
Abstract
Oral lichen planus (OLP) is a potentially malignant oral lesion that may transform into oral squamous cell carcinoma (OSCC). The purpose of this study was to assess the level of expression of MAPK/ERK1/2 gene, and microRNA (miR)-603, 4301, 8485, and 4731 in the MAPK signaling pathway in OLP and OSCC lesions. This case–control study evaluated 26 OSCC, 20 OLP and 20 healthy control tissue specimens. After RNA extraction, the respective miRNA and MAPK/ERK1/2 mRNA levels were assessed by quantitative reverse transcription polymerase chain reaction (RT-PCR). Significant upregulation of MAPK/ERK1/2 gene was noted in the OLP and OSCC specimens compared with healthy controls (p < 0.001). The expression level of miR-4731 was significantly lower in the OLP and OSCC specimens than in the healthy specimens (p < 0.001). The expression of MiR-603 was the lowest in OLP, followed by OSCC and then the control group (p < 0.001). No significant difference was found in miR-4801 levels between OSCC and OLP specimens compared with healthy controls (p = 0.43 and p = 0.86, respectively). In addition, a non-significant decrease in miR-8485 levels was noted in the OSCC and OLP specimens compared with healthy controls (p = 0.98 and p = 0.61, respectively). A significant decrease in level of miR-603 was noted in OLP compared with OSCC group (p < 0.001). The miR-4801 and miR-8485 expression levels were directly correlated with MAPK/ERK1/2 mRNA expression (p = 0.01). Higher expression level of MAPK/ERK1/2, miR-603, miR-4801, and miR-4731, and lower expression level of miR-8485 were correlated with significantly lower overall survival rate in OSCC patients. The increased expression of MAPK/ERK1/2 and decreased expression of miR-603 and miR-4731 are associated with greater risk of OLP malignant transformation and poor histopathological characteristics of OSCC.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Oral cancer is the sixth most common cancer worldwide. Squamous cell carcinoma (SCC) is the most common oral cancer, accounting for about 6% of all cancers [1]. Over the past few decades, the 5-year survival rate of SCC remained below 50% despite the advances in its diagnosis and treatment [2]. In many cases, a precancerous lesion transforms into oral cancer. Oral precancerous lesions require special attention because of their tendency for malignant transformation. Early diagnosis of cancerous and precancerous oral lesions leads to better therapeutic outcomes, higher survival rate and lower mortality [3]. Research is ongoing to find potential biomarkers for detection of malignant transformation of oral lesions and to achieve an effective approach to diagnosis and management of such conditions [4].
Oral lichen planus (OLP) is a chronic autoimmune disease, reported by the World Health Organization (WHO) as a potentially malignant oral lesion. Regular follow-ups are strongly recommended for these patients [5]. The annual risk of cancer in patients with OLP is 100 times the rate in normal oral mucosa [6]. The prevalence of OLP is 2% in the general population, and 25% of OLP patients only present oral lesions; therefore, the increased risk of cancer should be carefully considered in such patients [7].
Lifestyle, environmental factors, and genetic predisposition are the three main factors that affect the development and progression of malignant and premalignant lesions. The involved genetic factors include the inability to detect carcinogens or procarcinogens, impaired DNA repair, and polymorphism of various genes that have been identified as important risk factors for the occurrence of SCC [8]. Development of malignancy leads to impairment of several signaling pathways and the consequent overexpression of some genes as well as impaired differentiation, and apoptosis of cells. The mitogen-activated protein kinase (MAPK) is among the signaling pathways affected by malignancies. The series of successive protein kinases are activated in this pathway in cell response to different mitogens, osmotic stress, thermal shock and inflammatory cytokines, resulting in regulation of cell proliferation, differentiation, survival and apoptosis [9].
