
Abstract
Emerging adulthood (ages 18–25) is a period of identity exploration, particularly for young adults navigating the transition to post-secondary school. Little is known about how changes in identity exploration may be related to emerging adults’ mental health, or the role of social support plays in identity-related processes. In the present study, associations among identity exploration, internalizing symptoms, and perceived social support were examined. Participants included a diverse group of emerging adults (N = 1,125, Mage = 17.96 years) studying at a Canadian university. Random-intercept cross-lagged modeling demonstrated that within-person increases in exploration in breadth predicted fewer depressive symptoms over time, whereas within-person increases in exploration in depth predicted more depressive and anxious symptoms over time. A mediation effect from perceived support from significant other to depressive symptoms via exploration in breadth was also evident. Findings suggest that identity exploratory processes may be developmentally relevant in emerging adulthood, but their implications for mental health may differ. Perceived social support is also meaningfully related to identity exploration and mental health.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The process of attaining a coherent and synthesized sense of identity has long been underscored as a central developmental task during the transition to adulthood (Erikson, 1950). Identity development holds particular significance for emerging adults during the transition to post-secondary school, as this period, marked by opportunities and increased autonomy, encourages exploration across diverse domains (Arnett, 2000; Schwartz et al., 2011). However, this process of identity exploration may also evoke feelings of uncertainty and confusion, which have been linked to poorer well-being and mental health concerns (Crocetti et al., 2012; Crocetti et al., 2011; Hardy et al., 2013). Given that mental health issues are prevalent during emerging adulthood (Schwartz & Petrova, 2019), understanding the role of identity processes during this period is important. Longitudinal work that explores how emerging adults’ changing identity processes are associated with their mental health, are lacking. Further, although identity development is embedded within social contexts (Crocetti et al., 2022; Klimstra & Denissen, 2017), and social support has implications for mental health outcomes (Wang et al., 2018), the interplay among these factors has received little attention. To address these gaps in the literature, within-person effects in identity exploration processes, internalizing symptoms (i.e., depressive and anxious symptoms), and perceived social support were explored among emerging adults during the first-year of study in the present study.
Theoretical Framework
Several identity frameworks have been proposed based on the work of Marcia (1966) and Meeus (1996) (see van Doeselaar et al., 2018 for a review). In the present study, identity processes are defined based on the model proposed by Luyckx et al. (2006). According to this model, identity development can be grouped into two complementary cycles. In the commitment formation cycle (cycle 1), individuals may actively explore and consider potential identity alternatives with respect to their goals, values, and beliefs (i.e., exploration in breadth) prior to committing to one or more of the options considered (i.e., commitment making). In the commitment evaluation cycle (cycle 2), individuals actively manage their commitments by seeking additional information and comparing this new information to their own standards and values (i.e., exploration in depth). Although this evaluation process may be challenging for some individuals, it may eventually lead to feelings of certainty about the commitments and facilitate internalization (i.e., identification with commitment). However, some may return to the first cycle again to start another exploration. Others may become trapped in both cycles, wherein they continuously question and feel hesitant about their choices (i.e., ruminative exploration; Luyckx et al., 2008). As it is thought that emerging adults in college often have more exposure to different worldviews and opportunities to explore life alternatives (Arnett, 2000), the primary focus of this study was exploration in breadth, exploration in depth, and ruminative exploration. While exploration in breadth reflects one of the core processes of the commitment formation cycle, exploration in depth captures one aspect of the commitment evaluation cycle. Ruminative exploration further captures a more distressing from of exploration.
Theoretical frameworks on personality traits and psychopathology, including the vulnerability/predisposition and scar models (Klimstra & Denissen, 2017), may inform understanding of the nature between identity and mental health concerns among emerging adults. The vulnerability/predisposition model assumes a causal link between personality traits and psychopathology, such that individual differences in personality traits would increase risk of psychopathology (Durbin & Hicks, 2014). In contrast, the scar model proposes that the occurrence of psychopathology may alter an individual’s personality traits (Durbin & Hicks, 2014). These models suggest that personality traits may both influence, and be influenced by, an individual’s mental health (Durbin & Hicks, 2014). In the context of identity, the vulnerability model would suggest that individuals with identity struggles are at risk of experiencing mental health concerns (Klimstra & Denissen, 2017), such as depression and anxiety. Specifically, meaningful identity commitments may drive individuals to regulate themselves in the pursuit of self-relevant goals through providing a sense of direction, whereas healthy exploration of different identities may increase the likelihood of identifying solutions to uncertainties and information about possible alternatives (Waterman, 1993; Waterman, 2007). By pursuing self-relevant goals and having a clearer sense of self-relevant commitments, individuals may experience better mental health (Hofer et al., 2011; Waterman, 2007). For example, emerging adults who explore various student-led organizations may gain insights to career paths or life choices, which may mitigate the risks of poor mental health linked to feelings of uncertainty. In the same vein, those who experience more challenges in exploration may be less likely to benefit from the self-regulatory function provided by a committed identity (Crocetti, 2018). Accordingly, they may continue to struggle to identify a self-relevant identity; this stress, in turn, may hinder mental health.
By contrast, the scar model would suggest that an individual’s capacity to develop strong identity commitment would be hindered after experiencing internalizing symptoms (Klimstra & Denissen, 2017). A potential reason is that internalizing symptoms may reduce their sense of agency and motivation, which are needed to form strong commitments (Becht et al., 2018; Becht et al., 2019). Another reason is that internalizing symptoms may hinder executive functions, such as cognitive flexibility (i.e., changing perspectives, adapting to situations, solving unexpected problems) and selective attention (i.e., staying focused on task at hand and suppressing distractors; Morea & Calvete, 2021), which are needed to evaluate and make decisions (Schiebener et al., 2015). Given that identity development involves an interplay of exploration, evaluation, and decision-making (Crocetti, 2018), individuals with internalizing symptoms may struggle to make commitments or feel confused in the exploration process.
Identity Processes and Internalizing Symptoms
Although some cross-sectional work suggests that identity development is relevant to understanding mental health concerns among adolescents and emerging adults (Crocetti et al., 2011; Luyckx et al., 2008), longitudinal evidence on the link between identity and internalizing symptoms is limited. Moreover, previous research has largely focused on between-person differences (i.e., do individuals with greater exploration in breadth experience more distress than individuals lower in exploration in breadth?; Potterton et al., 2022). To clarify the link from a developmental perspective (e.g., how change in an individual’s identity is related to change in their mental health over time, and vice versa), emerging studies have adopted a within-person approach (Becht et al., 2019; Meca et al., 2019; Hatano et al., 2020). This approach can be used to capture an individuals’ fluctuations in both identity and mental health simultaneously over time, while considering between-person differences (Hamaker et al., 2015).
Extant studies that have adopted the within-person approach have been limited to adolescents, with inconsistent support for the scar and vulnerability/predispoistion models. For example, Meca et al. (2019) found support for both the scar and vulnerability/predisposition models, such that within-person increases in depressive symptoms among immigrant Hispanic adolescents (14–17 years old, Mage T1 = 14.51) in USA were associated with decreases in identity coherence (e.g., lower commitment) over time, and increases in identity coherence (e.g., commitment) were associated with decreases in depressive symptoms over time. In contrast, Becht et al. (2019) found that reconsideration of commitments and ruminative exploration predicted within-person increases in depressive symptoms across two Dutch samples from Netherlands (12–17 years old, Mage T1 = 14.03) and Belgium (12–21 years old, Mage T1 = 15.80), but not vice versa. Similarly, Hatano et al. (2020) found that ruminative exploration predicted within-person increases in depressive symptoms among adolescents aged 14 years old (T1) in Japan, supporting the vulnerability/predisposition model. Although these findings suggest that identity may have a stronger influence on mental health (than vice versa) at the within-person level, it is unclear whether these dynamics are also evident in emerging adults.
