
Abstract
Intracranial melanotic schwannomas (IMSch) are extremely rare nerve sheath tumors with features of Schwann cells that produce melanin. After a thorough review of the available literature since 1967, we report not only the 20th case of IMSch but a comprehensive modern-era analysis of radiographic and histological key-points to be considered when diagnosing and treating patients with this rare known entity. This is the case of a 43 years-old woman who presented with severe headaches 9 years ago (2008). At that time, MRI of the brain showed a 1.5 × 1.4 cm lesion at the level of the left cerebellar peduncle without any evidence of edema, mass effect or hydrocephalus. Given that the patient was neurologically intact, a conservative management with serial MRIs was recommended. Patient stopped following up due to the absence of symptoms. Over the course of the past year, patient noted mild left sided hearing loss and facial weakness, as well as some balance instability that progressed over the last 3 months. Given the presentation and progression of these signs and symptoms, a new MRI was performed in which considerable growth of the lesion was identified, measuring 2.5 × 2.8 × 2.6 cm with mass effect on the pons and the inferior fourth ventricle. She underwent a far lateral approach without a C1 hemilaminectomy for the resection of this lesion. Final pathology was consistent with a non-psammomatous melanotic schwannoma (NPMS) with areas of necrosis. Besides this case, only two other cases of IMSch with findings of necrosis have been reported in the literature, all of them reporting a subtotal resection. Evaluation of all previously reported cases of IMSch shows a male prevalence with a 1.6:1 male to female ratio. IMSch is radiographically T2 hypointense and can be differentiated from Schwannomas that are classically T2 hyperintense. In this case, only a subtotal resection was feasible due to the tumor’s overwhelming inherent attachment to vital structures such as cranial nerves (CN), brainstem, and vasculature. While MSch is considered histologically benign, several factors including localization, surrounding structures, the rate of growth, tumor volume resection and histological necrosis should be considered in determining prognosis and further adjuvant treatment planning.
Graphical Abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Melanotic schwannomas (MSch) are extremely rare pigmented neural tumors that are slow growing, encapsulated neoplasms derived from neuroectodermal origin [1,2,3]. MSch represents up to 1% of all nerve sheath tumors and can be found in paraspinal areas, sympathetic ganglion, skin, soft tissues, bone and visceral organs [4,5,6,7,8,9]. It is thought that this schwannoma variant can synthesize melanin and histologic examination shows both melanocytes and schwann cells [3, 9, 10]. A detailed review of the literature was conducted through PubMed and Google Scholar with the terms: melanotic schwannomas, melanotic tumors, and intracranial location. Only 19 cases of MSch with intracranial location were found since 1967, making IMSch an extremely rare pathology [9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26]. While MSch can be distinguished from typical schwannomas, it is challenging to distinguish MSch from malignant melanoma [3, 27, 28]. MS in general is considered a benign tumor, but it can become malignant and even metastasize in patients with familiar syndromes such as Carney complex or neurofibromatosis type II [10, 29, 30]. This manuscript aims to provide a platform with all the reported experiences to generate awareness and a critical thinking among readers for new hypothesis regarding this tumor pathophysiology and treatment.
Illustrative case
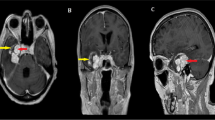
This is the case of a 43 years-old woman who presented with severe headaches 9 years ago (2008) and an MRI that showed a heterogeneously enhancing lesion centered within the left middle cerebellar peduncle with mass effect on the left pons measuring 1.5 × 1.4 × 1.0 cm (in the transverse, anteroposterior, and craniocaudal dimensions). The lesion was initially observed with yearly MRIs for the first few years. Given that the lesion was stable with apparent lack of symptoms, the patient stopped following up for almost 7 years. In the last year, she became symptomatic with new balance instability, left sided hearing difficulty, mild left facial paresis and decreased sensation on V2 and V3 distribution. An MRI of the brain demonstrated that the lesion had grown to 2.5 × 2.8 × 2.6 cm (in the transverse, anteroposterior, and craniocaudal dimensions) causing mass effect on the pons and inferior fourth ventricle (Fig. 1). A preoperative CT scan showed a hyperdense lesion arising from the skull base suggesting a vascularized dural based tumor.

