
Abstract
Pneumocystis pneumonia is a serious lung infection caused by an original ubiquitous fungus with opportunistic behavior, referred to as Pneumocystis jirovecii. P. jirovecii is the second most common fungal agent among invasive fungal infections after Candida spp. Unfortunately, there is still an inability to culture P. jirovecii in vitro, and so a great impairment to improve knowledge on the pathogenesis of Pneumocystis pneumonia. In this context, animal models have a high value to address complex interplay between Pneumocystis and the components of the host immune system. Here, we propose a protocol for a murine model of Pneumocystis pneumonia. Animals become susceptible to Pneumocystis by acquiring an immunocompromised status induced by iterative administration of steroids within drinking water. Thereafter, the experimental infection is completed by an intranasal challenge with homogenates of mouse lungs containing Pneumocystis murina. The onset of clinical signs occurs within 5 weeks following the infectious challenge and immunosuppression can then be withdrawn. At termination, lungs and bronchoalveolar lavage (BAL) fluids from infected mice are analyzed for fungal load (qPCR) and immune response (flow cytometry and biochemical assays). The model is a useful tool in studies focusing on immune responses initiated after the establishment of Pneumocystis pneumonia.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Pneumocystis pneumonia is a serious infection caused by an original ubiquitous fungus with opportunistic behavior, referred to as Pneumocystis jirovecii, which transmission is human-to-human airborne. It primarily affects individuals with impaired immune systems induced by use of immunosuppressive drugs (corticosteroids, TNF-alpha inhibitors…) and/or pathological underlying conditions (HIV, solid organ transplantation, hematological malignancy, solid tumor…) [1, 2]. Each year, no less than 500,000 people are affected worldwide by Pneumocystis pneumonia and P. jirovecii is the second most common fungal agent among invasive fungal infections after Candida spp. [3]. The significant mortality rate related to Pneumocystis pneumonia has been estimated between 10 and 40% according the underlying pathology [4, 5]. All these factors make Pneumocystis pneumonia a contemporary public health issue and a relevant topic of scientific investigation.
There remains an important need to improve knowledge about the pathogenesis of Pneumocystis pneumonia in order to optimize diagnostic and therapeutic management. Unfortunately, the study of P. jirovecii is a tough task as revealed by the inability to culture this organism in vitro [6]. In this context, animal models have a high value to address the complex interplay between Pneumocystis and the components of the host immune system [7].
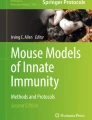
Based on the analysis of the published literature regarding these models and personal experience, we propose herein a ready-to-use protocol for a murine model of Pneumocystis pneumonia (Fig. 1). It is adapted to study the role and the kinetics of the actors of the immune system once the disease is established.

Timeline of the murine model of Pneumocystis pneumonia Female C57BL/6J mice are immunosuppressed during six weeks by administration of dexamethasone (2 mg/L) in drinking water. In the same time, tetracycline (1 mg/L) is added in drinking water to prevent from bacterial opportunistic infections. One week after the initiation of the immunosuppressive regimen, mice are anesthetized and intranasally inoculated with lung homogenates containing 5.0×105 P. murina asci or P. murina-free lung homogenates (Mock) or PBS alone (control groups). Five weeks after the infectious challenge, when Pneumocystis pneumonia occurs, the immunosuppressive regimen is stopped. Fungal load and immune response are analyzed by qPCR, flow cytometry and biochemical assays on lung and BAL at serialized times
Materials and Equipment and Methods
Preparation of Stocks of Lung Homogenates Loaded or Not with Pneumocystis murina
A stock of lung homogenates loaded with Pneumocystis murina was prepared using lungs of severe combined immunodeficiency disease (SCID) mice infected with P. murina asci. SCID mice are naturally susceptible to Pneumocystis pneumonia with high lung burdens of P. murina [8, 9]. The preparation of this stock is explained in detail in the supplementary data. In parallel, a control stock of P. murina-free lung homogenates using lungs of SCID mice uninfected with P. murina was prepared (Mock).
