
Abstract
Objectives Although several studies have examined risk factors associated with abuse during pregnancy or postpartum periods, many used clinic-based or small regional samples, and few were national or population-based, limiting their generalizability and clinical utility. The purpose of this study was to describe the correlates of abuse around the time of pregnancy among a nationally representative sample of women in Canada. Methods Using data from 6421 postpartum women (weighted n = 76,500) who completed the Canadian Maternity Experiences Survey from 10/2006 to 01/2007, we explored the association between demographic, psychosocial, behavioral, medical/obstetric factors and ‘any’ and ‘severe’ abuse. ‘Any abuse’ was defined as an affirmative answer to one or more of 10 items asked about physical or sexual abuse or threats of abuse. ‘Severe abuse’ was defined as experiencing a combination of threats and physical or sexual abuse. Odds ratios and their 95 % confidence intervals were generated from multivariable logistic regression models. Results 10.5 % of women (weighted n = 8400) reported ‘any’ abuse and 4.3 % (weighted n = 3400) reported ‘severe’ abuse in the previous 2 years. Correlates of severe abuse included: age <20 years; household income below the low income cut-off; single; stressful life events; history of depression or antidepressant use; smoking during pregnancy; and alcohol use prior to pregnancy. Correlates of ‘any’ abuse were the same as ‘severe’ abuse with the addition of age 20–34 years, developing a new health problem during pregnancy, and inadequate support during pregnancy. Increased odds of ‘any’ and ‘severe’ abuse were found for women who self-identified as Aboriginal and reduced odds of ‘any’ abuse were found among immigrant women and those who took folic acid pre-pregnancy. Conclusions We identified risk factors that may enhance early detection of abuse in the perinatal period, and inform the development of interventions and preventive strategies to address this important public health problem.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Significance
We identified risk factors for abuse in the perinatal period. These findings may enhance early detection of abuse in the perinatal period, and inform the development of interventions and preventive strategies to address this important public health problem.
Introduction
Abuse (during pregnancy and the postpartum period) is a significant public health problem [1] with serious adverse consequences for both mother and child. Pregnant and postpartum women experiencing abuse have increased risk of physical injury, homicide [2], perinatal mental health disorders including post-traumatic stress disorder [3–6], sexually transmitted diseases, the exacerbation of chronic health issues (e.g., hypertension, diabetes) [7], and inadequate or excessive gestational weight gain [8, 9]. Newborns of abused women have increased risk of low birth weight and preterm birth [10, 11] and neonatal mortality [11].
Abuse has been defined as threats or acts of harm that are physically, sexually, or emotionally harmful [12]. Reported prevalence rates of abuse during pregnancy vary widely from 0.9 to 20.1 %, depending upon the measure, form of violence, population, and study methods; however, studies of detailed and repeated assessments tend to report higher rates (7.4–20.1 %) [12, 13]. In the US, rates of abuse during pregnancy range from 4 to 8 % [12], while studies by the World Health Organization show rates higher than 5 % in 11 of 15 countries studied [14]. Canadian studies report a prevalence of physical intimate partner abuse during pregnancy of 1.2 % [15] to 6.6 % [16] and 10.9 % prior to pregnancy [16]. A recent meta-analysis of 92 studies reported an average prevalence of 28.4 % for emotional abuse, 13.8 % for physical abuse, and 8.0 % for sexual abuse during pregnancy [17]; overall rates of abuse were higher in developing countries compared to developed countries, and in hospital-based studies compared to at-home surveys [17].
Strong evidence exists that women experiencing abuse do not self-disclose their situations during routine prenatal care, but respond to provider-initiated inquiry [18, 19]. Furthermore, despite the increased number of contacts with healthcare providers in the course of routine prenatal care and higher utilization of medical services, few providers routinely assess pregnant and postpartum women for abuse [20, 21]. While evidence is limited, some studies demonstrated that routine, standardized screening of domestic violence in pregnancy increases detection, intervention, and follow-up [22]. However, few validated screening tools appropriate for primary care are available, few validation studies have been conducted on existing tools, and current research suggests that few of the current tools possesses excellent psychometric properties [23]. Given that the structure of existing tools focuses on inquiry of direct abuse (e.g., physical insult, threats, emotional abuse), improving our understanding of risk factors associated with abuse around the time of pregnancy could enhance the accuracy of existing tools and early detection—particularly for women who are unwilling to disclose abuse incidents [18].
Although several studies have examined risk factors for abuse during pregnancy in a variety of countries, as demonstrated in James et al.’s [17] meta-analysis of 55 studies, many of these studies used clinic-based or small regional samples, and few were national or population-based, limiting their generalizability and clinical utility. The majority of studies have been conducted in the United States [17], with US-based studies in general having the largest sample sizes of those reported [12, 24, 25]. Most notable was Saltzman et al.’s [25] study of 16 states using data on 64,994 births from the Pregnancy Risk Assessment Monitoring System (PRAMS), which was population-based but not national in scope. To our knowledge, only four studies have examined risk factors for abuse during pregnancy in Canadian settings, using samples obtained in the cities of Toronto [16], Saskatoon [26], Vancouver [15], and Winnipeg [27]. These studies found that women most at risk for abuse during pregnancy were Aboriginal, were socioeconomically disadvantaged, were younger, had unhealthy lifestyle behaviours (e.g., alcohol or illicit drug use), had partners with a drinking problem, reported high perceived stress, experienced a high number of negative life events in the preceding year, and had low social support. However, no Canadian studies have explored risk factors for abuse across the pregnancy and postpartum period.