a–c Different sections of an MRI T1 with contrast showing a partially calcified heterogeneously enhancing lesion centered within the left middle cerebellar peduncle with mass effect on the left pons. The lesion measures 2.5 × 2.8 × 2.6 cm (in the transverse, anteroposterior and craniocaudal dimensions). b, c Mild compression of the inferior fourth ventricle is identify without hydrocephalus
Operative details
Preoperative imaging suggested that this was a vascular lesion arising from the skull base with a potential dural attachment. Therefore, in order to safely resect the tumor, we chose a far lateral approach which allowed much better visualization of the cranial nerves and vasculature in this region. Using a diagonal trajectory, a linear skin incision was made between the asterion and the mastoid tip extending to the spinous process of C2 [31] (Fig. 2). The muscular flap was elevated en bloc with a sub-periosteal dissection performed medially and laterally while protecting the vertebral artery. A paracondylar variation of the Far Lateral approach was performed in the following manner: Three burr holes were placed, one close to the asterion, a second one next to the lower part of sigmoid sinus close to occipital condyle and the last one inferior-lateral to the inion. A suboccipital craniotomy was performed by cutting parallel to the transverse sinus and lateral to sigmoid sinus connecting to the foramen magnum and the occipital condyle. A meticulous drilling around the extracranial aspect of the jugular foramen was carried out using a diamond burr while monitoring for lower cranial nerves. A hemilaminectomy of C1 was not performed in this case. The dura was opened in a cruciate manner reflecting the leaflets toward the sigmoid and transverse sinuses. After opening the dura, the cisterna magna, premedular and cerebellomedular cisterns were dissected using Rhoton micro-instruments. This allowed the brain to relax improving the visualization of the CN V, VII-XI, as well as the tumor (Fig. 4a). The tumor location was very complex, and any manipulation of it would cause neuromonitoring changes on CN V and VII. After meticulous and delicate dissection, some parts of the tumor were freed from CN VII and IX, allowing us to resect parts of the tumor located around these structures; however, the majority of the tumor was tenaciously attached to the cranial nerves with no clear plane for dissection (Fig. 4b). The diffuse attachment also made it challenging to discern which CN gave rise to the tumor. A sizable vessel thought to be a branch of the anterior inferior cerebellar artery (A.I.C.A) was visualized within the tumor (Fig. 4c). Any further manipulation of the tumor caused significant firing of CN VII, therefore, we determined that a maximum safe resection was accomplished. At the end the procedure neuromonitoring was stable. The bone flap was secured in place and skin was closed. Post-operatively patient had left House Brackmann grade IV facial deficit with considerable improvement to House Brackmann grade II at her 3-month follow-up visit. The patient is currently undergoing Gamma Knife radiation at 15 Gy.

a Three burr holes were placed, one close to the asterion, a second one next to the lower part of sigmoid sinus close to occipital condyle and the last one inferior-lateral to the inion. b A suboccipital craniotomy was performed by cutting parallel to the transverse sinus and lateral to sigmoid sinus connecting to the foramen magnum and the occipital condyle. S superior, I inferior, TS transverse sinus, SS sigmoid sinus
Pathology result
After careful and extensive study, the final diagnosis was non-psammomatous melanotic schwannoma. It was challenging to make this diagnosis due to dense pigmentation and abundant associated melanophages (Fig. 3d). The cytomorphology of the neoplastic cells, as well as presence of focal collagen IV deposition around cell nests and lack of psammoma bodies supported the diagnosis of non-psammomatous MSch. Clinical and histological criteria for malignancy have not yet been clearly formulated for this pathology. Despite the lack of mitotic activity or nuclear anaplasia, the presence of extensive necrosis alludes to a more aggressive tumor behavior. Collagen IV immunohistochemical stain shows a continuous basement membrane around the tumor cells (Fig. 3f). Cells with schwannian differentiation have a continuous basement membrane whereas cells with melanocytic differentiation and histiocytes lack of this feature.

