
Abstract
Purpose
Elongation of telomeres is necessary for tumor cell immortalization and senescence escape; neoplastic cells use to alternative pathways to elongate telomeres: telomerase reactivation or a telomerase-independent mechanism termed alternative lengthening of telomeres (ALT). Telomerase and ALT pathway has been explored in adult and pediatric gliomas and medulloblastomas (MDBs); however, these mechanisms were not previously investigated in MDBs metastatic at the onset. Therefore, we analyzed the activation of telomerase and ALT pathway in a homogenous cohort of 43 pediatric metastatic medulloblastomas, to investigate whether telomere elongation could play a role in the biology of metastatic MDB.
Methods
We evaluated telomeres length via telomere-specific fluorescence in situ hybridization (Telo-FISH); we assessed nuclear expression of ATRX by immunohistochemistry (IHC). H3F3A and TERT promoter mutations were analyzed by pyrosequencing, while UTSS methylation status was analyzed via methylation-specific-PCR (MS-PCR).
Results
H3F3A mutations were absent in all MDBs, 30% of samples showed ATRX nuclear loss, 18.2% of cases were characterized by TERT promoter mutations, while 60.9% harboured TERT promoter hyper-methylation in the UTSS region. Elongation of telomeres was found in 42.8% of cases. Metastatic MDBs control telomere elongation via telomerase activation (10.7%), induced by TERT promoter mutations in association with UTSS hyper-methylation, and ALT mechanism (32.1%), triggered by ATRX inactivation. Among non-metastatic MDBs, only 5.9% (1/17) showed ATRX nuclear loss with activation of ALT.
Conclusions
Our metastatic cases frequently activate ALT pathway, suggesting that it is a common process for senescence escape in primary metastatic medulloblastomas. Furthermore, the activation of mechanisms for telomere elongation is not restricted to certain molecular subgroups in this high-risk group of MDBs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Telomeres preserve chromosome integrity by preventing loss of genetic information occurring as the consequence of lagging-strand shortening during DNA replication [1, 2]. At each cell division, telomeric DNA diminishes and telomeres progressively shorten; cells unable to maintain their telomeres undergo senescence. A key hallmark of cancer is unlimited replication and immortalization, which depend on escaping from replicative senescence induced by telomere shortening.
Most cancers overcome this critical barrier by up-regulating the enzyme telomerase, a telomere-specific reverse transcriptase, which elongates telomeres. However, in a subset of cancers that lack telomerase activity, telomeres are maintained by employing a non-telomerase-dependent mechanism, the alternative lengthening of telomeres (ALT) pathway, dependent on homologous recombination [3,4,5,6,7].
Approximately 90% of tumours maintain telomere length by up-regulating telomerase; activating mutations in the promoter of the human telomerase reverse transcriptase catalytic subunit (hTERT) were found in several tumours [4, 6,7,8,9,10,11], related to telomerase up-regulation [4, 6, 12, 13]. Furthermore, a previous study regarding TERT promoter methylation identified a subset of 5 CpG sites called UTSS (upstream of the transcription start site) region whose hyper-methylation increased TERT expression [14, 15]. With respect to Central Nervous System (CNS) tumours, adult gliomas show the highest frequency of TERT promoter mutations (30–50%), while these mutations are rare in pediatric gliomas (5–10%) [6, 16, 17, 18]. TERT promoter mutations were found also in ≈ 20% of medulloblastomas, associated with higher age at diagnosis and SHH molecular subgroup [3, 7].
Tumours which do not activate telomerase trigger the ALT phenotype for telomere length maintenance [7, 8, 19, 20]. ALT occurs by homologous recombination, although the mechanisms of ALT are still not well-known, previous studies revealed that somatic mutations in the genes encoding for the α-thalassemia/mental retardation syndrome X-linked proteins (ATRX), the death domain-associated protein (DAXX) chromatin remodelling complex and H3.3 histone, appear to be highly related to ALT-positive tumours [4, 21,22,23,24]. Mutations of ATRX/H3F3A have been frequently reported in pediatric gliomas, correlated with ALT activation (22–44%) [4, 12, 21,22,23,24,25,26]. Conversely, ALT was rarely observed in MDBs (2–5%) [7, 12], restricted to SHH and Group 3 subgroups [3, 7, 27].
Alternative Lenghtening of Telomere, defined by large very bright intranuclear foci of telomere FISH signal, was strongly related to loss of nuclear ATRX expression [22]. Alterations in ATRX has been considered to represent a “nearly perfect surrogate for the ALT phenotype” [16]. Telomere elongation via telomerase reactivation was defined by high telomere fluorescence intensity in presence of TERT promoter mutation and UTSS hypermethylation [14].
Medulloblastomas are heterogeneous tumours comprising four main molecular subgroups (WNT, SHH-TP53-wt, SHH-TP53 mutated, Non-WNT/Non SHH), associated with different clinical outcomes [28,29,30,31,32,33,34], and, more recently, each of them has been shown to comprise different genetic subtypes [27, 35]. Approximately 30% of pediatric MDBs occur with overtly clinical metastasis at the onset [36]; such metastatic presentation identifies the patients as high-risk and it occurs in all molecular variants [29, 31, 32, 37,38,39].