The Role of Social Support
Identity development is rooted from social relationships (Crocetti et al., 2022). Specifically, supportive relationships offer a secure base from which emerging adults can confidently experiment with different identities (Branje et al., 2021). In interacting with others, emerging adults may strengthen or modify their identity commitments, such as when they obtain social verification or lack thereof regarding their identity choices (Crocetti et al., 2022). In the same vein, individuals with a clearer sense of self (e.g., stronger identity commitment) may have better social relationships because they are able to navigate social contexts more effectively (Branje et al., 2021). For example, supportive parenting (e.g., autonomy support) has been found to predict changes in commitment making and exploration in breadth in Dutch emerging adults (19 years old at T1), while higher initial levels of identification with commitment and in-depth exploration predicted increased supportive parenting (Beyers & Goossens, 2008). Other studies involving adolescents from the Netherlands and USA also indicated longitudinal links between family support and identity processes at the between-person level (Crocetti et al., 2017; Pittman et al., 2012).
Comparatively, the literature on whether other social relationships (e.g., friends) are longitudinally related to emerging adults’ identity development is unclear. However, cross-sectional studies suggest that identity achievement is related to the quality of romantic relationship (e.g., companionship) but not friendship in emerging adults (Barry et al., 2009). Insights could also be gained from studies involving adolescents. For example, perceived balanced relatedness (e.g., autonomy support) from friends predicted reconsideration, and was predicted by in-depth exploration among Dutch adolescents (Mage = 14 years old at T1) (van Doeselaar et al., 2016). Therefore, although social support from different sources (e.g., family, friends, significant other) appear to be related to identity development in meaningful ways, empirical evidence on their longitudinal links at the within-person level and among emerging adults is limited. Differentiating these sources is critical because their implications may differ in emerging adulthood. Further, social support from friends and significant other (e.g., romantic partner) may become increasingly important during emerging adulthood as young adults gain greater autonomy and independence from their parents (Arnett, 2000).
Social relationships are also critical to mental health issues. For example, interpersonal theories of depression suggest a possible bidirectional association between social relationships and depressive symptoms (Hames et al., 2013). Corroboratively, extensive research suggests that individuals who perceive low levels of social support are at risk of experiencing mental health issues, such as depressive symptoms (see Wang et al., 2018 for a review). Adolescents and emerging adults with mental health issues also tend to perceive lower levels of social support over time (Needham, 2008; Stice et al., 2004). However, the extent to which different sources of perceived support predict or are predicted by mental health issues (e.g., depressive symptoms) in emerging adults at the within-person level have received little empirical support (Dawson & Samek, 2022). Thus, the association between social support and mental health issues was also considered in the present study.
Given that mental health issues have implications for identity processes (Klimstra & Denissen, 2017) and interpersonal relationships (Hames et al., 2013), both of which are also related (Crocetti et al., 2022), possible mediation effects may be evident. For example, a longitudinal study (T1-T3) involving first-year college students indicated that the effect of perceived social support on depressive symptoms was mediated by self-esteem; the association between self-esteem and depressive symptoms was also mediated by perceived social support (Lee et al., 2014). Therefore, both identity processes and social support were considered as mediators in the present study, including the association between identity processes and mental health via social support, and the association between social support and mental health via identity processes.
Gender Differences
To account for potential gender differences, gender was considered as a covariate. This consideration was necessary as females have greater predispositional vulnerability to depression and anxiety due to biological factors (e.g., limbic system hyperactivity) (Parker & Brotchie, 2010). Moreover, differences in identity development and perceived social support may emerge between male- and female-identifying individuals due to variations in socialization experiences (Beyers & Goossens, 2008), biological factors (Parker & Brotchie, 2010), and evolved psychological adaptations to socioecological contexts (Schmitt et al., 2017). For example, identity exploration involves searching for a path that aligns with one’s values and goals, which are often influenced by gender roles (Diekman et al., 2010; Hatano et al., 2022). Additionally, females are often socialized to prioritize and value social relationships (Leaper, 2015).
Current Study
Emerging adulthood is a crucial period marked by identity exploration, while also being a time when mental health issues are prevalent. However, within-person evidence on the link between identity processes and mental health concerns is limited to adolescents. Longitudinal evidence examining how within-person changes in social relationships relate to changes in identity processes and mental health issues is also limited despite possible links. Additionally, potential mediation effects within the interplay of identity processes, mental health issues, and social relationships have received little research attention. To address these gaps, the directionality and the developmental dynamic among identity exploratory processes (i.e., exploration in breadth and depth, and ruminative rumination), mental health (i.e., depressive and anxious symptoms), and perceived social support (i.e., from family, friends, and significant other) were examined in emerging adults at both between- and within-person levels. Additionally, mediation paths from identity processes to depressive and anxious symptoms via perceived social support, as well as from perceived social support to depressive and anxiousy symptoms via identity processes were examined. Bidirectional associations were expected among the identity processes, perceived social support from different sources, as well as depressive and anxious symptoms. Specifically, ruminative exploration would be more strongly associated with depressive and anxious symptoms compared to exploration in breadth and depth. Perceived social support would be associated with fewer depressive and anxious symptoms regardless of the source. Further, perceived social support would be associated with greater exploration in breadth and depth, but lower ruminative exploration. Mediating effects would be evident, such that identity processes would predict both depressive and anxious symptoms via perceived social support from different sources. Females would engage in greater ruminative exploration, experience more depressive and anxious symptoms, and perceive higher levels of social support overall.
Methods
Participants
Participants included 1,125 1st year undergraduate students at a large Canadian University (Toronto, Ontario) who participated in a longitudinal research study (September, 2018 – May, 2019) examining stress and coping among emerging adults who were transitioning to university. Participants were aged between 17–22 years (Mage = 17.96, SD = 0.69). Approximately 28% of participants described their gender identity as male, 71% as female, and 1% used another gender label. The majority of participants (84%) were heterosexual. The ethnic composition was 32% East Asian, 23 % South Asian, 21% White, 6% Arab or West Asian, 3% South East Asian, 3% Black, 1% West Indian, 2% Latin American, 4% Filipino, 0.1% Aboriginal, and 5% other (mixed ethnicity). At least 60% of participants had parents who received a university degree or higher. Participant demographics are representative of the population in Toronto. According to the Census Profile 2021, 55.7% of the population identified as belonging to a racialized group and 46.6% were immigrants (Statistics Canada, 2021).
Procedure
Participants were recruited at the same time through different means, including posters on campus, electronic advertisements (e.g., Facebook posts, course websites, student club list serves), and classroom announcements. Interested participants contacted the lab via email to determine their participation eligibility (i.e., currently enrolled in 1st year of university and lived in the surrounding area of the university). Each participant was assigned a unique identifier and was sent a Qualtrics link to a consent form and baseline survey. Participants were surveyed three times over one year, each four months apart. Each assessment point took approximately 40 min to complete. As a token of appreciation, participants were offered electronic gift cards (e.g., Amazon) in the amounts of $10 at T1, $15 at T2, and $20 at T3.
This study was approved by the University Ethics Board. All participants provided informed consent prior to each assessment point. Several steps were taken to minimize any discomfort participants might experience (no greater than those experienced in daily life) when responding to the survey. Participants could skip questions on the survey without penalty and could click on a “Feeling Distressed” button during the survey to access a list of local mental health resources and supports. Additionally, participants could withdraw from the study at any time. At the end of the survey, participants were asked to reflect and write about one good thing that happened to them on the previous day, which has been demonstrated to induce positive mood in previous studies (Seligman et al., 2005). Further, participants received a list of local mental health resources and supports, as well as a debriefing form with the principal investigator’s contact information.