The Canadian Maternity Experiences Survey (MES) provides a unique opportunity to study correlates of abuse around the time of pregnancy in a national, population-based sample of women in Canada. A previous study using MES data by members of our research team described the prevalence of abuse before, during and after pregnancy; the frequency, timing, and types of abuse; the category of perpetrator; and rates of abuse based on demographic characteristics (age, income, education, marital status, ethnicity) [28]. The purpose of this study was to explore the association between a wide variety of demographic, psychosocial, behavioral, and medical/obstetric factors and the outcome variables of “any abuse”, defined as experiencing one or more acts of abuse in the 2 years preceding the interview, and “severe abuse”, defined as experiencing a combination of physical abuse and threats, among a nationally representative sample of women who participated in the MES.
Methods
Procedures and Participants
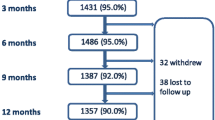
This study utilized data from the MES of the Public Health Agency of Canada [29, 30]. The MES is a national survey designed to provide information on Canadian women’s knowledge, experiences, and practices during pregnancy, birth and the early postpartum [29]. A stratified random sample of 8542 women was drawn from a sampling frame of 58,972 women who had completed the 2006 Canadian Census of Population and were 15 years of age and over, had delivered a live, singleton infant in the 3 months prior to the Census, and were living with their infant at the time of the interview [29, 31]. Detailed descriptions of the sampling process, survey development, pilot testing, survey methodology and data quality have been reported previously [29, 31, 32]. The survey was conducted by trained female interviewers from Statistics Canada between 10/2006 and 01/2007 using computer-assisted telephone interviews with an average length of 45 min. Mothers were interviewed between 5 and 14 months postpartum, with over 96 % interviewed between 5 and 9 months postpartum. The final response rate was 78 % (n = 6421) [29]. The MES final report and questionnaire can be retrieved from http://www.phac-aspc.gc.ca/rhs-ssg/survey-eng.php.
The MES research protocol was reviewed by Health Canada’s Science Advisory Board and Research Ethics Board, and the Federal Privacy Commissioner and approval was received from Statistics Canada’s Policy Committee prior to implementation [31]. This secondary analysis of the MES was approved by the St. Michael’s Hospital Research Ethics Board and by the Research Data Centre Access Granting Committee of Statistics Canada.
Outcome Variables
The outcomes were ‘any abuse’ and ‘severe abuse’ occurring either before, during or after the pregnancy. The MES included ten items related to physical and sexual abuse that were adapted from the Canadian Violence Against Women Survey [33]. Women were asked to respond “yes” or “no” to the following questions: “In the last two years, has anyone ever… (1) Threatened to hit you with his or her fist or anything else that could have hurt you? (2) Thrown anything at you that could have hurt you? (3) Pushed, grabbed, or shoved you in a way that could have hurt you? (4) Slapped you? (5) Kicked you, bit you, or hit you with his or her fist? [6] Hit you with something that could have hurt you? Exclude hitting with a fist. (7) Beaten you? (8) Choked you? (9) Used or threatened to use a gun or knife on you? (10) Forced you into any unwanted sexual activity by threatening you, holding you down, or hurting you in some way?” Our previous study indicated that the first three items were most frequently reported by women (ranging from 4.5 to 7.0 %), while more serious forms of physical abuse (items 4–10) were less common (ranging from 0.7 to 3.4 %) [28].
In this analysis, ‘any abuse’ was defined as an affirmative answer to one or more of the 10 items. ‘Severe abuse’ was defined as experiencing a combination of threats (an affirmative answer to one or more of items 1–3) and physical or sexual abuse (an affirmative answer to one or more of items 4–10).
Correlates of Abuse
The independent variables, or potential correlates of abuse, were selected based on a review of the literature and availability of variables in the MES that related to this study’s purpose of understanding how demographic, psychosocial, behavioral, and medical/obstetric factors were related to abuse. The variables are listed in Table 1. To classify income level, we used low-income cut-off levels (LICO) constructed by Statistics Canada based on the average level of expenditures on food, clothing and housing for a particular size of family and area of residence [34]. Immigrant status was identified by a negative response to the MES question, ‘Were you born a Canadian citizen?’ Aboriginal identity was determined by an affirmative response to the question, ‘Are you an Aboriginal person, that is, First Nations, Metis or Inuit?’ Perceived social support was rated as low if women responded none, a little, or some of the time to the question, ‘During your pregnancy, how often was support available to you when you needed it?’ Women indicated whether they had experienced any of a list of 13 stressful life events from the Newton and Hunt scale [35] during the 12 months before baby was born. To be consistent with other studies of pregnant and postpartum women that used this scale, high stress was defined as three or more stressful events [36]. Perceived stress was based on the question, Thinking about the amount of stress in your life during the 12 months before your baby was born, would you say that most days were______ with response choices of not, somewhat, or very stressful. An analysis of the stressful life events and perceived stress experienced by women in the MES has been reported in detail elsewhere [36]. Reaction to pregnancy was considered unhappy if women responded somewhat or very unhappy or neither happy/unhappy to the question, ‘When you first realized you were pregnant, what was your reaction? Were you…?
