
Abstract
A novel method for rapid radioanalytical measurement of uranium and plutonium in 100ml emergency urine samples was developed, through optimized selection of the separation and purification process and a combined measurement with ICP-TOF-MS and alpha spectrometry. The typical analytical time is within 6 h, the recovery rates are more than 80%, and the minimum detection activity concentrations are 3.4 × 10−4 Bq/L for 238U and 2.5 × 10−3 Bq/L for 239Pu respectively. The spiked test shows that this method can be used for quantitative evaluation of the activity concentration of 238U and 239Pu in urine samples accurately.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
A large nuclear accident following nuclear facilities or nuclear weapons might release a large amount of uranium, plutonium and other radioactive isotopes to air, and lead to a large number of people’s inner exposure [1]. 238U (T1/2 = 4.47 × 109 y) and 239Pu (T1/2 = 2.41 × 104 y) isotopes are mostly important isotopes due to their alpha emitter, high chemical toxicity and relatively long half-life, while the rapid evaluation and accurate measurement of internal exposure caused by uranium and plutonium isotopes have attracted widespread attention in recent years [2]. Typically, for the public intake of natural uranium from food and drink, the urinary uranium level is nearly 6 × 10−5Bq/L [3]. During a nuclear emergency, rapid radiochemical analysis of urine from contaminated people has become an essential part of radiobiological verification [4]. Different national standards have different requirements for the isotope analysis of urine samples. In the American National Standard, the Minimum Testing Level (MTL) for 239Pu and 238U is 10 mBq/L for indirect radiobioassay performance testing [5], while the Minimum Detection Activity (MDA) is 1m Bq/L for 239Pu and 10 mBq/L for 238U in China national standard [6]. The indirect bioassay means in vitro bioassay monitoring including analysis of nasal swabs, urine samples, fecal samples, blood, and tissue specimens, which is different from direct (in vivo) monitoring including whole-body counting, chest (lung) counting, and special organ or tissue counting [4]. Li provided a reference level (RL) for an emergency bioassay of adult urinary excretion samples which is taken on the third day after acute exposure, while the RLs are 3.4 × 10−3 Bq/L for 239Pu and 3.6 × 10−2 Bq/L for 238U with the reference dose 0.1Sv [7].
In order to realize the radioanalytical measurements of uranium and plutonium isotopes in urine samples, different methods have been developed based on different preparation, separation progress as well as different measurement systems. In 2001, Thakkar et al. first reported a method for the analysis of U, Pu, and Am in 1.2 L urine samples with UTEVA stacked with TRU resins, the recoveries of different isotopes were ranged from 70 to 105%, and the separation and purification time was nearly 2.5 h [8]. Maxwell et al. developed a rapid and reliable method for the analysis of actinides and Sr in urine, where a stack of TEVA, TRU, and Sr resins was used for separation. Alpha spectrometry system and low background gas proportional counter were used for measurement, with the recoveries of both nuclides nearly 100% and the sequential separation and analysis of the samples within 8 h [9,10,11]. In 2009, a more efficient pre-treatment method was proposed to fit the combined measurement of ICP-MS and alpha spectrometer, which realized the simultaneous extraction of 24 samples in nearly 3 h [12]. In 2011, Dai et al. developed a rapid urinary analysis method for emergency bioassay of actinides including Pu, U and Am/Cm isotopes at the same time, where HTiO co-precipitation and AGMP-1, UTEVA and DGA-N resins as well as alpha spectrometer are used, and MDA of 20 mBq/L with an 8-h sample turnaround time are realized [13]. In 2018, Vasile et al. improved Maxwell's method by using a combination of TEVA and TRU resins and lower acidity to avoid contamination, and finally reduce the sample turnaround time to 2 h [14].
To meet the requirement of rapid evaluation of uranium and plutonium nuclides inner exposure during a nuclear emergency, a new rapid radiochemical analysis of urine samples has been developed with simultaneous isotopes separation and combined measurement with ICP-TOF-MS as well as alpha spectrometry in our laboratory. The procedures of sample pretreatment and nuclide separation were optimally selected through comparison experiments, the recovery and the accuracy were carefully evaluated in detail, and a series of verification experiments were carried out with spiked samples.
Materials and methods
Basic procedures
The basic procedure of the rapid radiochemical analysis method is divided into three steps: sample preparation, nuclide separation and analytical measurement. Sample preparation involves acidification, co-precipitation, and digestion. Nuclide separation includes valence adjustment, adsorption and desorption processes. During analytical measurement, different instruments are usually used for different nuclide isotopes.