Measures
Identity processes
Identity processes were measured using the Dimensions of Identity Development Scale (DIDS; Luyckx et al., 2008), which assessed commitment making, identification with commitment, exploration in breadth, exploration in depth, and ruminative exploration. The DIDS consists of 25 items (5 items for each process) that are rated on a scale from 1 = completely disagree to 5 = completely agree. Items for each identity process were averaged to form a composite score for that process. In this study, only the exploration processes were used (e.g., “I keep looking for the direction I want to take in my life”). The DIDS has demonstrated construct validity and good reliability among university students in different cultures (Luyckx et al., 2008; Schwartz et al., 2011). The internal consistency for each process was excellent at each wave: exploration in breadth (T1 = 0.88, T2 = 0.89, T3 = 0.90), exploration in depth (T1 = 0.83, T2 = 0.85, T3 = 0.84), and ruminative exploration (T1 = 0.81, T2 = 0.84, T3 = 0.83).
Depressive symptoms
Depressive symptoms were measured using The Center for Epidemiologic Studies Depression Scale Revised (CESD-R, Eaton et al., 2004). The CESD-R measures depressive symptoms as specified by the American Psychiatric Association (APA) Diagnostic and Statistical Manual, fifth edition (DSM-V) with 20 items (e.g., “When I’m upset, I believe that I will end up feeling very depressed”) on a frequency scale from 0 = not at all or less than one day to 4 = nearly every day for 2 weeks. This measure has been validated for use in ethnically diverse student samples (Van Dam & Earleywine, 2011). In this study, two items about suicidality were removed due to ethics. The internal consistency was excellent at each wave T1 = 0.92, T2 = 0.94, T3 = 0.95.
Anxious symptoms
Anxious symptoms were measured using the Generalized Anxiety Disorder-7 (GAD-7; Spitzer et al., 2006), which is a brief measure designed to screen for GAD based on the APA DSM-IV criteria. Participants were asked to rate how frequently the listed symptoms (e.g., worrying about different things) have occurred over the last 2 weeks from 0 = not at all sure to 3 = nearly every day. This measure has demonstrated good validity and reliability in ethnically diverse student samples (Sriken et al., 2022). The internal consistency was excellent at each wave, T1 = 0.90, T2 = 0.91, T3 = 0.92.
Perceived social support
Perceived social support was measured using the Multidimensional Scale of Perceived Social Support (MSPSS; Zimet et al., 1988), which assesses social support from family, friends, and significant other. Each source of support includes 4 items (12 items in total) that are rated on a scale from 1 = very strongly disagree to 7 = very strongly agree. Sample items for each source of support include “My family really tries to help me”, “I can count on my friends when things go wrong”, and “I have a special person who is a real source of comfort to me”. The MSPSS has demonstrated reliability and validity among young adults from different ethnic groups and gender identities (Kler et al., 2022). The internal consistency was good at each wave for social support from significant other, T1 = 0.94, T2 = 95., T3 = 0.96, friends, T1 = 0.94, T2 = 0.93, T3 = 0.95, and family members, T1 = 0.92, T2 = 0.92, T3 = 0.92
Missing Data
There was little missing data within each wave (less than 1%). Overall retention rate was strong, with 83% of participants completing all three waves, 10% completing two waves, and 7% completing only one wave. Missing data occurred due to two primary reasons, including missing data within wave (i.e., participants did not answer some questions) and missing data between waves (i.e., participants did not complete a wave). Little’s MCAR test was not significant, χ2(305) = 335.10, p = 0.11, suggesting that missingness may be completely at random. Regression analysis indicated that younger participants were more likely to complete more than one wave, b = −0.10, p < 0.001. Independent samples t-test indicated significant gender differences, t (1107) = −3.29, p < 0.001, in which females were more likely to complete all waves. Multivariate analysis of variance (MANOVA) indicated that participants who completed only one wave did not differ significantly from those who completed two or all waves on the key variables at each wave, ps = 0.09 to 0.98 at T1, 0.07 to 0.89 at T2, 08 to 0.97 at T3. Given that missingness seemed to be missing at random, missing data were estimated using the full information maximum likelihood (FIML) estimation method.
Analytical Plan
Preliminary analyses were conducted with SPSS 28. All modeling analyses were tested with Mplus 8.10 (Muthén and Muthén, 1998–2022). Longitudinal measurement invariance and between-group invariance (i.e., male- and female-identifying adults) were examined to ensure that the measured constructs were comparable over time and gender (see supplementary material for further details). Intraclass correlations (ICCs) for all key constructs were examined to evaluate if there would be sufficient within-person variances. ICCs indicate the proportion of between-person variance relative to the total variance.
To test the direction of associations among identity processes, depressive and anxious symptoms, as well as perceived social support at the within-person level, the random-intercept cross-lagged panel modeling (RI-CLPM) approach was used (Hamaker et al., 2015). Following the recommended model building sequence (Mulder & Hamaker, 2021), an unconstrained RI-CLPM model was first tested. This model estimated stability paths within each variable over time (i.e., autoregressive paths), associations between variables over time (i.e., cross-lagged paths, including all possible reciprocal associations among examined variables), T1 correlations, and correlated residuals (changes) at T2 and T3. Mediation paths were examined using bootstrapping (k = 5000). Bootstrapping with bias-corrected bootstrapped CIs follows a nonparametric resampling procedure that increases power and does not assume normality or large sample size (see Preacher et al., 2011; Preacher & Hayes, 2008).
Next, the unconstrained RI-CLPM model was compared against a nested traditional CLPM model (i.e., by constraining the variances of the random intercepts and their covariances to zero) to determine whether there were indeed stable between-person differences that needed to be accounted for. To examine whether the longitudinal associations among identity, depressive symptoms, anxious symptoms and perceived social support were invariant across waves, the unconstrained RI-CLMP was compared against a constrained model with all autoregressive paths, cross-lagged paths, and correlated changes (Times 2–3) constrained to be equal across waves. Separate analyses were conducted for depressive and anxious symptoms to simply the model and in light of their strong correlation (r = 0.74). As models with constrained stability and cross-lagged paths are more desirable due to parsimony in CLPM and RI-CLPM (Orth et al., 2021), constrained models were used as much as possible. In all models, gender (0 = male-identifying, 1 = female-identifying) was treated as a time-invariant covariate predicting all observed variables within each wave. As only a very small percentage of participants identified as gender identities other than male and female (1%), they were excluded from analyses to obtain a more balanced gender ratio to understand gender differences. Additionally, age (T1) was treated as a covariate due to its association with missingness.
Several indices were used to evaluate model fit, including the comparative fit index (CFI), the root-mean-square error of approximation (RMSEA), and the standardized root-mean-square residual (SRMR). CFI values ≥ 0.90, RMSEA ≤ 0.08, and SRMR ≤ 0.08 would indicate acceptable model fit (Byrne, 2013). A significant chi-square difference (Δχ2), ΔCFI > 0.01 and ΔRMSEA > 0.015 would indicate variability in the developmental process during the time span of the study.
Results
Descriptive statistics and correlational results are presented in Table 1. In general, exploration in breadth was associated positively with exploration in depth, ruminative exploration, and different sources of social support within and across waves. Exploration in depth was associated positively with ruminative exploration and social support, but negatively with depressive symptoms within and across all waves. Ruminative exploration was associated positively with depressive and anxious symptoms, but negatively with social support within and across waves. Depressive and anxious symptoms were positively associated within and across waves. Additionally, both depressive and anxious symptoms were negatively associated with social support within and across waves.