Data Analysis
The MES is based upon a complex sampling design involving “stratification, multiple states of selectin and unequal probabilities of selection of respondents” [29]. Therefore, Statistics Canada requires that survey weights be used to account for the unequal probabilities of selection of respondents and to obtain unbiased point estimates representative of the Canadian population [32]. Special procedures for the analysis of survey data (SURVEYFREQ and SURVEYLOGISTIC) were used to obtain weighted proportions and odds ratios (OR) with 95 % confidence intervals (95 % CI) using the Taylor Series method of variance estimation [32]. Variables that were significantly associated with abuse at p < .10 in the univariable logistic regression analyses were included in the multivariable regression models. Statistical significance in the final multivariable models was defined as p < .05.
Missing data were very low (<6 %) for most variables and therefore were not considered in the analyses [29], with the exception of low income, for which we created a category labelled “Missing” to prevent a significant drop in the sample size. There was no imputation done for the Maternity Experiences Survey (p. 18, Microdata User Guide) [32]. The MES reporting guidelines prohibit the reporting of estimates based on cell counts less than five and recommend the reporting of weighted counts rounded to the nearest 100. The degree of sampling error affecting estimates was based on the coefficient of variation (CV). Estimates with a CV in excess of 33.3 % are considered unreliable and therefore not reported [29, 32].
Results
Most women that responded to the MES were Canadian-born, 20–34 years of age, married, had completed high school, and had incomes above the low-income cut-off (LICO) (Table 1). In the total weighted sample of 76,500 women, 8400 (10.5 %) experienced ‘any’ abuse in the 2 years prior to the interview and 3400 (4.3 %) experienced ‘severe’ abuse (Table 1).
In the unadjusted analyses, 22 of the 31 variables studied were significantly associated with increased odds of ‘any abuse’ and 23 of the 31 variables were significantly associated with increased odds of ‘severe abuse’ around the time of pregnancy (Table 1). The majority of the unadjusted odds ratios (UOR) were higher for correlates of ‘severe abuse’ than ‘any abuse’ (e.g., UOR 17.77 vs. 9.32 for age <20 years). Two of the 31 variables were significantly associated with a decreased odds of both ‘any’ or ‘severe’ abuse, providing a protective effect: being an immigrant, and taking folic acid in the 3 months before pregnancy.
In the final multivariable logistic regression models (Table 2), 15 variables increased and one decreased the odds of any abuse, while 9 variables increased and one decreased the odds of severe abuse, after adjusting for the effects of other variables in the model. The adjusted odds ratios were slightly higher for factors associated with severe abuse compared to any abuse. Demographic variables that were associated with increased likelihood of ‘any’ abuse in the previous 2 years were <20 or 20–34 years of age, single, self-reported Aboriginal identity, and household income at or below the LICO. These findings are similar to other Canadian studies that reported socioeconomic differentials between abused and non-abused women [15, 16, 26, 27]. Women who were not Canadian-born had reduced odds of experiencing ‘any’ abuse compared to Canadian-born women. Psychosocial variables were also associated with ‘any’ abuse. Women who reported high levels of perceived stress or three or more stressful life events in the 12 months prior to the birth of their infant, a prior diagnosis of depression or a prescription of antidepressants before pregnancy, and inadequate social support were more likely to report ‘any’ abuse, compared to women who reported lower stress, no depression diagnosis or antidepressant prescription, and adequate social support (respectively). Women who developed a new medical condition during pregnancy or who had a previous abortion were more likely to experience ‘any’ abuse than those not reporting a new medical condition or previous abortion. Health behaviors associated with ‘any’ abuse included smoking during pregnancy, or using illicit drugs or drinking three or more alcoholic beverages on one occasion before pregnancy. None of the anthropometric variables were associated with ‘any’ abuse in the final multivariable models.
Similar to ‘any’ abuse, women who experienced ‘severe’ abuse in the previous 2 years were more likely to be <20 years of age, single, have household incomes at or below the LICO, have self-reported as Aboriginal identity, reported having three or more stressful life events or that ‘most days’ were ‘very’ stressful in the 12 months prior to giving birth, have been previously given a diagnosis of depression or antidepressant prescription, smoked in the last 3 months of their pregnancy, or drank three or more alcoholic beverages on one occasion prior to pregnancy. Those correlates that were related to ‘any’ abuse, but not associated with ‘severe’ abuse, were age 20–34 years, immigrant status, low social support, having a new medical condition during pregnancy or a previous abortion, and using street drugs in the 3 months prior to pregnancy. A protective factor associated with ‘severe’ abuse was taking folic acid in the 3 months before pregnancy.