Animals
Specific-pathogen-free C57BL/6J female mice, five to six weeks of age, were purchased from Janvier Labs (Le Genest Saint-Isle, France). All mice were housed under specific-pathogen-free conditions in microisolator cages at the animal facility (Tours, France) and had access to food and water ad libitum. All caging procedures and manipulation were done under aseptic conditions. C57BL/6J mice were randomly assigned into three groups: on receiving P. murina (Pm, n = 12), another one that was given P. murina-free lung homogenates (Mock, n = 12) and the last one that was challenged with phosphate buffered saline (PBS, Thermo Fisher Scientific, Waltham, Massachusetts, USA) (n = 6). At each milestone, i.e. at day one, seven and fourteen post cessation of the immunosuppressive regimen (1dpci, 7dpci, 14dpci), one-third of animals were euthanized by injection of pentobarbital at 100 mg/kg (Vetoquinol, Magny-Vernois, France) after a general anesthesia of ketamine 70 mg/kg—xylazine 14 mg/kg IP. The experiment was carried out two times.
Immunosuppressive Regimen
C57BL/6J mice were immunosuppressed with dexamethasone (MSD, Summit, New-Jersey, USA) that was given in drinking water (2 mg/L) from one week before intranasal infection until five weeks after [7, 10]. Tetracycline (Sigma-Aldrich, St. Louis, Missouri, USA) was also added to drinking water (1 mg/mL) as a prophylactic strategy to prevent from the occurrence of opportunistic bacterial infection. This immunosuppressive regimen was changed three times a week.
Infectious Challenge with Pneumocystis murina
Mice were 7–8 weeks of age at the time of intranasal inoculation. Inoculums of lung homogenates were prepared in order to administrate 5.0 × 105 P. murina asci in 40 µL of PBS for the group of infected mice. The control groups were received lung homogenates from uninfected SCID mice (Mock) or PBS only. For intranasal inoculation, animals were sedated by a mixture of ketamine 70 mg/kg-xylazine 14 mg/kg (Elanco, Cuxhaven, Germany) injected intraperitoneally (IP). After an anesthesia performed as previously described [11], mice were held by the scruff of neck in order to have the nose-up position to facilitate administration. The filled tip was placed close to the mouse’s nostril and the inoculum was administrated drop by drop carefully to allow the animal to inhale each of them.
Tissue Sampling
Bronchoalveolar Lavage Fluids
Bronchoalveolar lavages (BAL) were prepared as previously described [12]. Briefly, after dissection to expose trachea, a polyurethane 18 G catheter (Terumo, Tokyo, Japan) was inserted into the trachea. With a sterile syringe connected to the catheter, 500 µL of PBS was slowly injected into the lung. The solution was then gently aspirated while massaging the thorax of the mouse. These steps were repeated 3 times in order to obtain 2000 µL of BAL fluid. The latter was then centrifuged for 5 min at 400 g and 4 °C and 500 µL of the supernatant was collected and frozen at − 80 °C for biochemical assays, and the rest was discharged. One hundred microliters of Red Blood Cell Lysing Buffer (Sigma-Aldrich, St. Louis, Missouri, USA) were added to the cell pellet and incubated for 5 min at room temperature. Then, 900 µL of PBS-FBS 2% (Fetal Bovine Serum) were added and homogenized before a filtration through a 40 µm filter. Filtrate was centrifuged for 5 min at 400 g and 4 °C, the supernatant was discarded and the cell pellet was resuspended in 250 µL of Fluorescence-Activated Cell Sorting (FACS) buffer (PBS, FBS 2%, 2 mM EDTA) for FACS analysis.
Lungs
Lungs were prepared as previously described [13]. Briefly, after heart perfusion with PBS, the lungs were aseptically removed and put in gentleMACS C tubes with 2 mL of sterile PBS with FBS 2%, Liberase TL 1/20 (Roche, Bâle, Swiss) and DNAse I 1/100 (Roche, Bâle, Swiss). Then, lungs were enzymatically and mechanically dissociated in gentleMACS Octo Dissociator, with the following program: 36 s at 165 rpm at room temperature, 30 min under agitation at 37 °C, and 36 s at 2080 rpm at room temperature. Tubes were centrifuged and each pellet was resuspended (250 µL were collected for qPCR analysis and 20 µL for microscopic observation) and suspension was filtered through a 100 µm filter. Filtrate was centrifuged and the supernatant was discarded. One milliliter of Red Blood Cell Lysing Buffer was added to the pellet and incubated for 5 min at room temperature. Then 9 mL of PBS-FBS 2% were added and homogenized before a filtration through a 40 µm filter. Filtrate was centrifuged, the supernatant was discarded and the pellet was resuspended in 1 mL of FACS buffer (PBS, FBS 2%, EDTA 2 mM) for FACS analysis. All centrifugations were performed for 5 min at 400 g and 4 °C.
