
Abstract
Introduction
Rwanda stands out in East Africa with the lowest infant mortality ratio at 29 per 1000 live births. It also leads in gender equality on the African continent, ranking sixth globally according to the 2022 Global Gender Gap Report. This makes Rwanda an ideal case for studying the link between women's empowerment and infant mortality.
Method
This study aims to assess the impact of women's empowerment on infant mortality using data obtained from the Rwanda Demographic and Health Survey conducted in 2005, 2010, and 2015. A three-category women's empowerment index was created using the principal component analysis method. The statistical analysis employed in this study is multivariate binary logistic regression.
Results
Results demonstrate a significant impact of women's empowerment on reducing infant mortality, considering regional and residential inequalities, bio-demographic factors, and healthcare variables.
Conclusion
The findings contribute to existing literature and highlight the importance of empowering women to improve maternal and child health outcomes. Such empowerment not only enhances health but also supports sustainable development and social progress. Policymakers, healthcare providers, and organizations should prioritize investing in women's empowerment to achieve maternal and child health goals, as empowered women play a pivotal role in driving positive change for a healthier and more equitable society.
Significance
This study highlights the critical importance of women's empowerment in improving infant survival rates and promoting population health in Rwanda. The study is significant due to the country's low infant mortality rate and leading position in gender equality in Africa. By demonstrating the strong association between women's empowerment and infant mortality, the findings highlight the need for ongoing efforts to empower women and ensure equitable access to healthcare services for all. This research provides valuable insights that can inform policies and programs aimed at reducing infant mortality and enhancing the well-being of both women and children in Rwanda and similar contexts.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Infant mortality is a crucial indicator of child health and serves as a key measure of a country’s development level. Significant global progress has occurred, and the infant mortality rateFootnote 1 has substantially decreased worldwide (WHO, 2023; UN-DESA, 2022). It dropped from 143 per thousand in 1950 to 65 per thousand in 1990, further declining to 28 per thousand in 2021 (Fig. 1). Concurrently, despite the reduction in the annual number of infant deaths from 13.1 million in 1950 to 9.2 million in 1990 and further to 3.7 million in 2021, the fact that 3.7 million live births are still lost before reaching the age of 1 highlights the persistent challenge in this crucial area (UN-DESA, 2022). While the infant mortality rate and the number of infant deaths has decreased over time in the African region, the probability of a child dying in the first year of age was still most pronounced in the African Region, surpassing that in more developed countries by over elevenfold. Rwanda stands out as a prominent and distinctive country in the African region in this regard. Among all East African countries (EAC), Rwanda boasts the lowest infant mortality rate of 29 deaths per 1000 live births. Additionally, Rwanda is the sole country in the region to have achieved Millennium Development Goal 4, which specifically targets the reduction of child mortality (Kitua, 2007).

Trends of infant mortality rates (1950–2021). Source: UN-DESA 2022
Child mortality is influenced by a myriad of factors, including socioeconomic, biological, environmental, and behavioral elements (Mosley & Chen, 1984). Mosley and Chen’s 1984 framework, which integrates social and biological variables, combines methodologies from medical and social sciences. The framework suggests that infant mortality is influenced by various social, economic, and cultural factors through five sets of proximate variables. Maternal factors, including age, child sex, birth order, and interval, play a pivotal role. Environmental factors such as air quality, access to clean water, and toilet facilities also contribute significantly. Nutrient deficiency, spanning inadequate calorie, protein, and micronutrient intake, forms another critical dimension. Injury, arising from accidental or intentional causes, further impacts health outcomes. Lastly, personal illness treatment, encompassing preventive measures and medical interventions, completes the spectrum of factors shaping health dynamics.
According to Mosley and Chen’s framework, these proximate determinants directly contribute to the risk of morbidity and mortality among infants. The framework serves as a primary reference in this study, providing a comprehensive perspective on the factors influencing infant mortality.
One of the most crucial social factors influencing infant mortality and child health is women’s empowerment. Women’s empowerment is an important concept that pertains to the description of women’s abilities and capacities in the social transformation of their lives and communities (Kabeer, 1999). Studies by Malhotra & Schuler (2005) have established various dimensions used to measure women’s empowerment, including socio-cultural, legal, economic, familial/relational, psychological, and political dimensions. Indicators used to measure empowerment at the individual or family levels are classified into domestic decision-making, control over resources, and flexibility/autonomy of movement (World Economic Forum, 2022).
