
Abstract
Objectives
Involuntary child removal via the child protection system disproportionately affects marginalized women, yet the impacts on maternal health are under-investigated. This study prospectively examined the association of child removal with self-rated health of mothers who are sex workers. Given high levels of intergenerational family separation in this population, particularly among Indigenous sex workers, we also estimated joint effects of child removal spanning two generations.
Methods
Analyses drew on 2010–2015 data from AESHA (An Evaluation of Sex Workers’ Health Access), a prospective cohort of sex workers (n = 950) in Vancouver, Canada. Using logistic regression with generalized estimating equations, we modeled the association of past child removal and current self-rated health in a sample of 466 sex workers who ever had a live birth. Joint effects of child removal and history of removal from own parents were also investigated.
Results
Of 466 sex workers, 180 (38.6%) reported child removal at baseline and 147 (31.6%) had a history of removal from own parents. In main effects model, child removal was associated with increased odds of poorer self-rated health [odds ratio (OR) 1.50, 95% confidence interval (CI) 1.04, 2.16]. Joint effects model showed higher odds of poorer self-rated health (OR 2.04, 95% CI 1.27, 3.27) among women with intergenerational family separation.
Conclusion for Practice
Child removal was negatively associated with sex workers’ health that was worsened when family separation spanned two generations. Findings underscore need to develop sex worker and Indigenous-led family support services, along with tailored interventions to address health needs of those separated from their children.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Significance
What is already known on this subject? Sex workers who are mothers experience high rates of child removal by child protective services. Qualitative research with sex workers shows that child removal increases mental health distress.
What this study adds? Sex workers whose children were removed by child protective services were more likely to have poor self-rated health. Sex workers who experienced family separation spanning two generations, a majority of whom were Indigenous women, had the worst self-rated health. Findings underscore need for sex worker and Indigenous-led family preservation services, along with tailored interventions to address health needs of those separated from their children.
Introduction
Recent population estimates of children residing out-of-home due to involvement with child protective services indicate that 428,000 children in the US and 62,428 children in Canada are currently living apart from their parents (Jones et al. 2015; US Department of Health and Human Services 2016). There is mounting evidence demonstrating that child protection involvement is a socially patterned phenomenon, where poor families are more likely to encounter the child protection system (Slack et al. 2007), have children removed (Rivaux et al. 2008), and face lower rates of reunification (Wells and Guo 1999) and, where racially marginalized families, especially Indigenous and Black families, are widely overrepresented (Blackstock 2015; Roberts 2009). While health studies in this area have primarily focused on the health of children placed out-of-home, showing a higher frequency of negative physical and psychological health outcomes over the life course (Zlotnick et al. 2012), the consequences of out-of-placement on parents’ health, particularly mothers (often primary caregivers at the time of out-of-home placement), remain under-investigated. Since a majority of children formally reunify or eventually reestablish ties with mothers, understanding the role of child removal in women’s lives and health, especially those cited in literature as already structurally disadvantaged and vulnerable to poor health, is an important step in preventing successive removals and supporting mother–child relationships, and further, constitutes an under-explored area of health disparities research.