Discussion
Few studies have examined correlates of abuse across pregnancy and the postpartum period. This study contributes to this body of literature by providing the first nationally representative Canadian data on correlates of abuse around the time of pregnancy. We found that demographic, psychosocial, and medical/obstetric factors, as well as risky health behaviours were related to abuse, with the strongest correlates being age <20 and experiencing three or more stressful life events in the 12 months prior to the birth of the infant. We also found stronger associations of correlates of abuse with ‘severe’ abuse compared to ‘any’ abuse.
Our findings suggested that women who experienced abuse in the 2-year period prior to the interview were more likely to experience social disadvantage. Indeed, the factor that was most strongly related to abuse in our study was being <20 years of age. The social patterning of abuse that we observed is similar to other studies from Australia and the US that have found that youth (<20 years) [15, 20, 37], being single [17, 20, 27, 38], and socioeconomic deprivation [17, 37–40] were associated with abuse during pregnancy. Poverty has also been identified as an important factor linked to the disproportionate burden of abuse experienced by Aboriginal women [41]. In addition to poverty, Aboriginal women in abusive relationships may face unique challenges when seeking to leave an abusive circumstance including, but not limited to, child protection; community responsibilities and kinship ties that go beyond the intimate partner; connections to and retention of access to land and property; and the geographic proximity and cultural relevance of support services [13].
Few studies have explored abuse in pregnant and postpartum Aboriginal women. The increased risk of abuse that we observed was also found in two other Canadian studies of Aboriginal pregnant/postpartum women [15, 27]. In a study focussing on the disproportionate abuse experienced by Aboriginal participants in the MES compared to Canadian-born participants, Daoud et al. [41] found this disparity could be partially, although not completely, explained by socioeconomic status. Daoud et al. [41] posit that a ‘colonization effect’ may contribute to this disparity, where traditionally “equal and complimentary roles” between men and women were disrupted by colonization, resulting in women’s status being diminished [42]. Others have suggested that the absence of historical Aboriginal governance structures for addressing perpetrators of abuse and promoting community healing has contributed to increased risk of abuse [43].
Psychosocial risk was one of the main correlates of ‘any’ and ‘severe’ abuse, with the strongest risk found among women reporting three or more stressful life events in the year prior to giving birth. This finding is similar to other studies that have found strong associations between stress and abuse [26, 27, 40]. For example, Heaman [27] reported that among numerous demographic, obstetrical, anthropometric, and health behaviour variables examined, women with high life event stress were over four times more likely to experience abuse than women with fewer stressful life events. Similarly, Almeida et al. [44] found that the vast majority of pregnant women who experienced physical abuse also experienced psychological/ emotional abuse and mental health problems, and a recent meta-analysis reported a large association between domestic violence and perinatal mental disorders [3]. Thus, our findings are consistent with national and international guidelines to conduct comprehensive, psychosocial assessments as part of routine prenatal and postnatal care that include both physical and emotional abuse and mental health [45–50]. These guidelines are consistent in their recommendations to assess for intimate partner violence and provide supportive care to ensure the safety of the woman and child. The recently released Marcé International Society position statement on psychosocial assessment and depression screening in perinatal women notes, “Equally important is the need to address adverse social circumstances (where possible) and history of current or past violence and trauma. With the research focus to date mainly on perinatal depression, interpersonal violence and past trauma have tended to be under-investigated as potential key risk and mediating factors” (p. 180) [45].
Similar to Charles and Perreira [51], we found that fewer immigrant women reported experiencing abuse in the 2-year period prior to the interview than non-immigrant women. Other studies have reported lower rates of violence among pregnant immigrant women than we observed in this study [52, 53], but found significant associations with poorer health behaviours, including not being current in vaccinations, not taking folic acid before pregnancy, and initiating prenatal care late [52]. Thus, some have suggested that immigrant status is not protective against abuse, but rather that abuse is under-reported by immigrant women [54] for reasons including male domination and patriarchy, lack of knowledge and access to social services, male attendance at social and health visits that discourage women from disclosing, financial dependency on their husbands, and fear of deportation if they report abuse [55].
The association between risky health behaviour (e.g., smoking) and abuse that we found has been reported in previous studies [17, 27, 56], with fewer reporting a relationship with previous abortion [57]. We did not find any other studies that explored the association between folic acid supplementation and abuse. However, the protective effect that we observed may be explained by evidence that uptake of folic acid is higher among women with less disadvantage [58] who would also tend to be less likely to experience abuse. That we did not find a relationship between abuse and obstetric history, response to the pregnancy, anthropometric variables, or healthcare utilization suggests that the social risk factors play predominant roles in the occurrence of abuse.
Implications
There is growing interest in identifying correlates for abuse that would promote early identification of women experiencing or at risk of abuse [20]. Given that pregnant and postpartum women frequently do not voluntarily disclose their abuse [59], risk factors correlated with abuse can help to increase its detection. As recommended by the Society of Obstetricians and Gynecologists of Canada (SOGC), a single correlate such as young age should prompt further investigation in the form of a comprehensive assessment that may include depression, anxiety, substance use, and social support systems [60].