Several studies have confirmed that dysregulation of this pathway is associated with the occurrence of various cancers [10, 11]. Elevated expression of extracellular signal-regulated protein kinases 1 and 2 (MAPK/ERK1/2) as the final products of the MAPK pathway has been reported in esophageal cancer, and its relationship with increased invasive serous carcinoma, lymphadenopathy and metastasis has been confirmed [12]. Inhibition of this pathway by increasing the expression of genes such as enhancer-binding protein (EBP), and trefoil factor 1 (TFF1) increases the tumor suppressor effects [13]. Genes, mRNAs, microRNAs (miRNAs), and proteins play a role in each signaling pathway. To date, 10 active miRNAs have been recognized that regulate the MAPK pathway. The miRNAs are a group of non-protein coding RNAs that regulate the expression of targeted mRNAs post-transcriptionally [14]. They play a role in regulating the biological processes such as the cell cycle, and differentiation, metabolism and aging of cells. Due to the ability to regulate gene expression, the miRNAs can act as oncogenes or tumor suppressor genes (TSGs) [15]. Dysregulation of miRNAs has been confirmed in a variety of cancer types, and is correlated with higher incidence of cancer, drug resistance, and metastasis [14]. Several miRNAs such as miR-125b [16], miR-27b [17], miR-137 [18], miR-146a [19], miR-138 [20], miR-155 [21] and miR-203 [22] are involved in the pathogenesis of OLP and its malignant transformation.
Therefore, the aim of this study was to investigate the level of expression of MAPK/ERK1/2 gene (as the final product of the cascade) and miR-603, 4301, 8485 and 4731 in the MAPK signaling pathway in oral SCC (OSCC) and OLP lesions to identify their role in malignant transformation of OLP into OSCC.
Materials and methods
Patients and tissue specimens
In this case–control study, the medical records of OSCC patients were retrieved from the archives of the Iran National Tumor Bank of Cancer Institute in Imam Khomeini Hospital, affiliated to Tehran University of Medical Sciences. The protocol of this study was approved by the TUMS Committee of Ethics with the number (code) of IR.TUMS.DENTISTRY.REC.1397.110. All patients willingly signed informed consent forms prior to participation in this study. Fresh frozen specimens of the tumor and normal adjacent tissue were collected from 26 OSCC patients (based on the McNemar’s test), who had not undergone treatments such as chemotherapy and radiotherapy prior to surgery. The patients were diagnosed with OSCC based on histopathological examination. All patients in this study underwent surgical operation and their histopathological characteristics including the size and grade of tumor, presence of necrosis, lymphovascular and perineural invasion and clinical tumor/node/metastasis (TNM) staging, as well as their 3-year survival rate were recorded. Information regarding their smoking status, alcohol consumption and family history was also obtained via an interview (Table 1). Patients with a history of other malignancies or chronic or acute inflammatory and/or infectious diseases were excluded. OLP specimens were collected from 20 patients referred to the Department of Oral and Maxillofacial Medicine at TUMS. The patients were clinically diagnosed with OLP (bilateral presence of reticular or papular lesions) and did not have any systemic disease or malignancy. They did not report systemic or topical use of medications, and did not have lichenoid reactions. Presence of OLP was histopathologically confirmed according to the WHO modified criteria for OLP [14]. None of the OLP specimens showed tissue dysplasia.
In addition, 20 healthy oral mucosal specimens (with no inflammation) were obtained from patients who underwent surgical procedures for other purposes such as surgical extraction of impacted third molars or frenectomy in the Department of Oral and Maxillofacial Medicine at TUMS. Healthy controls were matched with patient groups in terms of age and sex. Subsequently, the specimens were transferred to the Cancer Institute for RNA extraction and polymerase chain reaction (PCR).
MicroRNA selection
We examined four different algorithms to identify the miRNAs that target and regulate the mRNA translation of MAPK: TargetScan (http://www.targetscan.org/cgi-bin/targetscan/vert_70), miRDB (http://mirdb.org/cgi-bin/search.cgi), miR.org (http://www.miR.org/miR/searchGenes.do), and Diana microT (http://diana.imis.athena-innovation.gr/DianaTools/) (3). Accordingly, four miRNAs namely miR-603, miR-4301, miR-8485 and miR-4731 were identified.