Among populations of structurally disadvantaged women, mothers who are sex workers face an accumulation of social-structural stressors in their lives that are shaped by poverty, racism, and the sex work policy/legal environment, which differentially influence the likelihood of child protection intervention into their families (Duff et al. 2014). Research shows sex workers can face formidable fear of losing parental rights, which introduce additional barriers to accessing health, social, and legal services for themselves and their children (Dodsworth 2014; Jackson et al. 2007), and often contribute to a mistrust of government services (Sharpe 2001). Epidemiologic findings point to a high burden of child custody loss in this population, though research to date has been mostly limited to the experiences of street-based sex workers (Duff et al. 2011, 2014). In the largest North American study on reproductive outcomes in this population, findings from a sample of 350 sex workers in Vancouver (Canada), showed that 38% of women had experienced child removal, and among these 59% were Indigenous women (Duff et al. 2011). This racial disproportionality suggests interventions by the child protection system are more consequential for Indigenous sex workers, and also reflects a wider reality in Canada and the US, where Indigenous children are consistently reported to be at greatest risk for foster care compared to all other racial/ethnic groups (Blackstock 2015; Wildeman and Emanuel 2014). This phenomenon is recognized as an extension of government-sanctioned removal of Indigenous children from their families dating back to the 1600s with the beginning of the Residential and Boarding School Systems in North America, and later through involuntary adoptions (Jacobs 2009). Such colonial initiatives, along with ongoing removal of land and basic provisions of housing, food and income, have been acknowledged as forms of genocide and collective trauma for Indigenous peoples (Heart and DeBruyn 1998), and notably have also been linked to the overrepresentation of Indigenous women in street-based sex work (Bingham et al. 2014; Hunt 2013).
While the relationship between child removal via the child protection system and sex workers’ health status has not been directly studied in epidemiologic research, evidence from one cross-sectional study of factors associated with events of child removal, showed increased odds of injection drug use and reduced occupational safety as linked to these events (Duff et al. 2014). Findings from a small number of qualitative studies further describe child removal as precipitating elevated mental health distress, housing instability, and increased drug use (Dewey et al. 2018; Dodsworth 2014; Jackson et al. 2007). Previous research examining child removal among women in other populations also show higher levels of mental health distress (including suicidality, grief, depression, anxiety), increased drug use, poorer physical health, and higher mortality (Haight et al. 2002; Kenny et al. 2015; Nixon et al. 2013; Wall-Wieler et al. 2018, 2017a, 2017b). Among these, some studies postulate that child removal can constitute a traumatic exposure, (Nixon et al. 2013) associated with post-traumatic stress, and worsening social-structural disadvantages, including housing instability and incidence of intimate partner violence (Kenny et al. 2015; Wall-Wieler et al. 2017). Examining intergenerational involvement with child protection, studies also suggest that post-removal maternal mental health and reunification outcomes are worse for mothers who themselves were removed from their parents (Fusco 2015). This consideration is important for sex workers, among whom, recent findings suggest, face a higher frequency of intergenerational familial separation compared to the general population (Duff et al. 2014).
Looking to develop a theoretical foundation to better understand the potential deleterious mechanisms underlying the relationship between child removal and sex workers’ health, and its role in women’s health disparities overall, we draw on a life course perspective (Braveman and Barclay 2009) and the “weathering” process (Geronimus et al. 2006). We conceptualize that women’s experiences of child removal (themselves as children, their own children, or both) are structural-level traumatic stressors with potential reverberating effects, including on the pathways between child removal and traumatic stress, from traumatic stress to physiological stress, and from physiological stress to adverse physical health. From this perspective, we foreground the complex biosocial pathway through which an individual’s life course exposure to historical, social and structural conditions, along with biological factors, accumulate over time to shape health. Further, we rely on the “weathering” process to account for how child removal, like other stressors, may get “under the skin”, triggering a “wearing out” of the body and sustained increases in allostatic load, which over time leads to physiological dysregulation, accelerated aging or death (Geronimus et al. 2006). In this conceptualization, child removal is theorized as a structural stressor, hypothesized as independently and cumulatively increasing women’s traumatic stress, allostatic load, and health disadvantage; a process that is likely more damaging for Indigenous women because of conditions of historical and ongoing colonialism (Walters and Simoni 2002).
Drawing on this framework, the objective in our study was to examine the link between involuntary child removal and women’s self-rated health trajectories in a prospective cohort study of sex workers, An Evaluation of Sex workers’ Health Access (AESHA). We estimated the association between child removal and sex workers’ self-rated health over time, and also estimated the joint effects of child removal and childhood history of removal from one’s own parents.