In Rwanda, women’s empowerment is crucial for accessing healthcare services, supported by policies such as free education and increased opportunities in various sectors like finance, politics, education, economy, healthcare, and aviation (Musonera & Heshmati, 2017).
The Global Gender Gap Index assesses the disparity between men and women across four key categories: economic participation and opportunity, educational attainment, health and survival, and political empowerment (World Economic Forum, 2022). According to the report, when evaluating the top 10 countries in terms of gender equality, Iceland ranks first with an overall gender gap of 91%, followed by other Scandinavian countries such as Finland (86%), Norway (%84.5). Rwanda included in the list in 6th place (81%). Rwanda stands out as a leading country in the African continent regarding gender equality, particularly due to its achievements in the field of political empowerment. Rwanda has made significant progress in enhancing women’s participation in politics and decision-making. However, there are still challenges in empowering women economically, primarily stemming from deeply ingrained negative social norms and cultural beliefs (Abbott et al., 2017).
The United Nations’ Sustainable Development Goal 3 emphasizes the importance of ensuring healthy lives and promoting well-being for individuals of all ages. This goal includes specific targets for reducing neonatal mortality to at least 12 deaths per 1000 live births and under-5 mortality to 25 deaths per 1000 live births by the year 2030. Although Rwanda has made significant progress in terms of early-age mortality, there is still work to be done in order to reach these ambitious targets. The ultimate aim is to decrease the under-5 mortality rate to the lowest possible level of 25 deaths per 1000 live births.
Women’s empowerment plays a crucial role in promoting the health and social development of families and societies (Boserup, 1970; Duflo 2012). The Sustainable Development Goals (SDGs) for 2030, including Goal 5, emphasize the significance of women’s empowerment for sustainable development, aiming to achieve gender equality and empower all women and girls (United Nations Economic Commission for Africa, 2015).
The negotiation of authority within the household and the empowerment of women have the potential to contribute to the reduction of mortality and fertility rates (Bongaarts, 2008). Research by Eswaran (2002) suggests that empowering women in the family can have a positive impact on these indicators.
The census data from India reveals that certain factors associated with women’s empowerment, such as female labor force participation and female education, are strongly correlated with lower fertility rates, reduced child mortality, and decreased gender discrimination in child mortality (Bloom et al., 2001; Kishor & Parasuraman, 1998).
These findings highlight the transformative potential of women’s empowerment in improving health outcomes and achieving sustainable development goals. By empowering women and promoting gender equality, societies can create positive impacts on the well-being of individuals and communities.
The active participation of women in household decision-making processes has been found to have a positive impact on accessing healthcare services, which can contribute to child survival in developing countries (Islam, 2017). When women are empowered and have autonomy, they are more likely to seek antenatal care, give birth in a health facility, and use modern contraceptive methods, leading to reductions in maternal and child mortality rates (Merrell & Blackstone, 2020; Yaya et al., 2018).
However, it is worth noting that many studies on infant mortality do not specifically focus on the role of women’s empowerment in child mortality (Hossain, 2015). This gap in research hinders our comprehensive understanding of how women’s empowerment directly influences child mortality outcomes. Nonetheless, existing evidence suggests that empowering women and enhancing their decision-making power within households and communities can have significant implications for maternal and child health.
By addressing women’s empowerment as a key factor in child mortality reduction efforts, policymakers and researchers can gain valuable insights into the multifaceted determinants of child survival and develop more targeted interventions to promote women’s empowerment and improve health outcomes (Brunson et al., 2009; Doan et al., 1990).
The main objective of the study is to investigate the influence of women’s empowerment on infant mortality in Rwanda, a country that ranks highly in the global gender gap index among African nations. To achieve this objective, the study utilizes the principal component analysis method to construct a women’s empowerment index. Subsequently, the association between women’s empowerment and infant mortality is analyzed, controlling for other relevant variables.
By employing the principal component analysis method, the study aims to capture the multidimensional nature of women’s empowerment by combining various indicators into a single index. This index serves as a proxy for measuring the level of women’s empowerment in Rwanda. The study then proceeds to examine the relationship between women’s empowerment and infant mortality, taking into account the potential influence of other factors.