Tissue RNA extraction
The tissue was first crushed in a mortar. Next 1000 µL of TRIzol (TRI Reagent Sigma Aldrich T9424) was poured into a 1.5-mL RNase- and DNase-free Eppendorf microtube, and the wrapped tissue was then added to the microtube. The microtube was vortexed and shaken for 15 s, and then 500 µL of chloroform was added and centrifuged at 12,000 rpm for 15 min at 4 °C. The supernatant was transferred to another tube and 500 µL of isopropanol was also added to it. The mixture was then centrifuged at 8000 rpm for 15 min at 4 °C. Then 1000 µL of 70% ethanol was added and the previous step was repeated. After drying, 50–100 µL of nuclease-free water was added to the microtube. Then, the RNA yield was determined using ND2000 NanoDrop. The microtube containing the RNA was stored at − 80 °C.
Synthesis of cDNA
The cDNA synthesis (601-005, Gene All, Seoul, South Korea) for RNA and miRNA was performed using the HyperScript™ First Strand Synthesis kit and the Pars-zhengan kit according to the manufacturer’s instructions. The primers were prepared and kept at − 20 °C.
Real-time PCR
According to the protocol, the real-time PCR strips and then the primers were added to the samples. The reaction mixture was first grouped into Nunc NucleoLink/TopYield Frame (Cat. N. 249182) RT-PCR, and each cycle was repeated twice to check for errors. For the negative control (NTC), all reaction materials were added to the strips except for the cDNA. The strips were then placed in Exicycler™ 96—Bioneer device according to the program. The real-time PCR cycling conditions included a preliminary activation step at 95 °C for 2 min followed by 40 amplification cycles each set as denaturation at 95 °C for 15 s and annealing at 60 °C for 30 s.
Table 2 presents the sequence of primers for the gene and miRNAs.
The melting curve analysis was performed to ensure specific amplification of the target miRNA. The threshold cycles (CT) for the target miRNAs and the spiked-in control were determined for each sample. The CT values of MAPK/ERK1/2 were normalized relative to the CT value of beta-actin as a housekeeping gene, and the CT value of miR-603, miR-4731, miR4801 and miR-8485 was normalized relative to the CT value of U6 in all groups and their relative levels were calculated using the 2−ΔΔCt method. All real-time PCR measurements were performed in duplicate.
Statistical analysis
Data were analyzed using Statistical Package for Social Sciences version 23 (SPSS; Chicago, IL, USA). Pairwise comparisons were performed using independent-sample t test and the Mann–Whitney U test. The non-parametric Kruskal–Wallis test for K independent samples was used for the comparison of more than two groups. The correlation between the variables was analyzed using the Spearman’s correlation coefficient. The association between the overall survival rate of OSCC patients and the expression level of gene and miRNAs was evaluated using the Kaplan–Meier method and the log rank test. Data were expressed as mean ± standard error of the mean (SEM). p value < 0.05 was considered statistically significant.
Code availability
The obtained data and computer codes in this study are available in the Iran National Tumor Bank founded by the Cancer Institute of Tehran University of Medical Sciences for Cancer Research (Iran).
Results
Twenty-six OSCC patients, 20 OLP patients and 20 healthy controls were evaluated in this study. The mean age of OSCC patients, OLP patients and healthy controls was 63.5 ± 16.2, 59.5 ± 14.8 and 52.5 ± 13.1 years, respectively. Of all, 61.6% of OSCC patients, 40% of OLP patients and 35% of healthy controls were male (Table 1). OLP patients had clinical presentation of atrophic or erosive subtype.
MAPK/ERK1/2 gene expression was upregulated in the OLP and OSCC specimens
The level of MAPK/ERK1/2–mRNA expression in OLP and OSCC specimens was significantly higher than that in healthy specimens (p < 0.001).