a Cranial nerves V, VII, IX, and X are in close relation with the tumor. b A dark tumor can be appreciated after dissection and separation of the cranial nerves. c Yellow dashed line showing a branch of A.I.C.A within the tumor. d Yellow circle showing a tumor cells nest surrounded by melanophages (green arrows pointing at the melanophages that are macrophages that engulf the melanin pigment released by the tumor cells). The presence of focal collagen IV deposition (blue arrows) around cell nests and lack of psammoma bodies supports the diagnosis of non-psammomatous melanotic schwannoma. e Necrosis. f (collagen IV immunohistochemical stain) Blue arrow highlights a continuous basement membrane around a tumor cell supporting schwannian differentiation. On the left side of the dashed line, a mixture of cells that have basement membrane staining and ones that don’t, representing a mixture of melanophages and cells with schwannian differentiation. On the right hand side of the dashed line are a collection of just melanophages, note the lack of collagen IV staining. A.I.C.A anterior inferior cerebellar artery

a Schwannoma in left CPA with classical T2 iso-hyperintensity, while b shows an intracranial melanotic schwannoma that displays T2 iso-hypointense radiographical features. CPA cerebellopontine angle
Discussion
MSchs are a rare variant of schwannoma that accounts for 1% of all nerve sheath tumors that presents in young patients between the fourth and fifth decade [9, 10]. They are mostly found in paraspinal ganglia [4,5,6,7,8,9]. MSch with an intracranial location are extremely rare presentations and to the best of our knowledge we are reporting the most recent case of intracranial melanotic schwannoma IMSch, bringing the total in the world literature to only 20 cases since 1967 [9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26]. Histologically, MSch present characteristics of both melanocytes and Schwann cells [3, 26, 32]. Melanocytes and Schwann cells have their embryological origin from the neural crest cells (NC) after emigration form the neural tube (NT). NC cells that migrate dorsolaterally will give rise to melanocytes. NC cells that migrate dorsoventrally will generate Schwann cells progenitors (SCPs) that will later become mature Schwann cells if they stay in contact with nerve fibers. However, detached SCPs from the nerve environment can also indirectly generate melanocytes. This lineage switching from SCPs has been shown to respond to the up/down regulation of FOXD3 being the upregulation favorable to SC differentiation [3, 33, 34]. Their embryological origin, as well as the ability of the Schwann cells to dedifferentiate and re-enter the cell cycle in response to nerve damage [35,36,37] might be an interesting topic to further explore the etiology of this tumors. Macroscopically, MSchs have the appearance of a black tumor that differentiate it from classic schwannomas [1, 3, 5]. Both regular schwannomas and MSch are MRI contrast enhancing lesions, however the differential diagnosis of IMSch should be considered when a lesion is localized at the CPA with T2 hypointensity. All previously reported IMSch cases have been described as T2 isointense to hypointense lesions (Table 1, Fig. 4). The radiographic features of IMSch are consistence with other extracranial MSch and other tumors that contain melanin such as melanoma [28, 38]. In addition, histologically, MSch lacks all the characteristics of schwannoma such as clear cut Antoni A and B features or verocay bodies [7, 39]. A histological differentiation is much more challenging between MSch and malignant melanomas, which usually contains psammoma bodies and often exhibits malignant nuclear features such as mitotic figures, necrosis and high KI 67 index [5, 6].
