
Abstract
The kidney is a complex organ, comprised primarily of glomerular, tubular, mesangial, and endothelial cells, and podocytes. The fact that renal cells are terminally differentiated at 34 weeks of gestation is the main obstacle in regeneration and treatment of acute kidney injury or chronic kidney disease. Furthermore, the number of chronic kidney disease patients is ever increasing and with it the medical community should aim to improve existing and develop new methods of renal replacement therapy. On the other hand, as polypharmacy is on the rise, thought should be given into developing new ways of testing drug safety. A possible way to tackle these issues is with isolation and culture of renal cells. Several protocols are currently described to isolate the desired cells, of which the most isolated are the proximal tubular epithelial cells. They play a major role in water homeostasis, acid–base control, reabsorption of compounds, and secretion of xenobiotics and endogenous metabolites. When exposed to ischemic, toxic, septic, or obstructive conditions their death results in what we clinically perceive as acute kidney injury. Additionally, due to renal cells' limited regenerative potential, the profibrotic environment inevitably leads to chronic kidney disease. In this review we will focus on human proximal tubular epithelial cells. We will cover human kidney culture models, cell sources, isolation, culture, immortalization, and characterization subdivided into morphological, phenotypical, and functional characterization.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Kidney diseases can generally be classified as acute and chronic. Chronic kidney diseases (CKDs) are related to a spectrum of different pathophysiological mechanisms that result in worsening kidney function. On the other side, an important part of clinical manifestations of kidney disease are acute kidney injuries (AKIs), which are represented by nephrotoxicity and are most often related to (over)use of medication or exposure to other substances. In recent years both entities have been recognized as interlinked, meaning AKI often leads to progressive CKD, while CKD presents a major risk factor for acute worsening of patient condition (i.e. AKI) [1, 2].
The global prevalence of all-stage CKD in 2017 was 697.5 million or 9.1% [3]. Despite the clearly rising prevalence of CKD in the last century (29.3% increase since 1990), which even established CKD as one of the most common chronic diseases, the choice of renal replacement therapy (RRT) still remains limited [2, 3]. Currently, patients have to decide whether to undergo hemodialysis (HD) (at-home or in-center), peritoneal dialysis (PD), or kidney transplantation (from a living or deceased donor), whilst keeping in mind, that not all options are readily available around the world [4]. In Europe in 2017, 57% of CKD patients were treated with hemodialysis, 5% with peritoneal dialysis, and 37% with kidney transplantation [5]. Researchers are desperately trying to develop novel RRT that would improve the treatment of end-stage kidney disease patients. One goal is the construction of a bioartificial kidney (BAK) that could be implanted into the patient, while another approach is to improve the regular HD process by creating a living membrane device used instead of a dialyzer to filter blood more efficiently [6,7,8].
Another important segment in current basic and clinical research related to nephrology is the study of nephrotoxicity. Compared to CKD, this research is focusing more on AKI. About 1% of hospitalized adults above 60 years of age develop AKI due to their medication, such as non-steroidal anti-inflammatory drugs or antibiotics [7, 9, 10]. One of the problems in studying drug nephrotoxicity is the lack of appropriate models that could envision the related pathophysiology in high enough complexity to enable improvements in drug choice, especially in patients taking several drugs simultaneously. In the past, most nephrotoxicity studies were based on animal experiments, which are often difficult to translate into human use. At the same time, they are related to considerable costs and pose numerous ethical issues [10,11,12,13,14]. Metanalyses have shown that human responses to different medications are predicted correctly only in about 10–50% of times [7]. This figure is not only alarming because it is low, but also due to the huge interval, showing that current testing methods are far from reliable. One way to overcome these issues was to implement studies on 2D kidney cell cultures [15,16,17,18,19,20,21,22,23,24,25]. Furthermore, tissue-engineered kidney models were built [6, 26,27,28,29,30,31,32,33,34,35]. Their construction is based on appropriate cell lines that can be used in two ways. Individual cell types can be forced into establishing an architecture reliably simulating the functionality of in vivo tissues or parts of organs (i.e. already showing the appropriate structure) can be cut out and used for testing [12].
The following chapters will focus on various aspects of in vitro model formation based on the proximal tubular epithelial cells (PTEC). Systematically we deal with their isolation, characterization, model formation (i.e. culturing conditions), and testing. We briefly also introduce a “specific” part of the model formation, namely cell immortalization with its advantages and drawbacks.
Human kidney cell culture models
Human kidney cell culture models exist in a range of complexities (Fig. 1) [36]. The simplest designs are cultures based on a single cell type. When specific kidney cells are in question, one can isolate glomerular, tubular, and mesangial cells, podocytes, and others [37]. A problem with freshly isolated cells is that they are most useful for studying acute effects of nephrotoxins, whereas for long-term effects primary cell cultures should be established [10, 38].

Evolution of 2D and 3D tissue culture models, including advantages and disadvantages [36]. ECM extracellular matrix, HTS high throughput screening
A simple design can be further upgraded to sealed monolayers on filters with select permeability (for simulating “controlled” membrane transport), which can be exposed to different mediums on both cell sides. A 2D cell culture of human cells is simple, cost-efficient, and compatible with standard laboratory equipment. It can be even considered as potentially high throughput, since it enables testing of a variety of conditions and/or treatments. However, 2D cell cultures lack the structure of in vivo models, fail to interact with surrounding cells similarly to native tissues, and do not express kidney function as observed in vivo. As drug candidates strongly rely on results from early-stage in vitro assays to represent in vivo pharmacodynamics and -kinetics, further work had to be done [36, 39].
This led to novel tissue engineering strategies that employ kidney-on-a-chip technologies or bioprinted 3D structures using a biological cell source that is drafted on a scaffolding material and exposed to specific mediums that regulate growth, differentiation, and function [10,11,12,13,14, 40]. These modern built cell structures offer a much more complex simulation of the in vivo environment, and hence enable the study of physiology and pathophysiology of tissues. As such, these models provide a better framework for drug efficacy and toxicity studies compared to traditional methods [41].
Although many novel sophisticated technological culture systems (e.g. such that copy the cellular environment including native fluid flow, pressure, composition, and 3D extracellular matrices (ECM)) are available these days, the main aim of all models remains to form and maintain living cells that resemble the in vivo phenotype as closely as possible. The nephron, the kidney’s main structural and functional unit, consists of different segments, from which each performs a specific physiological function. Ideally, all cell types, as well as the vasculature system, should be incorporated into the design of a kidney-on-a-chip device. Nevertheless, the current state-of-the-art shows that combining two or more kidney cell types in a single model is still rather rare. Most of existing models are based on a single cell type. PTEC, which mimic secretion of the waste products and reabsorption of vital compounds from the glomerular filtrate, are the most common described cell [12, 13, 36, 40, 42].
Human proximal tubular epithelial cells sources
Primary human proximal tubular epithelial cells
Freshly isolated human PTEC from the cortex of the kidney are currently the gold standard for the development of tissue-engineered models [12, 29, 30, 32]. Considering genetic (and phenotypic) changes that can result from the techniques of cell immortalization and long-term cell passaging, these offer various advantages, as well as commonly yield far more representative results [43].
Viable human PTEC can be obtained directly from a kidney from the opposite pole of a cancerous kidney after nephrectomy, or they can be isolated using a kidney biopsy of a non-cancerous patient [12, 13]. Rarely, non-transplantable fresh post-mortem kidneys are available (e.g. due to excessive glomerulosclerosis, arterial plaques or other factors), which present a much more abundant source of fresh cells, although the time until their isolation, presents a significant limiting factor [15].