This research design allows for a comprehensive assessment of the role of women’s empowerment in shaping infant mortality outcomes in Rwanda. By controlling for other variables, the study isolates and analyzes the association between women’s empowerment and infant mortality, providing valuable insights into the importance of empowering women in promoting child health and well-being.
Methodology and Data
Data Source
The study utilized data obtained from three main Standard Rwanda Demographic and Health Surveys (RDHS) conducted in 2005, 2010, and 2015. These surveys are nationally representative sample surveys. The National Institute of Statistics of Rwanda (NISR) conducted the Rwanda DHS Surveys as part of the global Demographic and Health Surveys project, which received support from the United States Agency for International Development (USAID) and technical assistance from the International Cooperation Fund (ICF International) (NISR, 2005, 2010, 2015).
All three Rwanda DHS surveys (RDHS 2005, RDHS 2010, and RDHS 2015) comprise two questionnaires: the household questionnaire and the individual questionnaire. The household questionnaire gathers information about all household members residing in the house and visitors who spent the previous night. It captures basic characteristics such as age, gender, education level, marital status, and details about the house they inhabit. Additionally, the household questionnaire facilitates the identification of women in the 15–49 age group, of reproductive age, who will undergo individual interviews. The individual questionnaire for the 15–49 age group of ever-married women addresses critical issues including child nutrition, family planning, fertility, pregnancy, contraceptive use, child’s health, breastfeeding, and the respondent’s background. In the birth history module of the individual questionnaire, the birth dates, including month and year, are recorded for each interviewed woman’s live births, along with death dates if applicable. This module is crucial for studying infant mortality. Table 1 displays the count of households interviewed, the number of individually interviewed ever-married women aged 15–49, and the count of children for whom information was collected from these women.
For the study, we merged three waves of the Rwanda DHS data set. Each wave utilized a weighted, multi-stage, stratified cluster sampling method, and the questionnaires used were very similar, with negligible differences in the questions askedFootnote 2. The pooling of these three surveys yielded a large and comprehensive data set, offering two significant advantages. Firstly, it provided a sufficient number of observations for the analysis, resulting in narrower confidence intervals and more accurate point estimates. This was particularly advantageous for analyzing infant deaths, which are rare events, as it allowed for the inclusion of information from a large number of observations. To address potential biases or errors stemming from variations in the number of observations across the surveys, weighting factors were applied. These weighting factors were derived from the equation \(1/\left( {a \times n_{c} /n_{T} } \right)\), where a represents the number of surveys, nc is the number of respondents for a particular survey, and nT is the total number of respondents across all surveys (Marriot et al., 2007).
Variables
The dependent variable in the analysis was the survival status of infants. The dependent variable is a dichotomous variable, with a value of “1” indicating non-survival and a value of “0” indicating survival. The study comprises 25,507 unweighted children as the number of observations.
Along with the women’s empowerment index, a range of bio-demographic, socio-economic, and health-care variables were included as independent variables in the analysis.
The measurement of women’s empowerment holds significance in this study as it serves as the main independent variable. In the existing literature, three dimensions of women’s empowerment have been identified: decision making (1), gender attitudes and beliefs (2), and human and social assets (3).
The variables associated with the decision making dimension include having the final say on one’s own healthcare, having the final say on making significant household purchases, having the final say on visiting family or relatives. The questions related to this topic in the questionnaire were phrased as follows: Who usually makes decisions about health care for yourself/Who usually makes decisions about making major household purchases?/ Who usually makes decisions about visits to your family, relatives and friends?. The response categories for the questions are respondent alone, respondent and husband (partner), respondent and other person, Husband (partner) alone, someone else. These five categories were consolidated into a two-category variable. The first three categories, which encompassed women’s participation, were combined into one category, while the other two categories were treated separately.
The variables related to gender attitudes and beliefs dimension include justifying going out without informing the husband, justifying neglecting children, justifying refusal of sex, justifying if the woman burns food. The questions pertaining to this topic were phrased as follows:
In your opinion, is a husband justified in hitting or beating his wife in the following situations:
If she goes out without telling him?
If she neglects the children?
If she refuses to have sex with him?
If she burns the food?
Response options were coded as ‘yes,’ ‘no,’ or ‘don’t know.’ ‘Don’t know’ answers were treated as missing values. Variable information was reverse-coded, implying that a woman recorded 1 if she replied negatively. This coding reflects both empowerment and an additional belief in the rightful role of gender.