While MSch in general is histologically considered a benign tumor that can cause neurological symptoms due to mass effect, it is known to be a more difficult variant to treat than classical schwannomas [9]. After thorough literature search, there were only 26.7% of cases of MSch that were resected extra-cranially that recurred locally [4, 7,8,9]. Vallat-Decovelaere reviewed 77 cases of spinal MSch in which 17 patients that were followed > 5 years showed overall recurrence rate of 35.3%, metastasis rate of 29.5%, and mortality rate of 35% [4]. Of the 19 IMSch cases, only 6 cases recurred at their last follow-up (Table 1). There was only one case of metastasis to lung despite gross total resection [11]. There was another case where MSch was found intracranially and in subsequent imaging a second lesion was found in the spine. It is not clear if both lesions originated simultaneously, or if one metastasized from the other [12]. Despite the paucity of data available, radical surgical excision should be attempted when possible. Of the 19 IMSch cases, 50% had recurrence rate in patients that had subtotal resection while gross total resection only had 25% recurrence rate [10]. Nevertheless, maximum surgical resection must be tempered with preservation of function. In our case, it was not possible to do a gross total resection without major neurological deficit, since the tumor was inherently attached to CN V, VII–XI, as well as the pons.
Necrosis is generally considered as one of the histopathological features of tumor aggressiveness. After a careful review of the literature, only three cases, including the present case, have reported necrosis [24, 25], (Table 1). It is interesting to note that in the cases where necrosis was reported, a subtotal resection was only achieved. At the same time, from the 19 cases, only 8 formally reported the absence of necrosis; from these, 6 cases had a gross total resection [9, 10, 12, 17, 19, 20, 22, 23] (Table 1). This is an interesting finding that raises the question, “Does the presence of necrosis induce melanotic schwannomas to be more adherent to nearby structures?”. Further studies are needed to understand the effects of necrosis in MS and its adherent properties.
While there are no guidelines, review of the literature suggests that radiotherapy should be pursued especially when there is subtotal resection [10]. Given the recurrence rate and the metastatic potential, radiation has been strongly advocated by some authors especially if they display any features of malignancy [9, 11, 20, 25, 26]. There were 3 of the 19th reported IMSch cases where post-operative radiation showed disease control up to 48 months, and of those, only one case had a recurrence of tumor despite radiation [6, 13, 14]. Similarly, Zhang et al. reported 13 cases of extracranial MSch where they observed a lower rate of recurrence and metastasis in patients treated with Radiation postoperatively [6]. We have reviewed and discussed this research with the patient who decided to proceed with proton beam therapy. She is currently undergoing treatment.
Conclusion
Intracranial melanotic schwannomas should be part of the differential diagnosis for T2 hypointense tumors located at the skull base. Gross total resection should be pursued when anatomy allows. Although data is not yet significant, radiation therapy may be considered and further studied in patients with incomplete tumor resection.
References
Torres-Mora J, Dry S, Li X, Binder S, Amin M, Folpe AL (2014) Malignant melanotic schwannian tumor: a clinicopathologic, immunohistochemical, and gene expression profiling study of 40 cases, with a proposal for the reclassification of “melanotic schwannoma”. Am J Surg Pathol 38(1):94–105. doi: 10.1097/PAS.0b013e3182a0a150