Flow Cytometry
For surface-stained flow cytometry, cells were stained with extracellular mAbs in FACS buffer (PBS, FBS 2%, EDTA 2 mM) for 30 min at 4 °C. Cells were then washed and resuspended in FACS buffer for flow cytometric analysis. Flow cytometry experiments were performed in BAL and lungs samples using a MACSQuant® Analyzer (Miltenyi Biotec, Bergisch Gladbach, Germany) and analyzed using VenturiOne software (AppliedCytometry, Sheffield, South Yorkshire, England). The standard surface-stained flow cytometry was performed with the following mAbs: FITC-conjugated anti-CD4 (H129.19), FITC-conjugated anti-Ly6G (1A8), PE-Cy7-conjugated anti-CD3 (145-2C11), PE-Cy7-conjugated anti-CD11c (N418), APC-H7-conjuagated anti-CD45 (30-F11), PE-conjugated anti-CD69 (H1.2F3) from BioLegend (San Diego, California, USA); APC-conjugated anti-CD11b (M1/70) from Affymetrix eBioscience (Santa Clara, California, USA), and BV421-conjugated anti-Siglec-F (E50-2440), APC-conjugated anti-CD19 (1D3), PerCP-conjugated anti-CD8 (53–6.7) were from BD biosciences (East Rutherford, New Jersey, USA).
Enzyme-Linked Immunosorbent Assay
Interleukine-6 (IL-6) and Tumor Necrosis Factor alpha (TNF-α) in supernatant of BAL samples of mice were detected using ELISA Kits (R&D Systems, Minneapolis, Minnesota, USA) according to the manufacturer’s instructions.
Microscopic Observation of Pneumocystis murina in Lungs of Infected Mice
Lung homogenates obtained were diluted to facilitate quantification, and 20 µL were spotted onto a glass slide. The slides were fixed in methanol for 10 min and placed in contact with 0.2% calcofluor-blue brightener (Fluorescent Brightener 28®, Sigma, Saint-Louis, MO, USA) solution for 10 min [14]. Through observation of the whole spot of each glass slide, P. murina asci were evidenced microscopically using Nikon Eclipse 80i® microscope (Nikon, Champigny-sur-Marne, France) with a 100× objective and excitation at 510–560 nm.
Quantification of Pneumocystis murina by TaqMan Real-Time Quantitative PCR
Nucleic acids were isolated from lung suspensions using MycoGENIE® kit (Ademtech, Pessac, France) [15]. The PCR primers (10 µM) for P. murina are 5′-ATGAGGTGAAAAGTCGAAAGGG-3′ and 5′-TGATTGTCTCAGATGAAAAACCTCTT-3′ (Eurogentec, Seraing, Belgique) [16]. Quantitative real-time PCR was carried out using SYBR® Premix Ex Taq (Takara, Kusatsu, Japan). Each PCR was performed in 2 µL of extracted DNA (3 ng/µL) in a 20-µL reaction mix, using the LightCycler® 480 system instrument (Roche, Bâle, Swiss). The thermal cycle conditions consisted of an initial incubation at 95 °C for 2 s followed by 45 cycles of alternating incubations: 95 °C for 5 s and 60 °C for 30 s. A standard curve was generated by amplifying known copy number of a portion of P. murina DNA (GenBank accession no. AF257179) (Eurogentec, Seraing, Belgique).
Statistical Analysis
All data were analyzed using GraphPad Prism (version 8.0.2) software (GraphPad Software, San Diego, California, USA). Comparisons between groups were made with the non-parametric Mann Whitney test. A p-value less than 0.05 was considered as significant. ns: not significant; *, p < 0.05; **, p < 0.01; ***, p < 0.001.
Results
General Mortality
This animal model is associated with very low mortality within the time window defined in this study. No deaths were observed during the infectious challenge. Only two animals (out of 24, 12 for each experiment, infected with P. murina inoculum) died during the fifth week after intranasal instillation and before cessation of the immunosuppressive regimen.