The synthetic urine sample with a standard matrix formulation from ANSI is used in this paper [5], the main components are water, urea, sodium sulfate, potassium chloride, creatinine, other inorganic and organic substances. The reagents used in the experiments including HCl, HF, H2O2, sulfamic acid, ascorbic acid, hydroxylamine hydrochloride, NaNO2, TiCl3, ammonium hydrogen oxalate and Ce(NO3)3 are all analytical pure grade (Aladdin, China). Nitric acid was Trace Metal grade (Fisher Scientific, Inc., USA). The water used in the experimental process was all ultrapure grade produced by LDL-III-30 (Ludao Corp., China). The TEVA, TRU and UTEVA resins all have a particle size of 100–150 μm (Triskem International Corp., France), and 2 ml cartridges are used in this paper. Uranium standard solution purchased from China National Institute of Metrology, while the proportion of 238U to total uranium is 0.997. The 239Pu standard solution was a certified reference material (CRM) purchased from National Institute of Standard and Technology (NIST, Gaithersburg, USA), and the 242Pu as well as 233U standard solution was purchased from National Physical Laboratory (NPL, Teddington, UK), which are CRM with certificate of calibration. The standard solutions were first diluted and prepared to different intermediate concentrations during experiments. The solid-phase extraction systems used for the separation process were purchased from Triskem with 12 as well as 24 channels separately. The measurement instrument for Uranium was an Optimass 9500 ICP-TOF-MS (GBC, Australia) which is combined with an inductively coupled plasma ion source and a time-of-flight mass analyzer, and can realize full-spectrum detection at full mass (1–260 amu) with a high isotopic resolution of nearly 0.001 amu. An SDS270 automatic sampler is used to inject samples through a peristaltic pump and an atomization device, which is a cyclone spray chamber with a concentric nebulizer and argon is used as the carrier gas. The detection limit is nearly 10 ng/L for 238U. The measurement instrument for Plutonium was an 8 channels alpha spectrometry system, model ORTEC ALPHA-ENSEMBLE-8 (Ametek, Ortec Division, Oak Ridge, TN), the low background counting rate in the region of interesting of 239Pu is nearly 0.15 counts per day(cpd).
Optimized selection of each progress
Co-precipitation
Co-precipitation is a very rapid and effective method for enrichment of nuclides in urine samples. In order to find more optimal methods, two most frequently used calcium phosphate [15] and HTiO [16] co-precipitation methods were compared in this paper. The calcium phosphate method is performed by adding 1.25 M Ca(NO3)2 and 3.2 M H3PO4 to the samples, while the HTiO method is performed by adding 20%wt TiCl3 and NH3·H2O to the samples, which are also shown in Table 1.
Eight 100 mL urine samples were prepared, four samples were added with 1.24 × 10−2 Bq 238U and the other four were added with 0.165 Bq 239Pu. For calcium phosphate co-precipitation, four samples with separate U/Pu were mixed with 1 mL 1.25 M calcium nitrate and 3 mL 3.2M phosphoric acid, and then adjusted to pH 9.5 with concentrated ammonia. For HTiO co-precipitation, four samples were mixed with 2 mL 20%wt TiCl3, and then adjusted to pH 7 with concentrated ammonia. Then all samples were centrifuged at 8500 rpm for 5 min. Considering the measurement sensitivity of ICP-TOF-MS and the inference of large amounts of calcium to alpha spectrometry, the supernatants were used to evaluate the recovery of different coprecipitation methods. 238U in the supernatant was acidified to 1% nitric acid for ICP-TOF-MS measurements, and 239Pu in the supernatant was evaporated to dryness and dissolved in 2 M HNO3, then micro-precipitated and measured by alpha spectrometry. The recovery of the two nuclides by coprecipitation was calculated by volume correction and compared with added activity.
Valence adjustment
Before nuclides separation, it is needed to change the Pu to Pu (IV) and U to U(VI). The most commonly used is NaNO2 valence adjustment method [17], but also some other methods are used, such as using reductant first and then following oxidation. Different reductants used give different methods, including sulfamic acid mixed with ascorbic acid method or hydroxylamine hydrochloride method [9]. The NaNO2 method adjusts the valence by 4M NaNO2, while sulfamic acid mixed with ascorbic acid method adjusts the valence by 1.5M sulfamic acid + 1.5M ascorbic acid + 4M NaNO2, and the hydroxylamine hydrochloride method adjusts the valence by 3M Hydroxylamine hydrochloride + 4M NaNO2. All those methods are also shown in Table 2.