In addition, the expression of this gene in OLP specimens was significantly higher than that in OSCC specimens (p < 0.001). The expression of this gene did not have any significant correlation with the stage or the grade of tumor, or lymphovascular or perineural involvement in OSCC patients; however, we found a significant correlation between the level of MAPK/ERK1/2 mRNA expression and tumor necrosis in OSCC specimens (p < 0.05, Table 3).
The miR-603 expression was downregulated in the OLP and OSCC specimens
The expression level of miR-603 in OLP and OSCC specimens was significantly lower than that in healthy specimens (p < 0.001). In addition, the expression level of miR-603 in the OLP specimens was significantly lower than that in the OSCC specimens (p < 0.001, Table 3). The low expression level of this miRNA was significantly associated with a lower survival rate in OSCC patients (p < 0.05).
The miR- 4731 expression was downregulated in the OLP and OSCC specimens
The expression level of miR-4731 in the OLP and OSCC specimens was significantly lower than that in healthy specimens (p < 0.001). Although the expression level of miR-4731 was higher in OLP than OSCC specimens, this difference was not significant (p = 0.065). The low expression level of miR-4731 had a significant association with higher stage of disease and tumor necrosis, as well as the presence of familial history of oral cancer in patients (p < 0.05, Table 3).
The miR-4801 expression was upregulated in OSCC specimens
The expression level of miR-4801 was higher in the OSCC specimens in comparison with healthy specimens, although this difference was not statistically significant (p = 0.43). A similar finding was observed when comparing OLP and healthy specimens (p = 0.86, Table 3). We found no significant relationship between miR-4801 expression and clinical or histopathological characteristics of OSCC (p > 0.05).
The miR-8485 expression was downregulated in OSCC and OLP specimens
The expression levels of miR-8485 were not significantly lower in the OLP and OSCC specimens when compared with healthy specimens (p = 0.98 and 0.61, respectively). Moreover, there was no significant difference in the expression level of miR-8485 between the OSCC and OLP specimens (p = 0.48, Table 3). The miR-8485 was significantly upregulated in OSCC tumor specimens with vascular invasion (p < 0.05, Table 1). In OSCC patients, none of the variables showed a significant relationship with age, gender, site of primary tumor, grade of tumor and lymphatic or perineural involvement.
Correlation between MAPK/ERK1/2 mRNA expression and miR-603, miR-4301, miR-8485, and miR-4731 in OSCC patients
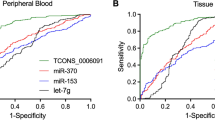
The miR-4801 (r = 0.570, p = 0.01) and miR-8485 (r = 0.472, p = 0.03) expression levels were directly correlated with MAPK/ERK1/2 mRNA expression. There was no significant relationship between miR-603 and miR-4731 with the expression level of MAPK/ERK1/2 mRNA (Fig. 1). To assess the effect of MAPK/ERK1/2, miR-603, miR-4801, miR-8485, and miR-4731 expression levels in tumor specimens on prognosis of OSCC, the 3-year survival rate of patients was analyzed. For this purpose, the patients were categorized into high and low expression level groups according to the median expression levels (after log-transformation) for the gene and miRNAs. As indicated in Fig. 2, the Kaplan–Meier survival curve analysis and the log rank test revealed that higher expression levels of MAPK/ERK1/2 (log rank = 13.98, p < 0.001), miR-603 (log rank = 6.27, p = 0.01), miR-4801 (log rank = 16.74, p < 0.001), and miR-4731 (log rank = 8.42, p = 0.004) were associated with significantly lower overall survival rate. Inversely, higher expression level of miR-8485 was associated with a significant increase in the survival rate of OSCC patients (log rank = 12.65, p < 0.001).