The variables associated with the human and social assets dimension include women’s education level, women’s occupation, and age at first marriage. The women’s education level variable was recoded into “no education” and “other education levels”, the women’s occupation variable were recoded into “not working/agricultural sector” and “non agricultural sector”, and women’s age at first marriage were recoded into “under 18” and “18+” (Table 2).
Alongside the women’s empowerment index, a range of bio-demographic, socio-economic, and health-care variables were included as independent variables in the analysis. Bio-demographic variables included variables such as sex of the child, birth order, birth interval (< 24 months, > 24 months), and birth type (single, multiple). Socio-economic variables encompassed region (City of Kigali, South, West, North), place of residence (urban, rural), source of drinking water (improved sources, non-improved sources)Footnote 3 and frequency of reading newspapers and magazine (not at all, reading newspaper and magazine). Health-care related variables included the place of delivery (home, public health facility, private health facility). The number of observations and the percent distribution of independent variables are presented in Table 3.
Methods of Analysis
Creation of Women’s Empowerment Index: Pricincipal Component Analysis
Principal Components Analysis (PCA) was employed to construct the women’s empowerment index. PCA is a statistical technique that enables the summarization of information from a set of variables into a smaller set of mutually orthogonal components. The purpose of this technique is to reduce the number of variables that interact with each other and facilitate the assessment of their explanatory effects. By transforming the initial set of correlated variables into a smaller number of uncorrelated variables known as principal components, PCA aids in capturing the majority of the total variance in the model (Smith, 2006). In the study, PCA included 10 variables listed in Table 2.
Table 4 illustrates the data’s suitability for PCA. The Kaiser–Meyer–Olkin Measure of Sampling Adequacy serves as a metric indicating the proportion of variance in the variables potentially caused by underlying factors. Higher values, nearing 1.0, generally suggest that a factor analysis could be beneficial for the data. Bartlett’s test of sphericity evaluates the hypothesis that the correlation matrix is an identity matrix, implying that the variables are unrelated and unsuitable for structure detection. If the significance level is less than 0.05, it suggests that a factor analysis may be beneficial for the data.
The scree plot (Fig. 2) illustrates the principal component number in competition with the corresponding Eigenvalues, showcasing the Eigenvalues from largest to smallest. By examining the structure of the curve presented in the scree plot, a notable transition occurs after the third principal component, with subsequent components describing a minimal percentage of variability, nearly approaching zero. These components are deemed less crucial.

Scree plot for identifying the component number of the WE index
The component plot (Fig. 3) illustrates the classification of the women’s empowerment index into three primary categories: High women’s empowerment index, Medium women’s empowerment index, and Low women’s empowerment index, utilizing variables mentioned in the preceding section.

Component plot
The Women’s Empowerment Index, as depicted in Table 5, was categorized using the component matrix values obtained from PCA. Interpreting the values of the component matrix reveals that the lowest values indicate a high empowerment level, moderate values describe a medium empowerment level, and, conversely, the highest values suggest a low empowerment level.
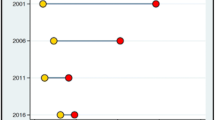
Figure 4 illustrates the trend of the women’s empowerment index across three DHS surveys conducted in Rwanda between 2005 and 2015. Over time, there is a notable increase in women’s empowerment, with the percentage of highly empowered women rising from 29 to 43%, and the percentage of low-empowered women decreasing from 33 to 23%.

Trend of women’s empowerment index (2005–2015)
Binary Logistic Regression Analysis
The study employed binary logistic regression as the method of analysis. The dependent variable in the analysis was the survival status of infants. Since the dependent variable is a dichotomous variable, with a value of “1” indicating non-survival and a value of “0” indicating survival, binary logistic regression was deemed appropriate for the analysis.
Binary logistic regression was employed in two models: a univariate model, where only the women’s empowerment variable, the primary independent variable, was analyzed independently, and a multivariate model, where other variables were controlled alongside the women’s empowerment index variable. The independent variables, recognized to be associated with infant mortality as documented in the literature and detailed in Table 3 in the preceding section, were collectively included in the multivariate model.