Telomerase/ALT pathway and their clinical utility has been explored in adult and pediatric gliomas [4, 23,24,25,26]. Few studies have investigated such alterations in medulloblastomas [3, 7, 27], however, none of these focused-on tumours with metastatic dissemination at the onset. Here we analyzed the activation of mechanisms involved in control of telomere lengthening in a homogenous cohort of pediatric MDBs with metastasis at the onset, with the aim of defining whether telomere elongation could play a role in metastatic behaviour of medulloblastoma.
Materials and methods
Study cohort—pediatric metastatic and non-metastatic medulloblastomas
Formalin-fixed paraffin embedded (FFPE) tissue specimens from 43 primary metastatic pediatric medulloblastomas were analyzed; all analyses were performed on samples from the initial operation of the primary site in the posterior fossa. Informed consent was obtained from all participants or parents included in the study. All tumors were classified by two independent neuropathologists according to the World Health Organization (WHO) classification of central nervous system tumors [32, 40], using standard histological and immunohistochemical methods. Metastatic MDBs (M1-M4 according to Chang staging system) included in this study were treated with the Milano HART protocol [41] and were recruited from 1998 to 2014 at INT Pediatric Oncology Unit Milano; the cohort included 32 classic MDBs (74%), nine with large cell/anaplastic (21%) and two with desmoplastic/nodular histology (5%). Age at diagnosis ranged from 3.2 to 21 years with a median age of 10.3 years and an average follow-up of 155 months. The female/male ratio was 4:39 (see Table 2 in Supplementary material for details).
Based on previously performed methylation profile analysis and molecular subgrouping according to WHO genetic classification [29, 30, 32, 40] there were five WNT (11.6%), seven SHH TP53 wt and two SHH TP53-mutated, (21%), 15 non-WNT/non-SHH (Group 3 and 4) (34.8%) and 14 (32.6%) not classifiable (NC) medulloblastomas.
We further analyzed 17 pediatric non-metastatic medulloblastomas (10M/7F), with a median age of 10.1 years, classified as above. This series included 11 classic MDBs (64.7%), four large cell/anaplastic (23.5%) and two desmoplastic/nodular histology (11.8%). Two cases were classified as WNT activated MB (11.8%), three in SHH TP53 wt (17.6%), eight in non-WNT/non-SHH (Group 3/ 4) (47%) and four (23.5%) were not classifiable (NC) (see supplementary Table 3). FFPE samples were analyzed via IHC for nuclear ATRX loss and Telo-FISH for telomeres length measurement.
Immunohistochemistry for evaluation of ATRX nuclear expression
Protein expression was evaluated via immunohistochemistry (IHC). This was carried out by streptavidin–biotin–immunoperoxidase technique on 3-µm sections of FFPE samples. Primary antibody incubation was performed with anti-ATRX antibodies (NBP1-83077 Novus Biologicals, rabbit polyclonal, 1:1000 dilution) overnight. Protein expression was quantified by counting stained tumor cell nuclei of 1000 cells in tumor regions considered as the most immunoreactive to determine the labelling index (LI) (% positive nuclear reactivity). Cases with ≤ 15% immunopositive tumor nuclei were considered suggestive to harbour an ATRX inactivating mutations, since loss of nuclear ATRX expression was published to be caused by mutation scattered at multiple positions in the ATRX coding sequence [16, 26]. Endothelial cells served as internal positive control.
PCR and pyrosequencing analysis for H3.3 and TERT promoter hotspot mutations
DNA from FFPE tumours was purified using the QIAamp DNA Mini Tissue Kit (Qiagen, Düsseldorf, Germany) according to the manufacturer’s instructions. All samples selected for DNA extraction contained at least 70% of tumor. Primers were designed to amplify the TERT promoter region containing the C228T and C250T hotspots, corresponding to positions 124 and 146 bp upstream of the ATG site. For H3F3A mutational analysis, primers were designed to amplify the hotspot codons in exon 2, corresponding to amino acids K27 and G34.
For pyrosequencing analysis, single-stranded DNA templates were immobilized on streptavidin-coated Sepharose high-performance beads (GE Health care, Uppsala, Sweden) using the PSQ Vacuum Prep Tool and Vacuum Prep Worktable (Biotage, Uppsala, Sweden), according to manufacturer’s instructions. Pyrosequencing was performed using PyroGold Reagents (Biotage) on the PyroMark Q24 instrument (Biotage), according to manufacturer’s instructions. Negative controls, in which the sequencing primer or template were omitted, were used to detect background signal. Pyrograms were analyzed by using the Pyro Mark Q24 software (Biotage), using the allele quantification (AQ) software to determine the percentage of mutant versus wild-type alleles according to percentage relative peak height as previously described [9, 25]. All primers and PCR conditions are described in Supplementary Materials (Supplementary Table 1).
Methylation-specific PCR (MS-PCR) for TERT promoter methylation status
A quasi-quantitative methylation specific polymerase chain reaction was used to determine methylation status in a subset of five CpG sites localized − 600 bp upstream of the transcription start site (UTSS region) of TERT. Genomic DNA samples were prepared using the QIAamp DNA Mini Tissue Kit (Qiagen) according to the manufacturer’s instructions. Bisulfite modification of DNA for methylation analysis was conducted using the EZ DNA Methylation Kit from ZYMO Research (Irvine, CA), according to the manufacturer’s instructions.
