base chordoma: a systematic literature review and meta-analysis. World Neurosurg 109:307–327
Jain RK, di Tomaso E, Duda DG, Loeffler JS, Sorensen AG, Batchelor TT (2007) Angiogenesis in brain tumours. Nat Rev Neurosci 8:610–622
Tamura R, Tanaka T, Miyake K, Yoshida K, Sasaki H (2017) Bevacizumab for malignant gliomas: current indications, mechanisms of action and resistance, and markers of response. Brain Tumor Pathol 34:62–77
Chen KW, Yang HL, Lu J, Wang GL, Ji YM, Wu GZ, Zhu LF, Liu JY, Chen XQ, Gu YP (2011) Expression of vascular endothelial growth factor and matrix metalloproteinase-9 in sacral chordoma. J Neurooncol 101:357–363
Li X, Ji Z, Ma Y, Qiu X, Fan Q, Ma B (2012) Expression of hypoxia-inducible factor-1α, vascular endothelial growth factor and matrix metalloproteinase-2 in sacral chordomas. Oncol Lett 3:1268–1274
Asklund T, Sandström M, Shahidi S, Riklund K, Henriksson R (2014) Durable stabilization of three chordoma cases by bevacizumab and erlotinib. Acta Oncol 53:980–984
Lebellec L, Bertucci F, Tresch-Bruneel E, Bompas E, Toiron Y, Camoin L, Mir O, Laurence V, Clisant S, Decoupigny E, Blay JY, Goncalves A, Penel N (2016) Circulating vascular endothelial growth factor (VEGF) as predictive factor of progression-free survival in patients with advanced chordoma receiving sorafenib: an analysis from a phase II trial of the French sarcoma group (GSF/GETO). Oncotarget 7:73984–73994
Yuan Y, Jiang YC, Sun CK, Chen QM (2016) Role of the tumor microenvironment in tumor progression and the clinical applications (review). Oncol Rep 35:2499–2515
Gabrilovich DI, Chen HL, Girgis KR, Cunningham HT, Meny GM, Nadaf S, Kavanaugh D, Carbone DP (1996) Production of vascular endothelial growth factor by human tumors inhibits the functional maturation of dendritic cells. Nat Med 2:1096–1103
Ohm JE, Gabrilovich DI, Sempowski GD, Kisseleva E, Parman KS, Nadaf S, Carbone DP (2003) VEGF inhibits T-cell development and may contribute to tumor-induced immune suppression. Blood 101:4878–4886
Weis SM, Cheresh DA (2005) Pathophysiological consequences of VEGF-induced vascular permeability. Nature 437:497–504
Zou MX, Lv GH, Wang XB, Huang W, Li J, Jiang Y, She XL (2018) Clinical impact of the immune microenvironment in spinal chordoma: immunoscore as an independent favorable prognostic factor. Neurosurgery 84:E318–E333
Di Maio S, Yip S, Al Zhrani GA, Alotaibi FE, Al Turki A, Kong E, Rostomily RC (2015) Novel targeted therapies in chordoma: an update. Ther Clin Risk Manag 11:873–883
Patel SS, Schwab JH (2016) Immunotherapy as a potential treatment for chordoma: a review. Curr Oncol Rep 18:55
Heery CR, Singh BH, Rauckhorst M, Marté JL, Donahue RN, Grenga I, Rodell TC, Dahut W, Arlen PM, Madan RA, Schlom J, Gulley JL (2015) Phase I trial of a yeast-based therapeutic cancer vaccine (GI-6301) targeting the transcription factor brachyury. Cancer Immunol Res 3:1248–1256
Tamura R, Tanaka T, Miyake K, Tabei Y, Ohara K, Sampetrean O, Kono M, Mizutani K, Yamamoto Y, Murayama Y, Tamiya T, Yoshida K, Sasaki H (2016) Histopathological investigation of glioblastomas resected under bevacizumab treatment. Oncotarget 7:52423–52435
Tamura R, Ohara K, Sasaki H, Morimoto Y, Yoshida K, Toda M (2018) Histopathological vascular investigation of the peritumoral brain zone of glioblastomas. J Neurooncol 136:233–241
Tamura R, Ohara K, Sasaki H, Morimoto Y, Kosugi K, Yoshida K, Toda M (2018) Difference in immunosuppressive cells between peritumoral area and tumor core in glioblastoma. World Neurosurg 120:e601–e610
Stacchiotti S, Tamborini E, Lo Vullo S, Bozzi F, Messina A, Morosi C, Casale A, Crippa F, Conca E, Negri T, Palassini E, Marrari A, Palmerini E, Mariani L, Gronchi A, Pilotti S, Casali PG (2013) Phase II study on lapatinib in advanced EGFR-positive chordoma. Ann Oncol 24:1931–1963
Zou MX, Guo KM, Lv GH, Huang W, Li J, Wang XB, Jiang Y, She XL (2018) Clinicopathologic implications of CD8+ /Foxp3+ ratio and miR-574-3p/PD-L1 axis in spinal chordoma patients. Cancer Immunol Immunother 67:209–224