Results
Table 3 presents the percentage distribution of covariates according to the survival status of the infants. The covariates were grouped into three categories: bio-demographic, socio-economic, and health-care variables, along with the women’s empowerment index. Descriptive analysis results revealed a decline in infant mortality as women’s empowerment increased.
The data showed slightly higher infant mortality rates for male children compared to female children. Additionally, the percentage of infant deaths was higher for first births and higher-order births (6th and above). Women who had birth spacing of less than 24 months had a higher likelihood of experiencing infant deaths compared to those with birth spacing of more than 24 months. The analysis also indicated that multiple births had a higher proportion of infant deaths (21.4%) compared to single births (6.3%).
In terms of regions, the City of Kigali exhibited the lowest infant mortality, while the Northern region had the highest. Furthermore, infant mortality rates were higher in rural areas compared to urban areas. Infants from households using non-improved water sources had a higher percentage of infant deaths, possibly due to health risks associated with contaminated water, which could affect the health of both the mother and the infant. Women who did not read any newspapers or magazines had a higher proportion of infant deaths.
Additionally, giving birth at home increased the likelihood of experiencing infant deaths compared to births in a health facility.
To examine the association between the main independent variable of the study, the women’s empowerment index, and infant mortality, a univariate model was initially created (Table 6). Subsequently, a multivariate model was developed, incorporating control for other relevant variables (Table 7).
The findings indicate that women’s empowerment is statistically significantly associated with the risk of infant mortality, both in univariate and multivariate models. Using the high level of the women’s empowerment index as the reference category, the study found that infants born to women with a moderate level of empowerment have a 32% higher risk of mortality in the univariate model (OR = 1.32, 95% CI 1.16–1.51) and a 20% higher risk of mortality in the multivariate model (OR = 1.20, 95% CI 1.05–1.37). Infants born to women with a low level of empowerment have a 47% higher risk of mortality in the univariate model (OR = 1.47, 95% CI 1.29–1.68) and a 30% higher risk of mortality in the multivariate model (OR = 1.30, 95% CI 1.13–1.48). The analysis reveals that as the level of women’s empowerment decreases, the risk of infant mortality increases. even after controlling for other explanatory variables. This suggests that children of women with lower levels of empowerment are more susceptible to mortality risks (Tables 6 and 7).
When examining the bio-demographic variables, it was found that the gender of the infant and the birth interval had a statistically significant association with the risk of infant mortality. Specifically, female infants were associated with a 16% lower risk of mortality compared to male infants (OR = 0.84, 95% CI 0.76–0.93). The variable of birth order did not yield statistically significant results, although it is worth noting that infants with a birth order of 6 and above had a 12% higher risk of mortality (although not statistically significant). When the birth interval is longer than 24 months, there is a 42% reduction in the likelihood of infant mortality compared to shorter birth intervals (OR = 0.58, 95% CI 0.51–0.65). The variable related to birth types revealed that infants born as multiple births were at a higher risk of mortality compared to infants born in single births (OR = 4.61, 95% CI 3.77–5.65).
The socio-economic variables included in the analysis were region, place of residence, source of drinking water, and frequency of reading newspapers and magazine. The results showed that in comparison to the City of Kigali, which is the most developed region and the capital of the country, the South, West, North, and East regions exhibited higher risks of infant mortality, with the highest odds ratios observed in the North (OR = 1.74, 95% CI 1.27–2.37) and East (OR = 1.51, 95% CI 1.13–2.01) regions. Although the results are not statistically significant, the risk of infant mortality was found to be 13% higher in rural areas compared to urban areas (OR = 1.13, 95% CI 0.92–1.39). The source of drinking water variable did not have a statistically significant effect on the risk of infant mortality. The frequency of reading newspapers and magazines was found to be associated with infant mortality (OR = 0.79, 95% CI 0.68–0.91). The likelihood of infant mortality was higher among women who did not read newspapers and magazines at all.
The variable of place of delivery, included in the analysis as a health-care variable, showed statistically significant effects on the risk of infant mortality. Giving birth in a health institution was found to significantly reduce the risk of infant death compared to home deliveries. Specifically, in comparison to home deliveries, which serve as the reference category, the risk of infant death was 50% lower for births in a public health institution (OR = 0.50, 95% CI 0.44–0.56) and 68% lower for births in a private health institution (OR = 0.32, 95% CI 0.13–0.78).