Basic protocols of human PTEC isolation consist of micro-dissection (mechanical pre-processing) of a tissue sample to obtain ~ 1 mm3 fragments, enzymatic dissociation with collagenase type I or hyaluronidase, filtration through a sieve (e.g. nylon-based, with mesh diameters in the range from 300 to 45 µm), density-gradient centrifugation, and use of a selective culture media. The culture media are protocol-specific but are usually based on the use of Dulbecco's modified Eagle's medium with nutrient mixture F-12 (DMEM/F-12), supplemented with fetal bovine serum, penicillin/streptomycin, human transferrin, selenium, hydrocortisone, insulin, and epidermal growth factor. This process results in PTEC that are > 95% of proximal tubular origin [13, 25, 28, 42, 44, 45]. Additional purification of PTEC can be performed with trypsinization and flowcytometric sorting for the proximal tubular marker leucine aminopeptidase (LAP) [44]. When the isolated cells are plated and cultured as described, they reach confluence approximately 10–13 days after seeding. After that they can be subcultured or frozen. The subcultured cells exhibit doubling times of 24–48 h and reach confluence in 3–5 days [25, 45]. Van der Hauwaert et al. described PTEC isolation by fluorescence-activated cell sorting (FACS) using antibodies to CD 10 (neutral endopeptidase, NEP) and CD13 (aminopeptidase-N, APN), two proximal tubular epithelial cell markers, which led to establishment of a pure, functional, and stable culture [28].
Purified PTEC can be cultured on semi-permeable membranes where one can access the apical and basal domains used in bi-directional flux assays (to be used for example in renal clearance studies) [29]. When seeded on Transwell™ or metal inserts, PTEC form a monolayer with an electrical resistance similar to the native tissue, expression of metabolic enzymes, formation of transport channels, and functional drug transporters, for up to 5 days [46]. Accordingly, primary PTEC have been mostly used to identify the routes and extent by which specific small molecules enter and leave PTEC. However, their use is limited to a week or two (a maximum of 12 doublings), since cells quickly lose their phenotypic properties during passaging [13, 25, 44]. New isolates can be obtained in case of longer experiments, but at the cost of potential differences in the phenotypic expression and transporter activity of the cells from respective sources. Therefore, primary PTEC are not suitable for long term exposures which are required to study kidney repair [12, 46].
Studies have shown that limited longevity and loss of functional differentiation seen in 2D monolayer cultures might be partly associated with the lack of a fluidic mechanosensory input found in the proximal tubule (PT) in vivo [29, 32]. When compared to static 2D models, PTEC in a microfluidic organ-on-a-chip device exhibited enhanced epithelial cell polarization with twofold longer microvilli, significantly greater functional characteristics (Na+/K+ ATPase activity, glucose and urea transport, albumin uptake, ammonia production, vitamin D biotransformation), their viability was extended up to 4 weeks [29,30,31,32]. Furthermore, toxicity studies have shown greater cisplatin-induced damage recovery of PTEC and injury-reversibility with organic cation transporter (OCT)-2 inhibitor cimetidine in microfluidic device compared to 2D models [29, 33].
Lastly, it is important to note that besides human, animal kidney cell lines (most commonly Madin-Darby canine kidney cells) are utilized in kidney tissue engineering as well but will not be discussed herein, since this review focuses on human tissue-derived cells [47].
Immortalized Cell Lines And Their Limitations
One way of dealing with the limited “expiration date” of PTEC is to develop immortal cell lines at the cost of losing (some) protein expression and differentiation [48]. First PTEC immortalization was performed with transduction of human papilloma virus 16 E6/E7 genes, which resulted in the so-called human kidney 2 (HK-2) cell line. They maintained proliferation of immortalized and sub-cloned cells for up to 30 passages [15]. HK-2 cells have some renal characteristics such as brush border enzymatic activity (i.e. activity related to alkaline phosphatase (ALP), γ-glutamyl transpeptidase (GGT), LAP and are positive for proximal tubular epithelial marker APN, as well as show some functional characteristics (Na+ dependent glucose transport, adenylate cyclase responsiveness to parathyroid hormone (PTH)) [15]. However, Tang et al. found that HK-2 cells expressed aquaporin (AQP)-3 which is also expressed in cells isolated from the early distal tubule [16, 49]. Jenkinson et al. compared HK-2 cells to human PTEC and found that both expressed similar ATP-binding cassette (ABC) transporters, however no uptake transporters such as organic anion transporter (OAT)-1, OAT3, OCTs, nor breast cancer resistance protein (BCRP) were found in the HK-2 line [18]. Toxicity studies have shown that HK-2 do not show a dose–response relationship to nephrotoxins (cisplatin, acetaminophen, gentamicin, 5-fluorouracil) that would resemble in vivo. This was concluded based on results, showing that these cells require extremely high doses to achieve a toxic response or even no response could be observed [17].
Another method of cell immortalization was tried using suppression of cell-cycle related genes using antisense oligonucleotides (ASOs) or small interference RNA (siRNA). Sanechika et al. transfected siRNA to a tumor suppressor protein p53 and cyclin-dependent kinase inhibitor protein p16INK4a and extended the viability of PTEC by 33 and 63 doublings, respectively. The lifespan of the transfected cells was also controllable since cell division ceased within 2 weeks after the transfection was ended. PTEC expressed the glucose transporter (GLUT)-1 and GGT equally throughout the doublings. In BAK, reabsorption of water, Na+, glucose, as well as metabolism of β-2 microglobulin and pentosidine were found. Nevertheless, the authors concluded that more studies will be necessary to fully evaluate the extend of phenotype preservation [27].
Recently, Li et al. reported the development of pseudo-immortalized SA7K cell line via a so-called zinc finger nuclease-mediated knockout of a cell cycle protein. SA7K cells exhibited normal epithelial morphology and phenotype. Compared to HK-2 cell line, SA7K maintained similar expression of uptake and efflux transporters as well as activity of CYP3A4 at early passages. However, no OAT1 and OAT3 mRNA expression was found, whereas uptake of OAT1 substrate p-aminohippuric acid (PAH) was demonstrated. The authors concluded that the reason for this disparity remained to be clarified [50].
Conditionally immortalized cell lines
Transduction of oncogenes into a human-derived cell line poses a risk of oncogene expression and hence potential complications in growth of such cells [48]. One approach to limit the risk is to transfect cells with an immortalizing construct that activates their replication under “permissive” conditions (low temperature, addition of doxycycline) and terminate it under “nonpermissive” conditions (high temperature) [12, 13, 46]. A successful technique to achieve conditional immortalization is transfection of PTECs with the temperature-sensitive mutant U19tsA58 of SV40 large T antigen (SV40T) [19]. When cultured at permissive temperatures of 33 \(^\circ\)C, the SV40T conditionally immortalized PTEC (ciPTEC) are maintained up to 50 passages [46]. Racusen et al. first constructed the so-called human proximal kidney tubule cell (HKC) lines immortalized with the SV40T. They described three HKC lines that formed apical microvilli, expressed brush border enzymes, and showed normal transporter activities. However, no well-formed tight junctions were found [19]. Recently, Nugraha et al. used the HKC-8 cell line to form a 3D model of kidney fibrosis. PTEC cell injury was found when triggered by cyclosporin A and aristolochic acid. Injured PTEC even induced differentiation of fibroblasts into myofibroblast [26].
Another method of conditional immortalization is transfection of PTECs with human telomerase reverse transcriptase (hTERT), which limits replicative senescence by maintaining telomere length [23]. Wieser et al. constructed the so-called RPTEC/TERT1 line, which formed tight junctions and densely packed microvilli, and could be stimulated by PTH but not with arginine vasopressin (AVP). The developed cell line reacted also with an enhanced ammonia genesis in lower pH, and showed functional Na+ dependent phosphate uptake, as well as activity of the megalin/cubilin transporter system [20]. Toxicity studies have shown that the RPTEC/TERT1 cell line responds to sub-cytotoxic doses of several xenobiotics and heavy metals [21, 22]. Long-term repeated dose exposure to non-cytotoxic concentrations of selected nephrotoxic compounds affected cellular regulation, activated specific stress responses (oxidative stress, DNA damage-induced stress, metal-induced stress), and decreased expression of differentiation markers, among them the tight junction protein claudin 2 (CLDN2), the Na+/K+ ATPase α1 subunit (ATP1A1), and parathyroid hormone receptor 1 (PTH1R) [22]. Additionally, several potentially clinically useful biomarkers of kidney injury (IL-19, DEFB4, CRYAB, SPINK1, LCN2, PI3, CEACAM6) were identified in toxicity studies on the RPTEC/TERT1 cell line [22].
