
Abstract
Prior research has demonstrated that behavioral, demographic, and mental health characteristics are associated with suicide, particularly among youth and young adults. Although recent research has begun to explore developmental trajectories of suicide-related outcomes, few studies to date have extended beyond late adolescence. Understanding different trajectories of suicide-related thoughts and behaviors from adolescence through mid-adulthood has the potential to refine developmental perspectives on suicide risk and to inform prevention efforts. Using National Longitudinal Study of Adolescent to Adult Health data (n = 9421 respondents with data at all four waves), this study analyzed suicide-related outcomes across ages 12–31 years. Growth mixture modeling (GMM) was used to estimate trajectory classes for past-year suicide ideation and attempts, followed by multinomial logistic regression to explore the association between race/ethnicity and class membership. In weighted descriptive analyses, the sample was 50.0% female; it was 15.5% African American, 2.1% Asian/Pacific Islander, 12.0% Hispanic, 0.9% other, and 65.9% White. GMM results revealed three trajectory classes for ideation: sustained higher risk, sustained lower risk, and adolescent-limited risk. Two trajectory classes emerged for attempts: declining higher risk and sustained lower risk. For ideation, African Americans were less likely than Whites to be in either the sustained higher risk or the adolescent-limited risk trajectory. For attempts, African Americans had significantly lower odds than Whites and Asians/Pacific Islanders had nearly four times the odds of Whites of being in the sustained higher risk trajectory, though the latter was only marginally significant. The finding of associations between race/ethnicity and distinct patterns of suicide-related behavioral development from early adolescence into mid-adulthood suggests new directions for developmental research and provides evidence to inform future suicide prevention efforts.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Suicide is a persistent and growing public health issue in the United States. On average, there are 121 completed suicides in the US every day (Xu 2017), and from 1999 to 2014, age-adjusted suicide rates increased 24% (Curtin et al. 2016). The proportion of total deaths attributable to suicide varies by race/ethnicity, with recent data showing highest proportions among American Indians/Alaskan Natives [3.0% of total deaths attributable to suicide], followed by Asians/Pacific Islanders [2.0%], Whites [1.7%], and Blacks [0.8%] (CDC and NCHS 2017). There are also important differences by gender, with suicide ideation and nonfatal attempts more common among females and completed suicide more common among males, across ages (CDC and NCHS 2017), though the gender difference is wider among Whites than in some other racial/ethnic groups (e.g., Native Hawaiians and some American Indians; Joe et al. 2008a, 2008b).
Recent research attention has focused particularly on youth suicide. Suicide is the second leading cause of death for 10–14, 15–24, and 25–34 year olds (CDC and NCHS 2017). Among US high school students, the 2017 Youth Risk Behavior Survey found 13.6% have made a plan to attempt suicide, 7.4% have attempted suicide, and 2.4% have made a suicide attempt that required treatment by a doctor or nurse in the previous 12 months (CDC 2018). Less research has examined suicide-related outcomes among adults older than college-age (typically 18–24 years old) or developmental trajectories of suicide behaviors from adolescence well into adulthood. A developmental science perspective that centers on when and how the outcomes of interest develop and change across the life course (Dahl et al. 2018) is important for targeted suicide prevention efforts in adolescence and beyond (Goldman-Mellor et al. 2014).
Several factors are known to be associated with suicide, particularly among adolescents. These include gender [girls are more likely than boys (Supple 2013)—and women more likely than men—(Olfson et al. 2017) to attempt suicide]; and sexual identity and orientation [sexual minority individuals may be more likely than heterosexual and cisgender persons to attempt or complete suicide (Hottes et al. 2016)]. Race/ethnicity is another factor found to be associated with suicide. Some research suggests suicide ideation and behaviors may be more prevalent among non-White youth (CDC 2018) and adults (CDC and NCHS 2017), while other studies find at least for suicide attempts among adults, compared to White adults, African American/Black adults (Borges et al. 2008) and Asian adults (Borges 2012) may be less likely to attempt. Also associated with suicide are behavioral and familial factors such as depression (Elgin 2014) and poverty (Kim et al. 2016).