Discussion
In this study, we explore the relationship between women’s empowerment and infant mortality, in the case of Rwanda, which stands out with a lower infant mortality rate compared to other countries in its African region and holds the sixth position globally in the Global Gender Gap index.
The results highlight the significance of empowered women in promoting child health and reducing infant deaths in the country. The strong correlation between women’s empowerment and child survival is evident in the ability and capacity of women to actively participate in household decision-making, contributing to a decline in infant mortality. As the important elements of women’s empowerment maternal education level and women’s occupation play essential role in declining infant mortality level because the children are more expected to have a higher possibility of survival due to access to all the basics needs for improving their lives (Schell et al., 2007). Elevating women’s involvement in decision-making processes, as well as their engagement in education and the labor force, will empower women and yield highly positive outcomes for their children.
Moreover, the study underscores the higher likelihood of infant deaths in rural areas compared to urban areas. Challenges in accessing healthcare services in rural regions contribute to this increased risk of mortality (Pierce et al., 2014). To address this disparity, it is crucial for the government to implement health extension programs that target the specific health needs of the rural population and bridge the gap between rural and urban areas. Sustaining and expanding policies such as training health community workers, who play a vital role in improving maternal and child health outcomes, is of utmost importance.
The study also reveals that high birth order and short birth intervals are associated with an increased risk of infant mortality. Addressing the unmet need for family planning is vital in reducing these risks. Furthermore, the place of delivery emerges as a significant determinant of infant mortality in Rwanda. Giving birth in healthcare facilities indicates the utilization of the health system, which is closely linked to crucial factors such as receiving prenatal and postnatal care for mothers and infants, as well as child vaccination. These findings emphasize the importance of accessing proper healthcare facilities during childbirth in order to decrease the risk of infant mortality.
In conclusion, the study findings strongly emphasize the significant link between women’s empowerment and infant mortality, highlighting the crucial importance of empowering women not only for their own well-being but also for the improved health and increased survival opportunities of their children.
The study was conducted using a cross-sectional survey data, restricting the analysis to the variables available in the dataset. Utilizing longitudinal survey data would offer enhanced opportunities to observe the evolution of women’s empowerment index components over time, incorporate a more comprehensive set of variables as control measures, and scrutinize the causal relationship between women’s empowerment and infant mortality.
Data Availability
The data that support the findings of this study are available and can be requested from the website of the DHS Program (https://dhsprogram.com/data/available-datasets.cfm).
Code Availability
Not applicable.
Notes
The infant mortality rate is the probability of a child born in a specific year or period dying before reaching the age of one, if subject to age-specific mortality rates of that period.
Improved sources comprise a piped into dwelling/yard/plot, public tap, tube well or borehole, protected well, protected spring, rain water. Non-improved sources include unprotected well, unprotected spring, tanker truch/car with tank, surface water and other sourves.
References
Abbott, P., Sapsford, R., & Binagwaho, A. (2017). Learning from success: How Rwanda achieved the millennium development goals for health. World Development, 92, 103–116.
Bloom, S. S., Wypij, D., & Das Gupta, M. (2001). Dimensions of women’s autonomy and the influence on maternal health care utilization in a north Indian city. Demography, 38, 67–78.
Bongaarts, J. (2008). Fertility transitions in developing countries: Progress or stagnation? Studies in Family Planning, 39(2), 105–110.
Boserup, E. (1970). Women’s role in economic development. George Allen and Unwin.
Brunson, E. K., Shell-Duncan, B., & Steele, M. (2009). Women’s autonomy and its relationship to children’s nutrition among the Rendille of Northern Kenya. Journal of Human Biology: The Official Journal of the Human Biology Association, 21(1), 55–64.
Doan, R. M., & Bisharat, L. (1990). Female autonomy and child nutritional status: The extended-family residential unit in Amman, Jordan. Social Science and Medicine, 31(7), 783–789.
Duflo, E. (2012). Women empowerment and economic development. Journal of Economic Literature, 50(4), 1051–1079.
Eswaran, M. (2002). The empowerment of women, fertility, and child mortality: Toward a theoretical analysis. Journal of Population Economics, 15(3), 433–454.
Hossain, B. (2015). Women empowerment and infant mortality in Bangladesh. Applied Economics, 47(51), 5534–5547.