Furthermore, several studies reported successful double transfection with SV40T and hTERT in PTEC exfoliated in urine [6, 23, 24]. ciPTEC isolated from urine (ciPTEC-U) were well characterized, expressed transporter proteins (multidrug resistance protein 4 (MRP4), P-glycoprotein (P-gp), OCT2, BCRP) and maintained drug transporter functionality (Na+ dependent phosphate uptake, albumin endocytosis), as well as metabolic activity for more than 45 passages [23, 24]. Theoretically, this should be enough for the development of BAK or a kidney-on-a-chip for most of applications. Jansen et al. compared ciPTEC-U to ciPTEC derived from kidney tissue (ciPTEC-T) and found similar functional as well as epithelial characteristics. However, expression of ECM proteins was higher in ciPTEC-T [24]. Mihajlovic et al. found that both ciPTEC lines showed absence of allostimulatory effects on peripheral blood mononuclear cells (PBMC) proliferation nor were these cell lines able to work as non-professional antigen presenting cells through the expression of human leukocyte antigen (HLA) and co-stimulatory molecules. Accordingly, ciPTEC could represent a “safe” option for BAK engineering application [6].
To conclude, as for all renal cell lines, the major limitation of ciPTEC is a rapid decrease in OATs expression upon culturing [46]. OATs functionality is essential for studying drug induced nephrotoxicity [51]. One approach to solve this issue is transduction of lentiviral particles containing genes encoding human OAT constructs. Nieskens et al. transduced OAT1 and OAT3 proteins in ciPTEC and constructed cell line with stable expression of OAT1 and OAT3 transporters for up to 29 passages [51]. On the contrary, two other studies, in which they transduced the OAT1 protein to ciPTEC, failed to demonstrate extended OAT1 gene expression [34, 35].
Pluripotent stem cell derived kidney cells
Stem cells emerged as an interesting option in the development of in vitro kidney models [52]. The nephron, the main functional unit of the kidney consist of glomeruli and renal tubules. It develops relatively early during fetal development from metanephric mesenchyme, which includes nephron progenitors (NP) along with stromal progenitors, and the ureteric bud (UB) [53,54,55,56]. The UB undergoes development and branching to form collecting ducts and signals the NP to begin differentiation into epithelial cells which connect to ductal cells [54]. A small subset of undifferentiated NP promotes UB proliferation, while the stromal progenitors support ureteric branching. Furthermore, endothelial progenitors take care of joining everything with the endothelial network. This complex interaction enables production of nephrons with systemic connection [55].
One of the main causes of the irreversibility of CKD is also the fact that NP in the metanephric mesenchyme cease propagation and are terminally differentiated at 34 weeks of gestation. This results in the inability of the kidney to regenerate itself with forming additional nephrons [53, 56]. With the rise in numbers of kidney patients and shortage of transplantable organs, researchers have tried culturing NP with the idea of being able to grow glomeruli and tubules on a differentiation medium, which could pose as a potential therapeutic application and represent a step toward kidney regenerative medicine and kidney organogenesis [57]. Additionally, it would also aid in drug and toxicity testing, as well as disease modelling, and could pose an innovative step towards renal replacement therapy [57,58,59]. Some results already show that adult kidney progenitor cells enhance the process of regeneration after acute kidney injury in rats [52].
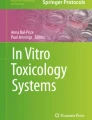
Currently, NP cells can be generated from embryonic stem cells or induced pluripotent stem cells using directed differentiation. Researchers identified during embryonic stem cell research that the UB precursors differentiate from the T+ immature mesoderm, which becomes the anterior intermediate mesoderm, and migrate caudally to form the Wolffian duct. On the other hand, the NP remain in the T+ immature mesoderm longer and differentiate into the posterior intermediate mesoderm (Fig. 2). As embryonic cells are difficult to attain, a lot of effort has been put into creating pluripotent stem cells from adult renal cells. Researchers have developed protocols for reprogramming primary normal human mesangial cells using retroviral delivery to develop induced pluripotent stem cell colonies capable of differentiation into renal progenitor cells. Additionally, they attempted generation of induced pluripotent stem cells from urine, as renal tubular cells are shed into urine each day. The idea is noteworthy as it does not require invasive procedures, but the reprogramming efficiency is currently quite low, up to 4%. Furthermore, several protocols are also described to obtain pluripotent stem cells from other tissues such the foreskin or cells such as keratinocytes and dermal fibroblast cells [55, 58].

Proposed model for kidney lineage specification (a), schematic of the dissociation/reaggregation assay (b), and schematic of the WD developmental process [55]
Several surface markers have been identified for NP cells, namely Neural Cell Adhesion Molecule 1 (NCAM1) and frizzled 7 protein (FZD7). NCAM1 is a glycoprotein that is expressed in condensed mesenchyme, nephrogenic zone, and Wilms’ tumor progenitor blastema and is not expressed in mature kidney epithelia. Additionally, NP cells can be identified by the expression of several transcriptional factors like SIX2 and odd-skipped related 1 (OSR1). These NP cells are multipotent and can differentiate into multi-segment nephron structures with characteristics of podocytes, proximal tubules, loops of Henle, and distal tubules [52, 55, 58].
Recently, researchers have used NP cells derived from urine to construct a 3D model, which could be used for nephrotoxicity tests, pharmacokinetics, nephrogenesis and kidney disease studies [60]. Additionally, a protocol has been described for Glomerulus Chip formation using directed differentiation of human induced pluripotent stem cells glomerular podocytes [61]. Another possible use of renal progenitor cells is repopulation of decellularized kidney scaffolds, which showed to be functional using a simulated bio-reactor set up [62]. Hiratsuka et al. have further reported a protocol for kidney tissue generation from human pluripotent stem cells (hPSC) using synthetic messenger ribonucleic acid (mRNA) encoding transcription factors. The first set (FIGLA, PITX2, ASCL1, and TFAP2C) induced NP cells from hPSC, and the second set (HNF1A, GATA3, GATA1, and EMX2) induced nephron epithelial cells [63].
Proximal tubular epithelial cells (PTEC) and their characterization
The PT is a segment of the nephron that lies between the Bowman’s capsule and the loop of Henley. PTEC are the most abundant cell type in the PT and play a major role in water homeostasis, acid–base control, reabsorption of compounds, as well as in secretion of xenobiotics and endogenous metabolites [64, 65].
Ideally, three segments of PTEC characteristics are evaluated when performing validation of any isolated PTEC. Phenotypical and morphological characterization are essential and independent from study design, whereas functional characterization depends on the study’s focus, which can be (various) transport mechanisms, intracellular metabolism, drug nephrotoxicity, hormone responses, etc.
A review of the latest most common techniques in each of the mentioned three characterization segments is described below.
Morphological characterization
PTEC are tall cuboidal epithelial cells with a polarized structure. Their apical and basolateral membrane domains are separated by a junctional complex (Fig. 3). The latter works like a seal and enables that molecules from the tubular lumen to travel transcellularly instead of paracellularly [66]. Any alterations in this tissue organization, as found for example in polycystic kidney disease or AKI, result in kidney dysfunction [28, 66].

Polarized structure of the proximal tubular epithelial cell [66]. The apical membrane domain has a long brushborder with microvilli (MV) and a terminal web (TW), which make connections with the lateral junctions. The lateral junctional complex separates the apical and basal domains. It consists of four types of junctions: tight junctions (zonula occludens (ZO)), anchoring junctions (zonula adherens (ZA) and desmosomes (D)), and lastly communicating (gap) junctions (GJ). The basal membrane domain is attached to the extracellular matrix (ECM) via hemidesmosomes (HD)
The apical (luminal, urine) membrane domain has a long brush border with microvilli, that increase the luminal surface, and a terminal web, which makes connections with the lateral junctions. Additionally, the apical membrane contains numerous endocytic vesicles and a prominent lysosomal compartment [25, 28, 66,67,68].
The basolateral (blood) membrane has deep infoldings, which enable extensive lateral cell processes to interdigitate with neighboring cells. Extensive interdigitations are also the site of numerous mitochondria, which provide energy for active transport. More detailed, the basolateral membrane is divided into a lateral and basal region. The lateral region is separated from the apical by the junctional complex. Four types of junctions are known (zonula occludens (ZO), zonula adherens, desmosomes, gap junctions), where especially expression of ZO-1 protein is among techniques for a quick scan of epithelial character [28, 66, 69]. The basal region is attached to the ECM via hemidesmosomes mediated by integrins [66, 68].