Fungal Load Decreases Rapidly After Withdrawal of Immunosuppression
To evaluate the persistence of P. murina in the lung when immunosuppression is removed, we performed fluorescent microscopic observations and PCR-based analysis of P. murina. P. murina organisms were eliminated very rapidly from the lungs of mice infected after the withdrawal of the immunosuppressive regimen. Indeed, P. murina asci were only visible by microscopic observation of lung preparation at 1dpci (Fig. 2a). In addition, the fungal load at 1dpci was on average at 5.66 × 105 copy/lung, then decreased rapidly to 6.55 × 102 copy/lung at 7dpci and finally to 3.89 × 102 copy/lung at 14dpci (Fig. 2b). In control mice, which underwent the same immunosuppressive protocol, all microscopic observations and qPCR were negative. Thus, these data indicate that the pulmonary immune response is able to rapidly control P. murina even when the infection is established.

Pneumocystis murina on lung homogenates after withdrawal of the immunosuppressive regimen in lungs of P. murina infected mice. Dexamethasone immunosuppressed mice were inoculated with P. murina asci, or Mock or PBS. After five weeks, immunosuppressive regimen was stopped and mice were sacrificed at day one, seven and fourteen post cessation of the immunosuppressive regimen (1dpci, 7dpci, 14dpci). P. murina asci (spotted by blue arrows) were evidenced in lung homogenates from P. murina infected mice by calcofluor-blue brightener (x 1250, excitation at 510–560 nm) at 1dpci (a). P. murina fungal burden was determined using quantitative PCR by calculating the copy number of P. murina mitochondrial large subunit ribosomal DNA and assessed with a standard curve at 1dpci, 7 dpci and 14 dpci (b)
Once established, Pneumocystis Pneumonia Elicits a Rapid Inflammatory and Cellular Response
To characterize the alveolar and pulmonary cellular responses during P. murina infection, neutrophil and T cell populations were analyzed in BAL and lungs (Figs. 3 and 4). A massive influx of neutrophils in the alveolar compartment was observed at 1dpci (Fig. 3a and c). As infection with P. murina is performed with lung homogenates containing P. murina asci, we used P. murina-free lung homogenates as control. In those mice, no influx of neutrophils into the BAL was observed as compared to PBS-control mice (Fig. 3a and c). Regarding T cell populations in the lungs, no differences in the CD3+ total T cells were observed at 1 dpci in P. murina-infected mice as compared to control mice (Fig. 3d). The percentages of CD4+ T cells and CD8+ T cells were also similar in P. murina-infected mice compare to control mice (Fig. 3e and g). Next, we assessed lung T-cell activation by analyzing CD69 expression levels. Interestingly, CD69 levels were strongly up-regulated on CD4+ and CD8+ T cells in infected mice as soon as 1 dpci as compared to control mice (Fig. 3b, f and h). In line with the neutrophilic recruitment in the BAL, no differences in T cells activation were observed in Mock-injected mice as compare to PBS-control mice at 1 dpci.

Neutrophil and T cell responses in Pneumocystis murina-infected mice one day after cessation of the immunosuppressive regimen. Mice were immunosuppressed by administration of dexamethasone in drinking water and subsequently inoculated with P. murina asci or Mock or PBS, one week after the initiation of the immunosuppressive regimen. After five weeks, immunosuppressive regimen was stopped and mice were sacrificed one day after. Relative proportion of neutrophils and T cells in BAL and lung parenchyma were evaluated by flow cytometry. Representative dot plots of neutrophils (Live CD45+ Cd11b+ CD11c– Ly6G+) in BAL at 1dpci (a). Representative dot plots of CD4+ T cells (Live CD45+ Nkp46– CD3e+ CD4+ CD8a–) and CD8+ T cells (Live CD45+ Nkp46– CD3e+ CD4– CD8a+) in lung at 1dpci and representative histogram overlays for the expression of CD69 on CD4+ (upper plot) and CD8+ T cells (downer plot) from P. murina (black line) and Mock (grey line) infected mice (b). Relative proportion of neutrophils in BAL (c) and CD3 T cells (d), Cd4+ T cells (e), activated Cd4+ T cells (f), Cd8+ T cells (g) and activated Cd8+ T cells (h) in lungs at 1dpci. Statistical analyses were performed between each group of mice. Results represent the mean ± SEM, *p < 0.05, **p < 0.01. N = 3 to 4 mice per experimental group for each time. Data are representative of two separate experiments

Kinetics of the immune response after cessation of the immunosuppressive regimen in Pneumocystis murina-infected mice. Mice were immunosuppressed by administration of dexamethasone in drinking water and subsequently inoculated with P. murina asci or Mock, one week after the initiation of the immunosuppressive regimen. After five weeks, immunosuppressive regimen was stopped and mice were sacrificed at day one, seven and fourteen post cessation of the immunosuppressive regimen (1dpci, 7dpci, 14dpci). Relative proportion of neutrophils in BAL (a) and CD3 T cells (b), Cd4+ T cells (c), activated Cd4+ T cells (d), Cd8+ T cells (e) and activated Cd8+ T cells (f) in lungs at 1 dpci, 7dpci and 14dpci. IL-6 (g); TNF-α (h) levels were measured in the BAL supernatants by ELISA at 1dpci, 7dpci and 14dpci. Statistical analyses were performed between each group of mice. Results represent the mean ± SEM, *p < 0.05, **p < 0.01. N = 3 to 4 mice per experimental group for each time. Data are representative of two separate experiments