Methods
Study Sample
Our study used data from the AESHA Study, a community-based open prospective cohort of on and off-street women sex workers (n = 950) initiated in 2010 in Metro Vancouver (Canada). The study builds upon longstanding community collaborations with sex work agencies since 2005, and continues to be monitored by a Community Advisory Board of representatives from 15 community agencies.
Individuals who self-identify as women (trans-inclusive), are 14 years and older, have exchanged sex for money in last 30 days, and provide written informed consent, are eligible for inclusion in cohort. Because of challenges of recruiting sex workers in isolated locations, time-location sampling was undertaken by a peer research outreach team (current/former sex workers) in spaces identified through a community mapping process where solicitation occurs and/or where services are exchanged, indoor sex work establishments (i.e., massage parlors), and outdoor sex work venues (i.e., parks, underpasses) (Shannon et al. 2007). The study holds ethical approval through Providence Health Care/University of British Columbia Research Ethics Board.
At enrollment and at every 6 months interview, participants complete an interviewer-administered questionnaire and HIV/STI/HCV serology testing by a project nurse. In the main questionnaire information is gathered on socio-demographic characteristics, sex work patterns, drug use patterns, physical work conditions, social/interpersonal/structural environmental factors, and geographic data. Sex workers have the option to visit one of two storefront offices in Vancouver or to complete the interview-administered questionnaire and nursing component at their work or home location. Participants receive an honorarium of $40 CAD at each biannual visit.
AESHA cohort members eligible for our analysis included all women who reported a live birth at baseline and responded to a baseline question about involuntary child removal. There were 469 women in the cohort of ever had a live birth. Of these women, we excluded three who did not answer the baseline question about involuntary child removal. The final analytic sample included 466 women. The median number of waves of follow-up for participants in our study was 5 (interquartile range: 2–7).
Measures and Statistical Analyses
We conceptualized the exposure of child removal as a structural-level traumatic stressor, and identified structural, interpersonal and individual-level confounders based on a directed acyclic graph of the relationship between baseline child removal and self-rated health in follow-ups.
Exposure–Involuntary Child Removal
Exposure to involuntary child removal was assessed at baseline according to participants’ response to the question “Have you ever had any children apprehended by Child Welfare Services?”. Participants who responded affirmatively to currently parenting any children or having a live birth in the last 6 months were again asked in follow-up interviews, if they had any children removed in the last 6 months.
Outcome: Self-rated Health
We assessed women’s health dynamics over time using repeated measures of self-rated health (every 6 months). Self-rated health is based on the following question “in general, how would you rate your health?” with answer options of “excellent”, “very good”, “good”, “fair”, or “poor”?’ Constructed as a five-point scale, it is frequently dichotomized as “excellent, very good, or good health” versus “fair or poor health”, and in our analysis was dichotomized following this approach. As a measure, self-rated health has been shown to be associated with people’s integrated perception of health across socio-economic positions (Burstrom 2001).
Covariates
Each model was adjusted for: age (continuous), education (high school completion vs. incomplete), Indigenous identity, childhood trauma (continuous, sum of 25-item scale from Childhood Trauma Questionnaire) (Bernstein and Fink 1998), childhood history of removal from parents by the child protection system, physical or sexual violence by a client or partner in last 6 months (any vs. none), material support from social network in last 6 months (any vs. none), residential stability in the last 6 months (stable vs. unstable), injection and/or non-injection drug use in the last 6 months (excluding marijuana and alcohol) (any vs. none), and place of sex work solicitation in the last 6 months (street-level vs. indoor/independent, off-street or no sex work). For descriptive purposes only, we also included a variable assessing whether a participant’s biological parents or family members spent any time in the Canadian Residential School System.
Statistical Analyses
Descriptive statistics were calculated for variables of interest, stratified separately by child removal and Indigenous identity. Subsequently, logistic regression fit with generalized estimating equations (GEE) and an exchangeable correlation structure was used to estimate crude and adjusted odds ratio (OR) and 95% confidence intervals (CI) of relationship between child removal and repeated measures of self-rated health assessed over an average of four waves of follow-up. A complete case analysis was used to handle missing observations in multivariable models.