Morphological characterization is usually performed using transmission electron microscopy, which enables a “clear” observation of the above-mentioned characteristics (Fig. 4). When using light microscopy, epithelial cobblestone appearance and formation of hemicysts or “domes” (subepithelial collections of fluid with upward displacement of portions of the monolayer) are indicative of the proximal tubule character [19, 20, 24, 28,29,30,31,32,33, 42, 44, 64].

Transmission electron microscopy of the proximal tubular epithelial cells at 6 weeks of growth in 3D bioprinted tubule [31]. a The apical membrane with long microvilli, indicative of brush border, scale bar = 1 µm, b the basolateral membrane with basolateral interdigitations (BI), circular interdigitations marked with white arrows, basement membrane (BM) proteins secreted by cells, and extracellular matrix (ECM) underneath, scale bar = 1 µm, c basement membrane proteins secreted by cells, laminin in red, collagen IV in green, scale bar = 10 µm, d tight junction between two proximal tubular epithelial cells (white arrow), scale bar = 500 nm, e stained cell junction protein K Cadherin, scale bar = 10 µm, f a comparison of microvilli length and g density in PTEC growth in 3D bioprinted proximal tubule (3DP) compared to PTEC growth on ECM in 2D model with perfusion (2DP), PTEC growth in 2D model without perfusion (2D), and PTEC growth on bare tissue culture dish without perfusion (Dish). (Color figure online)
Polarization and membrane integrity determination
Polarization of PTEC is quickly determined using a combination of electron microscopy (brush border, cobblestone morphology, tight junctions) (Fig. 4), immunocytochemistry (ZO-1 protein expression), and western blotting/immunofluorescence (apical location of brush border enzymes APN and GGT, basolateral location of the Na+/K+ ATPase) [42, 46].
Transepithelial/transendothelial electrical resistance (TEER) is a widely used method to measure the integrity of tight junction dynamics in PTEC monolayers as well as their polarity. TEER values are strong indicators of the integrity of cellular barriers before they are evaluated for transport of drugs and chemicals [28, 70]. Higher TEER values represent an increased tightening of the cell–cell contacts and thus reduced leakiness of the monolayer, while decreased TEER values suggest increased leakiness and therefore increased weakening of the tight junctions or even cell death [71].
Phenotypical characterization
To confirm the epithelial origin of PTEC, several epithelial markers of the PT have been described (AQP1, N-cadherin, neutral endopeptidase (NEP), APN, lotus lectin, beta catenin, pan-cytokeratin). Furthermore, markers of distal tubule and collecting duct (AQP 2/3, prominin 2, uromodulin, mucin 1, E-cadherin), mesenchymal (vimentin), and myofibroblast markers can be used as a control to ensure that the correct phenotype has been obtained (Fig. 5) [20, 24, 28,29,30,31,32,33, 42, 44,45,46, 64, 72, 73].

Immunofluorescence labelling for selected epithelial markers in a CD10/CD13 double-positive cells and b CD10/CD13 double-negative cells [28]. CD10/CD13 double-positive cells were positive for pan-cytokeratin and β-catenin (two epithelial markers), aquaporin-1 (proximal tubular marker), and were negative for vimentin (mesenchymal marker) as well as MUC1 and E-cadherin (distal tubular markers)
Functional characterization
PTEC have a variety of functional characteristics, which can be sorted into four groups: brush border enzyme expression and activity, drug transporter expression and activity, drug metabolism enzyme expression and activity, and cellular energetics with redox status.
Brush border enzyme expression and activity
The PT has a dominant role in the excretion of different enzymes in the urine. As enzymes of the brush border are location specific, they can be used as markers of differentiated PTEC function (Table 1) [29, 74]. The physiological role of many of these enzymes is not well understood. GGT, alanine aminopeptidase (AAP), and lactate dehydrogenase (LDH) are normally present in urine because of tubular cell shedding. Their activity is increased in the setting of AKI, which causes up-regulation of genes encoding urinary enzymes or increased leakage of enzymes due to membrane disruption [74]. Decreased activity of ALP is often indicative of PTEC dedifferentiation [29]. GGT plays an important role in the γ-glutamyl cycle which is a glutathione synthesis and degradation pathway [32]. APN is important in salt handling as it reduces basolateral Na+/K+ ATPase activity [75]. Dipeptidyl peptidase IV (DPPIV) is a marker of cellular polarization and brush border formation as it is associated with the membrane of the microvilli and apical invaginations [76]. NEP has a major role in the degradation of vasoactive peptides including angiotensin II and bradykinin, as well as generation of angiotensin-(1–7) [77].
Drug transporter expression and activity
Intact drug transporter expression and activity is very important when evaluating cell culture kidney models. PTEC are involved in the reabsorption of vital compounds from the glomerular filtrate and secretion of waste products and xenobiotics [36].
Reabsorption of vital compounds is taking place at the apical membrane. Freely filtered low molecular weight proteins are reabsorbed via megalin-cubilin receptor-mediated endocytosis. Next to transporter-mediated endocytosis, transporters of the solute carrier family (SLC) are responsible for the transporter-mediated reabsorption of phosphate (sodium-phosphate cotransporters NaPi-IIa and NaPi-IIc), amino acids (SLC1, SLC7, SLC36, SLC38, SLC43), and glucose (GLUT1, GLUT2, sodium-glucose cotransporter (SGLT)-1, SGLT2) [36, 51, 64, 65].
Many small molecules of clinical interests (uremic toxins, xenobiotics) are albumin-bound or are too large to be freely filtered by the glomerulus. Their secretion instead depends on tubular secretion which is a two-step process [51, 65]. The first step is their uptake from blood followed by their excretion into tubular lumen across the apical membrane [28, 44, 65].
Active uptake from blood is facilitated by uptake transporters at the basolateral membrane, which are members of the SLC family. SLC transporters transport substances down or against their concentration gradient, which is maintained by the basolateral Na+/K+ ATPase. Based on their substrate, they can be divided into two groups: organic cation transporters (major OCT isoform expressed in the PT is OCT2) and organic anion transporters (OAT 1, OAT3, anion transporter polypeptide 4C1 (OATP4C1)) (Fig. 6) [46, 65].

Transport system in the proximal tubular epithelial cell. OAT organic anion transporter, OCT organic cation transporter, OCTN organic cation/carnitine transporter, URAT urate transporter, MATE multidrug and toxin extrusion, P-gp P-glycoprotein, MRP multidrug resistance-associated protein, BCRP breast cancer resistance protein
Furthermore, intracellular accumulation of substrates is prevented by active efflux at the apical membrane. Efflux is mediated by SLC family transporters or ABC transporters. Compared to SLC transporters, ABC transporters use energy generated by hydrolyzation of adenosine triphosphate (ATP) to transport molecules across the cell membrane. The SLC transporters group includes the organic cation/carnitine transporters 1 and 2 (OCTN1/OCTN2), OAT4, urate transporter 1 (URAT1), and multidrug and toxin extrusion 1 (MATE1). The most studied ABC transporter is P-gp also known as multidrug resistance protein 1 (MDR1). Additionally, multidrug resistance-associated protein (MRP)-2/4 and BCRP are commonly studied (Fig. 6) [36, 46, 65].
When evaluating drug transport activity, PTEC need to be grown on a matrix-like Transwell™ filter plates. The matrix serves as a cell growth substrate and permits compounds to diffuse through the filter pores. Importantly, the polarized structure of cells is preserved. The apical membrane facing upwards mimics the tubular lumen, whereas the basolateral membrane facing downwards mimics renal interstitial space [79, 80].
Generally, drug transport activity assays are based on the principle of drug transport inhibition (Table 2). Inhibition of basolateral uptake (e.g. OATs, OCTs) reduces the intracellular accumulation of drugs and has a nephron protective effect. Contrary, inhibition of apical efflux transporters (e.g. P-gp, MRP2, BCRP, OCTN) reduces drug exit from PTEC, which can lead to intracellular drug accumulation and nephrotoxicity [81]. Special care should be given to basolateral transporters as they might be internalized into vesicles and become dysfunctional. Therefore, it is important to demonstrate both, expression as well as functionality of basolateral transporters. Similarly, functionality of apical membrane transporters needs to be demonstrated so that complete drug handling is intact [80].