Correlation between MAPK/ERK1/2 mRNA expression and miR-603, miR-4801, miR-4731 and miR-8485 levels in OSCC patients. Data are expressed as mean ± SE. p value < 0.05 considered significant

Kaplan–Meier survival curve analysis for different expression levels of MAPK/ERK1/2, miR-603, miR-4301, miR-8485, and miR-4731 in the OSCC patients. The higher expression level of MAPK/ERK1/2, miR-603, miR- 4301 and miR-4731 and lower expression level of miR-8485 was found to serve as negative predictors of overall survival rate
Discussion
In this study, we examined the role of miR-603, miR-4301, miR-8485, and miR-4731 in regulation of MAPK-ERK1/2 expression in patients with OLP and OSCC. We believe that this study is the first to report that miR-603 and miR-4731 serve as tumor suppressors in OSCC. We also demonstrated that MAPK/ERK1/2 was highly overexpressed by OSCC cells, and decreased expression or no expression of miR-603 and miR-4731 contribute to upregulation of MAPK/ERK1/2. Moreover, we found that MAPK/ERK1/2 and miR-603 are important predictive factors for malignant transformation of OLP to OSCC.
The role of competing endogenous RNA (ceRNA) in the pathogenesis of OSCC has not been well understood [23]. Overexpression and underexpression of several miRNAs have been identified so far in oral and laryngeal carcinomas [24,25,26].
The MAPK signaling pathway possesses various cascades. There are various MAPKs based on the active cascade: p38/stress-activated protein kinases (SAPKs), MAPK/ERK1/2, extracellular-signal-regulated kinases (ERK5), and Jun amino-terminal kinases (JNKs) [9].
We demonstrated that expression of MAPK/ERK1/2 gene was significantly higher in OSCC and OLP tissue specimens compared with the healthy control specimens. Various studies have shown overexpression of various components of this cascade in development of various cancers [10,11,12,13].
Evidence shows increased expression of epidermal growth factor receptor and MAPK/ERK1/2 in esophageal carcinoma and its association with increased lymph node metastasis. Researchers suggested that ERK/EGFR can be used as a prognostic marker in esophageal SCC [12]. Increased expression of MAPK/ERK1/2 by vascular endothelial growth factor receptor followed by increased angiogenesis and conversion of dendritic cells to endothelial-like cells have also been confirmed in patients with esophageal carcinoma [27]. Another study reported Raf1, MEK1/2 overexpression in all osteosarcoma specimens and sarcoma cell lines. They showed a reduction in proliferation of cancer cells by MEK-inhibitor and MAPK pathway inhibition [28]. Decreased proliferation of gastric cancer cells has also been reported following the use of MAPK pathway inhibitors by inducing the tumor suppressor genes [13]. In another study, K-RAS-activating mutations were reported in 20% of all cancers and 40% of colorectal cancers [10]. Overexpression of BRAF and K-RAS genes has been confirmed in ovarian cancer [11]. Based on our results, the increase in MAPK/ERK1/2 expression seems to be an effective prognostic marker for higher incidence and poorer prognosis of OSCC.
Increased expression of MAPK/ERK1/2 gene in OLP compared with SCC specimens may indicate an increase in extracellular stimuli such as mitogens, inflammatory cytokines, and growth factors in untreated precancerous lesions, increasing the risk of malignant transformation. However, these stimuli somewhat decrease following the occurrence of cancer and subsequent morphological changes in cells. The role of some miRNAs in regulating the MAPK signaling in SCC has been previously studied. For example, underexpression of miR-125 b-1 can effectively increase the incidence of head and neck SCC by increasing the expression of ERK [29]. The present study highlighted the role of four miRNAs, which had not been investigated in regulation of MAPK/ERK1 pathway in OSCC and OLP.