For the 12 participants who reported child removal in follow-up, all of whom had also reported prior events of child removal at baseline, a sensitivity analysis was conducted to ascertain whether including them in the exposed category introduced bias due to time-varying confounding. This analysis showed a negligible difference in the main effect estimate (< 2%) in full versus restricted sample where the 12 participants were excluded, and thus a decision was made to include these participants in the exposed category. To account for omitted cases due to non-random missing data for the childhood trauma covariate (13%), we also undertook a sensitivity analysis, where we imputed participants’ median value for childhood trauma for all of the observations with missing values. We then conducted multivariable logistic regression with full model including the imputed values. The magnitude and precision of estimates in full models with and without imputation were similar and thus have reported the non-imputed estimates. Other missing data considerations included multiple imputation for childhood trauma, however this approach was not possible based on available variables and the information collected by the AESHA study.
Confounders included in the full model were determined according to a priori justification and by strength of associations with: (a) exposure; and (b) outcome among unexposed. Since the outcome of self-rated health assesses dimensions of mental health, we did not adjust for mental health status to avoid blocking the hypothesized causal pathway leading to our outcome. To avoid over-adjustment, multicollinearity was assessed using variance inflation factors and Pearson correlation for each variable pair. The fully adjusted model was considered the least biased model, and a backwards elimination, change-in-estimate approach was used where inclusion of confounders was based on change in confidence limit ratios (a prior > 0.01) observed in comparison to a change in estimate (a priori > 0.05) (Vittinghoff et al. 2011).
Given high levels of child removal and intergenerational family separation among Indigenous women, effect measure modification by Indigenous identity and history of removal from own parents were assessed using the Quasi-likelihood Information Criteria to compare fully-adjusted main effects model and reduced models (not shown), and stratum-specific odds ratios with 95% CIs.
All analyses were performed using SAS (version 9.4; SAS Institute, Cary, NC).
Results
Baseline characteristics of the sample are shown in Table 1. Of 466 women, 180 (38.6%) experienced the exposure of involuntary child removal. Women who experienced child removal were more than twice as likely to have a history of removal from their parents (51.1% vs. 19.2%). They were also more likely to be Indigenous women, to be younger, to have elevated levels of childhood trauma, to have not completed high school, and to have a mental health diagnosis. Further, in the last 6 months they were more likely to have residential instability, to have done street-based sex work, to have used injection or non-injection drugs, and to have experienced physical and/or sexual violence by clients or intimate partners.
Indigenous women sex workers (n = 173) in the sample were more than twice as likely to have experienced child removal compared to non-Indigenous women (60.7% vs. 25.6%), and were more than three times as likely to have experienced intergenerational family separation (34.7% vs. 10.9%). Sixty percent of all Indigenous women in our sample further had a family member who attended Residential School, and among these, three-quarters also experienced intergenerational family separation through the child protection system. Across all characteristics described, Indigenous women were also more likely be structurally and socially marginalized, including a higher likelihood of being street-based workers, and to have experienced residential instability, and physical and sexual violence.
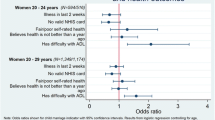
Table 2 shows the relationship between child removal and women’s self-rated health in a crude model and multivariable adjusted model. In the adjusted model, women who experienced child removal had an increased odds (OR 1.50, 95% CI 1.04, 2.16) of poorer health compared to women who did not.
The relationship between child removal and self-rated health was similar for both Indigenous and non-Indigenous women (not shown). When child removal and history of removal from one’s own parents were considered as joint exposures, each experience individually was associated with worse self-rated health and the combination of the two was associated with the worst health (OR 2.04, 95% CI 1.27, 3.27) (Table 3).