The five CpG sites were targeted using specific primers to amplify bisulfite-modified DNA. Two pairs of primers were used, each pair comprised of a forward and a reverse primer specific for unmethylated and methylated alleles (Supplementary Table 1). For quasi-quantitative MS-PCR we first serially diluted tumor bisulfite-DNA samples; finally, we used 100 ng of bisulfite-DNA for PCR amplification (detailed PCR and cycling conditions are available upon request). In each reaction, we used normal brain tissue as negative control and two positive controls: one genomic DNA fully methylated and one completely un-methylated, supplied by Chemicon. The PCR products were visualized on agarose gel using transilluminator and imaging system (Hartland, WI, USA), and the acquired images were digitalized using ImageJ Software (NIH, Bethesda MD, USA). We used the primarily generated digitalized data for the comparative analysis between methylated and un-methylated alleles. The Mean Intensity of the amplification bands (in pixels) was measured using ImageJ; the intensity of the bands for methylated DNA were compared to intensity for un-methylated DNA for each sample to assign a specific Methylation Value (MV). UTSS region was considered hyper-methylated when the MV was ≥ 30% compared to the un-methylated DNA for each analyzed sample.
Telomere-specific fluorescence in situ hybridization and analysis
The elongation of telomeres was investigated on consecutive sections via telomere-specific fluorescence in situ hybridization (Telo-FISH), by analyzing telomere length with FITC-PNA (Peptide Nucleic Acid) probes (K532511, Dako), complementary to the telomeric repeated sequences. The PNA probes do not recognize sub-telomeric sequences, allowing an exact measurement of the telomere length. Endothelial cell nuclei were used as normal internal control.
Five µm sections were cut from FFPE tissues for Telo-FISH technique and analyzed according to the manufacturer’s instructions (Dako). FISH sections were examined with an AxioImager M1 microscope (Carl Zeiss, Jena, Germany) by two investigators. Signals were counted for 200 tumor cells; as described in literature [22, 23], telomerase/ALT-positive cases were identified when ≥ 10% of tumor cells display large, very bright intranuclear foci of telomere FISH signals.
Deconvolved images were converted into TIFF files and exported for telomere specific image analysis using the TFL-Telo V2 software (BC Cancer Res. Centre, Vancouver, Canada) [42]. TFL-Telo is a quantitative program that measure telomeres intensity (in pixels) within the nuclear space. Telomeres analysis using TFL-Telo determined the numbers of telomeres, the signal intensities and the distribution for each image. Quantitative telomeres analysis was performed on ≥ 100 nuclei for patient (see supplementary Fig. 7 for details). The mean intensity of telomeres, considered to be proportional to the total length of telomeres, was measured for each case. We analyzed positive and negative controls for elongation of telomeres to establish a threshold (Fluorescence Mean Intensity ≈ 1000), used to identify different telomeric profiles in our cases (shown in Fig. 3).
TFL-Telo indicated the presence of two telomeric profiles, displaying significant differences in telomere length (p < 0.0001) and number of telomeric aggregates between positive controls (pediatric high-grade gliomas previously analyzed with telomerase/ALT activation) and negative controls (non-neoplastic brain tissues or telomerase/ALT negative brain tumours).
Statistical analysis
The association between categorical variables and survival of patients was tested using Kaplan–Meier method. Overall survival (OS) was determined from the date of diagnosis to the date of death or last follow-up visit before death; progression-free survival (PFS) was the interval from the date of starting chemotherapy to the date of progression or death, whichever occurred first, with censoring at the latest follow-up visit for alive and progression-free patients. The log-rank test was used to compare survival according to the prognostic factors.
Results
We screened a cohort of 43 primary metastatic pediatric MDBs, in order to define activating mechanisms that control telomere elongation in this aggressive presentation of the most common malignant pediatric brain tumor.
H3F3A (Fig. 1a) and TERT promoter (Fig. 1b) mutations were analyzed by pyrosequencing. Since the presence of inactivating mutations of the ATRX gene results in loss of nuclear expression, we evaluated its nuclear staining by IHC (Fig. 1c); UTSS methylation status was analyzed by methylation-specific-PCR (Fig. 1d).

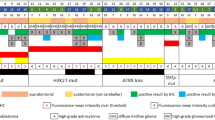
H3F3A and TERT promoter mutations, ATRX nuclear loss and UTSS methylation. a Selected wild-type sample without H3F3A mutation. b Selected wild-type sample without TERT mutation, a case with TERT C228T mutation and a case with TERT C250T mutation (arrows indicate proportional variations in the height of the peaks indicating the presence of a specific point mutation). c Selected samples with 100% nuclear positivity (left) and with > 60% nuclear negativity (right) for ATRX IHC, arrows indicate endothelial cells as internal positive control. d Selected samples with hyper-methylated and un-methylated UTSS region, positive and negative controls were included
ATRX nuclear loss was observed in 30% (9/30) of metastatic medulloblastomas, while none of the analyzed cases showed a H3F3A mutation (0/20, 0%). TERT promoter mutations were found in 18.2% (6/33) of MDBs: five cases with TERT C250T and one with TERT C228T mutation. Study of TERT promoter methylation status in UTSS region showed that 60.9% (25/41) of medulloblastomas were characterized by hypermethylation (Table 1).