Much of the research to date on suicide and related behaviors has used cross-sectional data and has focused exclusively on the period of adolescence. Indeed, in the US population as a whole, although suicide affects people of all ages, the highest prevalence of suicide ideation, plans, and attempts occur in adolescence (Substance Use and Mental Health Services Administration 2014). However, a result of this narrow focus is that little is known about the development of suicide-related thoughts and behaviors over time, including well into adulthood, when individuals are still at risk. Person-oriented research allows for the study of patterns and processes with a focus on the individual (Bergman and Lundh 2015). By using person-centered analytic approaches such as growth mixture modeling to study suicide thoughts and behaviors well into adulthood, there is the potential to improve understanding of changes across development and beyond adolescence. This developmental perspective allows for more targeted and effective interventions for those at different life stages and with potentially different needs. Given prior data indicating differences by race/ethnicity in prevalence of suicide, examining the potential for racial/ethnic differences in developmental trajectories of suicide-related outcomes is also of interest.
Developmental research over the past 20 years has advanced multifaceted conceptual models to show how distal and proximal variables—and their developmental sequence—interact and contribute to suicide behaviors (Séguin et al. 2014). Biological factors, negative life events, and other contextual factors have been examined, typically using cross-sectional designs. In the current study, the research questions were guided by theories about stress and coping among members of minority groups. Smedley and colleagues (1993) model of minority-status stresses emphasizes that although some life stressors are experienced across racial/ethnic groups, there are also specific stressors experienced by members of racial/ethnic minority groups that increase self-doubts about fitting in with the majority group and hamper social integration and thus the potential for social support (Smedley et al. 1993). Some stressful experiences—such as overt racial prejudice or discrimination—are directly linked to minority group membership. In addition, being a member of a minority group may compound stressors common to many youth, particularly when these youth are also socially, politically, and economically marginalized (Smedley et al. 1993).
At the same time, positive racial identity can contribute to resilience against poor mental health. For example, Sellers and colleagues showed that in a sample of African American adolescents, experiencing racial discrimination was associated with greater depressive symptoms and lower psychological well-being (Sellers et al. 2006). Furthermore, at least one component of positive racial identity was associated with better psychological outcomes, regardless of experience of racial discrimination (Sellers et al. 2006). Walker and colleagues examined the relationships among acculturative stress (the tension associated with navigating a minority cultural identity and adapting to a dominant culture), racial/ethnic identity (holding values and beliefs and engaging in practices important to an ethnic or cultural group), depression, and suicidal ideation among a sample of college students (Walker et al. 2008). They found that depression was more strongly associated with suicidal ideation for African American students who reported low racial/ethnic identity than for those who reported high racial/ethnic identity; no moderation of the depression-suicide association was found for White students (Walker et al. 2008).
Finally, the current study drew from Meyer’s Minority Stress Model (MSTM), which was proposed to explain poor mental health among sexual minority individuals (Meyer 2003). Maladaptive stress experienced by members of minority groups is viewed as a result of the interplay among distal stress processes (experiences of discrimination), proximal stress processes (individual fears of—and internalized reactions to—discriminatory experiences), environmental circumstances, minority identity, and coping and social support (Meyer 2003). The MSTM may be applicable to other groups that experience social exclusion, because members of these groups may experience similar interplay of stressors and circumstances (Moradi 2013). Figure 1 shows the MSTM adapted by the authors for the study of suicide-related outcomes during adolescence and into mid-adulthood, a period characterized by identity formation and changing social, familial, and economic circumstances. In this adapted model, circumstances in the social environment, status as a racial/ethnic minority in the context of dominant White US culture, and racial/ethnic self-identity combine to influence general stressors (those experienced by people regardless of their race/ethnicity, such as economic, educational, and familial/relationship stressors) and both distal and proximal stress processes unique to the experiences of members of racial/ethnic minority groups in the US. These stressors in turn are associated with suicide-related outcomes, via a pathway potentially moderated by the quantity and quality of available coping resources and social support.

A minority stress model for suicide-related outcomes in adolescence and early/mid-adulthood (adapted from Meyer 2003)
The Current Study
Despite increased research attention to suicide in the US, few studies have used longitudinal data extending beyond adolescence to examine developmental trajectories of suicide-related outcomes well into adulthood. Although theoretical models of minority stress and coping suggest that nonwhite racial/ethnic groups may be at increased risk for suicide compared with White peers, empirical studies to date show mixed findings regarding whether the timing or severity of suicide risk varies by race/ethnicity. To address these gaps, the framework of minority stress was used as a theoretical basis for examining the association of race/ethnicity with different developmental trajectories for suicide-related thoughts and behaviors across adolescence through mid-adulthood. The study tested whether, as suggested by extant minority stress models, experiencing structural discrimination acted as a mediator or moderator of the race/ethnicity-trajectory class association for both thoughts (suicide ideation) and behaviors (suicide attempts). This analysis controls for characteristics known to be associated with stress, coping, and suicidality: gender, parental education, family income, and baseline depressive symptoms (assessed in Wave I during grades 7–12), among participants in the National Longitudinal Study of Adolescent to Adult Health, known as Add Health (Harris 2009).