Measurement Invariance
Longitudinal and between group invariance were examined to determine whether key constructs were invariant over time and between male- and female-identifying adults. Although longitudinal MI and gender invariance were established for all key constructs based on recommended cutoffs, depressive symptoms and identity processes demonstrated poor fits based on CFI (see supplementary material). However, they demonstrated acceptable fits as indicated by RMSEA and SRMR, along with the observation of strong factor loadings.
RI-CLPM
The ICCs for the key constructs indicated that approximately of 50% - 66% of variances were explained by between-person differences. In other words, approximately 34% - 50% of variances were due to fluctuations within persons. For both depressive and anxious symptoms models, the unconstrained RI-CLPM model had excellent fit. As presented in Table 2, this model improved model fit compared to the nested traditional CLPM, reinforcing ICC values that there were stable between-person differences that needed to be accounted for. Hence, the unconstrained RI-CLPM models were retained. Next, these unconstrained models were compared against constrained models to determine if the associations among variables were time invariant. Results indicated that the constrained model did not worsen model fits based on ΔCFI <0.01 and ΔRMSEA <0.015 (see Table 2) for both depressive and anxious symptoms models, suggesting that constraints were tenable due to time-invariant processes across waves (Mulder & Hamaker, 2021). Thus, the constrained RI-CLPM models were retained for both depressive and anxious symptoms models.
Depressive Symptoms Model
Between-person effects were captured by the covariances among random intercepts (see Table 3). Higher levels of trait-like exploration in breadth were associated with higher levels of trait-like exploration in depth, ruminative exploration, support from significant other, family, and friends. Higher levels of trait-like exploration in depth were associated with higher support from significant other, family, and friends, as well as lower levels of depressive symptoms. Higher levels of trait-like ruminative exploration were associated with higher levels of trait-like depressive symptoms, but lower levels of perceived social support from significant other, family and friends. Higher levels of trait-like depressive symptoms were associated with lower levels of support from significant other, family, and friends. Higher levels of trait-like support from significant other were associated with higher levels of trait-like support from family and friends. Additionally, higher levels of trait-like support from family were associated with higher levels of trait-like support from friends.
Within-person covariances among the construct residuals are presented in Table 4.
At times when individuals explored in breadth greater than typical levels, they also explored in depth greater than typical levels (T1-T3), as well as greater than typical levels of ruminative exploration (T2-T3), and support from significant other, family, and friends at T1- T3. Additionally, at times when individuals explored in depth greater than typical levels, they also engaged in greater than typical levels of ruminative exploration (T2-T3), and received greater support from significant other (T2-T3), friends (T1-T3), family (T1-T3). Across T1-T3, at times when individuals engaged in greater than typical levels of ruminative exploration, they also experienced greater than typical levels of depressive symptoms (T1-T3). At times when individuals experienced greater than typical levels of depressive symptoms, they also perceived lower than typical levels of support from significant other (T2-T3), as well as family and friends (T1-T3). Across T1-T3, at times when individuals perceived greater than typical levels of support from significant other, they also perceived greater than typical levels of support from family and friends. Similarly, at times when individuals perceived greater than typical levels of support from family, they also perceived greater than typical levels of support from friends (T1-T3).
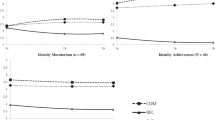
Auto-regressive and cross-lagged paths are presented in Fig. 1. Only one significant auto-regressive path was found for depressive symptoms at T1 ➔ T2, and T2 ➔ T3. In terms of cross-lagged paths, stronger support from significant other at T1 and T2 predicted within-person increases in exploration in breadth at T2 and T3. Similarly, higher exploration in breadth at T1 and T2 predicted within-person increases in support from significant other at T2 and T3 respectively. Higher exploration in breadth at T1 and T2 respectively predicted within-person decreases in depressive symptoms at T2 and T3. Higher exploration in depth at T1 and T2 predicted within-person increases in depressive symptoms at T2 and T3 respectively. Higher depressive symptoms at T1 predicted within-person decreases in support from family and friends at T2; this pattern was also found between T2-T3. A significant mediation effect was found, in which support from significant other (T1) predicted within-person increases in exploration in breadth (T2), which in turn, predicted within-person decreases in depressive symptoms (T3), β = −0.01, 90% CI [−0.04, −0.003].

Random intercept cross-lagged panel model (depressive symptoms model).
Anxious Symptoms Model
Between-person effects for the anxious symptoms model were similar to those in the depressive symptoms model (see Table 5). Identity processes were associated with social support in similar ways as the depressive symptoms model. Trait-like exploration in breadth and depth were not associated with trait-like anxious symptoms, but higher trait-like ruminative exploration was associated with higher trait-like anxious symptoms. Higher levels of trait-like anxious symptoms were associated with lower levels of trait-like support from significant other, friends, and family.
In terms of within-person covariances (see Table 6), identity processes were associated with perceived social support in similar ways as the depressive symptoms model. At times when individuals experienced greater than typical levels of anxious symptoms, they also engaged in more ruminative exploration than typical levels (T1-T3). Additionally, they perceived lower than typical levels of support from significant other, friends, and family (T2-T3).
As shown in Fig. 2, no significant cross-lagged path was found in the anxious symptoms model. Similar to the depressive symptoms model, a bi-directional association was found between exploration in breadth and support from significant other at T1-T2 and T2-T3. Higher exploration in depth at T1 and T2 respectively predicted within-person increases in anxious symptoms at T2 and T3. No significant mediation effect was found.

Random intercept cross-lagged panel model (anxious symptoms model).
Gender
In the depressive symptoms model, female-identifying adults reported higher ruminative exploration, βT1 = 0.13, βT2 = 0.13, βT3 = 0.13, ps < 0.001, perceived greater support from significant other, βT1 = 0.10, βT2 = 0.10, βT3 = 0.10, ps < 0.001, and friends, βT1 = 0.07, βT2 = 0.06, βT3 = 0.07, ps < 0.05. Additionally, they reported higher levels of depressive symptoms, βT1 = 0.10, βT2 = 0.09, βT3 = 0.08, ps < 0.001. Comparable results were evident in the anxious symptoms model where females reported more ruminative exploration and perceived social support from significant other and friends. Additionally, females reported more anxious symptoms across waves, βT1 = 0.16, βT2 = 0.16, βT3 = 0.15, ps < 0.001.
Discussion
The search for identity and evaluation of commitments are crucial tasks in emerging adulthood (Arnett, 2000; Erikson, 1968). However, navigating identity processes may be challenging for some, leading to distress (Potterson et al., 2022). Further, individuals with internalizing symptoms may struggle to form and evaluate their commitments (Durbin & Hicks, 2014). Another related construct is social support, which has been associated with identity (Beyers & Goossens, 2008) and mental health outcomes (Wang et al., 2018). However, empirical evidence on the interplay among identity processes, internalizing symptoms, and social support has been scant, especially among emerging adults at the within-person level. To extend current understanding, within-person dynamics among the key constructs and potential mediating paths (with depressive and anxious symptoms as outcomes) were examined.
Identity Processes and Depressive/Anxious Symptoms
Consistent with prior research indicating that higher levels of ruminative exploration are linked to poorer mental health (Luyckx et al., 2006; Luyckx et al., 2008), individuals who engaged in more ruminative exploration experienced greater depressive and anxious symptoms compared to those with lower levels of ruminative exploration. Similar patterns were observed at the within-person level, as evident from covariances among variable residuals. When emerging adults engaged in ruminative exploration more than their typical levels, they also experienced increased depressive and anxious symptoms relative to their typical levels. However, contrary to study hypotheses, individuals with higher ruminative exploration did not experience more depressive and anxious symptoms over time at the within-person level. One potential explanation for this deviation in findings is that previous studies linking ruminative exploration and internalizing symptoms at the within-person level focused on adolescents (Becht et al., 2019; Hatano et al., 2020), whereas the current sample consisted of emerging adults in post-secondary school. Given that emerging adulthood provides more opportunities for role experimentations and identity re-evaluations than adolescence (Arnett, 2000), the absence of clear answers to identity questions may not be experienced as strongly detrimental to well-being. For example, continued exploration may be perceived as normative at this developmental period. Accordingly, ruminative exploration may be less likely to predict later depressive and anxious symptoms among emerging adults.