As the fungus was rapidly eliminated from the lungs after immunosuppression was stopped, we then analyzed the kinetics of the immune response in P. murina-infected mice. Neutrophil frequency sharply decreased at 7 and 14 dpci in the BAL of P. murina-infected mice (Fig. 4a). On the opposite, T-cell percentages increased in the lungs of mice infected with P. murina at 7 dpci and 14 dpci (Figs. 4b, c, and e). Moreover, both CD4+ and CD8+ T-cell activation persisted over time, with high CD69 expression levels at 7 dpci and 14 dpci (Fig. 4d and f).
To gain insight into the pulmonary immune response during P. murina infection, we evaluated the levels of key cytokines of this immune response. Consistent with the cellular results, IL-6 and TNF-α were rapidly and massively released in the alveolar microenvironment after the withdrawal of immunosuppressive regimen. At 1dpci, cytokine levels were significantly higher in the P. murina-infected mice compared to the control group (Fig. 4g and h). Then, the level of these two cytokines decreased over time to reach negligible levels at 7 dpci and 14 dpci.
Collectively, these data indicate that, in the mouse model described here, a significant but transient immune response rapidly develops in the lungs after the cessation of immunosuppression leading to control of the fungal burden.
Discussion
Establishing an animal model to study an infection remains a considerable challenge, but this is even greater when the infection considered is Pneumocystis pneumonia. Indeed, Pneumocystis spp. is a fungus with many particularities, including that of not being cultivable in vitro, but also being specific to its host (e.g., P. jirovecii for humans, P. murina for the mouse or Pneumocystis carinii for the rat). We can add other inconvenient factors regarding the establishment of Pneumocystis pneumonia, such as the need, most of the time, to establish a favorable terrain (e.g., induce an immunosuppressive status) and the incubation period (several weeks). Thus, the study of Pneumocystis pneumonia remains delicate and it is essential to clearly establish the scientific question of interest in order to choose the appropriate model. We propose here a murine model of Pneumocystis pneumonia useful to explore the role and the kinetics of the actors of the immune system once the disease is established.
The first question that arises when establishing an animal model is the choice of animal. Here we chose the mouse for its multiple advantages, which we have detailed previously [7]. Mice are relevant for Pneumocystis infection research because of the extensive knowledge of the murine lung immune system and the genetically engineered strains that provide useful tools to study specifically a cell type or a signaling pathway [9]. However, unlike the young rabbit that spontaneously develops Pneumocystis pneumonia [17], the mouse must acquire an immunosuppressed status to develop the disease, similar to what is found in humans. In this context, we chose to induce this immunosuppression via the administration of steroid, considered as a major risk factor for the development of Pneumocystis pneumonia in humans, directly in the drinking water [18, 19]. This method is convenient, safe and compatible with refinement of experimental procedures compared to injection of immunotherapy that imposes regular handling and stress for mice. The dose of 2 mg/L in drinking water is a compromise that avoids too intense immunosuppression and alteration of the animals [20]. Immunosuppression should be initiated prior to the infectious challenge, so that the animal is most susceptible to develop Pneumocystis pneumonia; one week is sufficient. This immunosuppression must then be continued for five weeks after the challenge, the time necessary to establish Pneumocystis pneumonia (high fungal load) but without strong clinical signs of infection (major infection signs appear after six weeks of immunosuppression post-challenge and evolve very quickly towards the death of the animal) [21]. The experimenter should pay particular attention to the choice of steroids because their anti-inflammatory effects can interfere with the immune response. Note that this immunosuppressive strategy is not representative of the viral induced immunosuppression in HIV patients for example. In addition, it should be noted that the bottles must be changed regularly, especially to avoid degradation of tetracycline (prophylaxis strategy against bacterial infections), very sensitive to light.