Drug metabolism enzyme expression and activity
The general belief in terms of kidney’s drugs metabolizing capacity has been that the metabolic clearance of drugs is determined exclusively by the liver while the kidneys play a minor role. However, multiple in vitro and in vivo studies demonstrated that kidneys have also a significant drug-metabolizing capacity [87].
Currently, immortalized or ciPTEC are used to understand the pathophysiology of kidney diseases, therapeutic efficacy of drugs, nephrotoxicity of compounds, and for studying therapeutic interventions for kidney repair. Understanding the metabolic enzymes present in PTEC cell lines is important for prediction of probable in vitro behavior of drugs being tested. Accordingly, determination of expression (both mRNA and protein), as well as activity of relevant enzymes, is essential [46, 80, 88].
Enzymes involved in drug metabolism are divided into two classes. Phase I metabolizing enzymes are members of the cytochrome (CYP) P450 system or they belong to the group of flavin-containing monooxygenases (FMO). They are responsible for oxidation, reduction, and hydrolyzation of xenobiotics. Compared to animal PTEC, only few CYP enzymes (CYP3A4/5, CYP4A11, CYP1B1, CYP2B6, CYP2D6, CYP4F2) were found to be constantly expressed in human PTEC. Among them, especially CYP3A4/5 and CYP4A11 are expressed at relatively high levels in the PT [46, 87, 89]. Summary of CYP enzymes activity assays is presented in Table 3.
Phase II metabolizing enzymes are members of glutathione S-transferases (GSTA1/2/4/5, GSTM1/2/3/4/5, GSTP1, GSTT1/2, FSTZ), UDP-glucuronosyltransferases (UGT1A1/6/9, UGT2B7, UGT8), and sulfontransferases (SULT1A1/3, SULT1B1/2). They are responsible for glucuronidation, sulfation, methylation, acetylation, and glutathione or amino acids conjugation. Conjugated products are more hydrophilic and therefore water-soluble, which makes them easily excretable and reduces their toxicity potential [46, 87, 88].
Cellular energetics and redox status
PTEC cellular energetics validation consists of mitochondrial function, glycolysis rate, gluconeogenesis rate, and adenine nucleotide charge evaluation. Redox status is evaluated with the glutathione (GSH)/glutathione disulphide (GSSG) ratio and rate of lipid peroxidation (Table 4) [80].
Mitochondria produce energy for the Na+/K+ ATPase to drive ion transport across the cellular membrane. Furthermore, they supply energy for cellular repair and regeneration [91]. Their function is evaluated with mitochondrial oxygen consumption and intracellular ATP concentration both indicating intact aerobic respiration [92]. Another technique is measurement of the mitochondrial membrane potential (ΔΨM), which plays a central role in processes such as ATP production, reactive oxygen species generation, and Ca2+ uptake. Decreased values of ΔΨM are associated with the opening of mitochondrial permeability pores and loss of electrochemical gradient indicating PTEC apoptosis [93, 94].
The glycolysis rate is evaluated with pyruvate and lactate production as well as LDH and hexokinase activity. Increased pyruvate and lactate concentrations or increased hexokinase and lactate dehydrogenase activity are indicators of cells hypoxia and their dysfunction [95].
Gluconeogenesis rate is evaluated with fructose-1,6-bisphosphatase activity and detection of net production of glucose from precursors lactate and glutamine [96, 97].
The adenylate energy charge (AEC) is a simple index which measures the energy status of the cell. AEC is defined as the ratio between ([ATP] + 0.5 [ADP]) and ([ATP] + [ADP] + [AMP]). When all energy poll is in the form of AMP, the energy charge is zero. Contrary, when all energy pool is in the form of ATP, the energy charge is one. Optimal AEC ranges between 0.7 and 0.95 [98].
GSH/GSSG ratio is a useful indicator of the oxidative stress. Reduced glutathione (GSH) is an important redox buffer and main antioxidant, which prevents damage caused by free radicals and peroxides. Healthy cells store more than 90% of total glutathione in the reduced form. When cells are exposed to oxidative stress, the glutathione reductase catalyzes the reaction where oxidized glutathione (GSSG) is formed. Accumulation of GSSG decreases GSH/GSSG ratio and switches the redox potential towards a more oxidized state [99, 100].
Lipid peroxidation status is another indicator of oxidative stress. Among many secondary products formed during lipid peroxidation, 4-hydroxynonenal (4-HNE) is the most toxic and therefore a major bioactive marker of lipid peroxidation [101].
Conclusions
The field of renal cell studies is ever evolving. As more and more patients succumb to CKD and are in need for RRT, innovative approaches must be invented to tackle the increasing incidence, either in the form of new drug (therapy) development, as well as on the level of better understanding of the related disease pathophysiology, again leading to novel potential treatment strategies. Additionally, polypharmacy is on the rise and as the population grows older, potential toxic drug–drug interactions and changes in drug efficiency in patients with renal diseases must be studied even more vigorously. Some of the future goals that are already on the horizon are development of advanced in vitro kidney models, 3D bioprinting methods to generate bioengineered kidneys, using decellularized kidneys and later repopulating them with human renal cells, and using microfluidic organ-on-a-chip devices to study renal disease and drug toxicity in vitro. As we are more and more successful in isolating, growing, and differentiating renal cells individually, slowly we will begin to develop increasingly complex 3D models using several cells in an in vivo like structure. Until then, we must rely on older drug assays and observational studies, and existing RRT.
Abbreviations
- AAP:
-
Alanine aminopeptidase
- ABC:
-
ATP-binding cassette
- ACE:
-
Angiotensin-converting enzyme
- AEC:
-
Adenylate energy charge
- AKI:
-
Acute kidney injury
- Albumin-FITC:
-
Albumin-fluorescein isothiocyanate conjugate protein bovine
- ALP:
-
Alkaline phosphatase
- AQP:
-
Aquaporin
- ASO:
-
Antisense oligonucleotide
- ATP:
-
Adenosine triphosphate
- ADP:
-
Adenosine diphosphate
- AMP:
-
Adenosine monophosphate
- AVP:
-
Arginine vasopressin
- BAK:
-
Bioartificial kidney
- BCRP:
-
Breast cancer resistance protein
- CD:
-
Cluster of differentiation
- ciPTEC:
-
Conditionally immortalized proximal tubular epithelial cells
- ciPTEC-T:
-
Conditionally immortalized proximal tubular epithelial cells isolated from tissue
- ciPTEC-U:
-
Conditionally immortalized proximal tubular epithelial cells isolated from urine
- CKD:
-
Chronic kidney disease
- CLDN:
-
Claudin
- CYP:
-
Cytochrome
- DPP:
-
Dipeptidyl peptidase
- ECM:
-
Extracellular matrix
- ELISA:
-
Enzyme-linked immunosorbent assay
- FACS:
-
Fluorescence-activated cell sorting
- FBP:
-
Fructose-1,6-bisphosphatase
- FMO:
-
Flavin monooxygenase
- G6PD:
-
Glucose-6-phosphate dehydrogenase
- GGT:
-
γ-Glutamyl transpeptidase
- GLUT:
-
Glucose transporter
- GSH:
-
Glutathione
- GSSG:
-