Another potential explanation for the lack of predictive effects of ruminative exploration on depressive and anxious symptoms over time is that moderators may be involved. For example, previous theorizing suggests that identity processes are intricately related to the coherency of self (i.e., self-concept clarity; see Schwartz et al., 2017 for a review). In support of this, identity commitment and self-concept clarity have been found to predict one another across days within a week in adolescents, whereas the daily dynamics between reconsideration of commitment and self-concept clarity were weaker (Schwartz et al., 2011). Based on this line of theorizing and the established link between self-concept clarity and mental health in adolescents and young adults (Richman et al., 2016; Xiang et al., 2020), ruminative exploration may interact with self-concept clarity to predict depressive and anxious symptoms over time. Additional research is needed to address this speculation.
Individuals with higher exploration in breadth did not differ in symptoms of depression and anxiety compared with individuals with lower exploration in breadth. However, when emerging adults explored more in breadth than their typical level, they experienced decreases in depressive symptoms one wave later. In contrast, individuals with higher exploration in depth tended to have less depressive symptoms than individuals with lower exploration in depth. However, this identity process predicted greater depressive and anxious symptoms over time within individuals. Specifically, when emerging adults explored greater in depth than their typical level, they experienced increases in depressive and anxious symptoms at the subsequent wave. These findings reinforce the vulnerability/predisposition model by indicating that identity development may have implications for internalizing symptoms over time. These findings also suggest that the association between identity processes and mental health outcomes may differ in terms of directionality (i.e., positive vs. negative) at the between-person and within-person level. Therefore, future research should be more cognizant of possible between-person and within-person effects.
The differential implication of exploration in breadth and depth could be interpreted from a developmental perspective. For example, exploration in breadth may be perceived more positively because it reflects the diversity of choices and options available in emerging adulthood, and thus, would be related to better mental health (e.g., less depressive symptoms). By contrast, a deep evaluation of existing commitments amidst the variety of choices and opportunities may be experienced as stressful, and thus, result in more depressive and anxious symptoms. Aligned with this assumption, previous theorizing suggests that exploration in depth may lead to reconsideration of existing commitments if they are no longer perceived as satisfactory (Luyckx et al., 2008). Arguably, this sense of dissatisfaction may, in turn, trigger depressive and anxious symptoms. Longitudinal research that spans across emerging adulthood to later adulthood is needed to address these speculations. Specifically, although exploration of different identities may be felt as developmentally relevant in adolescence and emerging adulthood in contemporary societies, a prolonged process of broad-based exploration beyond these developmental periods may be experienced as more challenging (Luyckx et al., 2013). For example, exploration in breadth may be negatively associated with depressive and anxious symptoms for young adults in their early 20’s because exploring different opportunities is seen as functional in emerging adulthood. However, individuals who continue to explore into their late 20’s may experience more depressive and anxious symptoms because the prolonged exploration in breadth period may be perceived as more challenging.
Identity Processes and Perceived Social Support
Consistent with theoretical assumptions that identity development is embedded within social relationships (Branje et al., 2021; Crocetti et al., 2022), current findings indicated that exploration in breadth and depth were associated positively with perceived support from different sources at the between-person level. Conversely, ruminative exploration was associated negatively with support from significant other, friends, and family. Comparable patterns emerged when looking at covariances among variable residuals at the within-person level. Generally speaking, at times when emerging adults reported stronger exploration in breadth and depth, they also tended to perceive more support than typical levels from different sources. However, at times when individuals engaged in ruminative exploration, they tended to perceive lower than typical levels of social support.
Extending previous literature on identity processes and family support at the between-person level (Crocetti et al., 2017; Pittman et al., 2012), current findings indicated that support from significant other predicted within-person increases in exploration in breadth and vice versa. These findings align with the previous theoretical notion that supportive relationships may serve as a secure base for young adults to confidently explore and experiment with different identities (Branje et al., 2021). Additionally, these findings build upon existing cross-sectional studies examining the link between identity and romantic relationships (Barry et al., 2009) by revealing a temporal association. Specifically, current results suggest that when emerging adults perceive above-average levels of support from their significant other, they tend to be more opened to exploring a wider range of alternatives at the next wave. This heightened exploration in turn, predicts a reciprocated increase in perceived support from significant other. A potential reason for this bidirectional association is that when individuals feel an elevated sense of support from their significant other, they may feel more motivated to explore different opportunities. This heighted level of exploration in breadth may act as a positive reinforcement loop that impacts their perceptions of support or prompts greater encouragement and support from their significant other.
Identity processes did not predict within-person changes in support from family and friends and vice versa. These findings are inconsistent with previous literature indicating a bi-directional association between identity and friendship quality in adolescents (van Doeselaar et al., 2016) as well as identity and support from parents (Beyers & Goossens, 2008), but may be attributed to differences in how support from family (e.g., autonomy support vs. general support in this study) and friends were operationalized (e.g., perceived balanced relatedness vs. general support in this study). These findings also imply potential differences resulting from the developmental periods (i.e., adolescence vs. emerging adulthood). For example, as emerging adults become more independent, they may rely less on their family and friends for support, which could weaken the bi-directional link observed during adolescence. Additional research that follows individuals from adolescence through emerging adulthood would offer insights to how identity development and support from family and friends evolve over time.
Perceived Social Support and Depressive/Anxious Symptoms
Consistent with previous research (Wang et al., 2018), individuals with greater depressive and anxious symptoms tended to perceive lower social support than individuals with higher levels of social support. However, contrary to previous literature that did not find evidence for individual-level changes in parent and peer support in relation to depressive symptoms among emerging adults (Dawson & Samek, 2022), current findings indicated that when individuals experienced less depressive symptoms compared to their typical levels, they perceived greater support from both family and friends at the next wave. These findings offer partial support to interpersonal theories of depression postulating a bi-directional association between social relationships and depressive symptoms (Hames et al., 2013). Specifically, current findings suggest that when individuals experience a reduction in depressive symptoms, they may be more receptive to the support provided by family and friends. A potential reason why support from significant other was not predicted of and predicted by depressive symptoms is that this source of support may be qualitatively distinct from family and friend support. For example, the level of intimacy and the roles played by each support system may be distinct, consequently leading to varying associations with depressive symptoms. In support of this, high-quality social connection with friends and family members, but not frequency of contact, have been associated with lower odds of depression in adolescents and young adults (aged 16–34 years; Werner-Seidler et al., 2017).
Indirect Paths
An interplay among identity processes, social support, and depressive symptoms was evident. Results indicated that when emerging adults perceived support from significant other greater than typical levels, they subsequently engaged in higher levels of exploration in breadth. This heightened exploration, in turn, predicted a decrease in depressive symptoms below typical levels at the next wave. Thus, support from significant other may encourage emerging adults to venture into a wider range of identity possibilities, which in turn, may promote better mental well-being. Further research is needed to explore the interplay among identity processes, social support from different sources, and depressive symptoms. For example, future studies may consider more domain-specific social support (e.g., support related to identity) because it may be related to a given outcome in ways that differs from global social support (Sheets & Mohr, 2009), which was measured in this study.