Chaudhry IH, O'Donovan DG, Brenchley PE, Reid H, Roberts IS (2001) Vascular endothelial growth factor expression correlates with tumour grade and vascularity in gliomas. Histopathology 39:409–415
Schmidt NO, Westphal M, Hagel C, Ergün S, Stavrou D, Rosen EM, Lamszus K (1999) Levels of vascular endothelial growth factor, hepatocyte growth factor/scatter factor and basic fibroblast growth factor in human gliomas and their relation to angiogenesis. Int J Cancer 84:10–18
Tauziéde-Espariat A, Bresson D, Polivka M, Bouazza S, Labrousse F, Aronica E, Pretet JL, Projetti F, Herman P, Salle H, Monnien F, Valmary-Degano S, Laquerrière A, Pocard M, Chaigneau L, Isambert N, Aubriot-Lorton MH, Feuvret L, George B, Froelich S, Adle-Biassette H (2016) Prognostic and therapeutic markers in chordomas: a study of 287 tumors. J Neuropathol Exp Neurol 75:111–120
Lin C, McGough R, Aswad B, Block JA, Terek R (2004) Hypoxia induces HIF-1alpha and VEGF expression in chondrosarcoma cells and chondrocytes. J Orthop Res 22:1175–1181
Liang D, Chang JR, Chin AJ, Smith A, Kelly C, Weinberg ES, Ge R (2001) The role of vascular endothelial growth factor (VEGF) in vasculogenesis, angiogenesis, and hematopoiesis in zebrafish development. Mech Dev 108:29–43
Sumoy L, Keasey JB, Dittman TD, Kimelman D (1997) A role for notochord in axial vascular development revealed by analysis of phenotype and the expression of VEGR-2 in zebrafish flh and ntl mutant embryos. Mech Dev 63:15–27
Goel HL, Mercurio AM (2013) VEGF targets the tumour cell. Nat Rev Cancer 13:871–882
Holzer TR, Fulford AD, Nedderman DM, Umberger TS, Hozak RR, Joshi A, Melemed SA, Benjamin LE, Plowman GD, Schade AE, Ackermann BL, Konrad RJ, Nasir A (2013) Tumor cell expression of vascular endothelial growth factor receptor 2 is an adverse prognostic factor in patients with squamous cell carcinoma of the lung. PLoS ONE 8:e80292
Lalla RV, Boisoneau DS, Spiro JD, Kreutzer DL (2003) Expression of vascular endothelial growth factor receptors on tumor cells in head and neck squamous cell carcinoma. Arch Otolaryngol Head Neck Surg 129:882–888
Masood R, Cai J, Zheng T, Smith DL, Hinton DR, Gill PS (2001) Vascular endothelial growth factor (VEGF) is an autocrine growth factor for VEGF receptor-positive human tumors. Blood 98:1904–1913
Strizzi L, Catalano A, Vianale G, Orecchia S, Casalini A, Tassi G, Puntoni R, Mutti L, Procopio A. (2001) Vascular endothelial growth factor is an autocrine growth factor in human malignant mesothelioma. J Pathol 193:468-475
Jackson MW, Roberts JS, Heckford SE, Ricciardelli C, Stahl J, Choong C, Horsfall DJ, Tilley WD (2002) A potential autocrine role for vascular endothelial growth factor in prostate cancer. Cancer Res 62:854–859
Mentlein R, Forstreuter F, Mehdorn HM, Held-Feindt J (2004) Functional significance of vascular endothelial growth factor receptor expression on human glioma cells. J Neurooncol 67:9–18
Price DJ, Miralem T, Jiang S, Steinberg R, Avraham H (2001) Role of vascular endothelial growth factor in the stimulation of cellular invasion and signaling of breast cancer cells. Cell Growth Differ 12:129–135
Seghezzi G, Patel S, Ren CJ, Gualandris A, Pintucci G, Robbins ES, Shapiro RL, Galloway AC, Rifkin DB, Mignatti P (1998) Fibroblast growth factor-2 (FGF-2) induces vascular endothelial growth factor (VEGF) expression in the endothelial cells of forming capillaries: an autocrine mechanism contributing to angiogenesis. J Cell Biol 141:1659–1673
Hamerlik P, Lathia JD, Rasmussen R, Wu Q, Bartkova J, Lee M, Moudry P, Bartek J Jr, Fischer W, Lukas J, Rich JN, Bartek J (2012) Autocrine VEGF-VEGFR2-Neuropilin-1 signaling promotes glioma stem-like cell viability and tumor growth. J Exp Med 209:507–520
Wang M, Zhao J, Zhang L, Wei F, Lian Y, Wu Y, Gong Z, Zhang S, Zhou J, Cao K, Li X, Xiong W, Li G, Zeng Z, Guo C (2017) Role of tumor microenvironment in tumorigenesis. J Cancer 8:761–773