Discussion
Using prospectively collected data on sex workers in Vancouver (Canada), we found that women’s prior experience of involuntary child removal was associated with poorer self-rated health over the study follow-up period. This relationship was attenuated but remained significant after adjustment for individual, interpersonal and structural-level risk factors, highlighting their potential explanatory and mediating influences. We also found some evidence that the joint intergenerational effect of child removal and history of removal from one’s parents was associated with a higher burden of poor health.
Results are consistent with our hypothesis that child removal is a unique exposure, and one where traumatic stress from these events may affect women for years, activating a plausible “weathering” effect on their health, including potential acceleration of biological aging, and, as shown in previous research, increased risk of mortality (Wall-Wieler et al. 2018). This adverse exposure may also increase likelihood of other stressful events, such as loss of income and housing (Hook et al. 2016; Wall-Wieler et al. 2017), which are well-established as also having deleterious effects on health. Results support earlier studies with mothers who are sex workers documenting the aftermath of child removal as characterized by worsened mental health and increased drug use (Dewey et al. 2018; Dodsworth 2014; Jackson et al. 2007), while also extending this literature by formally assessing the relationship between child removal and health status in this population. Together, these findings are compatible with the theory that child removal can be a widely disruptive life event conferring additional health and social-structural disadvantages to sex workers, and, as shown in our study, trajectories of poorer self-rated health.
Increased odds of poorer self-rated health were greatest for sex workers facing two generation of child removal, a majority of whom were Indigenous women. Descriptive results showed extremely high prevalence of family separation among Indigenous mothers, which in some cases spanned three or more generations, including removal from biological parents and familial attendance at Residential School. This finding supports earlier research on diminished wellbeing of second generation mothers involved in child protection (Fusco 2015), and adds to a growing evidence base positioning the child protection system as a vector of colonization, which is inseparable and reliant on other forms of colonial dispossession, including losses of land and culture, and inequitable provisions of housing, food, income, and health services (Blackstock 2015; Truth and Reconciliation Canada 2015). Our finding suggests that intergenerational child removal may have a larger influence on life course health trajectories than each generation individually, and thus supports the likelihood of family separation being more adversely consequential for the health of Indigenous women (compared to non-Indigenous women) due to the well-documented cumulative losses they face (Walters and Simoni 2002). Similar to the established association between attendance at Residential School and poorer health among Indigenous peoples (Truth and Reconciliation Canada 2015), our results suggest the current child protection system also has important implications for population-level health disparities between Indigenous and non-Indigenous peoples, of which the extent and impact requires attention.
Our findings confirm the salience of existing initiatives to prevent child removal among marginalized women, such as efforts to promote positive parenting experiences from birth. These include ‘rooming-in’ hospital-based programs for mothers with drug-exposed newborns, which have been shown to decrease lengths of stay of newborns, increase maternal custody of infants at discharge (Abrahams et al. 2010), and reduce hospital expenditures (Grossman et al. 2017). The sheer magnitude of this exposure among sex workers in our study also highlights the need for tailored services for marginalized mothers, including sex worker-led family support and preservation services, including systemic advocacy to prevent child removal, and in cases of removal, post-removal health, legal, and social supports. Further, the disproportionately high number of Indigenous sex workers dealing with child removal, and intergenerational family separation, greatly emphasize the need to challenge contemporary colonial structures, and ensure development of Indigenous sex worker-led pregnancy and parenting services, including culturally safe birthing services and family-centered housing (Nathoo et al. 2013).