These findings underlined that ATRX and TERT alterations were mutually exclusive, except for one medulloblastoma analyzed, and that hypermethylation in UTSS region was very frequent. Interestingly, alterations involved in the activation of mechanisms for telomere elongation were found to be present in all molecular subgroups, with lower frequency in non-WNT/non-SHH MDBs of the Group 4 variant (Table 1).
Presence of TERT mutations was not associated with older age at diagnosis in our metastatic MDB cohort (median = 10.03 WT vs. 12.87 mut; p = 0.17, t test assuming un-equal variances) (see results in Supplementary Fig. 1).
Telomere elongation is frequently detected in metastatic medulloblastomas
Twenty-eight metastatic MDBs with available material were tested via Telo-FISH to evaluate the elongation of telomeres (Fig. 2).

Telo-FISH analysis of telomere length in metastatic MDBs. Image shows a representative case with elongation of telomeres in > 20% of neoplastic nuclei (a), compared to a case with basal level of telomeres in 100% of cells (b) (magnification × 100). Green signals represent telomeres; insert a shows neoplastic nucleus with large and very bright telomere FISH signals, indicative of the activation of telomere elongation; insert b shows neoplastic nucleus with basal level of telomeres characterized by small and homogeneous telomere foci
Elongation of telomeres was found in 42.8% (12/28) of cases and it was present in all molecular subgroups (Table 1), suggesting that the activation of these mechanisms is not restricted to certain molecular variants of metastatic medulloblastomas.
All clinical, genetic and molecular features, histological characteristics, and telomere lengthening results were shown in Supplementary Materials (Supplementary Table 2).
Correlation of variables with overall survival (OS) and progression free survival (PFS) was not statistically significant due to the limited number of cases (see Supplementary material for details).
ALT/telomerase activation
Telomere length association with ATRX, H3F3A and TERT promoter alterations showed that cases with ATRX nuclear loss were always associated with telomere elongation (9/9, 100%), with a significant increase in fluorescence signals (compared to normal tissue and negative controls) indicative of ALT activation. The differences in fluorescence intensity of telomeres between medulloblastomas with ATRX alterations compared to wild-type cases were statistically significant (p value = 0.0019) (Fig. 3).

Telomere length related to the status of ATRX and TERT promoter. Figure shows the TFL-Telo quantification of telomeres fluorescence intensity in cases characterized by ATRX nuclear loss, TERT promoter mutations and/or UTSS hypermethylation, and double wildtype; positive and negative controls were included. The dotted black line represents the telomere elongation threshold
Medulloblastomas with TERT promoter mutations were frequently associated with increase of telomere length (4/5, 80%) in association with UTSS hypermethylation, which was not sufficient by itself to activate elongation of telomeres (data not shown).
Samples with ATRX/H3F3A/TERT wild-type did not show telomere elongation (0/16, 0%); all these wild-type cases showed a significantly reduced fluorescence signals and the mean intensities of telomeres were comparable to those of the negative controls.
Cases with ALT or telomerase activation showed the same level of fluorescence intensity of telomeres measured via TFL-Telo, highlighting that Telo-FISH is useful to identify telomere elongation.
Cases with ALT activation (n = 9) and negative cases (n = 16) showed worse OS compared to medulloblastomas with telomerase activation (n = 3), with an overall survival of 66.6% and 68.7% respectively compared to 100%. These data were not statistically significant (p = 0.55 for OS and p = 0.54 for PFS) (Supplementary Fig. 6).
Furthermore, we analyzed 17 non-metastatic medulloblastomas, in order to evidence cases with ALT activation. Interestingly, only one of 17 cases (5.9%) showed loss of nuclear ATRX with activation of ALT analyzed by Telo-FISH; this case was classified as Group 3 MDB and showed a classic histology. All the other cases (16/17; 94.1%) did not show evidence for ATRX loss and/or ALT (Supplementary Table 3). These data confirmed published data of a frequency of approximately 5% [3, 7, 27].
Discussion and conclusion
Telomere elongation is necessary for tumor cell immortalization and senescence escape. In neoplastic cells, this is achieved through two alternative mechanisms: the reactivation of telomerase via TERT promoter mutations, or a telomerase-independent mechanism called ALT, dependent on homologous recombination [3,4,5,6,7]. We analyzed the activation of mechanisms involved in control of telomere lengthening, in order to investigate the role of telomere elongation in metastatic behaviour of MDBs.
To this end we screened a homogeneous cohort of pediatric metastatic MDBs, evaluating telomere length increase, ATRX nuclear loss, H3F3A and TERT promoter mutations and methylation status at UTSS.
Our results show that elongation of telomeres is frequently activated in primary metastatic medulloblastomas (42.8%), Telo-FISH is useful to identify telomere elongation, however it is not sufficient by itself to evidence the activation of one of the two specific pathways of elongation, with this respect our results show a prevalence of ALT mechanism (32.1%) compared to telomerase up-regulation (10.7%) in metastatic MDBs.
Most cancers up-regulate the enzyme telomerase to elongate telomeres. In particular, hotspot activating mutations of the TERT promoter (C228T and C250T) lead to enhanced expression of telomerase, being responsible for telomere length maintenance [4, 12, 38,39,46]; these mutations were found in several tumours, including pediatric brain tumours [4, 6, 7, 9]. TERT promoter mutations were detected in approximately 20% of medulloblastomas, with higher frequency in SHH methylation subgroup [3, 27]. Our results, in line with previous studies, show that metastatic medulloblastomas harbour these alterations (18.2%); differently from previous reports, we provide evidence that all molecular subgroups, unless Group 4, harbour TERT promoter mutations suggesting that telomerase up-regulation is not restricted to SHH variant in this high-risk group of patients.