Limitations and Future Direction
Several study limitations need to be noted. First, the present study focused on depressive and anxious symptoms only. As psychosocial problems can also manifest behaviorally, future studies could examine the behavioral aspects of mental health. For example, non-suicidal self-injury (NSSI) is prevalent in emerging adulthood (Gandhi et al., 2018), and related to identity distress in adolescents (Claes et al., 2014). Accordingly, NSSI may be associated with identity development in emerging adults. Second, identity processes were measured globally in the future domain (e.g., which direction to take on in life). As identity can be considered in different domains in emerging adulthood, such as friendship, partnership, education, and work domains (Vosylis et al., 2018), future studies could explore how identity processes in specific domains are related to mental health. This examination is important because global identity processes only partially explain domain-specific ones, and that identity development in different domains may have different implications (Schwartz et al., 2013; Vosylis et al., 2018). Third, the present sample consisted of largely females from one Canadian university, which may conceal potential gender differences and limit the broader generalizability of current findings. However, this gender distribution aligns with the university’s actual gender ratio. A more diversified sample, such as young adults with different gender identities and/or from different universities or occupations, is needed to examine gender differences and generalizability of present results. Further, although ethnic, culture and socio-economic differences may contribute partially to identity development (Galliher et al., 2017), these differences were not accounted in the study to streamline the model. However, exploring the nuanced effects of these demographics on identity processes and their subsequent impact on mental health might offer insights to targeted intervention (e.g., identifying young adults who may benefit form additional support in navigating different identities). Relatedly, participation was student-initiated (i.e., students contacted the lab to request participation), suggesting potential self-selection bias. Finally, self-reports were used in this study, which might have inflated shared method variance or respondent bias. However, self-reports are considered appropriate in the assessments of constructs related to personal experiences (Whitcomb, 2012), such as identity processes and internalizing symptoms. Additionally, perceived social support tends to have stronger implications for developmental outcomes than actual received support (Eagle et al., 2019). Nonetheless, future research could use a multi-informant approach, such as clinical measures of internalizing symptoms, to reduce bias.
Implications
Current findings suggest that intervention efforts on post-secondary campuses may want to focus on targeting and helping emerging adults engaging in ruminative exploration. Moreover, findings underscore that encouraging breadth of exploration may also be helpful, but that additional supports may be needed to guide emerging adults through deeper exploration (which may be distressing at time). Fostering social support, particularly support from significant others, may also be beneficial in reducing risk for depressive symptoms directly, and by encouraging breadth of exploration. Findings also suggest that depressive and anxious symptoms may exacerbate risk for identity struggles, and lead to worsening perceived social support. Thus, helping emerging adults who are struggling with depressive symptoms with identity development, and navigating social relationships is important.
Conclusion
Although identity development is intertwined with social relationships and mental health issues can be influenced by perceived social support, little is known about how these factors may be associated within emerging adults in the post-secondary context. To address this gap in the literature, the associations among identity processes, perceived social support from different sources, as well as depressive and anxious symptoms were examined in emerging adults, while considering the possible mediating effects of social support. This study contributes to the understanding of the dynamics between identity processes and psychopathological symptoms in emerging adults. Current findings not only reinforce the vulnerability/predisposition model and the role of social relationships in identity development, but also provide partial support to interpersonal theories of depression. Mediating effects also suggest that within-person changes in perceived social support may be longitudinally linked to depressive symptoms via identity exploratory processes.
References
Arnett, J. J. (2000). Emerging adulthood: a theory of development from the late teens through the twenties. American Psychologist, 55(5), 469–480. https://doi.org/10.1037/0003-066X.55.5.469.
Barry, C. M., Madsen, S. D., Nelson, L. J., Carroll, J. S., & Badger, S. (2009). Friendship and romantic relationship qualities in emerging adulthood: Differential associations with identity development and achieved adulthood criteria. Journal of Adult Development, 16, 209–222. https://doi.org/10.1007/s10804-009-9067-x.
Becht, A. I., Bos, M. G., Nelemans, S. A., Peters, S., Vollebergh, W. A., Branje, S. J., & Crone, E. A. (2018). Goal‐directed correlates and neurobiological underpinnings of adolescent identity: a multimethod multisample longitudinal approach. Child Development, 89(3), 823–836. https://doi.org/10.1111/cdev.13048.
Becht, A. I., Luyckx, K., Nelemans, S. A., Goossens, L., Branje, S. J. T., Vollebergh, W. A. M., & Meeus, W. H. J. (2019). Linking identity and depressive symptoms across adolescence: a multisample longitudinal study testing within-person effects. Developmental Psychology, 55(8), 1733–1742. https://doi.org/10.1037/dev0000742.
Beyers, W., & Goossens, L. (2008). Dynamics of perceived parenting and identity formation in late adolescence. Journal of Adolescence, 31(2), 165–184. https://doi.org/10.1016/j.adolescence.2007.04.003.
Branje, S., De Moor, E. L., Spitzer, J., & Becht, A. I. (2021). Dynamics of identity development in adolescence: a decade in review. Journal of Research on Adolescence, 31(4), 908–927. https://doi.org/10.1111/jora.12678.
Byrne, B. M. (2013). Structural equation modeling with Mplus: Basic concepts, applications, and programming. Routledge.
Claes, L., Luyckx, K., & Bijttebier, P. (2014). Non-suicidal self-injury in adolescents: prevalence and associations with identity formation above and beyond depression. Personality and Individual Differences, 61, 101–104. https://doi.org/10.1016/j.paid.2013.12.019.
Crocetti, E. (2018). Identity dynamics in adolescence: processes, antecedents, and consequences. European Journal of Developmental Psychology, 15(1), 11–23. https://doi.org/10.1080/17405629.2017.1405578.
Crocetti, E., Albarello, F., Meeus, W., & Rubini, M. (2022). Identities: a developmental social-psychological perspective. European Review of Social Psychology, 1–41. https://doi.org/10.1080/10463283.2022.2104987
Crocetti, E., Branje, S., Rubini, M., Koot, H. M., & Meeus, W. (2017). Identity processes and parent–child and sibling relationships in adolescence: a five‐wave multi‐informant longitudinal study. Child Development, 88(1), 210–228. https://doi.org/10.1111/cdev.12547.
Crocetti, E., Luyckx, K., Scrignaro, M., & Sica, L. S. (2011). Identity formation in Italian emerging adults: a cluster-analytic approach and associations with psychosocial functioning. European Journal of Developmental Psychology, 8(5), 558–572. https://doi.org/10.1080/17405629.2011.576858.
Crocetti, E., Schwartz, S., Fermani, A., Klimstra, T., & Meeus, W. H. J. (2012). A cross-national study of identity statuses in Dutch and Italian adolescents: status distributions and correlates. European Psychologist, 17, 171–181. https://doi.org/10.1027/1016-9040/a000076.
Dawson, M. R., & Samek, D. R. (2022). Parent and peer social-emotional support as predictors of depressive symptoms in the transition into and out of college. Personality and Individual Differences, 192, 111588 https://doi.org/10.1016/j.paid.2022.111588.
Diekman, A. B., Brown, E. R., Johnston, A. M., & Clark, E. K. (2010). Seeking congruity between goals and roles: a new look at why women opt out of science, technology, engineering, and mathematics careers. Psychological Science, 21(8), 1051–1057. https://doi.org/10.1177/0956797610377342.
Durbin, C. E., & Hicks, B. M. (2014). Personality and psychopathology: a stagnant field in need of development. European Journal of Personality, 28(4), 362–386. https://doi.org/10.1002/per.1962.
Eagle, D. E., Hybels, C. F., & Proeschold-Bell, R. J. (2019). Perceived social support, received social support, and depression among clergy. Journal of Social and Personal Relationships, 36(7), 2055–2073. https://doi.org/10.1177/026540751877613.