Although the American College of Obstetricians and Gynecologists (ACOG) has recommended routine screening of abuse as part of annual examinations, during each trimester of pregnancy, and during the postpartum checkup [59], few healthcare providers screen for abuse as part of routine care [7, 20, 21]. However, structured screening of abuse improves detection rates, particularly when repeated questioning on multiple occasions is used [22] and universal psychosocial screening has been associated with improved pregnancy outcomes [61]. Routine screening by self-report, clinic staff interview, and physician interview have all been found to be acceptable by both abused and non-abused women when conducted by a skilled provider with an established trust relationship with the client [62]. Single item assessments for abuse (i.e., one question evaluating whether or not abuse is present) are less effective at detecting abuse. In addition, screening tools that ask detailed questions about types of abuse experienced (e.g., Abuse Assessment Screen [63]; Conflict Tactics Scale [64]) have been used in some clinical settings as effective approaches to identifying specific forms of current abuse. Comprehensive prenatal psychosocial assessment that includes a range of risk factors including stressful life events, abuse, substance use and lack of social support, such as the Antenatal Risk Questionnaire, has been shown to be acceptable to women and highly useful to clinicians in identifying and triaging women with low, moderate and high psychosocial risk [65]. Our findings may help inform the refinement of these comprehensive assessment tools to enhance their accuracy in detecting both abuse and mental health problems. Given evidence from a recent Cochrane review that screening alone does not increase referral or linkage to healthcare services [66], future research should also develop and evaluate the effectiveness and feasibility of integrated processes that link abuse assessment to comprehensive referral and service provision [67]. An additional policy implication is the need to advocate for an ongoing national survey of women’s maternity experiences in Canada in order to enable examination of changes in risk factors for abuse over time and other important variables not available in administrative databases.
Limitations
Women participating in the MES may have been reluctant to disclose abuse during the interview, and therefore the prevalence of abuse may be underestimated. The MES excluded women who lived on First Nations reserves and those who did not have their child living with them at the time of the interview; yet, these women may be more likely to experience many of the social risk factors that we found associated with abuse. Risk factors for abuse have been categorized as victim-, perpetrator-, and pregnancy-related factors [68]. We were unable to assess perpetrator-related factors (such as substance use [17, 51]) in detail as these data were not collected as part of the MES. Because of the cross-sectional design of the MES, it was not possible to determine the directional effect of many variables that were associated with abuse (e.g., substance use); thus, we chose to use the term correlates of abuse rather than risk factors. While folic acid supplementation may be a marker for healthy pregnancy behavior, the association between folic acid supplementation and abuse may be spurious. Caution should be taken in the interpretation of this finding. Although emotional abuse is more common than physical abuse [17], the MES did not include questions about emotional abuse. These limitations may have led to some women at risk not being identified, and thus the prevalence and magnitude of risk we report may be underestimated. The MES was conducted in 2006/07 and the relative importance of some of the correlates of abuse may have changed over time due to changes in population characteristics or in the provision of health and social services. However, this is unlikely, given that screening for abuse and provision of resources are not components of routine prenatal and postnatal care in most countries. Finally, while a 78 % response rate in survey-based research may suggest a lack of generalizability of the findings, we adjusted survey weights for non-response so that the conclusions (based on weighted frequencies) are representative of the Canadian population.
Conclusions
Our findings indicate that the most predominant correlates of abuse are socioeconomic disadvantage and psychosocial risk, including poverty, age under 20 years, single marital status, stressful life events, and perceived stress. Policies and practices that promote screening for current abuse and evaluation of contextual factors (such as socioeconomic status and stressful life events) in order to identify women ‘at risk’ for abuse during the prenatal and postnatal period are warranted.
References
Spivak, H. R., Jenkins, L., VanAudenhove, K., et al. (2014). CDC grand rounds: A public health approach to prevention of intimate partner violence. Morbidity and Mortality Weekly Report, 63(2), 38–41.
McFarlane, J., Maddoux, J., Cesario, S., et al. (2014). Effect of abuse during pregnancy on maternal and child safety and functioning for 24 months after delivery. Obstetrics and Gynecology, 123(4), 839–847. doi:10.1097/AOG.0000000000000183.
Howard, L. M., Oram, S., Galley, H., et al. (2013). Domestic violence and perinatal mental disorders: A systematic review and meta-analysis. PLoS Medicine, 10(5), e1001452. doi:10.1371/journal.pmed.1001452.
Urquia, M. L., O’Campo, P. J., Heaman, M. I., et al. (2011). Experiences of violence before and during pregnancy and adverse pregnancy outcomes: An analysis of the Canadian Maternity Experiences Survey. BMCPregnancyChildbirth, 11, 42. doi:10.1186/1471-2393-11-42.
Janssen, P. A., Heaman, M. I., Urquia, M. L., et al. (2012). Risk factors for postpartum depression among abused and nonabused women. American Journal of Obstetrics and Gynecology, 207(6), 489 e1–489 e8. doi:10.1016/j.ajog.2012.09.022.
Beydoun, H. A., Beydoun, M. A., Kaufman, J. S., et al. (2012). Intimate partner violence against adult women and its association with major depressive disorder, depressive symptoms and postpartum depression: A systematic review and meta-analysis. Social Science and Medicine, 75(6), 959–975. doi:10.1016/j.socscimed.2012.04.025.