Hu W, Yu J, Huang Y, Hu F, Zhang X, Wang Y (2018) Lymphocyte-related inflammation and immune-based scores predict prognosis of chordoma patients after radical resection. Transl Oncol 11:444–449
Tamura R, Tanaka T, Yamamoto Y, Akasaki Y, Sasaki H (2018) Dual role of macrophage in tumor immunity. Immunotherapy 10:899–909
Guadagno E, Presta I, Maisano D, Donato A, Pirrone CK, Cardillo G, Corrado SD, Mignogna C, Mancuso T, Donato G, Del Basso De Caro, M, Malara N, (2018) Role of Macrophages in Brain Tumor Growth and Progression. Int J Mol Sci 27:E1005
Quail DF, Joyce JA (2013) Microenvironmental regulation of tumor progression and metastasis. Nat Med 19:1423–1437
Hamilton A, Sibson NR (2013) Role of the systemic immune system in brain metastasis. Mol Cell Neurosci 53:42–51
Vignali DA, Collison LW, Workman CJ (2008) How regulatory T cells work. Nat Rev Immunol 8:523–532
Wada J, Yamasaki A, Nagai S, Yanai K, Fuchino K, Kameda C, Tanaka H, Koga K, Nakashima H, Nakamura M, Tanaka M, Katano M, Morisaki T (2008) Regulatory T-cells are possible effect prediction markers of immunotherapy for cancer patients. Anticancer Res 28:2401–2408
Abbott NJ, Patabendige AA, Dolman DE, Yusof SR, Begley DJ (2010) Structure and function of the blood-brain barrier. Neurobiol Dis 37:13–25
Asklund T, Malmström A, Björ O, Blomquist E, Henriksson R (2013) Considerable improvement in survival for patients aged 60–84 years with high grade malignant gliomas—data from the Swedish Brain Tumour Population-based Registry. Acta Oncol 52:1041–1043
Suzuki H, Onishi H, Wada J, Yamasaki A, Tanaka H, Nakano K, Morisaki T, Katano M (2010) VEGFR2 is selectively expressed by FOXP3high CD4+ Treg. Eur J Immunol 40:197–203
Terme M, Pernot S, Marcheteau E, Sandoval F, Benhamouda N, Colussi O, Dubreuil O, Carpentier AF, Tartour E, Taieb J (2013) VEGFA-VEGFR pathway blockade inhibits tumor-induced regulatory T-cell proliferation in colorectal cancer. Cancer Res 73:539–549
Xue S, Song G, Yu J (2017) The prognostic significance of PD-L1 expression in patients with glioma: A meta-analysis. Sci Rep 7:4231
Mathios D, Ruzevick J, Jackson CM, Xu H, Shah SR, Taube JM, Burger PC, McCarthy EF, Quinones-Hinojosa A, Pardoll DM, Lim M (2015) PD-1, PD-L1, PD-L2 expression in the chordoma microenvironment. J Neurooncol 121:251–259
Zou MX, Peng AB, Lv GH, Wang XB, Li J, She XL, Jiang Y (2016) Expression of programmed death-1 ligand (PD-L1) in tumor-infiltrating lymphocytes is associated with favorable spinal chordoma prognosis. Am J Transl Res 8:3274–3287
He J, Hu Y, Hu M, Li B (2015) Development of PD-1/PD-L1 Pathway in Tumor Immune Microenvironment and Treatment for Non-Small Cell Lung Cancer. Sci Rep 5:13110
Voron T, Colussi O, Marcheteau E, Pernot S, Nizard M, Pointet AL, Latreche S, Bergaya S, Benhamouda N, Tanchot C, Stockmann C, Combe P, Berger A, Zinzindohoue F, Yagita H, Tartour E, Taieb J, Terme M (2015) VEGF-A modulates expression of inhibitory checkpoints on CD8+ T cells in tumors. J Exp Med 212:139–148
Xue S, Hu M, Li P, Ma J, Xie L, Teng F, Zhu Y, Fan B, Mu D, Yu J (2017) Relationship between expression of PD-L1 and tumor angiogenesis, proliferation, and invasion in glioma. Oncotarget 8:49702–49712
Eriksson B, Gunterberg B, Kindblom LG: Chordoma, (1981) A clinicopathologic and prognostic study of a Swedish national series. Acta Orthop Scand 52:49–58
Acknowledgements
The authors greatly thank Ms. Naoko Tsuzaki in the department of Neurosurgery for technical assistance of laboratory works.
Funding
This work was supported in part by grants from the Japan Society for the Promotion of Science (JSPS) (17H04306 to M.T.).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare nothing to disclose.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Morimoto, Y., Tamura, R., Ohara, K. et al. Prognostic significance of VEGF receptors expression on the tumor cells in skull base chordoma. J Neurooncol 144, 65–77 (2019). https://doi.org/10.1007/s11060-019-03221-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-019-03221-z