We found that the expression level of miR-603 was the highest in healthy tissue specimens. Decreased expression of this miRNA can increase the mortality rate of SCC patients. Accordingly, this miRNA can play a TSG role in oral SCC. It is noteworthy that the minimum expression level of this miRNA was noted in OLP patients, indicating that miR-603 is a strong marker for malignant transformation of precancerous lesions, and is likely to slightly increase after the onset of cancer. Lower levels of miR-603 in OLP can be associated with higher rate of inflammation, which probably leads to malignant transformation of this lesion in a short time. Similar to our study, two other studies reported a significant decrease in miRNA-603 in triple negative breast cancer (TNBC) and vaginal cancer [15, 30]. Decreasing the expression of this miRNA by overexpression of eukaryotic elongation factor 2 kinase (eEF2K) led to tumorigenesis, tumor progression, drug resistance, and poorer prognosis in TNBC patients [15]. The abovementioned two studies also confirmed the TSG role of miRNA-603. However, another study discussed that increased expression of miR-603 in osteosarcoma patients suggests its oncogenic role [31].
We also found lower expression of miR-4731 in OLP and SCC patients compared with healthy controls; this expression was the lowest in SCC patients. These results also confirm the TSG role of this miRNA. Some studies conducted in 2015 and 2016 confirmed the role of miR-4731 as TSG in melanoma. They showed that increased expression of this miRNA had a significant relationship with lower tumor stage [32, 33]. Similar to our study, another study demonstrated underexpression of miR-4731 and overexpression of K-Ras in the MAPK signaling pathway in patients with colorectal cancer [34].
In the present study, the expression levels of miR-4801 and miR-8485 were not significantly different in the three groups. However, miR-4801 showed the highest level of expression in SCC while miR-8485 showed the highest level of expression in healthy specimens, which somewhat confirmed the oncogenic and TSG role of these miRNAs, respectively. To the best of the authors’ knowledge, no previous study has evaluated the role of these two miRNAs in development of precancerous and cancerous lesions, but several studies reported the role of miR-8485 in development of neurodegenerative diseases and heart failure [23, 35, 36].
In this study, downregulation of 8485, 4731 and 603 miRNAs and overexpression of MAPK/ERK1/2 gene in both OLP and SCC specimens compared with healthy controls confirmed the premalignant nature of OLP. An interesting finding of this study was the significant increase in MAPK/ERK1/2 gene expression and the significant decrease in miR-603 expression in OLP specimens compared with SCC, which indicate their more important role in malignant transformation of precancerous lesions compared with other miRNAs evaluated in this study. Thus, they can be effectively used for monitoring and prediction of the risk of malignant transformation of OLP to SCC. However, larger cohorts are recommended to validate our findings and confirm the exact values of expression of miRNAs involved in malignant transformation of OLP.
Future studies are also required on other miRNAs with possibly important roles in malignant transformation of OLP to OSSC. Moreover, the role of other components of the MAPK signaling pathway in other oral premalignant and dysplastic lesions and therapeutic strategies targeting the MAPK signaling pathway components, including MAPK/ERK1/2 by miR-4731 and miR-603 in patients with OSCC should be evaluated in further investigations.
Conclusion
The increased expression of MAPK/ERK1/2 and decreased expression of miR-603 and miR-4731 are associated with greater risk of OLP malignant transformation and poor histopathological characteristics of OSCC.