Bailey, B. A. (2010). Partner violence during pregnancy: Prevalence, effects, screening, and management. International Journal of Women’s Health, 2, 183–197.
Beydoun, H. A., Tamim, H., Lincoln, A. M., et al. (2011). Association of physical violence by an intimate partner around the time of pregnancy with inadequate gestational weight gain. Social Science and Medicine, 72(6), 867–873. doi:10.1016/j.socscimed.2011.01.006.
Moraes, C. L., Amorim, A. R., & Reichenheim, M. E. (2006). Gestational weight gain differentials in the presence of intimate partner violence. International Journal of Gynecology & Obstetrics, 95(3), 254–260. doi:10.1016/j.ijgo.2006.08.015.
Shah, P. S., & Shah, J. (2010). Maternal exposure to domestic violence and pregnancy and birth outcomes: A systematic review and meta-analyses. Journal of Women’s Health, 19(11), 2017–2031. doi:10.1089/jwh.2010.2051.
Sharps, P. W., Laughon, K., & Giangrande, S. K. (2007). Intimate partner violence and the childbearing year: Maternal and infant health consequences. Trauma Violence Abuse, 8(2), 105–116.
Gazmararian, J. A., Lazorick, S., Spitz, A. M., et al. (1996). Prevalence of violence against pregnant women. JAMA, 275(24), 1915–1920.
Public Health Agency of Canada. (2008). Aboriginal women and family violence. Ottawa: National Clearinghouse on Family Violence.
World Health Organization. (2005). Summary report: WHO multicountry study on women’s health and domestic violence against women. Switzerland: World Health Organization.
Janssen, P. A., Holt, V. L., Sugg, N. K., et al. (2003). Intimate partner violence and adverse pregnancy outcomes: A population-based study. American Journal of Obstetrics and Gynecology, 188(5), 1341–1347.
Stewart, D. E., & Cecutti, A. (1993). Physical abuse in pregnancy. CMAJ, 149(9), 1257–1263.
James, L., Brody, D., & Hamilton, Z. (2013). Risk factors for domestic violence during pregnancy: A meta-analytic review. Violence and Victims, 28(3), 359–380.
Salmon, D., Baird, K. M., & White, P. (2013). Women’s views and experiences of antenatal enquiry for domestic abuse during pregnancy. Health Expectations. doi:10.1111/hex.12060.
Renker, P. R., & Tonkin, P. (2006). Women’s views of prenatal violence screening: Acceptability and confidentiality issues. Obstetrics and Gynecology, 107, 348–354. doi:10.1097/01.AOG.0000195356.90589.c5.
Anderson, B. A., Marshak, H. H., & Hebbeler, D. L. (2002). Identifying intimate partner violence at entry to prenatal care: Clustering routine clinical information. Journal of Midwifery & Women’s Health, 47(5), 353–359.
Yelland, J., & Brown, S. J. (2014). Asking women about mental health and social adversity in pregnancy: Results of an Australian population-based survey. Birth, 41(1), 79–87. doi:10.1111/birt.12083.
O’Reilly, R., Beale, B., & Gillies, D. (2010). Screening and intervention for domestic violence during pregnancy care: A systematic review. Trauma, Violence, & Abuse, 11(4), 190–201. doi:10.1177/1524838010378298.
Rabin, R. F., Jennings, J. M., Campbell, J. C., et al. (2009). Intimate partner violence screening tools: A systematic review. American Journal of Preventive Medicine, 36(5), 439–445. doi:10.1016/j.amepre.2009.01.024.
Goodwin, M. M., Gazmararian, J. A., Johnson, C. H., et al. (2000). Pregnancy intendedness and physical abuse around the time of pregnancy: Findings from the pregnancy risk assessment monitoring system, 1996–1997. PRAMS Working Group. Pregnancy Risk Assessment Monitoring System. Maternal and Child Health Journal, 4(2), 85–92.
Saltzman, L. E., Johnson, C. H., Gilbert, B. C., et al. (2003). Physical abuse around the time of pregnancy: An examination of prevalence and risk factors in 16 states. Maternal and Child Health Journal, 7(1), 31–43.
Muhajarine, N., & D’Arcy, C. (1999). Physical abuse during pregnancy: Prevalence and risk factors. Canadian Medical Association Journal, 160(7), 1007–1011.
Heaman, M. I. (2005). Relationships between physical abuse during pregnancy and risk factors for preterm birth among women in Manitoba. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 34(6), 721–731. doi:10.1177/0884217505281906.
Daoud, N., Urquia, M. L., O’Campo, P., et al. (2012). Prevalence of abuse and violence before, during, and after pregnancy in a national sample of Canadian women. American Journal of Public Health, 102(10), 1893–1901. doi:10.2105/AJPH.2012.300843.
Dzakpasu, S., Kaczorowski, J., Chalmers, B., et al. (2008). The Canadian Maternity Experiences Survey: Design and methods. Journal of Obstetrics and Gynaecology Canada, 30(3), 207–216.
Public Health Agency of Canada. (2006). What mothers say: The Canadian Maternity Experiences Survey. Ottawa: Public Health Agency of Canada.