For the infectious challenge, we have chosen intranasal deposition of a lung homogenate from Pneumocystis-infected SCID mice. Contrary to the strategy of co-housing of healthy animals with Pneumocystis-pre-infected seeder mate fellows, which is closer to natural transmission, the instillation method allows to precisely control the time and the dose of infection. This is of great importance for the reproducibility of the results and therefore the number of mice used in the protocol (avoid the need to breed pre-infected mice in the laboratory). The inoculum must be removed from the liquid nitrogen, washed and prepared just before the challenge. Regarding the anesthesia, it is advisable to be vigilant with the ketamine-xylazine association, which is well tolerated by most of the mice, with the exception of certain very sensitive strains such as NOD-SCID mice (personal experience). It’s worth mentioning that as a control, we used intranasal deposition of lung homogenate from uninfected SCID mice and no differences in the inflammatory parameters analyzed (neutrophil recruitment, T cell activation and IL-6 and TNF-α release) were observed compared to PBS control mice.
Tissue sampling is a crucial step for subsequent analyses. When collecting the BAL, the experimenter must be careful not to alter the surrounding tissues and avoid contamination of the BAL with peripheral blood, which would distort the flow cytometry analyses. Regarding the BAL and the lungs cellularity, a total of 50.000 (in non-infected mice) and up to 1 million cells (in infected mice), and between 5 million (in non-infected mice) and 12 million (in infected mice) is expected respectively.
To confirm the effective infection and quantify the microorganism load, we chose to combine a microscopic method with a nucleic acid amplification-based method using qPCR. The former, utilizing calcofluor-blue brightener, allows for a rapid qualitative assessment of P. murina asci. Notably, this is the first instance of employing this method in an animal model of Pneumocystis pneumonia. However, molecular biology is indispensable for quantitative evaluation.
In our model, we chose to follow markers of interest of the immune response during Pneumocystis pneumonia such as neutrophils and T cells. Host response to Pneumocystis pneumonia is characterized by a larger and rapid influx of neutrophil in alveolar compartment [22,23,24] as we observe in our model in BAL. Pulmonary lymphocyte populations drive the immune response in humans and animals during Pneumocystis pneumonia [25,26,27]. In our model, Cd4+ T cells and Cd8+ T cells were rapidly activated and progressively mobilized in lung after the withdrawal of immunosuppression. In parallel to cellular markers, we chose to monitor IL-6 and TNF-α, two major pleotropic proinflammatory cytokines, because they are commonly associated with host response and clearance of P. murina [24, 28, 29]. In this model, we observe a rapid inflammatory and immune response after the cessation of the immunosuppressive regimen which coincided with the rapid decrease of the fungal load. This kinetics is important to consider and the analysis of the actors of the immune response must be early, between 1 and 7 dpci. These data also demonstrate that when the immune system becomes fully functional, it is able to clear P. murina rapidly even though the infection was deeply established in the lung.
In total, we present here a murine model of Pneumocystis pneumonia suitable for studying the kinetics of the host immune response once the disease is established. We believe that the clarity and rigor of our methodology make it an easy-to-handle model and thus contribute to its interest to the scientific community This model can be customized and adapted, for example, by using genetically modified mice or by modulating the immunosuppressive regimen. Following the example of the study conducted by Elsegeiny et al. which focuses on the modeling of human primary immune deficiencies inducing susceptibility to Pneumocystis pneumonia, we can consider comparative study to reflect the great diversity of populations developing Pneumocystis pneumonia [9]. Indeed, depending on the association between different immunosuppressive therapeutics with favourable fragile medical conditions (cancer, hematological malignancies, auto-immune diseases…), Pneumocystis pneumonia may have different characteristics (intensity, speed of evolution) which could involve distinct immune processes.