Millar WG (1932) A malignant melanotic tumour of ganglion cells arising from a thoracic sympathetic ganglion. J Pathol 35(3):351–357
Arvanitis LD (2010) Melanotic schwannoma: a case with strong CD34 expression, with histogenetic implications. Pathol Res Pract 206(10):716–719. doi:10.1016/j.prp.2010.02.011
Burns DK, Silva FG, Forde KA, Mount PM, Clark HB (1983) Primary melanocytic schwannoma of the stomach. Evidence of dual melanocytic and schwannian differentiation in an extra-axial site in a patient without neurofibromatosis. Cancer 52(8):1432–1441
Höllinger P, Godoy N, Sturzenegger M (1999) Magnetic resonance imaging findings in isolated spinal psammomatous melanotic schwannoma. J Neurol 246(11):1100–1102
Marton E, Feletti A, Orvieto E, Longatti P (2007) Dumbbell-shaped C-2 psammomatous melanotic malignant schwannoma. Case report and review of the literature. J Neurosurg Spine 6(6):591–599. doi:10.3171/spi.2007.6.6.14
Myers JL, Bernreuter W, Dunham W (1990) Melanotic schwannoma. Clinicopathologic, immunohistochemical, and ultrastructural features of a rare primary bone tumor. Am J Clin Pathol 93(3):424–429
Shields JA, Font RL, Eagle RC Jr, Shields CL, Gass JD (1994) Melanotic schwannoma of the choroid. Immunohistochemistry and electron microscopic observations. Ophthalmology 101(5):843–849
Spina A, Gagliardi F, Boari N, Terreni MR, Mortini P (2015) Intracranial melanotic schwannomas. J Neurol Surg A 76(5):399–406. doi:10.1055/s-0034-1393926
Er U, Kazanci A, Eyriparmak T, Yigitkanli K, Senveli E (2007) Melanotic schwannoma. J Clin Neurosci 14(7):676–678
Beck DW, Menezes AH (1987) Lesions in Meckel’s cave: variable presentation and pathology. J Neurosurg 67(5):684–689
Buhl R, Barth H, Hugo HH, Mautner VF, Mehdorn HM (2004) Intracranial and spinal melanotic schwannoma in the same patient. J Neurooncol 68(3):249–254
Carney JA (1990) Psammomatous melanotic schwannoma: a distinctive, heritable tumor with special associations, including cardiac myxoma and the Cushing syndrome. Am J Surg Pathol 14(3):206–222
Carrasco CA, Rojas-Salazar D, Chiorino R, Venega JC, Wohllk N (2006) Melanotic nonpsammomatous trigeminal schwannoma as the first manifestation of Carney complex: case report. Neurosurgery 59(6):E1334
Dastur DK, Sinh G, Pandya S (1967) Melanotic tumor of the acoustic nerve: case report. J Neurosurg 27(2):166–170
Díaz Beveridge R, Richart Aznar P, Núñez Lozano C, Chirivella Casanova M, Corbellas Aparicio M, Montalar Salcedo J (2010) Orbital and myocardial metastases of a primary pulmonary melanotic schwannoma. Clin Transl Oncol 12(7):509–511
Ditz C, Brunswig K, Meyer C, Reusche E, Nowak G, Tronnier V (2011) Intracranial melanotic schwannoma: a case report of recurrence with extra-and intradural manifestation two decades after initial diagnosis and treatment. Cent Eur Neurosurg 72(04):211–215
Earls JP, Robles HA, McAdams H, Rao K (1994) General case of the day. Malignant melanotic schwannoma of the eighth cranial nerve. Radiographics 14(6):1425–1427
Jensen O, Bretlau P (1990) Melanotic schwannoma of the orbit. Apmis 98(7–12):713–723
Mey K, Buchwald C, Daugaard S, Prause J (2006) Sinonasal schwannoma—a clinicopathological analysis of five rare cases. Rhinology 44(1):46
Miller R, Sarikaya H, Sos A (1986) Melanotic schwannoma of the acoustic nerve. Arch Pathol Lab Med 110(2):153–154
Quencer RM, Stokes NA, Wolfe D, Page LK (1979) Melanotic nerve sheath tumor of the gasserian ganglion and trigeminal nerve. Am J Roentgenol 133(1):142–144
Ranjan A, Chacko G, Chandi S (1995) Intracerebellar melanotic schwannoma: a case report. Br J Neurosurg 9(5):687–690