Islam, R. M. (2017). Utilization of maternal health care services among indigenous women in Bangladesh: A study on the Mru Tribe. Women & Health, 57(1), 108–118.
Kabeer, N. (1999). Resources, agency, achievements: Reflections on the measurement of women’s empowerment. Development and Change, 30(3), 435–464.
Kishor, S., & Parasuraman, S. (1998). Mother’s employment and infant and child mortality in India: National Family Health Survey Subject Reports. International Institute for Population Sciences.
Kitua, A. Y. (2007). Health research agenda for East Africa in the new millennium: Looking ahead. Tanzania Journal of Health Research, 9(3), 147–153.
Malhotra, A., & Schuler, S. R. (2005). Women’s empowerment as a variable in international development. Measuring Empowerment: Cross-disciplinary Perspectives, 1(1), 71–88.
Marriott, B. M., Campbell, L., Hirsch, E., & Wilson, D. (2007). Preliminary data from demographic and health surveys on infant feeding in 20 developing countries. The Journal of Nutrition, 137(2), 518–523.
Merrell, L. K., & Blackstone, S. R. (2020). Women’s empowerment as a mitigating factor for improved antenatal care quality despite impact of 2014 Ebola outbreak in Guinea. International Journal of Environmental Research and Public Health, 17(21), 8172.
Mosley, W. H., & Chen, L. C. (1984). An analytical framework for the study of child survival in developing countries. Population and Development Review, 10, 25–45.
Musonera, A., & Heshmati, A. (2017). Measuring women’s empowerment in Rwanda. Studies on economic development and growth in selected African countries (pp. 11–39). Springer.
National Institute of Statistics Rwanda (NISR), Ministry of Health. (2005). Rwanda demography and health survey. Government of Rwanda.
National Institute of Statistics of Rwanda (NISR), Ministry of Health. (2010). Rwanda demography and health survey. Government of Rwanda.
National Institute of Statistics Rwanda (NISR), Ministry of Health. (2015). Rwanda demography and health survey. Government of Rwanda.
Pierce, H., Heaton, T. B., & Hoffmann, J. (2014). Increasing maternal health care use in Rwanda: Implications for child nutrition and survival (Vol. 107, pp. 61–67). Social Science & Medicine.
Schell, C. O., Reilly, M., Rosling, H., Peterson, S., & Mia Ekström, A. (2007). Socioeconomic determinants of infant mortality: A worldwide study of 152 low-, middle-, and high-income countries. Scandinavian Journal of Public Health, 35(3), 288–297.
Smith, L. I. (2006). A tutorial on principal components analysis. Wiley.
United Nations Economic Commission for Africa (2015). MDG Report 2015: Assessing progress in Africa toward the Millennium Development Goals. Addis Ababa, Ethiopia.
United Nations, Department of Economic and Social Affairs, Population Division–UN-DESA (2022). World population prospects 2022, Online Edition.
World Economic Forum. (2022). Global gender gap report 2022. World Economic Forum.
World Health Organization (WHO). (2023). World health statistics 2023: Monitoring health for the SDGS, sustainable development goals. World Health Organization.
Yaya, S., Uthman, O. A., Ekholuenetale, M., & Bishwajit, G. (2018). Women empowerment as an enabling factor of contraceptive use in sub-saharan Africa: A multilevel analysis of cross-sectional surveys of 32 countries. Reproductive Health, 15, 214. https://doi.org/10.1186/s12978-018-0658-5
Funding
The author(s) reported there is no funding associated with the work featured in this article.
Author information
Authors and Affiliations
Contributions
GN and MAE: Conceptualization, Formal analysis, Writing—original draft, Writing—review & editing.
Corresponding author
Ethics declarations
Conflict of interest
No potential conflict of interest was reported by the author(s).
Ethical Approval
This study adhered to ethical guidelines and principles for research involving human subjects. This study is a secondary analysis of the RDHS data. The RDHS data used in this study were collected following informed consent from the participants, and all data were de-identified to ensure confidentiality and privacy.
Consent to Participate
The RDHS data used in this study were collected following informed consent from the participants.
Consent for Publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Nibogore, G., Eryurt, M.A. Women’s Empowerment and Infant Mortality: Evidence from Rwanda. Matern Child Health J 28, 1092–1102 (2024). https://doi.org/10.1007/s10995-024-03918-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-024-03918-2