References
Thomas CF, Limper AH. Pneumocystis pneumonia. N Engl J Med. 2004;350:2487–98.
Fillatre P, Decaux O, Jouneau S, Revest M, Gacouin A, Robert-Gangneux F, et al. Incidence of Pneumocystis jiroveci pneumonia among groups at risk in HIV-negative patients. Am J Med. 2014;127(1242):e11-17.
Bongomin F, Gago S, Oladele RO, Denning DW. Global and multi-national prevalence of fungal diseases—estimate precision. J Fungi (Basel). 2017;3:57.
Li M-C, Lee N-Y, Lee C-C, Lee H-C, Chang C-M, Ko W-C. Pneumocystis jiroveci pneumonia in immunocompromised patients: delayed diagnosis and poor outcomes in non-HIV-infected individuals. J Microbiol Immunol Infect. 2014;47:42–7.
Wasserman S, Engel ME, Griesel R, Mendelson M. Burden of pneumocystis pneumonia in HIV-infected adults in sub-Saharan Africa: a systematic review and meta-analysis. BMC Infect Dis. 2016;16:482.
Cushion MT, Tisdale-Macioce N, Sayson SG, Porollo A. The persistent challenge of pneumocystis growth outside the mammalian lung: past and future approaches. Front Microbiol. 2021;12:681474.
Chesnay A, Paget C, Heuzé-Vourc’h N, Baranek T, Desoubeaux G. Pneumocystis pneumonia: pitfalls and hindrances to establishing a reliable animal model. J Fungi (Basel). 2022;8:129.
Roths JB, Marshall JD, Allen RD, Carlson GA, Sidman CL. Spontaneous Pneumocystis carinii pneumonia in immunodeficient mutant scid mice. Natural history and pathobiology. Am J Pathol. 1990;136:1173–86.
Elsegeiny W, Zheng M, Eddens T, Gallo RL, Dai G, Trevejo-Nunez G, et al. Murine models of Pneumocystis infection recapitulate human primary immune disorders. JCI Insight. 2018;3:e91894.
Khalife S, Chabé M, Gantois N, Audebert C, Pottier M, Hlais S, et al. Relationship between Pneumocystis carinii burden and the degree of host immunosuppression in an airborne transmission experimental model. J Eukaryot Microbiol. 2016;63:309–17.
Magnen M, Gueugnon F, Petit-Courty A, Baranek T, Sizaret D, Brewah YA, et al. Tissue kallikrein regulates alveolar macrophage apoptosis early in influenza virus infection. Am J Physiol Lung Cell Mol Physiol. 2019;316:L1127–40.
Baranek T, Morello E, Valayer A, Aimar R-F, Bréa D, Henry C, et al. FHL2 regulates natural killer cell development and activation during streptococcus pneumoniae infection. Front Immunol. 2017. https://doi.org/10.3389/fimmu.2017.00123.
Hassane M, Jouan Y, Creusat F, Soulard D, Boisseau C, Gonzalez L, et al. Interleukin-7 protects against bacterial respiratory infection by promoting IL-17A-producing innate T-cell response. Mucosal Immunol. 2020;13:128–39.
Desoubeaux G, Franck-Martel C, Caille A, Drillaud N, Carluer L, de Kyvon M-A, Bailly É, et al. Use of calcofluor-blue brightener for the diagnosis of Pneumocystis jirovecii pneumonia in bronchial-alveolar lavage fluids: a single-center prospective study. Med Mycol. 2017;55:295–301.
Bailly E, Debieu E, Franck-Martel C, Desoubeaux G, Chandenier J. Extraction d’ADN de Pneumocystis jirovecii à l’aide de la trousse MycoGENIE® Aspergillus fumigatus DNA extraction (Ademtech). J Mycol Méd. 2015;25:232.
Zheng M, Shellito JE, Marrero L, Zhong Q, Julian S, Ye P, et al. CD4+ T cell-independent vaccination against Pneumocystis carinii in mice. J Clin Invest. 2001;108:1469–74.