For comparing different valence adjustment methods, 12 urine samples were prepared after pretreatment including co-precipitation and digest. Each 15 mL sample was added with 0.165 Bq 239Pu and 1.24 × 10−2 Bq 238U, and then separated into three groups, 1 mL 4M NaNO2, 0.5 mL 1.5M sulfamic acid + 1.25 mL 1.5M ascorbic acid + 1 mL 4M NaNO2, 0.5 mL 3M Hydroxylamine hydrochloride + 1 mL 4M NaNO2 was added separately and then stirred at 40 ℃ for 10 min. All 12 solutions were separated with TEVA and TRU resin column, and separately eluted with 20 mL 0.1M HCl-0.05M HF-0.03M TiCl3 for 239Pu and 15 mL 0.1M Ammonium hydrogen oxalate for 238U. The eluted solutions were then separately measured by ICP-TOF-MS and alpha spectrometry, and the recovery of different adjustment methods was compared.
Resin selection and elution condition
Considering most commonly used resin, TEVA resin was usually selected for Pu separation and TRU or UTEVA was selected for U separation recently [8, 10]. Different elution condition usually gives different recovery rate. For optimized nuclides separation of our method, TEVA resin was selected for Pu but two different elution conditions were compared including 20 mL 0.1M HCl-0.05M HF-0.03M TiCl3 [12] and 20 mL 0.1M HCl-0.05M HF-0.05M NH2OH·HCl [14]. For U, two different resins combined with different eluent methods were compared through experiments, which are 15 mL 0.1M Ammonium hydrogen oxalate eluent [11] and 15 mL 0.03M H2C2O4-0.1M HCl eluent [18] for TRU resin, and also 15 mL 0.1M HCl eluent [19] and 15 mL 0.01M HNO3 eluent [20] for UTEVA resin.
During comparison experiments, 24 urine samples with 15 mL volume after pretreated by co-precipitation, digest and valence adjustment. 8 samples were added with 0.165 Bq 239Pu and loaded on TEVA resins, and then divided into two groups to elute with two different methods. The other 16 samples were added with 1.24 × 10−2 Bq 238U. Among them, 8 samples were loaded on TRU resins and 8 samples on UTEVA resins. The 238U on different resins were separated into 4 groups and eluted with above methods. U/Pu was separately measured and the recovery rates were compared simultaneously.
The recovery and MDAs
After optimized selection of sample pretreatment progresses and control conditions, the final design of our measurement method for uranium and plutonium in urine samples is shown in Fig. 1, where the typical analytical time of each progress is also given.

Flow chart and timescale of the rapid radiochemical analysis for urine sample
The optimized procedure used calcium phosphate co-precipitation, the valence states of uranium and plutonium were adjusted by sulfamic acid, ascorbic acid, and sodium nitrite together, and the combined TEVA + TRU resin columns are used. After rinsing and sample loading, the TEVA and TRU resins were separated and eluted simultaneously. After source preparation, 238U was measured by ICP-TOF-MS, and 239Pu was measured by alpha spectrometry. It’s worth noting that the spiked 242Pu and 233U are not always needed if the operational progress is reliable and the recovery rate remains stable. But sometimes it also could be added one or two isotopes to help confirm results or the recovery rate during actual sample measurement as a spiked sample.
The total time of sample preparation as well as nuclide separation is within 4 h, and the typical measurement is nearly 2 h, so the whole analytical time is usually within 6 h.
The whole method’s recovery and accuracy were checked carefully through experiment and the minimum detection activities of 238U/239Pu were evaluated through calculation. For the recovery rate estimation, 12 standard urine samples with 100ml were prepared with 0.165 Bq 239Pu and 1.24 × 10−2 Bq 238U added. Each sample was dealt with under the standard procedure, all the elution solutions were carefully treated and measured. For 238U, the mass concentration \(C_{x}\) (ng/ml) is given by ICP-TOF-MS after calibrating with a series of prepared standard solutions and corrected by internal standard addition, then the recovery rate (Yi) could be as follow:
where the \(V\) is the volume of urine sample (= 100 mL); \(f\) is the factor for converting mass concentration to activity (= 1.24 × 10–5 Bq/ng); and \(A_{0}\) is the initial added 238U activity (= 1.24 × 10–2 Bq).