Furthermore, a previous study on TERT promoter DNA methylation identified a specific region, named as UTSS, that was hypermethylated in high-grade brain tumours, increasing TERT expression [14]; UTSS hyper-methylation was also associated with tumour progression and poor prognosis [14]. Our results show that hypermethylation in UTSS region is very frequent in metastatic MDBs (60.9%), and trend (p = 0.1) towards association with a worse outcome, supporting the concept that such molecular alteration is associated with more aggressive behaviour of tumours. Moreover, our findings suggest that UTSS hypermethylation is not sufficient by itself to activate elongation of telomeres in MDBs; however, TERT promoter mutations correlate with increase of telomere length only in association with UTSS hypermethylation. Interestingly, TERT promoter mutations and hypermethylation seem to act synergistically, increasing telomere length via telomerase up-regulation.
A subset of tumours, which do not up-regulate telomerase, can activate the ALT mechanism to elongate telomeres. ALT pathway is frequently activated by mutations on H3F3A and/or ATRX genes, previously reported in pediatric brain tumours and correlated with increase of telomere length [23,24,25,26, 43].
H3F3A mutations were absent in our series, suggesting that telomere elongation via ALT pathway can be selectively activated by ATRX alterations in MDBs. In fact, ALT activation and telomere elongation are strongly correlated with ATRX nuclear loss in our metastatic medulloblastomas, as previously reported for gliomas [4, 21, 22, 25].
Previous studies revealed that ALT was highly activated in pediatric high-grade gliomas (22–44%), but rarely found in medulloblastomas (2–5%) [7, 12, 27]. Interestingly, we show that metastatic medulloblastomas activate ALT pathway with higher incidence (32.1%) compared to our series of non-metastatic MDBs (1/17; 5.9%) and previously analyzed series in literature (≈ 5%) [3, 7, 27], highlighting the differences between metastatic and non-metastatic tumors in control of telomere elongation, and suggesting that ALT mechanism is a common process to escape from senescence in metastatic MDBs. Differently from previous studies [3, 7, 27] where ALT/telomerase activation was restricted to SHH and Group 3 MDBs, we provide evidence that these mechanisms can be activated in all molecular subgroups.
Metastatic MDBs with ALT activation showed worse OS, even if not statistically significant, compared to cases with telomerase activation. Interestingly, in line with our findings, recent data in literature showed an association between ALT and worse OS in a subset of pediatric malignant gliomas [47].
Inhibitors against mechanisms of telomere maintenance are in development for pediatric brain tumors; current therapies include telomerase inhibitors for gliomas with TERT promoter mutation and ATRX inhibitors for gliomas with ALT [48]. Our findings might contribute to the development of new therapeutic strategies using these specific targeted treatments for a subset of metastatic tumors with telomerase/ALT activation; however, further validation on a larger prospective cohort will be necessary to clarify the role of ALT/telomerase activation on pediatric metastatic MDB outcome.
In conclusion, we show that elongation of telomeres is frequently activated in metastatic medulloblastomas (42.8%), which could control elongation of telomeres both via telomerase up-regulation (10.7%), induced by TERT promoter mutations in combination with UTSS hypermethylation, and ALT mechanism (32.1%), triggered by ATRX inactivation but not by H3F3A mutations.
In all analyzed cases, except one in which ATRX and TERT alterations coexist, ALT and telomerase activation are mutually exclusive. Furthermore, the activation of mechanisms for telomere elongation is not restricted to certain molecular subgroups of metastatic medulloblastomas.
Due to the low incidence of primary metastatic medulloblastoma, our study has the intrinsic limit of the small size of our cohort: extending the enrollment period would improve the statistical significance of our results.
Understanding of molecular mechanisms to activate elongation of telomeres in metastatic MDBs can improve knowledge about tumour cells escape from senescence and may contribute to the risk stratification of patients and development of new targeted treatments [48] for a subset of these tumours.