Our study adds to existing literature on child removal and women’s health by expanding its scope to mothers who are sex workers, an understudied and high priority population. Other strengths include being among the first known studies to apply quantitative methods to estimate the association between child removal and women’s health, and to conduct a comparison of self-rated health status between first-generation and second-generation women involved in the child protection system. Our findings, however, must be interpreted within the limitations of the study design. First, a primary limitation is that we were not able to establish temporal ordering of self-rated health status pre- and post-child removal to assess causality, nor could we ascertain specific reasons for child removal, and whether these were associated with health status. Second, while we had acceptable data on child removal, we did not have data on event timing and could not account for how time-lapse since the event may differentially affect health. Third, we could not assess current status of mother–child relationship, including whether reunification had occurred following events of removal. Fourth, measurement inaccuracy of variables is also a limitation due to poor recall, a wish for privacy, or other reasons, however, good rapport with the AESHA interview staff may minimize social desirability bias. Finally, our findings are from a time-location based sample of sex workers and should be replicated in population-based samples to assess generalizability to other populations in and outside of Canada.
Our findings echo calls for researchers to take account of the effects of the child protection system in the patterning of health among marginalized populations, including attention to how social and health inequities may be both causes and consequences of encounters with this system. Having prior exposure to family separation through the child protection system was found to be associated with poorer health trajectories among mothers in our study, that were further worsened when family separation spanned two generations. To better characterise this disparity, future studies should examine the association of child removal with specific health outcomes. Findings also underscore the need to develop sex worker and Indigenous-led community-based services to prevent child removal and preserve families, including tailored health and social supports for those separated from their children.
References
Abrahams, R. R., MacKay-Dunn, M. H., Nevmerjitskaia, V., MacRae, G. S., Payne, S. P., & Hodgson, Z. G. (2010). An evaluation of rooming-in among substance-exposed newborns in British Columbia. Journal of Obstetrics and Gynaecology Canada, 32(9), 866–871. https://doi.org/10.1016/S1701-2163(16)34659-X.
Bernstein, D. P., & Fink, L. (1998). Childhood trauma questionnaire: A retrospective self-report: Manual. Orlando: Psychological Corporation.
Bingham, B., Leo, D., Zhang, R., Montaner, J., & Shannon, K. (2014). Generational sex work and HIV risk among Indigenous women in a street-based urban Canadian setting. Culture, Health and Sexuality, 16(4), 440–452.
Blackstock, C. (2015). Should governments be above the law? The Canadian human rights tribunal on first nations child welfare. Children Australia, 40(02), 95–103. https://doi.org/10.1017/cha.2015.6.
Braveman, P., & Barclay, C. (2009). Health disparities beginning in childhood: A life-course perspective. Pediatrics, 124(Supplement 3), S163–S175.
Burstrom, B. (2001). Self rated health: Is it as good a predictor of subsequent mortality among adults in lower as well as in higher social classes? Journal of Epidemiology and Community Health, 55(11), 836–840. https://doi.org/10.1136/jech.55.11.836.
Dewey, S., Orchard, T., & Brown, K. (2018). Shared precarities and maternal subjectivities: Navigating motherhood and child custody loss among North American women in street-based sex work. Ethos, 46(1), 27–48.
Dodsworth, J. (2014). Sex worker and mother: Managing dual and threatened identities. Child and Family Social Work, 19(1), 99–108. https://doi.org/10.1111/j.1365-2206.2012.00889.x.
Duff, P., Bingham, B., Simo, A., Jury, D., Reading, C., & Shannon, K. (2014). The “stolen generations” of mothers and daughters: Child apprehension and enhanced HIV vulnerabilities for sex workers of aboriginal ancestry. PLoS ONE. https://doi.org/10.1371/journal.pone.0099664.
Duff, P., Shoveller, J., Zhang, R., Alexson, D., Montaner, J. S., & Shannon, K. (2011). High lifetime pregnancy and low contraceptive usage among sex workers who use drugs- an unmet reproductive health need. BMC Pregnancy and Childbirth, 11(1), 61. https://doi.org/10.1186/1471-2393-11-61.
Fusco, R. A. (2015). Second generation mothers in the child welfare system: Factors that predict engagement. Child and Adolescent Social Work Journal. https://doi.org/10.1007/s10560-015-0394-4.
Geronimus, A. T., Hicken, M., Keene, D., & Bound, J. (2006). “Weathering” and age patterns of allostatic load scores among blacks and whites in the United States. American Journal of Public Health, 96(5), 826–833. https://doi.org/10.2105/AJPH.2004.060749.