Methods
Measures
Suicide ideation
Respondents at each wave were asked whether they ever seriously thought about committing suicide in the prior 12 months; valid responses were no or yes.
Suicide attempts
Respondents at each wave were asked, “During the past 12 months, how many times did you actually attempt suicide?” and the response categories were 0 times, 1, 2–3, 4–5, and 6 or more times (except for the highest response category was 5 or more times in Waves 3 and 4). Although multiple suicide attempts were rarely reported (see Table 1 for any attempts reported), to address that multiple attempts in a single year may represent a different phenomenon than a single attempt, suicide attempts were collapsed into three groups: 0 (no attempts), 1 attempt, and >1 attempt.
Race/ethnicity
This variable was created based on Wave I response to “What is your race?” as recommended by Add Health (Add Health 2016), with the following groups: Hispanic, non-Hispanic Black/African American, non-Hispanic Asian, non-Hispanic Native American, non-Hispanic Other, and non-Hispanic White. Because of the small number of participants with Native American or Other race/ethnicities, these cases were excluded prior to analysis of trajectories and their correlates.
Sex
An indicator variable for sex (female or male) was created and used as a covariate in analysis (see Data Analysis below).
Socioeconomic status (SES)
This construct was operationalized using two available separate measures: parental education level (college graduate, some college, high school graduate, less than high school graduate) and household income based on parent interviews congruent with the timing of Wave I of Add Health.
Baseline depressive symptoms
Depressive symptoms were operationalized as continuous scores on the Center for Epidemiologic Studies Depression Scale (CES-D; Eaton et al. 2004) from Wave I adolescent interview data (Cronbach’s α = 0.86).
Structural discrimination
Structural discrimination at Wave I of Add Health was studied using two measures. Respondents were asked how much they agree or disagree with two statements, referring to their current school year or, if interviewed over the summer, their prior school year: (1) “Students at your school are prejudiced.” and (2) “The teachers at your school treat students fairly.” Response options were: strongly agree = 5, agree = 4, neither agree nor disagree = 3, disagree = 2, and strongly disagree for both = 1. Responses for (1) “The teachers at your school…” were reverse scored.
This study of existing data was approved by the Institutional Review Board at The University of North Carolina Greensboro.
Data Analysis
Trajectories of any suicide ideation (any vs. none) and attempt category (no suicide attempts, 1 attempt, >1 attempt) were investigated using growth mixture modeling (GMM) through an accelerated longitudinal study design approach (ALD; (Galbraith et al. 2017)). Using an ALD allowed the analysis of behaviors from Waves I-IV of the Add Health study through trajectories across ages 12–31 years by GMM. Growth curves with quadratic trends fit best across analyses relative to curves with linear trends only using Bayesian Information Criteria (BIC). The number of trajectories chosen for each of the two suicide outcomes was based on GMM methodology recommendations by Ram and Grimm (2009). Assessing model entropy was one recommendation by Ram and Grimm (2009): an entropy of one would describe perfect classification accuracy of placing participants into classes based on a given model’s posterior probabilities (Celeux and Soromenho 1996), with an entropy > 0.80 considered desirable. Akaike Information Criteria (AIC) and Sample Size-Adjusted Bayesian Information Criteria (SSA-BIC) were also considered. AIC and SSA-BIC are relative fit information criteria that can suggest one model fits better relative to another. A model with a difference of four or more relative to the minimum value of all considered models has less empirical support (Burnham and Anderson 2010). More parsimonious models with fewer latent classes) with similar empirical support were preferred. Likelihood ratio tests (LRTs) were also considered: The Lo-Mendell-Rubin (LMR) LRT and LMR adjusted LRT (LMR-A-LRT) are tests with the null hypothesis that the model with the given number of classes (c) fits equally well relative to a model with c-1 classes (one less latent class). Thus, p < 0.05 for these tests imply c classes fit better than c-1, and when nonsignificant, the more parsimonious c-1 solution is equally desirable (Lo et al. 2001).