References
Najafi S, Gholizadeh N, Manifar S, Rajabzadeh S, Kharazi FM (2015) Salivary antioxidant level in oral squamous cell carcinoma. Iran J Blood Cancer 7:57–60
Gholizadeh N, Razavi HE, Haftkhani GJ, Sheykhbahaei N (2019) Predictive factors of survival rate in oral squamous cell carcinoma: a retrospective study in Iran. J Contemp Med Sci 5:101–105
Agha-Hosseini F, Sheykhbahaei N, SadrZadeh-Afshar M (2016) Evaluation of potential risk factors that contribute to malignant transformation of oral lichen planus: a literature review. J Contemp Dent Pract 17:692–701
Rupakar P, Kureshi A, Balar A, Khatri M, Parmar M, Pujara P et al (2016) Estimation of serum B2-microglobulin in oral precancerous lesions and oral squamous cell carcinoma. Natl J Integr Res Med 7:51–55
Aghbari SMH, Abushouk AI, Attia A, Elmaraezy A, Menshawy A, Ahmed MS et al (2017) Malignant transformation of oral lichen planus and oral lichenoid lesions: a meta-analysis of 20095 patient data. Oral Oncol 68:92–102
Van der Waal I (2014) Oral potentially malignant disorders: is malignant transformation predictable and preventable? Med Oral Patol Oral Cir Bucal 19:e386
Gholizadeh N, Poorfar HK, TaghaviZenouz A, Vatandoost M, Mehdipour M (2015) Comparison of serum autoantibodies to desmogleins I, III in patients with oral lichen planus and healthy controls. Iran J Pathol 10:136
Kumar SS, Zain RB (2018) Aetiology and risk factors for oral cancer–a brief overview. Ann Dent Univ Malaya 11:41–50
Morrison DK (2012) MAP kinase pathways. Cold Spring Harb Perspect Biol 4:a011254
Pierro C, Zhang X, Kankeu C, Trebak M, Bootman MD, Roderick HL (2018) Oncogenic KRAS suppresses store-operated Ca2+ entry and ICRAC through ERK pathway-dependent remodelling of STIM expression in colorectal cancer cell lines. Cell Calcium 72:70–80
Mayr D, Hirschmann A, Löhrs U, Diebold J (2006) KRAS and BRAF mutations in ovarian tumors: a comprehensive study of invasive carcinomas, borderline tumors and extraovarian implants. Gynecol Oncol 103:883–887
Cui X, Li S, Li T, Pang X, Zhang S, Jin J et al (2014) Significance of elevated ERK expression and its positive correlation with EGFR in Kazakh patients with esophageal squamous cell carcinoma. Int J Clin Exp Pathol 7:2382
Regalo G, Resende C, Wen X, Gomes B, Durães C, Seruca R et al (2010) C/EBPα expression is associated with homeostasis of the gastric epithelium and with gastric carcinogenesis. Lab Investig 90:1132
Pipan V, Zorc M, Kunej T (2015) MicroRNA polymorphisms in cancer: a literature analysis. Cancers (Basel) 7:1806–1814
Bayraktar R, Pichler M, Kanlikilicer P, Ivan C, Bayraktar E, Kahraman N et al (2017) MicroRNA 603 acts as a tumor suppressor and inhibits triple-negative breast cancer tumorigenesis by targeting elongation factor 2 kinase. Oncotarget 8:11641
Wang J, Luo H, Xiao Y, Wang L (2016) miR-125b inhibits keratinocyte proliferation and promotes keratinocyte apoptosis in oral lichen planus by targeting MMP-2 expression through PI3 K/Akt/mTOR pathway. Biomed Pharmacother 80:373–380
Aghbari SM, Zayed SO, Shaker OG, Abushouk AI (2019) Evaluating the role of tissue micro RNA-27b as a diagnostic marker for oral lichen planus and possible correlation with CD 8. J Oral Pathol Med 48:68–73
Aghbari SMH, Abushouk AI, Shakir OG, Zayed SO, Attia A (2018) Correlation between tissue expression of microRNA-137 and CD8 in oral lichen planus. Clin Oral Investig 22:1463–1467
Ahmadi-Motamayel F, Bayat Z, Hajilooi M, Shahryar-Hesami S, Mahdavinezhad A, Samie L et al (2017) Evaluation of the miRNA-146a and miRNA-155 expression levels in patients with oral lichen planus. Iran J Immunol 14:316–324