Eaton, W. W., Smith, C., Ybarra, M., Muntaner, C., & Tien, A. (2004). Center for epidemiologic studies depression (CES-D) Scale. In M. E. Maruish (Ed.), The use of psychological testing for treatment planning and outcomes assessment (3rd ed., pp. 363–377). Lawrence Erlbaum. https://doi.org/10.1007/978-94-007-0753-5_300
Erikson E. H. (1950). Growth and crises of the “healthy personality”. In Senn M. J. E. (Ed.), Symposium on the healthy personality (pp. 91–146). Josiah Macy, Jr. Foundation.
Erikson, E. H. (1968) Youth, Identity and Crisis. Norton.
Galliher, R. V., McLean, K. C., & Syed, M. (2017). An integrated developmental model for studying identity content in context. Developmental Psychology, 53(11), 2011–2022. https://doi.org/10.1037/dev0000299.
Gandhi, A., Luyckx, K., Baetens, I., Kiekens, G., Sleuwaegen, E., Berens, A., Maitra, S., & Claes, L. (2018). Age of onset of non-suicidal self-injury in Dutch-speaking adolescents and emerging adults: an event history analysis of pooled data. Comprehensive Psychiatry, 80, 170–178. https://doi.org/10.1016/j.comppsych.2017.10.007.
Hamaker, E. L., Kuiper, R. M., & Grasman, R. P. (2015). A critique of the cross-lagged panel model. Psychological Methods, 20(1), 102–116. https://doi.org/10.1037/a0038889.
Hames, J. L., Hagan, C. R., & Joiner, T. E. (2013). Interpersonal processes in depression. Annual Review of Clinical Psychology, 9, 355–377. https://doi.org/10.1146/annurev-clinpsy-050212-185553.
Hardy, S. A., Francis, S. W., Zamboanga, B. L., Kim, S. Y., Anderson, S. G., & Forthun, L. F. (2013). The roles of identity formation and moral identity in college student mental health, health‐risk behaviors, and psychological well‐being. Journal of Clinical Psychology, 69(4), 364–382. https://doi.org/10.1002/jclp.21913.
Hatano, K., Hihara, S., Sugimura, K., & Mizokami, S. (2022). Identity formation with gender differences in University students: a three-wave longitudinal study. Current Psychology, 1–13. https://doi.org/10.1007/s12144-022-04036-4.
Hatano, K., Sugimura, K., & Luyckx, K. (2020). Do identity processes and psychosocial problems intertwine with each other? Testing the directionality of between-and within-person associations. Journal of Youth and Adolescence, 49(2), 467–478. https://doi.org/10.1007/s10964-019-01182-0.
Hofer, J., Busch, H., & Kärtner, J. (2011). Self–regulation and well–being: the influence of identity and motives. European Journal of Personality, 25(3), 211–224. https://doi.org/10.1002/per.789.
Kler, S., Arora, S., & Le, T. P. (2022). Validation of the Multidimensional Scale of Perceived Social Support (MSPSS) among LGBTQ+ people of color. Measurement and Evaluation in Counseling and Development, 1–14. https://doi.org/10.1080/07481756.2022.2109174.
Klimstra, T. A., & Denissen, J. J. A. (2017). A theoretical framework for the associations between identity and psychopathology. Developmental Psychology, 53(11), 2052–2065. https://doi.org/10.1037/dev0000356.
Leaper, C. (2015). Gender and social-cognitive development. In R. M. Lerner & M. E. Lamb (Eds.), Handbook of Child Psychology and Developmental Science: Vol. 2. Cognitive processes (7th ed., pp. 806–853). John Wiley & Sons.
Lee, C., Dickson, D. A., Conley, C. S., & Holmbeck, G. N. (2014). A closer look at self-esteem, perceived social support, and coping strategy: a prospective study of depressive symptomatology across the transition to college. Journal of Social and Clinical Psychology, 33(6), 560–585. https://doi.org/10.1521/jscp.2014.33.6.560.
Luyckx, K., Klimstra, T. A., Duriez, B., Van Petegem, S., & Beyers, W. (2013). Personal identity processes from adolescence through the late 20s: Age trends, functionality, and depressive symptoms. Social Development, 22(4), 701–721. https://doi.org/10.1111/sode.12027.
Luyckx, K., Schwartz, S. J., Berzonsky, M. D., Soenens, B., Vansteenkiste, M., Smits, I., & Goossens, L. (2008). Capturing ruminative exploration: extending the four-dimensional model of identity formation in late adolescence. Journal of Research in Personality, 42(1), 58–82. https://doi.org/10.1016/j.jrp.2007.04.004.
Luyckx, K., Soenens, B., & Goossens, L. (2006). The personality-identity interplay in emerging adult women: convergent findings from complementary analyses. European Journal of Personality, 20, 195–215. https://doi.org/10.1002/per.579.
Marcia, J. E. (1966). Development and validation of ego–identity status. Journal of Personality and Social Psychology, 3, 551–558. https://doi.org/10.1037/h0023281.
Meca, A., Rodil, J. C., Paulson, J. F., Kelley, M., Schwartz, S. J., Unger, J. B., & Zamboanga, B. L. (2019). Examining the directionality between identity development and depressive symptoms among recently immigrated Hispanic adolescents. Journal of Youth and Adolescence, 48(11), 2114–2124. https://doi.org/10.1007/s10964-019-01086-z.
Meeus, W. (1996). Studies on identity development in adolescence: an overview of research and some new data. Journal of Youth and Adolescence, 25(5), 569–598. https://doi.org/10.1007/BF01537355.
Morea, A., & Calvete, E. (2021). Cognitive flexibility and selective attention’s associations with internalizing symptoms in adolescents: are they reciprocal? Journal of Youth and Adolescence, 50(5), 921–934. https://doi.org/10.1007/s10964-021-01402-6.
Mulder, J. D., & Hamaker, E. L. (2021). Three extensions of the random intercept cross-lagged panel model. Structural Equation Modeling: A Multidisciplinary Journal, 28(4), 638–648. https://doi.org/10.1080/10705511.2020.1784738.
Muthén, L., & Muthén, B. (1998-2022). Mplus (Version 8.5). Muthén & Muthén.
Needham, B. L. (2008). Reciprocal relationships between symptoms of depression and parental support during the transition from adolescence to young adulthood. Journal of Youth and Adolescence, 37, 893–905. https://doi.org/10.1007/s10964-007-9181-7.
Orth, U., Clark, D. A., Donnellan, M. B., & Robins, R. W. (2021). Testing prospective effects in longitudinal research: comparing seven competing cross-lagged models. Journal of Personality and Social Psychology, 120(4), 1013–1034. https://doi.org/10.1037/pspp0000358.
Parker, G., & Brotchie, H. (2010). Gender differences in depression. International Review of Psychiatry, 22(5), 429–436. https://doi.org/10.3109/09540261.2010.492391.
Pittman, J. F., Kerpelman, J. L., Soto, J. B., & Adler-Baeder, F. M. (2012). Identity exploration in the dating domain: the role of attachment dimensions and parenting practices. Journal of Adolescence, 35(6), 1485–1499. https://doi.org/10.1016/j.adolescence.2012.04.006.
Potterton, R., Austin, A., Robinson, L., Webb, H., Allen, K. L., & Schmidt, U. (2022). Identity development and social-emotional disorders during adolescence and emerging adulthood: a systematic review and meta-analysis. Journal of Youth and Adolescence, 1-14. https://doi.org/10.1007/s10964-021-01536-7.
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40(3), 879–891. https://doi.org/10.3758/BRM.40.3.879.
Preacher, K. J., Zhang, Z., & Zyphur, M. J. (2011). Alternative methods for assessing mediation in multilevel data: the advantages of multilevel SEM. Structural Equation Modelling, 18, 161–182. https://doi.org/10.1080/10705511.2011.557329.