Multinomial logistic regression taking into account trajectory classification uncertainty (Asparouhov and Muthén 2014) was then used to model associations between trajectory membership and race/ethnicity groups after controlling for the covariates of gender, parental education, family income, discrimination measures and baseline CES-D scores for depressive symptoms at Wave I. Moderation and mediation testing with race/ethnicity and covariates were additionally performed using manual 3-step methods (Asparouhov and Muthén 2014). Moderation using pairwise interactions between race/ethnicity and covariates (where continuous variables were first centered on the sample mean value) were checked for significance and none were statistically significant and therefore not included. Additionally, mediation effects of structural discrimination items were checked and also found to be not statistically significant. Full information maximum likelihood estimation was used to adjust for effects of missing data (Enders 2010) in all analyses beyond sampling weights adjusted for longitudinal attrition. Modeling took into account the Add Health survey design through recommended weighting, clustering, and stratification adjustments (Chen and Chantala 2014) and subdomain adjustments (Graubard and Korn 1996). Mplus v7.3 (Muthén and Muthén 2015) and SAS v9.4 (SAS Institute 2012) were used to perform analyses. A two-sided p-value < 0.05 was considered significant.
Results
Description of the sample based on Wave I data for gender, race/ethnicity, and SES have been previously reported (Park et al. 2018). Briefly, the sample included 9421 respondents with data at all four waves. In weighted descriptive analyses, the sample was 50.0% female; for self-identified race/ethnicity, the sample was 15.5% African American, 2.1% Asian/Pacific Islander, 12.0% Hispanic, 0.9% Other, and 65.9% White. (The remaining 3.6% of the sample was Native American; these respondents were excluded from subsequent analyses due to small sample size.) For structural discrimination, 42% agreed or strongly agreed that students at their school were prejudiced in the last year at Wave I (M = 3.1 on 1–5 scale), and 58% agreed or strongly agreed that teachers at their school treated students fairly in the last year (M = 2.5 on a 1–5 scale). The average CES-D score (weighted) at Wave I (adolescents in grades 7–12) was 15.1 (Med = 13.8), where 59.8% were considered to have no depressive symptoms (CES-D score < 16), 33.3% with mild depressive symptoms (16 ≤ CES-D < 24), and 6.9% with severe depressive symptoms (CES-D ≥ 24).
Weighted percentages for suicide ideation and any suicide attempts by race/ethnicity and wave of data collection are given in Table 1. The percent with suicidal thoughts were lowest at Wave III: 8.1% for non-Hispanic White, 8.0% for Asian/Pacific Islander, 7.3% for Hispanic, and 4.1% for non-Hispanic African American. Interestingly, this increased to 7.6% for African Americans at Wave IV (adults aged 24–31) and 15.2% for Asian/Pacific Islander participants. During adolescence (in grades 7–12), any suicidal thoughts in the past 12 months were most prevalent for Asian/Pacific Islander adolescents (15.4%) and least prevalent for African Americans (12.3%). The percent with any suicide attempts ranged from 3.5% for Asian/Pacific Islanders to 4.8% for Hispanics during adolescence (in grades 7–12) and steadily declined for each race/ethnicity except for Asian/Pacific Islanders. Here, this went from 3.5 to 5.7% during adolescence (grades 8–12) and was markedly higher at 3.7% at Wave III (young adults aged 18–26) relative to the other race/ethnicity groups (range = 1.6–2.0%).
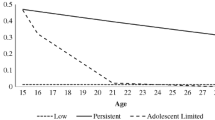
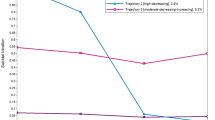
For both suicide attempts and ideation, there was evidence to suggest that young people in the US could fall into different developmental trajectories across the period from early adolescence to mid-adulthood (see Figs. 2 and 3, respectively, where the predicted probability of the outcome occurring is plotted by year of age based on modeling results). There is a subgroup whose past 12-month risk is largely confined to the period between ages 12–19 years (9.2% had suicidal thoughts, and 4.6% were classified as attempters with a predicted probability of ~0.18–0.31 of one attempt and 0.10 to 0.18 of multiple attempts). For suicidal thoughts, there is also a subgroup with higher sustained risk (predicted probability of ~0.50–0.55) across the entire studied range from 12 to 31 years (8.0% with consistent ideation).