For 239Pu, the net counting rate in region of interesting \(n_{x}\) is given by the alpha spectrometry and the recovery rate (YA) could be as follow:
where the \(\varepsilon\) is the detection efficiency(dimensionless), which is calibrated with a standard electroplated Am-Pu source; \(A_{0}\) is the initial added activity of 239Pu (= 0.165 Bq).
Assuming that the measurement sensitivity of ICP-TOF-MS (\(S\)), the recovery rate (\(R\)) of 238U and 239Pu as well as the detection efficiency (\(\varepsilon\)) are constant. The minimum detection activity concentration(MDA) of this method could be calculated using the following equation [21]:
where \(\sigma_{B}\) is the average background rate of ICP-TOF-MS with ten blank samples, which is gotten from the blank urine samples undergoing the whole procedure and is nearly 10ng/L. \(S\) is the measurement sensitivity, which is nearly 6.8 × 104 cps/ng/ml during measurement. \(R\) is the recovery rate of 238U and 239Pu. \(bg\) is the background counts rate of alpha spectrometry system (= 0.15 cpd), and T is the sample measurement time (h).
Comparison experiments
For verification, combined comparison experiments were carried out with 10 blind urine samples. Each two samples was added with different 238U and 239Pu isotopes, which are the MDA level of China national standard (MDAL) [6], the Minimum Testing Level (MTL) of ANSI [5], the Reference Level (RL) from Li’s paper [7], and 10 times of MTL as well as 10 times of RL. Due to the missing of 233U, only 242Pu was spiked for confirming results and the recovery rate, each sample is added with nearly 0.2 Bq. The measurement results were compared with preset concentrations, and the related bias was obtained through calculation.
Results and discussion
Comparison results of different progress
Co-precipitation
The comparison results of the recovery of 238U and 239Pu under different co-precipitation methods are shown in Table 1. Results show that Calcium phosphate co-precipitation gave a recovery of 97.9 ± 0.1% for 238U and 97.7 ± 0.1% for 239Pu. HTiO co-precipitation gave a recovery of 96.8 ± 0.1% for 238U and 97.6 ± 0.5% for 239Pu. Both methods show good enrichment of uranium and plutonium in urine samples, and without significant difference in recovery rates. Calcium phosphate is the most commonly used co-precipitation method as the urine matrix contains a certain amount of calcium ions and phosphate ions itself, so it has been proposed to use the ions in the matrix together with the appropriate amount of reagents to generate co-precipitation [22]. Considering without new ions, calcium phosphate co-precipitation was chosen as our pre-concentration method.
Valence adjustment
The comparison results of the recovery rates of 238U and 239Pu under three different valence adjustment methods are shown in Table 2. The average recovery rates of 238U by the three methods are 83.1 ± 8.0%, 86.6 ± 7.7%, and 86.6 ± 2.7%, respectively, while the recoveries of 239Pu are 94.6 ± 7.8%, 95.3 ± 2.2%, and 89.4 ± 4.5%, which are a little higher than 238U. Ideally, all of three methods are capable for adjusting U to U(VI) and Pu to Pu (IV). Taking into account of the recovery rates and stability of different nuclides, the second method 0.5 mL 1.5M sulfamic acid + 1.25 mL 1.5 M ascorbic acid + 1 mL 4M NaNO2 was chosen for our method.
Resin and elution
The comparison results of different eluents for three resin columns are shown in Table 3. The recovery of 239Pu from TEVA resin column is 95.2 ± 2.6% by using 20 mL of 0.1M HCl-0.05M HF-0.03M TiCl3 eluent, and 93.7 ± 2.9% by using 20 mL of 0.1M HCl-0.05M HF-0.05M NH2OH-HCl eluent, which seems no big difference. The more stable 20 mL 0.1 M HCl-0.05M HF-0.03M TiCl3 eluent has been chosen finally for our method.
The recovery of 238U is 85.7 ± 0.6% when the TRU resin column is eluted with 15 mL of 0.1 M Ammonium hydrogen oxalate, and 34.3 ± 16.2% when the column is eluted with 15 mL of 0.03 M H2C2O4-0.1 M HCl. The recoveries of 238U are 31.4 ± 1.5% by using 15 mL of 0.1 M HCl eluent and 72.1 ± 5.8% by using 15 mL of 0.01 M HNO3 eluent for the UTEVA resin column. The 0.01 M HNO3 eluent method seems to be better than the 0.1 M HCl eluent method for UTEVA resin, but neither eluent method of UTEVA resin is better than the 0.1 M ammonium hydrogen oxalate eluent of the TRU resin. So, the 0.1M Ammonium hydrogen oxalate eluent method and the TRU resin column were chosen for better recovery and stability.