Sanchez CA, Chabé M, Aliouat EM, Durand-Joly I, Gantois N, Conseil V, et al. Exploring transplacental transmission of Pneumocystis oryctolagi in first-time pregnant and multiparous rabbit does. Med Mycol. 2007;45:701–7.
Bienvenu A-L, Traore K, Plekhanova I, Bouchrik M, Bossard C, Picot S. Pneumocystis pneumonia suspected cases in 604 non-HIV and HIV patients. Int J Infect Dis. 2016;46:11–7.
Turner PV, Brabb T, Pekow C, Vasbinder MA. Administration of substances to laboratory animals: routes of administration and factors to consider. J Am Assoc Lab Anim Sci. 2011;50:600–13.
Powles MA, McFadden DC, Pittarelli LA, Schmatz DM. Mouse model for Pneumocystis carinii pneumonia that uses natural transmission to initiate infection. Infect Immun. 1992;60:1397–400.
Ripamonti C, Bishop LR, Kovacs JA. Pulmonary Interleukin-17-positive lymphocytes increase during Pneumocystis murina Infection but are not required for clearance of pneumocystis. Infect Immun. 2017. https://doi.org/10.1128/IAI.00434-16.
Benfield TL, Kharazmi A, Larsen CG, Lundgren JD. Neutrophil chemotactic activity in bronchoalveolar lavage fluid of patients with AIDS-associated Pneumocystis carinii pneumonia. Scand J Infect Dis. 1997;29:367–71.
Swain SD, Wright TW, Degel PM, Gigliotti F, Harmsen AG. Neither neutrophils nor reactive oxygen species contribute to tissue damage during Pneumocystis pneumonia in mice. Infect Immun. 2004;72:5722–32.
Linke M, Ashbaugh A, Demland J, Koch J, Tanaka R, Walzer P. Resolution of Pneumocystis murina infection following withdrawal of corticosteroid induced immunosuppression. Microb Pathog. 2006;40:15–22.
Masur H, Ognibene FP, Yarchoan R, Shelhamer JH, Baird BF, Travis W, et al. CD4 counts as predictors of opportunistic pneumonias in human immunodeficiency virus (HIV) infection. Ann Intern Med. 1989;111:223–31.
Shellito JE, Tate C, Ruan S, Kolls J. Murine CD4+ T lymphocyte subsets and host defense against Pneumocystis carinii. J Infect Dis. 2000;181:2011–7.
Zhang N-N, Huang X, Feng H-Y, Huang L-N, Xia J-G, Wang Y, et al. Circulating and pulmonary T-cell populations driving the immune response in non-HIV immunocompromised patients with Pneumocystis jirovecii Pneumonia. Int J Med Sci. 2019;16:1221–30.
Thomas CF, Limper AH. Current insights into the biology and pathogenesis of Pneumocystis pneumonia. Nat Rev Microbiol. 2007;5:298–308.
Chou C-W, Lin F-C, Tsai H-C, Chang S-C. The importance of pro-inflammatory and anti-inflammatory cytokines in Pneumocystis jirovecii pneumonia. Med Mycol. 2013;51:704–12.
Acknowledgements
The authors would like to thank Professor El Moukhtar Aliouat and Doctor Magali Chabé from the Pasteur Institute of Lille for their helpful discussions and experience sharing on the development of murine model of Pneumocystis pneumonia, but also for having kindly provided us with lung homogenates of Pneumocystis infected mice. Figure 1 and Supplementary data—Figure 1 were created in BioRender.com.
Funding
Région Centre Val de Loire grant: Project APR-IA FLUKILLER. French National Research Agency (ANR) grant: ANR-21-CO16-0001–01.
Author information
Authors and Affiliations
Contributions
AC, GD and TB contributed to conception and design of the study, AC, LG, CP and TB performed research, AC and TB analysed data, AC wrote the first draft of the manuscript, GD and TB wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Ethical Approval
All animal experiments complied with the current European legislative, regulatory and ethical requirements and were reviewed and approved by the local animal care and use committee (reference: APAFIS#23509-2020022815336519).
Additional information
Handling Editor: Anamelia Lorenzetti Bocca.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Chesnay, A., Gonzalez, L., Parent, C. et al. Description of a Murine Model of Pneumocystis Pneumonia. Mycopathologia 189, 42 (2024). https://doi.org/10.1007/s11046-024-00846-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11046-024-00846-1