Richman, S. B., Pond, Jr, R. S., Dewall, C. N., Kumashiro, M., Slotter, E. B., & Luchies, L. B. (2016). An unclear self leads to poor mental health: self-concept confusion mediates the association of loneliness with depression. Journal of Social and Clinical Psychology, 35(7), 525–550. https://doi.org/10.1521/jscp.2016.35.7.525.
Schiebener, J., García-Arias, M., García-Villamisar, D., Cabanyes-Truffino, J., & Brand, M. (2015). Developmental changes in decision making under risk: the role of executive functions and reasoning abilities in 8-to 19-year-old decision makers. Child Neuropsychology, 21(6), 759–778. https://doi.org/10.1080/09297049.2014.934216.
Schmitt, D. P., Long, A. E., McPhearson, A., O’Brien, K., Remmert, B., & Shah, S. H. (2017). Personality and gender differences in global perspective. International Journal of Psychology, 52, 45–56. https://doi.org/10.1002/ijop.12265.
Schwartz, S. J., Beyers, W., Luyckx, K., Soenens, B., Zamboanga, B. L., Forthun, L. F., & Waterman, A. S. (2011). Examining the light and dark sides of emerging adults’ identity: a study of identity status differences in positive and negative psychosocial functioning. Journal of Youth and Adolescence, 40(7), 839–859. https://doi.org/10.1007/s10964-010-9606-6.
Schwartz, S. J., Meca, A., Petrova, M. (2017). Who am I and why does it matter? Linking personal identity and self-concept clarity. In: Lodi-Smith, J., DeMarree, K. (eds). Self-concept clarity. Springer. https://doi.org/10.1007/978-3-319-71547-6_8.
Schwartz, S. J., & Petrova, M. (2019). Prevention science in emerging adulthood: a field coming of age. Prevention Science, 20(3), 305–309. https://doi.org/10.1007/s11121-019-0975-0.
Schwartz, S. J., Zamboanga, B. L., Luyckx, K., Meca, A., & Ritchie, R. A. (2013). Identity in emerging adulthood: reviewing the field and looking forward. Emerging adulthood, 1(2), 96–113. https://doi.org/10.1177/2167696813479781.
Seligman, M. E. P., Steen, T. A., Park, N., Peterson, C., & Report, P. (2005). Positive psychology progress: empirical validation of interventions. American Psychologist, 60(5), 410–421. https://doi.org/10.1037/0003-066X.60.5.410.
Sheets, Jr., R. L., & Mohr, J. J. (2009). Perceived social support from friends and family and psychosocial functioning in bisexual young adult college students. Journal of Counseling Psychology, 56(1), 152–163. https://doi.org/10.1037/0022-0167.56.1.152.
Spitzer, R. L., Kroenke, K., Williams, J. B., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: the GAD-7. Archives of Internal Medicine, 166(10), 1092–1097. https://doi.org/10.1001/archinte.166.10.1092.
Sriken, J., Johnsen, S. T., Smith, H., Sherman, M. F., & Erford, B. T. (2022). Testing the factorial validity and measurement invariance of college student scores on the Generalized Anxiety Disorder (GAD-7) Scale across gender and race. Measurement and Evaluation in Counseling and Development, 55(1), 1–16. https://doi.org/10.1080/07481756.2021.1902239.
Statistics Canada (2021). Census profile, 2021 census of population. https://www12.statcan.gc.ca/census-recensement/2021/dp-pd/prof/index.cfm?Lang=E.
Stice, E., Ragan, J., & Randall, P. (2004). Prospective relations between social support and depression: differential direction of effects for parent and peer support. Journal of Abnormal Psychology, 113(1), 155–159. https://doi.org/10.1037/0021-843X.113.1.155.
Van Dam, N. T., & Earleywine, M. (2011). Validation of the Center for Epidemiologic Studies Depression Scale—Revised (CESD-R): Pragmatic depression assessment in the general population. Psychiatry Research, 186(1), 128–132. https://doi.org/10.1016/j.psychres.2010.08.018.
van Doeselaar, L., Becht, A. I., Klimstra, T. A., & Meeus, W. H. (2018). A review and integration of three key components of identity development. European Psychologist, 23, 278–288. https://doi.org/10.1027/1016-9040/a000334.
van Doeselaar, L., Meeus, W., Koot, H. M., & Branje, S. (2016). The role of best friends in educational identity formation in adolescence. Journal of Adolescence, 47, 28–37. https://doi.org/10.1016/j.adolescence.2015.12.002.
Vosylis, R., Erentaitė, R., & Crocetti, E. (2018). Global versus domain-specific identity processes: which domains are more relevant for emerging adults. Emerging Adulthood, 6(1), 32–41. https://doi.org/10.1177/2167696817694698.
Wang, J., Mann, F., Lloyd-Evans, B., Ma, R., & Johnson, S. (2018). Associations between loneliness and perceived social support and outcomes of mental health problems: a systematic review. BMC Psychiatry, 18(1), 1–16. https://doi.org/10.1186/s12888-018-1736-5.
Waterman, A. S. (1993). Two conceptions of happiness: contrasts of personal expressiveness (eudaimonia) and hedonic enjoyment. Journal of Personality and Social Psychology, 64(4), 678–691. https://doi.org/10.1037/0022-3514.64.4.678.
Waterman, A. S. (2007). Doing well: the relationship of identity status to three conceptions of well-being. Identity, 7, 289–307. https://doi.org/10.1080/15283480701600769.
Werner-Seidler, A., Afzali, M. H., Chapman, C., Sunderland, M., & Slade, T. (2017). The relationship between social support networks and depression in the 2007 National Survey of Mental Health and Well-being. Social Psychiatry and Psychiatric Epidemiology, 52, 1463–1473. https://doi.org/10.1007/s00127-017-1440-7.
Whitcomb, S. (2012). Behavioral, social, and emotional assessment of children and adolescents (4th ed.). Routledge. https://doi.org/10.4324/9780203818596.
Xiang, G., Li, Q., Du, X., Liu, X., Xiao, M., & Chen, H. (2020). Links between family cohesion and subjective well-being in adolescents and early adults: The mediating role of self-concept clarity and hope. Current Psychology, 1-10. https://doi.org/10.1007/s12144-020-00795-0.
Zimet, G. D., Dahlem, N. W., Zimet, S. G., & Farley, G. K. (1988). The multidimensional scale of perceived social support. Journal of Personality Assessment, 52(1), 30–41. https://doi.org/10.1207/s15327752jpa5201_2.
Funding
This research was supported by the Social Sciences and Humanities Research Council (Grant number: 435-2018-0961) awarded to Chloe A. Hamza. Dr. Hamza would also like to acknowledge that this research was undertaken in part thanks to funding from the Canada Research Chairs Program (CRC-2021-00090).
Data Sharing DeclarationThis manuscript’s data will not be deposited.
Author information
Authors and Affiliations
Contributions
T.W. contributed to the conceptualization and design of the study, led the analysis and interpretation of data, as well as drafted and revised the manuscript; CH contributed to the conceptualization and design of the study, led the acquisition of data, supported the analysis and interpretation of data, as well as provided critical comments and revised the manuscript. Both authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Ethical Approval
This study involved human participants and was conducted in accordance with the ethical standards of the institutional review board of University of Toronto. All research reported on in the manuscript was conducted in compliance with APA ethical principles.
Informed Consent
Active informed consent was obtained from all participants in the study at each time of assessment.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Wong, T.K.Y., Hamza, C.A. Longitudinal Associations among Identity Processes and Mental Health in Young Adulthood: The Mediating Role of Social Support. J. Youth Adolescence 53, 814–832 (2024). https://doi.org/10.1007/s10964-023-01883-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-023-01883-7