The recovery and repeatability
After careful evaluation, the recovery rates of 239Pu and 238U for the whole procedure are shown in Table 4. Results show that the recovery of 239Pu varies from 81.8 to 99.7% with an average value of 86.1 ± 5.7%, and the precision is 6.6%. The recovery of 238U varied from 80.0 to 88.4% with an average value of 84.7 ± 2.3%, and the precision is 2.7%. Those recovery rates are higher than Dai’s 50–55% [13] but a little lower than Maxwell's nearly 100% [11]. Taking into account the uncertainty of measurement system, this recovery stability seems could be accepted for rapid radiochemical analysis of a large number of samples during an emergency. For routine laboratory analysis or single sample analysis, the 233U and 242Pu tracer are recommended to be added, in order to improve the measurement accuracy further.
Using the recovery rates and Eqs. (3–4), the minimum detection activity concentration could be obtained, which is nearly 3.4 × 10–4 Bq/L for 238U, while 2.5 × 10–3 Bq/L for 239Pu with a typical counting interval of 2 h. The MDA of 239Pu could be improved by a longer counting time if needed. The MDA of 238U is quite lower than that of the reference level in Li’s paper, which is 3.6 × 10–2 Bq/L [7], and lower than the MDA level of China national standard 1.0 × 10–2 Bq/L [6]. The MDA of 239Pu is a little bit lower than the reference level in Li’s paper 3.4 × 10–3 Bq/L [7], but higher than the MDA level of China national standard, which is 1.0 × 10–3 Bq/L [6]. Different from routine measurement just as the China national standard requires, the emergency measurement needs more rapid analysis, and then the MDAs of this method could be accepted for measurement during an emergency.
Verification measurement
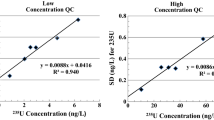
Verification measurement was carried out with ten urine samples mixed with a certain 238U and 239Pu, and 242Pu tracer was also added. The comparison results of 238U and 239Pu are separately shown in Tables 5 and 6, where the different reference levels and added activities are also shown. The measurement results were calculated with an average recovery rate of 84.7% for 238U and 86.1% for 239Pu. Results show that those measurement results are nearly in accordance with added activities at different concentrations. For 238U, the biases ranged from −11.5% to 9.8%, with an average of −3.94 ± 6.64%. For 239Pu, the biases ranged from −30.1% to 8.4%, with an average of −4.4 ± 13.35%. The Root Mean Squared Error (RMSE) for 238U and 239Pu were 7.72% and 14.05%, and within the 25% specified in ANSI/HPS N13.30–2011 standard [5], which indicated that there is a good agreement among those measurement results. Among these results, we also find some negative bias for some samples. The main reasons come from statistical errors and the slightly inhomogeneous distribution of source during the co-precipitation process. One result should be pointed out that the 239Pu activity concentration in MDAL is quite low, a much longer counting time is needed and the variety is relatively larger than others.
Compared the recovery rate of 242Pu tracer, the average value is 83.9 ± 2.7%, nearly in accordance with the former 86.1 ± 5.7%. Those recalculated results of 239Pu using each sample’s recovery have not so much difference with measured 239Pu results, which also indicated that this rapid analytical method could be used to measure uranium and plutonium activity concentration in urine samples accurately.
Conclusion
For rapid radioanalytical measurement of uranium and plutonium in urine samples, a new optimized method was proposed and carefully verified through a series of comparison experiments. 100 mL urine sample was pretreated by co-precipitation, digest, valence adjust, then nuclide separated by TEVA + TRU resins, and then measured by ICP-TOF-MS as well as alpha spectrometry. A stable recovery was gotten that 84.7 ± 2.3% for 238U and 86.1 ± 5.7% for 239Pu, and the low detection limit of this method was 3.4 × 10–4 Bq/L for 238U and 2.5 × 10–3 Bq/L for 239Pu. Verification results show that this method could be used to measure uranium and plutonium activity concentration in urine samples accurately.
Of course, a larger urine sample means higher accuracy and lower uncertainty. But large urine sample of more than 1L is hardly realized during an emergency, and larger sample usually lead to longer analytical time, which is not suitable for huge amount of samples analysis from nuclear accident. In the future, a more optimized method for large samples might be developed and a multi-channel automated nuclide separations system will be introduced to improve stability and reduce operation time.