Glutathione disulphide
- GST:
-
Glutathione S-transferase
- HD:
-
Hemodialysis
- HK-2:
-
Human kidney 2
- HKC:
-
Human kidney tubule cell
- HPLC:
-
High-performance liquid chromatography
- hTERT:
-
Human telomerase reverse transcriptase
- LAP:
-
Leucine aminopeptidase
- LDH:
-
Lactate dehydrogenase
- LSC:
-
Liquid scintillation counting
- LC–MS:
-
Liquid chromatography-mass spectrometry
- MATE:
-
Multidrug and toxin extrusion
- MDR:
-
Multidrug resistance
- MRP:
-
Multidrug resistance-associated protein
- NADH:
-
Nicotine adenine dinucleotide
- NCAM:
-
Neural cell adhesion molecule
- NEP:
-
Neutral endopeptidase
- NP:
-
Nephron progenitors
- OAT:
-
Organic anion transporter
- OCT:
-
Organic cation transporter
- OCTN:
-
Organic cation/carnitine transporter
- OSR:
-
Odd-skipped related
- PBMC:
-
Peripheral blood mononuclear cells
- P-gp:
-
P-glycoprotein
- PT:
-
Proximal tubule
- PTEC:
-
Proximal tubular epithelial cells
- PTH:
-
Parathyroid hormone
- RNAi:
-
Interference RNA
- RRT:
-
Renal replacement therapy
- SGLT:
-
Sodium-glucose cotransporter
- SLC:
-
Solute carrier
- SV40T:
-
SV40 large T antigen
- TEER:
-
Transepithelial/transendothelial electrical resistance
- UB:
-
Ureteric bud
- UGT:
-
UDP-glucuronosyltransferase
- ZO:
-
Zonula occludens
References
Ferenbach DA, Bonventre JV (2016) Acute kidney injury and chronic kidney disease: from the laboratory to the clinic. Nephrol Ther 12(Suppl 1):S41–S48
Murphy D, McCulloch CE, Lin F, Banerjee T, Bragg-Gresham JL, Eberhardt MS et al (2016) Trends in prevalence of chronic kidney disease in the United States. Ann Intern Med 165(7):473–481
GBD Chronic Kidney Disease Collaboration (2020) Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 395(10225):709–733
Hemodialysis Adequacy 2006 Work Group (2006) Clinical practice guidelines for hemodialysis adequacy, update 2006. Am J Kidney Dis 48(Suppl 1):S2–S90
Kramer A, Boenink R, Noordzij M, Bosdriesz JR, Stel VS, Beltrán P et al (2020) The ERA-EDTA Registry Annual Report 2017: a summary. Clin Kidney J 13(4):693–709
Mihajlovic M, van den Heuvel LP, Hoenderop JG, Jansen J, Wilmer MJ, Westheim AJF et al (2017) Allostimulatory capacity of conditionally immortalized proximal tubule cell lines for bioartificial kidney application. Sci Rep 7(1):7103
Davies JA, Chang CH, Lawrence ML, Mills CG, Mullins JJ (2014) Engineered kidneys: principles, progress, and prospects. Adv Regen Biol 1(1):24990
Jansen J, De Napoli IE, Fedecostante M, Schophuizen CM, Chevtchik NV, Wilmer MJ et al (2015) Human proximal tubule epithelial cells cultured on hollow fibers: living membranes that actively transport organic cations. Sci Rep 5:16702
Naughton CA (2008) Drug-induced nephrotoxicity. Am Fam Physician 78(6):743–750
Davies JA (2015) Self-organized kidney rudiments: prospects for better in vitro nephrotoxicity assays. Biomarker Insights 10(Suppl 1):117–123
Sochol RD, Gupta NR, Bonventre JV (2016) A role for 3D printing in kidney-on-a-chip platforms. Curr Transplant Rep 3(1):82–92
DesRochers TM, Palma E, Kaplan DL (2014) Tissue-engineered kidney disease models. Adv Drug Deliv Rev 69–70:67–80
Davies J (2014) Engineered renal tissue as a potential platform for pharmacokinetic and nephrotoxicity testing. Drug Discov Today 19(6):725–729
Astashkina A, Mann B, Grainger DW (2012) A critical evaluation of in vitro cell culture models for high-throughput drug screening and toxicity. Pharmacol Ther 134(1):82–106
Ryan MJ, Johnson G, Kirk J, Fuerstenberg SM, Zager RA, Torok-Storb B (1994) HK-2: an immortalized proximal tubule epithelial cell line from normal adult human kidney. Kidney Int 45(1):48–57
Tang S, Leung JC, Lam CW, Lai FM, Chan TM, Lai KN (2001) In vitro studies of aquaporins 1 and 3 expression in cultured human proximal tubular cells: upregulation by transferrin but not albumin. Am J Kidney Dis 38(2):317–330
Wu Y, Connors D, Barber L, Jayachandra S, Hanumegowda UM, Adams SP (2009) Multiplexed assay panel of cytotoxicity in HK-2 cells for detection of renal proximal tubule injury potential of compounds. Toxicol In Vitro 23(6):1170–1178
Jenkinson SE, Chung GW, van Loon E, Bakar NS, Dalzell AM, Brown CD (2012) The limitations of renal epithelial cell line HK-2 as a model of drug transporter expression and function in the proximal tubule. Pflugers Arch 464(6):601–611
Racusen LC, Monteil C, Sgrignoli A, Lucskay M, Marouillat S, Rhim JG et al (1997) Cell lines with extended in vitro growth potential from human renal proximal tubule: characterization, response to inducers, and comparison with established cell lines. J Lab Clin Med 129(3):318–329
Wieser M, Stadler G, Jennings P, Streubel B, Pfaller W, Ambros P et al (2008) hTERT alone immortalizes epithelial cells of renal proximal tubules without changing their functional characteristics. Am J Physiol Renal Physiol 295(5):F1365–F1375
Simon BR, Wilson MJ, Wickliffe JK (2014) The RPTEC/TERT1 cell line models key renal cell responses to the environmental toxicants, benzo[a]pyrene and cadmium. Toxicol Rep 1:231–242
Aschauer L, Limonciel A, Wilmes A, Stanzel S, Kopp-Schneider A, Hewitt P et al (2015) Application of RPTEC/TERT1 cells for investigation of repeat dose nephrotoxicity: a transcriptomic study. Toxicol In Vitro 30(1 Pt A):106–116
Wilmer MJ, Saleem MA, Masereeuw R, Ni L, van der Velden TJ, Russel FG et al (2010) Novel conditionally immortalized human proximal tubule cell line expressing functional influx and efflux transporters. Cell Tissue Res 339(2):449–457
Jansen J, Schophuizen CM, Wilmer MJ, Lahham SH, Mutsaers HA, Wetzels JF et al (2014) A morphological and functional comparison of proximal tubule cell lines established from human urine and kidney tissue. Exp Cell Res 323(1):87–99
Detrisac CJ, Sens MA, Garvin AJ, Spicer SS, Sens DA (1984) Tissue culture of human kidney epithelial cells of proximal tubule origin. Kidney Int 25(2):383–390
Nugraha B, Mohr MA, Ponti A, Emmert MY, Weibel F, Hoerstrup SP et al (2017) Monitoring and manipulating cellular crosstalk during kidney fibrosis inside a 3D in vitro co-culture. Sci Rep 7(1):14490
Sanechika N, Sawada K, Usui Y, Hanai K, Kakuta T, Suzuki H et al (2011) Development of bioartificial renal tubule devices with lifespan-extended human renal proximal tubular epithelial cells. Nephrol Dial Transplant 26(9):2761–2769
Van der Hauwaert C, Savary G, Gnemmi V, Glowacki F, Pottier N, Bouillez A et al (2013) Isolation and characterization of a primary proximal tubular epithelial cell model from human kidney by CD10/CD13 double labeling. PLoS ONE 8(6):e66750
Jang K-J, Mehr AP, Hamilton GA, McPartlin LA, Chung S, Suh K-Y et al (2013) Human kidney proximal tubule-on-a-chip for drug transport and nephrotoxicity assessment. Integr Biol 5(9):1119–1129
Ng CP, Zhuang Y, Lin AWH, Teo JCM (2013) A fibrin-based tissue-engineered renal proximal tubule for bioartificial kidney devices: development, characterization and in vitro transport study. Int J Tissue Eng 2013:10
Homan KA, Kolesky DB, Skylar-Scott MA, Herrmann J, Obuobi H, Moisan A et al (2016) Bioprinting of 3D convoluted renal proximal tubules on perfusable chips. Sci Rep 6:34845