References
Oganasian L, Karlseder J (2009) Telomeric armor: the layers of end protection. J Cell Sci 122:4013–4025. https://doi.org/10.1242/jcs.050567
Rubtsova MP, Vasilkova DP, Malyavko AN, Naraikina YV, Zvereva MI, Dontsova OA (2012) Telomere lengthening and other functions of telomerase. Acta Nat 4(2):44–61
Remke M, Ramaswamy V, Peackock J, Shih DJH, Koelsche C, Northcott PA, Hill N, Cavalli FMG, Kool M, Wang X, Mack SC, Barszczyk M, Morissi AS, Wu X, Agnihotri S, Luu B et al (2013) TERT promoter mutations are highly recurrent in SHH subgroup medulloblastoma. Acta Neuropathol 126:917–929. https://doi.org/10.1007/s00401-013-1198-2
Ceccarelli M, Barthel FP, Malta TM, Sabedot TS, Salama SR, Murray BA, Morozova O, Newton Y, Radenbaugh A, Pagnotta SM, Anjum S, Wang J, Manyam G, Zoppoli P, Ling S, Rao AA et al (2016) Molecular profiling reveals biologically discrete subsets and pathways of progression in diffuse glioma. Cell 164:550–563. https://doi.org/10.1016/j.cell.2015.12.028
Cesare AJ, Reddel RR (2010) Alternative lengthening of telomeres: models, mechanisms and implications. Nat Rev Genet 11:319–330. https://doi.org/10.1038/nrg2763
Koelsche C, Sahm F, Capper D, Reuss D, Sturm D, Jones DTW, Kool M, Northcott PA, Wiestler B, Bohmer K, Meyer J, Marwin C, Hartmann C, Mittelbronn M, Platten M, Brokinkel B et al (2013) Distribution of TERT promoter mutations in pediatric and adult tumors of the nervous system. Acta Neuropathol 126:907–914. https://doi.org/10.1007/s00401-013-1195-5. doi
Mangerel J, Price A, Castelo-Branco P, Brzezinski J, Buczkowicz P, Rakopoulos P, Merino D, Baskin B, Wasserman J, Mistry M, Barszczyk M, Picard D, Mack S, Remke M, Starkman H et al (2014) Alternative lengthening of telomeres is enriched in, and impacts survival of TP53 mutant pediatric malignant brain tumors. Acta Neuropathol 128:853–862. https://doi.org/10.1007/s00401-014-1348-1
Bechter OE, Zou Y, Shay JW, Wright WE (2003) Homologous recombination in human telomerase-positive and ALT cells occurs with the same frequency. EMBO Rep 4:1138–1143. https://doi.org/10.1038/sj.embor.7400027
Gessi M, Van De Nes J, Griewank K, Barresi V, Buckland ME, Kirfel J, Caltabiano R, Hammes J, Lauriola L, Pietsch T, Waha A (2014) Absence of TERT promoter mutations in primary melanocytic tumors of the central nervous system. Neuropathol Appl Neurobiol 40(6):794–797. https://doi.org/10.1111/nan.12138
Horn S, Figl A, Rachakonda PS, Fischer C, Sucker A, Gast A, Kadel S, Moll I, Nagore E, Hemminki K, Schadendorf D, Kumar R (2013) TERT promoter mutations in familial and sporadic melanoma. Science 339:959–961. https://doi.org/10.1126/science.1230062
Kim J-H, Huse JT, Huang Y, Lyden D, Greenfield JP (2013) Molecular diagnostics in paediatric glial tumours. Lancet Oncol 14:19. https://doi.org/10.1016/S1470-2045(12)70577-6. doi
Dorris K, Sobo M, Onar-Thomas A, Panditharatna E, Stevenson CB, Gardner SL, DeWire MD, Pierson CR, Olshefski R, Rempel SA, Goldman S, Miles L. Fouladi M, Drissi R (2014) Prognostic significance of telomere maintenance mechanisms in pediatric high-grade gliomas. J Neurooncol 117(1):67–76. https://doi.org/10.1007/s11060-014-1374-9
Huang DS, Wang Z, He XJ, Diplas BH, Yang R, Killela PJ, Liang J, Meng Q, Ye ZY, Wang W, Jiang XT, Hu L, He XL, Zhao ZS, Xu WJ, Wang HJ, Ma YY, Xia YJ, Li L, Zhang RX, Jin T et al (2015) Recurrent TERT promoter mutations identified in a large-scale study of multiple tumor types are associated with increased TERT expression and telomerase activation. Eur J Cancer 51(8):969–976. https://doi.org/10.1016/j.ejca.2015.03.010
Castelo-Branco P, Sanaa C, Mack S, Gallagher D, Zhang C, Lipman T, Zhukova N, Walker EJ, Martin D, Merino D, Wasserman JD, Elizabeth C, Alon N, Zhang L, Hovestadt V, Kool M et al (2013) Methylation of the TERT promoter and risk stratification of childhood brain tumours: an integrative genomic and molecular study. Lancet Oncol 14:534–542. https://doi.org/10.1016/S1470-2045(13)70110-4
Noushmehr H, Weisenberger DJ, Diefes K, Phillips HS, Pujara K, Bergman BP, Pan F, Pelloskj CE, Sulman EP, Bhat KP, Verhaan RG, Hoadley KA, Hayes DN, Perou CM, Schmidt HK et al (2010) Identification of a CpG island methylator phenotype that defines a distinct subgroup of glioma. Cancer Cell 17(5):510–522. https://doi.org/10.1016/j.ccr.2010.03.017
Killela PJ, Reitman ZJ, Jiao Y, Bettegowda C, Agrawal N, Diaz LA Jr, Friedman AH, Friedman H, Gallia GL, Giovanella BC, Grollman AP, He TC, He Y, Hruban RH, Jallo GI, Mandahl N, Meeker AK et al (2013) TERT promoter mutations occur frequently in gliomas and a subset of tumors derived from cells with low rates of self-renewal. Proc Natl Acad Sci USA 110:6021–6026. https://doi.org/10.1073/pnas.1303607110