Trajectories of suicide ideation in past year

Trajectories of suicide attempt categories in past year
Further, there is evidence of associations with race/ethnicity, which appear protective for African Americans and appear to indicate increased risk for Asians and Pacific Islanders (see Table 2). GMM analyses resulted in three trajectory classes for suicide ideation representing sustained higher risk, sustained lower risk, and adolescent-limited risk. In particular, African Americans had 53% lower odds than non-Hispanic Whites (AOR = 0.47, 95% CI = [0.29, 0.75], p = 0.002) to be in the sustained higher risk trajectory for suicide ideation (again ~8.0% of all) versus in the sustained lower risk trajectory, controlling for gender, socioeconomic status, discrimination, baseline depressive symptoms, and classification uncertainty. Among the 9.2% of participants that had suicide ideation during adolescence, African American participants had 77% lower odds relative to non-Hispanic Whites (AOR = 0.23, 95% CI = [0.08, 0.63], p = 0.004) of being in this trajectory relative to being in the sustained lower risk trajectory.
For suicide attempts category (no attempts, 1 attempt, >1 attempt), two trajectory classes emerged with ~95.4% as members of a no attempts trajectory (predicted probability < 0.02 across all ages) and 4.6% in an “attempters” trajectory where the predicted probability of single or multiple attempts were higher in younger ages (entropy = 0.85, lowest AIC = 7421.4, SSA-BIC = 7450.4; all LRTs with more classes nonsignificant). Further, African Americans had 79% lower odds compared to non-Hispanic White participants (AOR = 0.21, 95% CI = [0.06, 0.72], p = 0.013) of being in more frequently attempting suicide attempts category relative to the no attempts risk trajectory.
Asians and Pacific Islanders (about 1.7% of all respondents) had almost four times the odds of being in a more frequently attempting risk trajectory for suicide attempts as non-Hispanic Whites had relative to the sustained lower risk trajectory (AOR = 3.73, 95% CI = [0.87, 16.0]), however this effect was only marginally significant (p = 0.076). Of note, when attempts were analyzed as a dichotomous variable rather than an ordinal variable with three categories in post hoc sensitivity analyses, three trajectory classes emerged, and Asian and Pacific Islanders had more than five times the odds of being in the higher sustained risk trajectory for suicide attempts compared with non-Hispanic Whites, and the association was statistically significant (AOR = 5.49, p = 0.04).
Discussion
Research indicates that race, ethnicity, and culture play a role in the development of suicidal thoughts and behavior (Colucci et al. 2013). However, the field of suicide prevention is still in a nascent stage of understanding racial/ethnic and cultural differences in suicide-related behaviors across the life course and exploring the pathways that may contribute to these differences (Joe et al. 2008a). The research questions of this study centered on quantifying developmental trajectories and exploring racial/ethnic differences in these trajectories from adolescence into mid-adulthood. Informed by Meyer’s Minority Stress Model (Meyer 2003) and other theoretical and empirical work on minority stress, this study also investigates whether structural discrimination experienced in adolescence (from peers and from teachers) moderates the relationship between race/ethnicity and trajectory class.
The findings of this study suggest that across a wide span of the life course, ages 12–31 years, there are distinct developmental trajectories for suicide ideation and suicide attempts. Similar to prior research, the current study found that adolescence can be a time of increased likelihood of suicide ideation or attempts (Substance Use and Mental Health Services Administration 2014). Further, results showed these suicide-related outcomes were reported at all ages under study, through mid-adulthood. In analyses conducted separately for past-year suicide ideation, three distinct developmental trajectories emerged: a sustained higher-risk trajectory, a sustained low-risk trajectory, and an adolescent-limited risk trajectory. For suicide attempts, two developmental trajectories emerged: higher-risk trajectories of single or multiple attempters and a sustained low-risk trajectory.