Weber EJ, Chapron A, Chapron BD, Voellinger JL, Lidberg KA, Yeung CK et al (2016) Development of a microphysiological model of human kidney proximal tubule function. Kidney Int 90(3):627–637
King SM, Higgins JW, Nino CR, Smith TR, Paffenroth EH, Fairbairn CE et al (2017) 3D Proximal tubule tissues recapitulate key aspects of renal physiology to enable nephrotoxicity testing. Front Physiol 8:123
Fedecostante M, Westphal KGC, Buono MF, Sanchez Romero N, Wilmer MJ, Kerkering J et al (2018) Recellularized native kidney scaffolds as a novel tool in nephrotoxicity screening. Drug Metab Dispos 46(9):1338–1350
Vriend J, Nieskens TTG, Vormann MK, van den Berge BT, van den Heuvel A, Russel FGM et al (2018) Screening of drug-transporter interactions in a 3D microfluidic renal proximal tubule on a chip. Aaps J 20(5):87
Nieskens TT, Wilmer MJ (2016) Kidney-on-a-chip technology for renal proximal tubule tissue reconstruction. Eur J Pharmacol 790:46–56
Schlondorff D (1986) Isolation and use of specific nephron segments and their cells in biochemical studies. Kidney Int 30(2):201–207
Pfaller W, Gstraunthaler G (1998) Nephrotoxicity testing in vitro—what we know and what we need to know. Environ Health Perspect 106(Suppl 2):559–569
Eneko M, Andraž S, Sebastjan B, Uroš M (2019) In vitro toxicity model: upgrades to bridge the gap between preclinical and clinical research. Bosn J Basic Med Sci 20(2):157–168
Ashammakhi N, Wesseling-Perry K, Hasan A, Elkhammas E, Zhang YS (2018) Kidney-on-a-chip: untapped opportunities. Kidney Int 94(6):1073–1086
Sakolish CM, Esch MB, Hickman JJ, Shuler ML, Mahler GJ (2016) modeling barrier tissues in vitro: methods, achievements, and challenges. EBioMedicine 5(Supplement C):30–39
Sharpe CC, Dockrell ME (2012) Primary culture of human renal proximal tubule epithelial cells and interstitial fibroblasts. Methods Mol Biol 806:175–185
Lipps C, May T, Hauser H, Wirth D (2013) Eternity and functionality—rational access to physiologically relevant cell lines. Biol Chem 394(12):1637–1648
Brown CD, Sayer R, Windass AS, Haslam IS, De Broe ME, D’Haese PC et al (2008) Characterisation of human tubular cell monolayers as a model of proximal tubular xenobiotic handling. Toxicol Appl Pharmacol 233(3):428–438
Valente MJ, Henrique R, Costa VL, Jerónimo C, Carvalho F, Bastos ML et al (2011) A rapid and simple procedure for the establishment of human normal and cancer renal primary cell cultures from surgical specimens. PLoS ONE 6(5):e19337
Masereeuw R, Vriend J, Wilmer MJ (2017) Chapter 82—kidney-on-a-chip: technologies for studying pharmacological and therapeutic approaches to kidney repair. In: Orlando G, Remuzzi G, Williams DF (eds) Kidney transplantation, bioengineering and regeneration. Academic Press, London, pp 1119–1133
Irvine JD, Takahashi L, Lockhart K, Cheong J, Tolan JW, Selick HE et al (1999) MDCK (Madin-Darby canine kidney) cells: a tool for membrane permeability screening. J Pharm Sci 88(1):28–33
Maqsood MI, Matin MM, Bahrami AR, Ghasroldasht MM (2013) Immortality of cell lines: challenges and advantages of establishment. Cell Biol Int 37(10):1038–1045
Baer PC, Geiger H (2008) Human renal cells from the thick ascending limb and early distal tubule: characterization of primary isolated and cultured cells by reverse transcription polymerase chain reaction. Nephrology (Carlton) 13(4):316–321
Li S, Zhao J, Huang R, Steiner T, Bourner M, Mitchell M et al (2017) Development and application of human renal proximal tubule epithelial cells for assessment of compound toxicity. Curr Chem Genom Transl Med 11:19–30
Nieskens TT, Peters JG, Schreurs MJ, Smits N, Woestenenk R, Jansen K et al (2016) A human renal proximal tubule cell line with stable organic anion transporter 1 and 3 expression predictive for antiviral-induced toxicity. Aaps J 18(2):465–475
Morizane R, Miyoshi T, Bonventre JV (2017) Concise review: kidney generation with human pluripotent stem cells. Stem cells 35(11):2209–2217
Tanigawa S, Taguchi A, Sharma N, Perantoni Alan O, Nishinakamura R (2016) Selective in vitro propagation of nephron progenitors derived from embryos and pluripotent stem cells. Cell Reports 15(4):801–813
Kaku Y, Taguchi A, Tanigawa S, Haque F, Sakuma T, Yamamoto T et al (2017) PAX2 is dispensable for in vitro nephron formation from human induced pluripotent stem cells. Scientific reports 7(1):4554
Taguchi A, Nishinakamura R (2017) Higher-order kidney organogenesis from pluripotent stem cells. Cell Stem Cell 21(6):730–46.e6
Tanigawa S, Nishinakamura R (2016) Expanding nephron progenitors in vitro: a step toward regenerative medicine in nephrology. Kidney Int 90(5):925–927
Becherucci F, Mazzinghi B, Allinovi M, Angelotti ML, Romagnani P (2018) Regenerating the kidney using human pluripotent stem cells and renal progenitors. Expert Opin Biol Ther 18(7):795–806
Francipane MG, Lagasse E (2016) Pluripotent stem cells to rebuild a kidney: the lymph node as a possible developmental niche. Cell Transplant 25(6):1007–1023
Chuah JKC, Zink D (2017) Stem cell-derived kidney cells and organoids: recent breakthroughs and emerging applications. Biotechnol Adv 35(2):150–167
Nguyen L, Spitzhorn LS, Adjaye J (2019) Constructing an isogenic 3D human nephrogenic progenitor cell model composed of endothelial, mesenchymal, and SIX2-positive renal progenitor cells. Stem Cells Int 2019:3298432
Morizane R, Lam AQ (2015) Directed differentiation of pluripotent stem cells into kidney. Biomark Insights 10(Suppl 1):147–152
Du C, Narayanan K, Leong MF, Ibrahim MS, Chua YP, Khoo VM et al (2016) Functional kidney bioengineering with pluripotent stem-cell-derived renal progenitor cells and decellularized kidney scaffolds. Adv Healthc Mater 5(16):2080–2091
Hiratsuka K, Monkawa T, Akiyama T, Nakatake Y, Oda M, Goparaju SK et al (2019) Induction of human pluripotent stem cells into kidney tissues by synthetic mRNAs encoding transcription factors. Sci Rep 9(1):913
Zhuo JL, Li XC (2013) Proximal nephron. Compr Physiol 3(3):1079–1123
Nigam SK, Wu W, Bush KT, Hoenig MP, Blantz RC, Bhatnagar V (2015) Handling of drugs, metabolites, and uremic toxins by kidney proximal tubule drug transporters. Clin J Am Soc Nephrol CJASN 10(11):2039–2049
Wagner MC, Molitoris BA (1999) Renal epithelial polarity in health and disease. Pediatr Nephrol 13(2):163–170
Hoppensack A, Kazanecki CC, Colter D, Gosiewska A, Schanz J, Walles H et al (2014) A human in vitro model that mimics the renal proximal tubule. Tissue Eng Part C Methods 20(7):599–609
Verlander JW (1998) Normal ultrastructure of the kidney and lower urinary tract. Toxicol Pathol 26(1):1–17
Kriz W, Elger M, Floege J, Johnson RJ, Feehally J (2010) Chapter 1—renal anatomy. Mosby, Philadelphia, pp 3–14
Srinivasan B, Kolli AR, Esch MB, Abaci HE, Shuler ML, Hickman JJ (2015) TEER measurement techniques for in vitro barrier model systems. J Lab Automat 20(2):107–126
Secker PF, Luks L, Schlichenmaier N, Dietrich DR (2018) RPTEC/TERT1 cells form highly differentiated tubules when cultured in a 3D matrix. Altex 35(2):223–234
Sánchez-Romero N, Martínez-Gimeno L, Caetano-Pinto P, Saez B, Sánchez-Zalabardo JM, Masereeuw R et al (2019) A simple method for the isolation and detailed characterization of primary human proximal tubule cells for renal replacement therapy. Int J Artif Org. https://doi.org/10.1177/0391398819866458