References
ICRP (2020) Radiological protection of people and the environment in the event of a large nuclear accident: update of ICRP Publications 109 and 111. ICRP Publication 146. Ann ICRP 49(4):11–135
Rodríguez-Maese R, Ferrer L, Leal LO (2020) Automatic multicommuted flow systems applied in sample treatment for radionuclide determination in biological and environmental analysis. J Environ Radioactiv 223–224:106390
Centers for Disease Control and Prevention (2017) Biomonitoring summary uranium. https://www.cdc.gov/biomonitoring/Uranium_BiomonitoringSummary.html
Thakur P, Ward AL (2019) An overview of analytical methods for in vitro bioassay of actinides. Health Phys 116:694–714
ANSI/HPS N13.30–2011 (2011) Performance criteria for radiobioassy. Health Phys Soc
GBZ 129–2016 (2016) Specification for individual monitoring of occupational internal exposure. Nat Health Fam Plann Comm (In Chinese)
Li C, Vlahovich S, Dai X et al (2010) Requirements for radiation emergency urine bioassay techniques for the public and first responders. Health Phys 99:702–707
Thakkar AH (2001) Rapid sequential separation of actinides using Eichrom’s extraction chromatographic material. J Radioanal Nucl Chem 248:453–456
Maxwell SL (2008) Rapid analysis of emergency urine and water samples. J Radioanal Nucl Chem 275:497–502
Maxwell SL, Culligan BK (2009) New column separation method for emergency urine samples. J Radioanal Nucl Chem 279:105–111
Maxwell SL, Culligan BK (2009) Rapid separation method for emergency water and urine samples. J Radioanal Nucl Chem 279:901–907
Maxwell SL, Jones VD (2009) Rapid determination of actinides in urine by inductively coupled plasma mass spectrometry and alpha spectrometry: a hybrid approach. Talanta 80:143–150
Dai X, Kramer-Tremblay S (2011) An emergency bioassay method for actinides in urine. Health Phys 101:144–147
Vasile M, Jacobs K, Bruggeman M et al (2018) On the sequential separation and quantification of 237Np, 241Am, thorium, plutonium, and uranium isotopes in environmental and urine samples. Appl Radiat Isotopes 134:455–460
Zoriy MV, Pickhardt C, Ostapczuk P et al (2004) Determination of Pu in urine at ultratrace level by sector field inductively coupled plasma mass spectrometry. Int J Mass Spectrom 232:217–224
Wu Y, Xu Y, Xing S et al (2021) Rapid determination of ultra-trace plutonium in large volume of urine samples by tandem quadrupole inductively coupled plasma-mass spectrometry. Spectrochim Acta B 184:106259
Ridone S, Arginelli D, Berton G et al (2006) Radioanalytical determination of 239+240Pu and 241Am in bioassay samples by anion exchange and extraction chromatography: preliminary considerations about the two methods. Czech J Phys 56:195–207
Hang W, Zhu L, Zhong W et al (2004) Separation of actinides at ultra-trace level from urine matrix using extraction chromatography-inductively coupled plasma mass spectrometry. J Anal At Spectrom 19:966–972
Mcalister DR, Horwitz EP, Harvey JT (2011) Rapid methods for the isolation of actinides Sr, Tc And Po from raw urine. Health Phys 101:176–179
How EP, Dletz ML, Chlanzla R et al (2005) Separation and preconcentration of uranium from acidic media by extraction chromatography. Anal Chim Acta 266:25–37
Kumar R, Rao DD, Dubla R et al (2017) A rapid method for estimation of Pu-isotopes in urine samples using high volume centrifuge. Appl Radiat Isotopes 125:176–179
Kuwabara J, Noguchi H (2002) Development of rapid bioassay method for plutonium. J Radioanal Nucl Chem 2:273–276
Acknowledgements
We would like to thank the financial support of the National Natural Science Foundation of China (No. 12375319).
Funding
National Natural Science Foundation of China, 12375319, Lei Zhang.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Declarations
The authors declare that they have no competing financial interests or personal relationships.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Mei, L., Shao, H., Cui, L. et al. Rapid radiochemical analysis of uranium and plutonium in emergency urine samples. J Radioanal Nucl Chem 333, 1357–1365 (2024). https://doi.org/10.1007/s10967-024-09357-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10967-024-09357-1