After controlling for gender, socioeconomic status, structural discrimination, and prior depressive symptoms, the odds of experiencing a particular trajectory varied by race/ethnicity. For past-year suicidal thoughts, African Americans had significantly lower odds than Whites of being in either the sustained higher-risk trajectory or the adolescent-limited risk trajectory. This is consistent with prior findings from the National Comorbidity Study, which showed that in a general-population adult sample, African Americans tend to have lower risk than Whites for suicidal thoughts, planning, and attempts (both impulsive and planned) (Kessler et al. 1999). This is in contrast, however, with other studies that have shown essentially no difference by race/ethnicity in frequency or severity of suicidal thoughts (Gutierrez et al. 2005) or attempts (Kim et al. 2011), at least among adolescents. For past-year suicide attempts, African Americans had significantly lower odds than Whites while Asian/Pacific Islanders had marginally higher odds than Whites of being in the single or multiple attempts trajectories. These findings expand previous studies showing that Asian/Pacific Islanders in some age groups may be at greater risk for suicide than White youth or adults (Balis and Postolache 2008).
This study has important limitations. First, the measure of race/ethnicity in this study treated several heterogeneous groups as single groups. The Asian and Pacific Islander racial/ethnic category, for example, included immigrants and US-born persons with heritage from many very different Asian and Pacific Island countries, with potentially vastly different languages, ethnicities, religions, and other aspects of culture. This analysis of secondary data did not allow the examination of the degree to which members of any racial/ethnic category may share cultural influences. However, there may be shared values and beliefs related to suicide at work, such as how illness is defined, the role of family, and the structure of social networks (Balis and Postolache 2008). Additional research is needed to examine these issues.
The current study also exclusively focused on self-report of past-year suicidal thoughts and attempts. This is important for several reasons. First, under-diagnosis of depression in African Americans has been documented (Stevenson et al. 2003), and depressive symptoms are linked to suicidal thoughts and behaviors. An evaluation of one suicide-prevention program found African American youth were less likely than White and Latino youth to report suicidal thoughts; those who did report suicidal thoughts were less likely than youth in other racial/ethnic groups to receive help (Aseltine and DeMartino 2004). It is possible that some of the same factors that result in under-diagnosis of depression among African Americans also result in lower self-reports of suicide ideation among African Americans in the Add Health sample as compared to their White peers. As Joe and colleagues note, there is a strong social stigma around suicide, which may be more acutely experienced by racial/ethnic minorities and particularly African Americans (Joe et al. 2008b). Similarly, literature suggests that Asian American youth with mental health concerns may be less likely than White youth to seek or receive the help they need (Pirkis et al. 2003). This study attempted to address this issue by controlling for baseline depressive symptoms in analyses.
The current study examined some but not all the mechanisms that create or reinforce racial/ethnic differences in self-reported suicide-related outcomes. This study did examine whether experiences of structural discrimination mediated or moderated the race/ethnicity-trajectory class association for both suicide-related outcomes. Because the only discrimination measures available in the Add Health data were two single items about structural discrimination relating to peers and teachers, future studies should continue to explore the role of other discrimination experiences in the development of suicide-related thoughts and behaviors across racial/ethnic groups. Based on the finding that African American adolescents and adults experience lower risk than Whites for suicide ideation and attempts, future studies should examine protective factors that result in this reduced likelihood. With regard to the marginally-significant finding that Asian Americans may experience increased risk relative to Whites for suicide attempts across adolescence and well into mid-life, future research is needed on individual, family, and structural factors that may contribute to and sustain this risk, and the potential importance of the timing of risk exposures. Research is needed on the role of group and individual beliefs about mental illness and suicide, health care access, and provider issues such as culturally appropriate patient engagement and care.
Finally, the current study did not control for the intent or lethality of the method of suicide attempt, which may influence both rates and the association of race/ethnicity to trajectory classes. This issue is particularly important if lethality of method varies by racial/ethnic group, which some research has shown (Stack and Wasserman 2005).
Despite these limitations, this study makes important contributions to the developmental understanding of suicide-related outcomes. The analytic approach, the span of ages covered, and the findings themselves regarding racial/ethnic differences in likelihood of experiencing a particular trajectory extend the understanding of suicide-related behaviors and provide new directions for future research and prevention interventions.