Saint-Blancard P, Goasguen O, Kossowski M, Dulou R (2008) A rare primary tumor of the cerebellopontine angle: melanotic schwannoma, a pigmented tumor with unpredictable prognosis. La Revue de medecine interne 29(7):587–590
Scheithauer BW, Erdogan S, Rodriguez FJ, Burger PC, Woodruff JM, Kros JM, Gokden M, Spinner RJ (2009) Malignant peripheral nerve sheath tumors of cranial nerves and intracranial contents: a clinicopathologic study of 17 cases. Am J Surg Pathol 33(3):325–338
Zhang HY, Yang GH, Chen HJ, Wei B, Ke Q, Guo H, Ye L, Bu H, Yang K, Zhang YH (2005) Clinicopathological, immunohistochemical, and ultrastructural study of 13 cases of melanotic schwannoma. Chin Med J 118(17):1451–1461
Culhaci N, Dikicioglu E, Meteoglu I, Boylu S (2003) Multiple melanotic schwannoma. Ann Diagn Pathol 7(4):254–258
Atlas SW, Grossman RI, Gomori JM, Guerry D, Hackney DB, Goldberg HI, Zimmerman RA, Bilaniuk LT (1987) MR imaging of intracranial metastatic melanoma. J Comput Assist Tomogr 11(4):577–582
Tawk RG, Tan D, Mechtler L, Fenstermaker RA (2005) Melanotic schwannoma with drop metastases to the caudal spine and high expression of CD117 (c-kit). J Neurooncol 71(2):151–156. doi:10.1007/s11060-004-9301-0
Vallat-Decouvelaere AV, Wassef M, Lot G, Catala M, Moussalam M, Caruel N, Mikol J (1999) Spinal melanotic schwannoma: a tumour with poor prognosis. Histopathology 35(6):558–566
Benet A, Rincon-Torroella J, Vivas-Buitrago T, Quiñones-Hinojosa A (2016) Far lateral approach. In: Quinones-Hinojosa A (ed) Video Atlas of neurosurgery, contemporary tumor and skull base surgery. Elsevier, New York, pp 137–146
Font RL, Truong LD (1984) Melanotic schwannoma of soft tissues. Electron-microscopic observations and review of literature. Am J Surg Pathol 8(2):129–138
Nitzan E, Pfaltzgraff ER, Labosky PA, Kalcheim C (2013) Neural crest and Schwann cell progenitor-derived melanocytes are two spatially segregated populations similarly regulated by Foxd3. Proc Natl Acad Sci USA 110(31):12709–12714
Thomas AJ, Erickson CA (2009) FOXD3 regulates the lineage switch between neural crest-derived glial cells and pigment cells by repressing MITF through a non-canonical mechanism. Development 136(11):1849–1858. doi:10.1242/dev.031989
Napoli I, Noon LA, Ribeiro S, Kerai AP, Parrinello S, Rosenberg LH, Collins MJ, Harrisingh MC, White IJ, Woodhoo A, Lloyd AC (2012) A central role for the ERK-signaling pathway in controlling schwann cell plasticity and peripheral nerve regeneration in vivo. Neuron 73(4):729–742. doi:10.1016/j.neuron.2011.11.031
Adameyko I, Lallemend F, Aquino JB, Pereira JA, Topilko P, Müller T, Fritz N, Beljajeva A, Mochii M, Liste I, Usoskin D, Suter U, Birchmeier C, Ernfors P (2009) Schwann cell precursors from nerve innervation are a cellular origin of melanocytes in skin. Cell 139(2):366–379. doi:10.1016/j.cell.2009.07.049
Rizvi TA, Huang Y, Sidani A, Atit R, Largaespada DA, Boissy RE, Ratner N (2002) A novel cytokine pathway suppresses glial cell melanogenesis after injury to adult nerve. J Neurosci 22(22):9831–9840
Hoover JM, Bledsoe JM, Giannini C, Krauss WE (2012) Intramedullary melanotic schwannoma. Rare Tumors 4(1):e3. doi:10.4081/rt.2012.e3
Merat R, Szalay-Quinodoz I, Laffitte E, Kaya G (2015) Psammomatous melanotic schwannoma: a challenging histological diagnosis. Dermatopathology 2(3):67–70. doi:10.1159/000442708
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Mahato, D., Vivas-Buitrago, T., Gassie, K. et al. Intracranial melanotic schwannomas: a rare variant with unusual adherent features. J Neurooncol 136, 299–306 (2018). https://doi.org/10.1007/s11060-017-2653-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-017-2653-z