Grossman, M. R., Berkwitt, A. K., Osborn, R. R., Xu, Y., Esserman, D. A., Shapiro, E. D., et al. (2017). An Initiative to improve the quality of care of infants with neonatal abstinence syndrome. Pediatrics, 139(6), e20163360. https://doi.org/10.1542/peds.2016-3360.
Haight, W. L., Black, J. E., Mangelsdorf, S., Giorgio, G., Tata, L., Schoppe, S. J., et al. (2002). Making visits better: The perspectives of parents, foster parents, and child welfare workers. Child Welfare, 81(2), 173–202.
Heart, M. Y. H. B., & DeBruyn, L. M. (1998). The American Indian holocaust: Healing historical unresolved grief. American Indian and Alaska Native Mental Health Research, 8(2), 56.
Hook, J. L., Romich, J. L., Lee, J. S., Marcenko, M. O., & Kang, J. Y. (2016). Trajectories of economic disconnection among families in the child welfare system. Social Problems. https://doi.org/10.1093/socpro/spw006.
Hunt, S. (2013). Decolonizing sex work: Developing an intersectional indigenous approach. In E. van der Muelen, E. M. Durisin, & V. Love (Eds.), Selling sex: Experience, advocacy, and research on sex work in Canada (p. 364). Vancouver: UBC Press.
Jackson, L. A., Bennett, C. G., & Sowinski, B. A. (2007). Stress in the sex trade and beyond: Women working in the sex trade talk about the emotional stressors in their working and home lives. Critical Public Health, 17(3), 257–271. https://doi.org/10.1080/09581590701549535.
Jacobs, M. D. (2009). White mother to a dark race: Settler colonialism, maternalism, and the removal of indigenous children in the American West and Australia, 1880–1940. Lincoln: U of Nebraska Press.
Jones, A., Sinha, V., & Trocmé, N. (2015). Children and youth in out-of-home care in the Canadian provinces. CWRP Information Sheet E, 167.
Kenny, K. S., Barrington, C., & Green, S. L. (2015). “I felt for a long time like everything beautiful in me had been taken out”: Women’s suffering, remembering, and survival following the loss of child custody. International Journal of Drug Policy, 26(11), 1158–1166.
Nathoo, T., Poole, N., Bryans, M., Dechief, L., Hardeman, S., Marcellus, L., et al. (2013). Voices from the community: Developing effective community programs to support pregnant and early parenting women who use alcohol and other substances. First Peoples Child and Family Review, 8, 93–106.
Nixon, K. L., Radtke, H. L., & Tutty, L. M. (2013). “Every day it takes a piece of you away”: Experiences of grief and loss among abused mothers involved with child protective services. Journal of Public Child Welfare, 7(2), 172–193. https://doi.org/10.1080/15548732.2012.715268.
Rivaux, S. L., James, J., Wittenstrom, K., & Jeffries, V. (2008). The intersection of race, poverty, and risk: understanding the decision to provide services to clients and to remove children. Child Welfare, 87, 151–169.
Roberts, D. (2009). Shattered bonds: The color of child welfare. New York: Civitas Books.
Shannon, K., Bright, V., Allinott, S., Alexson, D., Gibson, K., & Tyndall, M. W. (2007). Community-based HIV prevention research among substance-using women in survival sex work: The Maka Project Partnership. Harm Reduction Journal, 4(1), 20.
Sharpe, T. T. (2001). Sex-for-crack-cocaine exchange, poor black women, and pregnancy. Qualitative Health Research, 11(5), 612–630. https://doi.org/10.1177/104973201129119334.
Slack, K. S., Lee, B. J., & Berger, L. M. (2007). Do welfare sanctions increase child protection system involvement? A cautious answer. Social Service Review, 81(2), 207–228.