Ghallab NA, Kasem RF, El-Ghani SFA, Shaker OG (2017) Gene expression of miRNA-138 and cyclin D1 in oral lichen planus. Clin Oral Investig 21:2481–2491
Tao Y, Ai R, Hao Y, Jiang L, Dan H, Ji N et al (2019) Role of miR-155 in immune regulation and its relevance in oral lichen planus. Exp Ther Med 17:575–586
Danielsson K, Wahlin Y-B, Gu X, Boldrup L, Nylander K (2012) Altered expression of miR-21, miR-125b, and miR-203 indicates a role for these microRNAs in oral lichen planus. J Oral Pathol Med 41:90–95
Wang G, Zheng X, Zheng Y, Cao R, Zhang M, Sun Y et al (2019) Construction and analysis of the lncRNA-miRNA-mRNA network based on competitive endogenous RNA reveals functional genes in heart failure. Mol Med Rep 19:994–1003
Cheng J, Chen J, Wang Z, Yu D, Zu Y (2017) The functional role of microRNAs in laryngeal carcinoma. Open Life Sci 12:460–464
Ayaz L, Görür A, Yaroğlu HY, Özcan C, Tamer L (2013) Differential expression of microRNAs in plasma of patients with laryngeal squamous cell carcinoma: potential early-detection markers for laryngeal squamous cell carcinoma. J Cancer Res Clin Oncol 139:1499–1506
Scapoli L, Palmieri A, Muzio LL, Pezzetti F, Rubini C, Girardi A et al (2010) MicroRNA expression profiling of oral carcinoma identifies new markers of tumor progression. Int J Immunopathol Pharmacol 23:1229–1234
Lu J, Zhao J, Liu K, Zhao J, Yang H, Huang Y et al (2010) MAPK/ERK1/2 signaling mediates endothelial-like differentiation of immature DCs in the microenvironment of esophageal squamous cell carcinoma. Cell Mol Life Sci 67:2091–2106
Sasaki K, Hitora T, Nakamura O, Kono R, Yamamoto T (2011) The role of MAPK pathway in bone and soft tissue tumors. Anticancer Res 31:549–553
Nakanishi H, Taccioli C, Palatini J, Fernandez-Cymering C, Cui R, Kim T et al (2014) Loss of miR-125b-1 contributes to head and neck cancer development by dysregulating TACSTD2 and MAPK pathway. Oncogene 33:702
Yang X, Wu X (2016) miRNA expression profile of vulvar squamous cell carcinoma and identification of the oncogenic role of miR-590-5p. Oncol Rep 35:398–408
Ma C, Zhan C, Yuan H, Cui Y, Zhang Z (2016) MicroRNA-603 functions as an oncogene by suppressing BRCC2 protein translation in osteosarcoma. Oncol Rep 35:3257–3264
Stark MS, Klein K, Weide B, Haydu LE, Pflugfelder A, Tang YH et al (2015) The prognostic and predictive value of melanoma-related microRNAs using tissue and serum: a microRNA expression analysis. EBioMedicine 2:671–680
Stark MS, Tom LN, Boyle GM, Bonazzi VF, Soyer HP, Herington AC et al (2016) The ‘Melanoma-enriched’microRNA miR-4731-5p acts as a tumour suppressor. Oncotarget 7:49677
Hiraki M, Nishimura J, Takahashi H, Wu X, Takahashi Y, Miyo M et al (2015) Concurrent targeting of KRAS and AKT by MiR-4689 is a novel treatment against mutant KRAS colorectal cancer. Mol Ther-Nucleic Acids 4:e231
Fan Z, Chen X, Chen R (2014) Transcriptome-wide analysis of TDP-43 binding small RNAs identifies miR-NID1 (miR-8485), a novel miRNA that represses NRXN1 expression. Genomics 103:76–82
Kattimani Y, Veerappa AM (2018) Dysregulation of NRXN1 by mutant MIR8485 leads to calcium overload in pre-synapses inducing neurodegeneration in Multiple sclerosis. Mult Scler Relat Disord 22:153–156
Funding
This research received grant from deputy of research of Tehran University of Medical Science.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Gholizadeh, N., Emami Razavi, A., Mohammadpour, H. et al. Association of MAPK and its regulatory miRNAs (603, 4301, 8485, and 4731) with the malignant transformation of oral lichen planus. Mol Biol Rep 47, 1223–1232 (2020). https://doi.org/10.1007/s11033-019-05223-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11033-019-05223-6