Nonoguchi N, Ohta T, Oh JE, Kim YH, Kleihues P, Ohgaki H (2013) TERT promoter mutations in primary and secondary glioblastomas. Acta Neuropathol 126:931–937. https://doi.org/10.1007/s00401-013-1163-0
Reifenberger G, Weber RG, Riehmer V, Kaulich K, Willscher E, Wirth H, Gietzelt J, Hentschel B, Westphal M, Simon M, Schackert G, Schramm J, Matschke J, Sabel MC, Gramatzki D et al (2014) Molecular characterization of long-term survivors of glioblastoma using genome- and transcriptome-wide profiling. Int J Cancer 135(8):1822–1831. https://doi.org/10.1002/ijc.28836
Episkopou H, Draskovic I, Van Beneden A, Tilman G, Mattiussi M, Gobin M, Arnoult N, Londono-Vallejo A, Decottignies A (2014) Alternative lengthening of telomeres is characterized by reduced compaction of telomeric chromatin. Nucleic Acids Res 42:4391–4405. https://doi.org/10.1093/nar/gku114
Nabetani A, Ishikawa F (2011) Alternative lengthening of telomeres pathway: recombination-mediated telomere maintenance mechanism in human cells. J Biochem 149:5–14. https://doi.org/10.1093/jb/mvq119
Ebrahimi A, Skardelly M, Bonzheim I, Ott I, Mühleisen H, Eckert F, Tabatabai G, Schittenhelm J (2016) ATRX immunostaining predicts IDH and H3F3A status in gliomas. Acta Neuropathol Commun 4:60. https://doi.org/10.1186/s40478-016-0331-6
Heaphy CM, De Wilde RF, Jiao Y, Klein AP, Edil BH, Shi C, Bettegowda C, Rodriguez FJ, Eberhart CG, Hebbar S, Offerhaus GJ, McLendon R, Rasheed BA, He Y, Yan H, Bigner DD et al (2011) Altered telomeres in tumors with ATRX and DAXX mutations. Science 333(6041):425. https://doi.org/10.1126/science.1207313
Heaphy CM, Subhawong AP, Hong SM, Goggins MG, Montgomery EA, Gabrielson E, Netto GJ, Epstein JI, Lotan TL, Westra WH, Shih Ie M, Iacobuzio-Donahue CA, Maitra A, Li QK et al (2011) Prevalence of the alternative lengthening of telomeres telomere maintenance mechanism in human cancer subtypes. Am J Pathol 179:1608–1615. https://doi.org/10.1016/j.ajpath.2011.06.018
Lovejoy CA, Li W, Reisenweber S, Thongthip S, Bruno J, de Lange T, De S, Petrini JHJ, Sung PA, Jasin M, Rosenbluh J, Zwang Y, Weir BA, Hatton C, Invanova E et al (2012) Loss of ATRX, genome instability, and an altered DNA damage response are Hallmarks of the alternative lengthening of telomeres pathway. PLoS Genet 8(7):e1002772. https://doi.org/10.1371/journal.pgen.1002772
Gerrit H, Gielen GH, Gessi M, Hammes J, Kramm CM, Waha A, Pietsch T (2013) H3F3A K27M mutation in pediatric CNS tumors: a marker for diffuse high-grade astrocytomas. Am J Clin Pathol 139:345–349. https://doi.org/10.1309/AJCPABOHBC33FVMO
Schwartzentruber J, Korshunov A, Liu XY, Jones DT, Pfaff E, Jacob K, Sturm D, Fontebasso AM, Quang DA, Tonjes M, Hovestadt V, Albercht S, Kool M, Nantel A, Konermann C et al (2012) Driver mutations in histone H3.3 and chromatin remodelling genes in paediatric glioblastoma. Nature 482:226–231. https://doi.org/10.1038/nature10833
Cavalli FMG, Remke M, Rampasek L, Peacock J, Shih DJH, Luu B, Garzia L, Torchia J, Nor C, Morrissy AS et al (2017) Intertumoral heterogeneity within medulloblastoma subgroups. Cancer Cell 31:737–754.e6. https://doi.org/10.1016/j.ccell.2017.05.005
Northcott PA, Korshunov A, Witt H, Hielscher T, Eberhart CG, Mack S, Taylor MD (2011) Medulloblastoma comprises four distinct molecular variants. J Clin Oncol 29(11):1408–1414. https://doi.org/10.1200/JCO.2009.27.4324
Ramaswamy V, Remke M, Bouffet E, Bailey S, Clifford SC, Doz F, Kool M, Dufour C, Vassal G, Milde T, Witt O, · Von Hoff K, Pietsch T, Northcott PA, Gajjar A, Robinson GW et al (2016) Risk stratification of childhood medulloblastoma in the molecular era: the current consensus. Acta Neuropathol 131:821–831. https://doi.org/10.1007/s00401-016-1569-6
Taylor MD, Northcott PA, Korshunov A, Remke M, Cho YJ, Clifford SC, Eberhart CG, Parsons DW, Rutkowski S, Gajjar A, Ellison DW, Lichter P, Gilbertson RJ, Pomeroy SL, Kool M, Pfister SM (2012) Molecular subgroups of medulloblastoma: the current consensus. Acta Neuropathol 123(4):465–472. https://doi.org/10.1007/s00401-011-0922-z
Van Bueren AO, Kortmann RD, Von Hoff K, Friedrich C, Mynarek M, Muller K, Goschzik T, Mühlen A, Gerber N, Warmuth-Metz M, Soerensen N, Deinlein F, Benesch M, Zwiener I et al (2016) Treatment of children and adolescents with metastatic medulloblastoma and prognostic relevance of clinical and biologic parameters. J Clin Oncol 34(34):4151–4160. https://doi.org/10.1200/JCO.2016.67.2428