Conclusion
Longitudinal research on suicide-related outcomes that extends beyond adolescence is rare, and little is known about racial/ethnic variation in the likelihood of experiencing a particular developmental trajectory. Using a person-oriented approach (growth mixture modeling), this study examined patterns in suicide ideation and attempts across a wide span of life course development, while retaining individual focus. This study has several implications for future research and practice in suicide prevention. First, adolescents in general need developmentally targeted interventions to address their suicidal thoughts. Second, expanding upon theories of minority stress (Meyer 2003; Smedley et al. 1993), racial/ethnic minority adolescents may need tailored interventions to help them deal with self-doubts about fitting in with the majority group, which may interfere with their social integration and negatively affect their social support. They may also benefit from opportunities to act as agents of change in the face of discrimination and structural racism. More fundamentally, structural interventions that address the dual issues of suicide stigma and structural discrimination are needed to address the root causes and have the potential to improve suicide prevention. Finally, because Asian Americans are suggested to be at greatest risk for suicide ideation and attempts, this group may need particular attention. Preventive interventions are needed that address individual, family, and social-structural issues at different developmental stages associated with this increase in risk behaviors. More research is warranted to examine mechanisms by which racial identity and experiences are linked to coping mechanisms, mental health, and suicide behaviors.
References
Add Health. (2016). What is the best way to compute race in the Add Health Wave I in-home data? http://www.cpc.unc.edu/projects/addhealth/faqs/aboutdata/index.html#RACE. Accessed 20 Mar 2018.
Aseltine, R. H., & DeMartino, R. (2004). An outcome evaluation of the SOS suicide prevention program. American Journal of Public Health, 94(3), 446–451.
Asparouhov, T., & Muthén, B. (2014). Auxiliary variables in mixture modeling: three-step approaches using Mplus. Structural Equation Modeling: A Multidisciplinary Journal, 21(3), 329–341. https://doi.org/10.1080/10705511.2014.915181.
Balis, T., & Postolache, T. T. (2008). Ethnic differences in adolescent suicide in the United States. International journal of child health and human development, 1(3), 281–296.
Bergman, L. R., & Lundh, L.-G. (2015). The person-oriented approach: Roots and roads to the future. Journal for Person-Oriented Research, 1(1–2), 1–6.
Borges, G. (2012). Suicidality, ethnicity and immigration in the USA. Psychological Medicine, 42, 1175–1184. https://doi.org/10.1017/S0033291711002340.
Borges, G., Angst, J., Nock, M. K., Ruscio, A. M., & Kessler, R. C. (2008). Risk factors for the incidence and persistence of suicide-related outcomes: A 10-year follow-up study using the National Comorbidity Surveys. Journal of Affective Disorders, 105(1), 25–33. https://doi.org/10.1016/j.jad.2007.01.036.
Burnham, K. P., & Anderson, D. R. (2010). Model Selection and Multimodel Inference: A Practical Information-Theoretic Approach. 2nd ed. New York, NY: Springer. https://www.springer.com/us/book/9780387953649. Accessed 14 June 2019.
CDC, & NCHS. (2017). National Vital Statistics System, United States, 2017. Web-based Injury Statistics Query and Reporting System [WISQARS]. https://webappa.cdc.gov/sasweb/ncipc/leadcause.html. Accessed 8 Jun 2019.
Celeux, G., & Soromenho, G. (1996). An entropy criterion for assessing the number of clusters in a mixture model. Journal of Classification, 13(2), 195–212.
Centers for Disease Control and Prevention (CDC). (2018). 1991–2017 High school youth risk behavior survey data. https://nccd.cdc.gov/Youthonline/App/Default.aspx. Accessed 8 Jun. 2019.
Chen, P., & Chantala, K. (2014). Guidlines for Analyzing Add Health data. (pp. 53). Chapel Hill, NC: Carolina Population Center, University of North Carolina at Chapel Hill. http://www.cpc.unc.edu/projects/addhealth/documentation/guides/wt_guidelines_20161213.pdf.
Colucci, E., Lester, D., Hjelmeland, H. & Park, B. C. B. (Eds.) (2013). Suicide and Culture: Understanding the Context. Cambridge, MA, US: Hogrefe Publishing.
Curtin, S. C., Warner, M., & Hedegaard, H. (2016). Increase in suicide in the United States, 1999–2014. NCHS Data Brief, no. 241. Hyattsville, MD: National Center for Health Statistics. https://www.cdc.gov/nchs/products/databriefs/db241.htm. Accessed 3 Oct 2017.
Dahl, R. E., Allen, N. B., Wilbrecht, L., & Suleiman, A. B. (2018). Importance of investing in adolescence from a developmental science perspective. Nature, 554(7693), 441–450. https://doi.org/10.1038/nature25770.