Legouis D, Bataille A, Hertig A, Vandermeersch S, Simon N, Rondeau E et al (2015) Ex vivo analysis of renal proximal tubular cells. BMC Cell Biol 16:12
Waring WS, Moonie A (2011) Earlier recognition of nephrotoxicity using novel biomarkers of acute kidney injury. Clin Toxicol (Phila) 49:720–728
Kotlo K, Shukla S, Tawar U, Skidgel RA, Danziger RS (2007) Aminopeptidase N reduces basolateral Na+-K+-ATPase in proximal tubule cells. Am J Physiol Renal Physiol 293(4):F1047–F1053
Andersen KJ, Maunsbach AB, Christensen EI (1998) Biochemical and ultrastructural characterization of fluid transporting LLC-PK1 microspheres. J Am Soc Nephrol 9(7):1153–1168
Vio CP, Salas D, Cespedes C, Diaz-Elizondo J, Mendez N, Alcayaga J et al (2018) Imbalance in renal vasoactive enzymes induced by mild hypoxia: angiotensin-converting enzyme increases while neutral endopeptidase decreases. Front Physiol. https://doi.org/10.3389/fphys.2018.01791
Sakolish CM, Philip B, Mahler GJ (2019) A human proximal tubule-on-a-chip to study renal disease and toxicity. Biomicrofluidics 13(1):014107
Yeste J, Illa X, Alvarez M, Villa R (2018) Engineering and monitoring cellular barrier models. J Biol Eng. 12:18
Lash LH (2016) Predictive in vitro models for assessment of nephrotoxicity and drug–drug interactions in vitro. Drug Discov Toxicol. https://doi.org/10.1002/9781119053248.ch10
Yin J, Wang J (2016) Renal drug transporters and their significance in drug-drug interactions. Acta Pharm Sin B 6(5):363–373
Vedula EM, Alonso JL, Arnaout MA, Charest JL (2017) A microfluidic renal proximal tubule with active reabsorptive function. PLoS ONE 12(10):e0184330
Caetano-Pinto P, Janssen MJ, Gijzen L, Verscheijden L, Wilmer MJ, Masereeuw R (2016) Fluorescence-based transport assays revisited in a human renal proximal tubule cell line. Mol Pharm 13(3):933–944
Vormann MK, Gijzen L, Hutter S, Boot L, Nicolas A, van den Heuvel A et al (2018) Nephrotoxicity and kidney transport assessment on 3D perfused proximal tubules. Aaps J 20(5):90
Kumari M, Sharma R, Pandey G, Ecelbarger CM, Mishra P, Tiwari S (2019) Deletion of insulin receptor in the proximal tubule and fasting augment albumin excretion. J Cell Biochem 120(6):10688–10696
Diekjurgen D, Grainger DW (2018) Drug transporter expression profiling in a three-dimensional kidney proximal tubule in vitro nephrotoxicity model. Pflugers Arch 470(9):1311–1323
Knights KM, Rowland A, Miners JO (2013) Renal drug metabolism in humans: the potential for drug-endobiotic interactions involving cytochrome P450 (CYP) and UDP-glucuronosyltransferase (UGT). Br J Clin Pharmacol 76(4):587–602
Shah H, Patel M, Shrivastava N (2017) Gene expression study of phase I and II metabolizing enzymes in RPTEC/TERT1 cell line: application in in vitro nephrotoxicity prediction. Xenobiotica 47(10):837–843
Lash LH, Putt DA, Cai H (2008) Drug metabolism enzyme expression and activity in primary cultures of human proximal tubular cells. Toxicology 244(1):56–65
Wang Z, Senn T, Kalhorn T, Zheng XE, Zheng S, Davis CL et al (2011) Simultaneous measurement of plasma vitamin D(3) metabolites, including 4β,25-dihydroxyvitamin D(3), using liquid chromatography-tandem mass spectrometry. Anal Biochem 418(1):126–133
Bhargava P, Schnellmann RG (2017) Mitochondrial energetics in the kidney. Nat Rev Nephrol 13(10):629–646
Lash LH, Putt DA, Hueni SE, Krause RJ, Elfarra AA (2003) Roles of necrosis, Apoptosis, and mitochondrial dysfunction in S-(1,2-dichlorovinyl)-L-cysteine sulfoxide-induced cytotoxicity in primary cultures of human renal proximal tubular cells. J Pharmacol Exp Ther 305(3):1163–1172
Hall AM, Rhodes GJ, Sandoval RM, Corridon PR, Molitoris BA (2013) In vivo multiphoton imaging of mitochondrial structure and function during acute kidney injury. Kidney Int 83(1):72–83
Xu F, Papanayotou I, Putt DA, Wang J, Lash LH (2008) Role of mitochondrial dysfunction in cellular responses to S-(1,2-dichlorovinyl)-l-cysteine in primary cultures of human proximal tubular cells. Biochem Pharmacol 76(4):552–567
Lan R, Geng H, Singha PK, Saikumar P, Bottinger EP, Weinberg JM et al (2016) Mitochondrial pathology and glycolytic shift during proximal tubule atrophy after ischemic AKI. J Am Soc Nephrol JASN 27(11):3356–3367
Conjard-Duplany A, Martin M, Guitton J, Baverel G, Ferrier B (2001) Gluconeogenesis from glutamine and lactate in the isolated humanrenal proximal tubule: longitudinal heterogeneity and lack of response to adrenaline. Biochem J. https://doi.org/10.1042/0264-6021:3600371
Curthoys NP, Gstraunthaler G (2014) pH-responsive, gluconeogenic renal epithelial LLC-PK1-FBPase+cells: a versatile in vitro model to study renal proximal tubule metabolism and function. Am J Physiol Renal Physiol 307(1):F1–F11
De la Fuente IM, Cortés JM, Valero E, Desroches M, Rodrigues S, Malaina I et al (2014) On the dynamics of the adenylate energy system: homeorhesis vs homeostasis. PLoS ONE 9(10):e108676
Sumayao R Jr, Newsholme P, McMorrow T (2018) The role of cystinosin in the intermediary thiol metabolism and redox homeostasis in kidney proximal tubular Cells. Antioxidants (Basel, Switzerland) 7(12):179
Jozefczak M, Remans T, Vangronsveld J, Cuypers A (2012) Glutathione is a key player in metal-induced oxidative stress defenses. Int J Mol Sci 13(3):3145–3175
Ayala A, Muñoz MF, Argüelles S (2014) Lipid peroxidation: production, metabolism, and signaling mechanisms of malondialdehyde and 4-hydroxy-2-nonenal. Oxid Med Cell Longev. https://doi.org/10.1155/2014/360438
Crean D, Bellwon P, Aschauer L, Limonciel A, Moenks K, Hewitt P et al (2015) Development of an in vitro renal epithelial disease state model for xenobiotic toxicity testing. Toxicol In Vitro 30(1):128–137
Lash LH, Putt DA, Hueni SE, Cao W, Xu F, Kulidjian SJ et al (2002) Cellular energetics and glutathione status in NRK-52E cells: toxicological implications. Biochem Pharmacol 64(10):1533–1546
Long KR, Shipman KE, Rbaibi Y, Menshikova EV, Ritov VB, Eshbach ML et al (2017) Proximal tubule apical endocytosis is modulated by fluid shear stress via an mTOR-dependent pathway. Mol Biol Cell 28(19):2508–2517
Winther JR, Thorpe C (2014) Quantification of thiols and disulfides. Biochem Biophys Acta 1840(2):838–846
Cristóbal-García M, García-Arroyo FE, Tapia E, Osorio H, Arellano-Buendía AS, Madero M et al (2015) Renal oxidative stress induced by long-term hyperuricemia alters mitochondrial function and maintains systemic hypertension. Oxid Med Cell Longev. https://doi.org/10.1155/2015/535686
Funding
This study was funded from the Slovenian Research Agency (Grant Numbers: P3-0036, L4-1843), and from the University Medical Centre Maribor, Grant Number: IRP 2018/01-07.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Mihevc, M., Petreski, T., Maver, U. et al. Renal proximal tubular epithelial cells: review of isolation, characterization, and culturing techniques. Mol Biol Rep 47, 9865–9882 (2020). https://doi.org/10.1007/s11033-020-05977-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11033-020-05977-4