Truth and Reconciliation Canada. (2015). Honouring the truth, reconciling for the future: Summary of the final report of the Truth and Reconciliation Commission of Canada. Winnipeg: Truth and Reconciliation Commission of Canada.
US Department of Health and Human Services. (2016). Trends in Foster Care and Adoption: FY 2006–FY 2015, 2015, 1–3. Retrieved October 7, 2017, from https://www.acf.hhs.gov/sites/default/files/cb/trends_fostercare_adoption2015.pdf.
Vittinghoff, E., Glidden, D. V., Shiboski, S. C., & McCulloch, C. E. (2011). Regression methods in biostatistics: Linear, logistic, survival, and repeated measures models. Springer Science & Business Media.
Wall-Wieler, E., Roos, L. L., Bolton, J., Brownell, M., Nickel, N. C., & Chateau, D. (2017a). Maternal health and social outcomes after having a child taken into care: Population-based longitudinal cohort study using linkable administrative data. Journal of Epidemiology and Community Health, 71(12), 1145–1151.
Wall-Wieler, E., Roos, L. L., Brownell, M., Nickel, N., Chateau, D., & Singal, D. (2017b). Suicide attempts and completions among mothers whose children were taken into care by child protection services: A cohort study using linkable administrative data. Canadian Journal of Psychiatry. Revue Canadienne de Psychiatrie. https://doi.org/10.1177/0706743717741058.
Wall-Wieler, E., Roos, L. L., Nickel, N. C., Chateau, D., & Brownell, M. (2018). Mortality among mothers whose children were taken into care by child protection services: A discordant sibling analysis. American Journal of Epidemiology, 187, 1182–1188.
Walters, K. L., & Simoni, J. M. (2002). Reconceptualizing native women’s health: An “indigenist” stress-coping model. American Journal of Public Health, 92(4), 520–524.
Wells, K., & Guo, S. (1999). Reunification and reentry of foster children. Children and Youth Services Review, 21(4), 273–294.
Wildeman, C., & Emanuel, N. (2014). Cumulative risks of foster care placement by age 18 for US children, 2000–2011. PLoS ONE, 9(3), e92785.
Zlotnick, C., Tam, T. W., & Soman, L. A. (2012). Life course outcomes on mental and physical health: The impact of foster care on adulthood. American Journal of Public Health, 102(3), 534–540. https://doi.org/10.2105/AJPH.2011.300285.
Acknowledgements
This research is supported by the US National Institutes of Health (R01DA028648), a Canadian Institutes of Health Research Foundation Grant, and MacAIDS. KSK is supported by the Dissertation Completion Fellowship at the University of North Carolina at Chapel Hill. KS is supported by partially supported by a Canada Research Chair in Global Sexual Health, NIH, and HIV/AIDS and Michael Smith Foundation for Health Research. We thank all those who contributed their time and expertise to this project, particularly participants, AESHA community advisory board members and partner agencies, and the AESHA team, including: Sarah Moreheart, Jennifer Morris, Sylvia Machat, Jane Li, Minshu Mo, Sherry Wu, Emily Leake, Anita Dhanoa, Meaghan Thumath, Alka Murphy, Jenn McDermid, Tave Cole, Jaime Adams, Roisin Heather, Anna Mathen, Bridget Simpson, and Carly Glanzberg. We also thank Abby Rolston, Peter Vann, Erin Seatter, Jill Chettiar, and Patricia McDonald for their research and administrative support. KSK would also like to thank Clare Barrington, Carolyn Halpern, Kavita Singh Ongechi, and Brian Pence at the University of North Carolina at Chapel Hill for their dissertation supervisory and research support.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kenny, K.S., Ranville, F., Green, S.L. et al. Family Separation and Maternal Self-rated Health: Evidence from a Prospective Cohort of Marginalized Mothers in a Canadian Setting. Matern Child Health J 23, 1232–1239 (2019). https://doi.org/10.1007/s10995-019-02762-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-019-02762-z