Public Health Agency of Canada. (2009). What mothers say: The Canadian Maternity Experiences Survey. Ottawa: Public Health Agency of Canada.
Statistics Canada. (2007). Microdata user guide: Maternity experiences survey. Ottawa: Statistics Canada.
Statistics Canada. (1993). Canadian violence against women survey. Ottawa: Statistics Canada. http://www.statcan.gc.ca/cgi-bin/imdb/p2SV.pl?Function=getSurvey&SDDS=3896&lang=en&db=imdb&adm=8&dis=2-a1. Accessed June 17 2014.
Statistics Canada. (2006). Low-income cut-offs for 2005 and low income measure for 2006. Ottawa: Ministry of Industry.
Newton, R. W., & Hunt, L. P. (1984). Psychosocial stress in pregnancy and its relation to low birth weight. BMJ, 288(6425), 1191–1194.
Kingston, D., Heaman, M., Fell, D., et al. (2012). Factors associated with perceived stress and stressful life events in pregnant women: Findings from the Canadian Maternity Experiences Survey. Maternal and Child Health Journal, 16(1), 158–168. doi:10.1007/s10995-010-0732-2.
Brown, S. J., McDonald, E. A., & Krastev, A. H. (2008). Fear of an intimate partner and women’s health in early pregnancy: Findings from the Maternal Health Study. Birth, 35(4), 293–302.
Bowen, E., Heron, J., Waylen, A., et al. (2005). Domestic violence risk during and after pregnancy: Findings from a British longitudinal study. BJOG, 112(8), 1083–1089. doi:10.1111/j.1471-0528.2005.00653.x.
Cokkinides, V. E., & Coker, A. L. (1998). Experiencing physical violence during pregnancy: Prevalence and correlates. Family & Community Health, 20(4), 19–37.
Bullock, L., Bloom, T., Davis, J., et al. (2006). Abuse disclosure in privately and medicaid-funded pregnant women. Journal of Midwifery & Women’s Health, 51(5), 361–369.
Daoud, N., Smylie, J., Urquia, M., et al. (2013). The contribution of socio-economic position to the excesses of violence and intimate partner violence among aboriginal versus non-Aboriginal women in canada. Canadian Journal of Public Health, 104(4), e278–e283.
Wilson, D., de la Ronde, S., Brascoupe, S., et al. (2013). Health professionals working with First Nations, Inuit, and Metis consensus guideline. JOGC, 35(6), 550–558.
Boyer, Y. (2011). First Nations, Metis and Inuit health and the law: A framework for the future (Dissertation). Ottawa: University of Ottawa.
Almeida, C. P., Cunha, F. F., Pires, E. P., et al. (2012). Common mental disorders in pregnancy in the context of interpartner violence. Journal of Psychiatric and Mental Health Nursing. doi:10.1111/j.1365-2850.2012.01937.x.
Austin, M. P., & Marce Society Position Statement Advisory Committee. (2014). Marce International Society position statement on psychosocial assessment and depression screening in perinatal women. Best Practice & Research Clinical Obstetrics & Gynaecology, 28(1), 179–187. doi:10.1016/j.bpobgyn.2013.08.016.
US Preventive Services Task Force. (2013). Intimate partner violence and abuse of elderly and vulnerable adults: Screening. Rockville, MD: US Preventive Services Task Force.
World Health Organization-WHO. (2011). Intimate partner violence during pregnancy. Switzerland: World Health Organization.
Committee on Obstetric Pratice. (2015). The American College of Obstetricians and Gynecologists Committee Opinion No. 630. Screening for perinatal depression. Obstetrics and Gynecology, 125(5), 1268–1271. doi:10.1097/01.AOG.0000465192.34779.dc.
National Institute for Health and Care Excellence-NICE. (2014). Antenatal and postnatal mental health: Clinical management and service guidance, Contract No. 192. UK: NICE.
Austin, M. P., Highet, N., & the Guidelines Expert Advisory Committee. (2011). Clinical practice guidelines for depression and related disorders—anxiety, bipolar disorder and puerperal psychosis—in the perinatal period. A guideline for primary care health professionals. Melbourne: Beyondblue.
Charles, P., & Perreira, K. M. (2007). Intimate partner violence during pregnancy and 1-year post-partum. Journal of Family Violence, 22(7), 609–619.
Stewart, D. E., Gagnon, A. J., Merry, L. A., et al. (2012). Risk factors and health profiles of recent migrant women who experienced violence associated with pregnancy. Journal of Women’s Health, 21(10), 1100–1106. doi:10.1089/jwh.2011.3415.
Miszkurka, M., Zunzunegui, M. V., & Goulet, L. (2012). Immigrant status, antenatal depressive symptoms, and frequency and source of violence: What’s the relationship? Archives of Women’s Mental Health, 15(5), 387–396. doi:10.1007/s00737-012-0298-7.
Hyman, I., Forte, T., Du Mont, J., et al. (2009). Help-seeking behavior for intimate partner violence among racial minority women in Canada. Womens Health Issues, 19(2), 101–108. doi:10.1016/j.whi.2008.10.002.