Louis DN, Ohgaki H, Wiestler OD, Cavenee WK (eds) (2016) WHO classification of tumours of the central nervous system, 4th edn. IARC, Lyon
Kool M, Koster J, Bunt J, Hasselt NE, Lakeman A, van Sluis P, Troost D, Schouten-van Meeteren N, Caron HB, Cloos J, Mrsic A, Ylstra B, Grajkowska W, Hartmann W, Pietsch T, Ellison D, Clifford SC, Versteeg R (2008) Integrated genomics identifies five medulloblastoma subtypes with distinct genetic profiles, pathway signatures and clinicopathological features. PLoS ONE 3(8):e3088. https://doi.org/10.1371/journal.pone.0003088
Schwalbe EC et al (2017) Novel molecular subgroups for clinical classification and outcome prediction in childhood medulloblastoma: a cohort study. Lancet Oncol 18:958–971. https://doi.org/10.1016/S1470-2045(17)30243-7
Morrissy AS, Cavalli FMG, Remke M, Ramaswamy V et al (2017) Spatial heterogeneity in medulloblastoma. Nat Genet 49(5):780–788. https://doi.org/10.1038/ng.3838
Wu X, Northcott PA, Dubuc A, Dupuy AJ, Shih DJ, Witt H et al (2012) Clonal selection drives genetic divergence of metastatic medulloblastoma. Nature 482:529–533. https://doi.org/10.1038/nature10825
Lannering B, Rutkowski S, Doz F, Pizer B, Gustafsson G, Navajas A et al (2012) Hyperfractionated versus conventional radiotherapy followed by chemotherapy in standard-risk medulloblastoma: results from the randomized multicenter HITSIOP PNET 4 trial. J Clin Oncol 30:3187–3193. https://doi.org/10.1200/jco.2011.39.8719
Shih DJ, Northcott PA, Remke M, Korshunov A, Ramaswamy V, Kool M et al (2014) Cytogenetic prognostication within medulloblastoma subgroups. J Clin Oncol 32:886–896. https://doi.org/10.1200/jco.2013.50.9539
De Braganca KC, Packer RJ (2013) Treatment options for medulloblastoma and CNS primitive neuroectodermal tumor (PNET). Curr Treat Options Neurol 15:593–606. https://doi.org/10.1007/s11940-013-0255-4
Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A, Scheithauber BW, Kleihues P (2007) The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol 2007 114(2):97–109. https://doi.org/10.1007/s00401-007-0243-4
Gandola L, Massimino M, Cefalo G, Solero C, Spreafico F, Pecori E, Riva D, Collini P, Pignoli E, Giangaspero F, Luksch R, Berretta S, Poggi G, Biassoni V, Ferrari A, Pollo B, Favre C, Sardi I, Terenziani M, Fossati-Bellani F (2009) Hyperfractionated accelerated radiotherapy in the milan strategy for metastatic medulloblastoma. J Clin Oncol 27(4):566–571. https://doi.org/10.1200/JCO.2008.18.4176
Poon SS, Lansdorp PM (2001) Quantitative fluorescence in situ hybridization (Q-FISH). Curr Protoc Cell Biol Chapter 18:Unit18 14
Sturm D, Witt H, Hovestadt V, Khuong-Quang DA, Jones DT, Konermann C, Pfaff E, Tonjes M, Sill M, Bender S, Kool M, Zapatka M, Becker N, Zucknick M, Hielscher T, Liu XY et al (2012) Hotspot mutations in H3F3A and IDH1 define distinct epigenetic and biological subgroups of glioblastoma. Cancer Cell 22:425–437. https://doi.org/10.1016/j.ccr.2012.08.024
Cifuentes-Rojas C, Shippen DE (2012) Telomerase regulation. Mutat Res 730:20–27. https://doi.org/10.1016/j.mrfmmm.2011.10.003
Montanaro L, Calienni M, Ceccarelli C, Santini D, Taffurelli M, Pileri S, Trere D, Derenzini M (2008) Relationship between dyskerin expression and telomerase activity in human breast cancer. Cell Oncol 30:483–490. https://doi.org/10.3233/CLO-2008-0436
Nandakumar J, Cech TR (2013) Finding the end: recruitment of telomerase to telomeres. Nat Rev Mol Cell Biol 14:69–82. https://doi.org/10.1038/nrm3505
Rodriguez FJ, Brosnan-Cashman JA, Allen SJ et al (2019) Alternative lengthening of telomeres, ATRX loss and H3-K27M mutations in histologically defined pilocytic astrocytoma with anaplasia. Brain Pathol 29(1):126–140. https://doi.org/10.1111/bpa.12646
Lee J, Solomon DA, Tihan T (2017) The role of histone modifications and telomere alterations in the pathogenesis of diffuse gliomas in adults and children. J Neurooncol 132(1):1–11. https://doi.org/10.1007/s11060-016-2349-9
Acknowledgements
Simone Minasi was supported by “Associazione Fabrizio Procaccini Onlus” (Grant No. 121). The study was also supported by “Associazione con Lorenzo per mano” (Grant No. 212).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethical approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Minasi, S., Baldi, C., Pietsch, T. et al. Telomere elongation via alternative lengthening of telomeres (ALT) and telomerase activation in primary metastatic medulloblastoma of childhood. J Neurooncol 142, 435–444 (2019). https://doi.org/10.1007/s11060-019-03127-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-019-03127-w