Daoud, N., O’Campo, P., Urquia, M. L., et al. (2012). Neighbourhood context and abuse among immigrant and non-immigrant women in Canada: Findings from the Maternity Experiences Survey. International Journal of Public Health, 57(4), 679–689. doi:10.1007/s00038-012-0367-8.
Fanslow, J., Silva, M., Whitehead, A., et al. (2008). Pregnancy outcomes and intimate partner violence in New Zealand. Australian and New Zealand Journal of Obstetrics and Gynaecology, 48(4), 391–397. doi:10.1111/j.1479-828X.2008.00866.x.
Kita, S., Yaeko, K., & Porter, S. E. (2013). Prevalence and risk factors of intimate partner violence among pregnant women in Japan. Health Care for Women International. doi:10.1080/07399332.2013.857320.
McGuire, M., Cleary, B., Sahm, L., et al. (2010). Prevalence and predictors of periconceptional folic acid uptake—prospective cohort study in an Irish urban obstetric population. Human Reproduction, 25(2), 535–543. doi:10.1093/humrep/dep398.
American College of Obstetricians andGynecologists. (2012). Committee opinion no. 518: Intimate partner violence. Obstetrics and Gynecology, 119, 412–417.
Society of Obstetricians and Gynaecologist of Canada. (2011). Substance use in pregnancy. Journal of Obstetrics and Gynaecology Canada, 33(4), 367–384.
Coker, A. L., Garcia, L. S., Williams, C. M., et al. (2012). Universal psychosocial screening and adverse pregnancy outcomes in an academic obstetric clinic. Obstetrics and Gynecology, 119(6), 1180–1189. doi:10.1097/AOG.0b013e318253d76c.
Roelens, K., Verstraelen, H., Van, E. K., et al. (2008). Disclosure and health-seeking behaviour following intimate partner violence before and during pregnancy in Flanders, Belgium: A survey surveillance study. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 137(1), 37–42. doi:10.1016/j.ejogrb.2007.04.013.
McFarlane, J., & Parker, B. (1994). Abuse during pregnancy: A protocol for prevention and intervention. New York: March of Dimes Birth Defects Foundation.
Straus, M. A. (1979). Measuring intra family conflict and violence: The Conflict Tactics (CT) Scales. Journal of Marriage and the Family, 41(1), 13.
Austin, M. P., Colton, J., Priest, S., et al. (2011). The Antenatal Risk Questionnaire (ANRQ): Acceptability and use for psychosocial risk assessment in the maternity setting. Women Birth. doi:10.1016/j.wombi.2011.06.002.
Taft, A., O’Doherty, L., Hegarty, K., et al. (2013). Screening women for intimate partner violence in healthcare settings. Cochrane Database of Systematic Reviews, 4, CD007007. doi:10.1002/14651858.CD007007.pub2.
O’Campo, P., Kirst, M., Tsamis, C., et al. (2011). Implementing successful intimate partner violence screening programs in health care settings: Evidence generated from a realist-informed systematic review. Social Science and Medicine, 72(6), 855–866. doi:10.1016/j.socscimed.2010.12.019.
Taillieu, T. L., & Brownridge, D. A. (2010). Violence against pregnant women: Prevalence, patterns, risk factors, theories, and directions for future research. Aggression and Violent Behavior, 15(1), 14–35. doi:10.1016/j.avb.2009.07.013.
Acknowledgments
This research was supported by funds to the Canadian Research Data Centre Network (CRDCN) from the Social Science and Humanities research Council (SSHRC), the Canadian Institute for Health Research (CIHR), and the Canadian Foundation for Innovation (CFI) and Statistics Canada. Although the research and analysis are based on data from Statistics Canada, the opinions expressed do not represent the views of Statistics Canada or the Canadian Research Data Centre Network (CRDCN). The authors would like to acknowledge the members of the Maternity Experiences Study Group of the Public Health Agency of Canada’s Canadian Perinatal Surveillance System who were instrumental in the development of the MES and Statistics Canada for its collaboration with the Public Health Agency of Canada in the implementation of the MES. We would like to thank Erin Corston, former Director, Health and Environment, Native Women’s Association of Canada, for reviewing the manuscript for relevance to Aboriginal women’s health. Dr. Heaman received career support from a Canadian Institutes of Health Research (CIHR) Chair in Gender and Health award (2008–2013). Dr. Kingston receives career support from the Alberta Centre for Child, Family and Community Research (2013–2015) and a CIHR New Investigator Award (2015–2019). Dr. Urquia is supported by a CIHR New Investigator Award (2013–2018). Dr. O’Campo is supported by the Alma and Baxter Ricard Chair in Inner City Health. Dr. Janssen is supported by a career salary award from the Child and Family Research Institute. Dr. Smylie receives career support through a CIHR New Investigator Award in Knowledge Translation. No funding was received for this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that there is no conflict of interest.
Rights and permissions
About this article

Cite this article
Kingston, D., Heaman, M., Urquia, M. et al. Correlates of Abuse Around the Time of Pregnancy: Results from a National Survey of Canadian Women. Matern Child Health J 20, 778–789 (2016). https://doi.org/10.1007/s10995-015-1908-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-015-1908-6