Eaton, W. W., Smith, C., Ybarra, M., Muntaner, C., & Tien, A. (2004). Center for Epidemiologic Studies Depression Scale: review and Revision (CESD and CESD-R). In M. E. Maruish (Ed.), The use of psychological testing for treatment planning and outcomes assessment: Instruments for adults (pp. 363–377). Mahwah, NJ, US: Lawrence Erlbaum Associates Publishers.
Elgin, J. E. (2014, October 13). Examining the Relationships Between Suicidal Ideation, Substance Use, Depressive Symptoms, and Educational Factors in Emerging Adulthood. Thesis. https://digital.lib.washington.edu:443/researchworks/handle/1773/26285.
Enders, C. K. (2010). Applied missing data analysis. New York, NY: Guilford Press.
Galbraith, S., Bowden, J., & Mander, A. (2017). Accelerated longitudinal designs: an overview of modelling, power, costs and handling missing data. Statistical Methods in Medical Research, 26(1), 374–398. https://doi.org/10.1177/0962280214547150.
Goldman-Mellor, S. J., Caspi, A., Harrington, H., Hogan, S., Nada-Raja, S., Poulton, R., & Moffitt, T. E. (2014). Suicide attempt in young people: a signal for long-term health care and social needs. JAMA Psychiatry, 71(2), 119–127. https://doi.org/10.1001/jamapsychiatry.2013.2803.
Graubard, B. I., & Korn, E. L. (1996). Survey inference for subpopulations. American Journal of Epidemiology, 144(1), 102–106.
Gutierrez, P. M., Muehlenkamp, J. J., Konick, L. C., & Osman, A. (2005). What role does race play in adolescent suicidal ideation? Archives of Suicide Research, 9(2), 177–192. https://doi.org/10.1080/13811110590904025.
Harris, K. M. (2009). The National Longitudinal Study of Adolescent to Adult Health (Add Health), Waves I & II, 1994–1996; Wave III, 2001–2002; Wave IV, 2007–2009 [machine-readable data file and documentation]. Chapel Hill, NC: Carolina Population Center, University of North Carolina at Chapel Hill. 10.3886/ICPSR27021.v9.
Hottes, T. S., Bogaert, L., Rhodes, A. E., Brennan, D. J., & Gesink, D. (2016). Lifetime prevalence of suicide attempts among sexual minority adults by study sampling strategies: a systematic review and meta-analysis. American Journal of Public Health, 106(5), e1–e12.
Joe, S., Canetto, S. S., & Romer, D. (2008a). Advancing prevention research on the role of culture in suicide prevention. Suicide and Life-Threatening Behavior, 38(3), 354–362. https://doi.org/10.1521/suli.2008.38.3.354.
Joe, S., Canetto, S. S., & Romer, D. (2008b). Advancing prevention research on the role of culture in suicide prevention. Suicide and Life-Threatening Behavior, 38(3), 354–362. https://doi.org/10.1521/suli.2008.38.3.354.
Kessler, R. C., Borges, G., & Walters, E. E. (1999). Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Archives of General Psychiatry, 56(7), 617–626.
Kim, J. L., Kim, J. M., Choi, Y., Lee, T.-H., & Park, E.-C. (2016). Effect of socioeconomic status on the linkage between suicidal ideation and suicide attempts. Suicide and Life-Threatening Behavior, 46(5), 588–597.
Kim, Y. J., Moon, S. S., & Kim, M. J. (2011). Physical and psycho-social predictors of adolescents’ suicide behaviors. Child and Adolescent Social Work Journal, 28(6), 421–438. https://doi.org/10.1007/s10560-011-0241-1.
Lo, Y., Mendell, N. R., & Rubin, D. B. (2001). Testing the number of components in a normal mixture. Biometrika, 88(3), 767–778.
Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychological Bulletin, 129(5), 674–697. https://doi.org/10.1037/0033-2909.129.5.674.
Moradi, B. (2013). Discrimination, Objectification, and dehumanization: toward a pantheoretical framework. In Objectification and (de)humanization (pp. 153–181). Springer, New York, NY. https://doi.org/10.1007/978-1-4614-6959-9_7.
Muthén, L., & Muthén, B. (2015). Mplus v7.3. Los Angeles, CA: Muthén & Muthén.
Olfson, M., Blanco, C., Wall, M., Liu, S.-M., Saha, T. D., Pickering, R. P., & Grant, B. F. (2017). National trends in suicide attempts among adults in the United States. JAMA Psychiatry, 74(11), 1095–1103.
Park, E., McCoy, T. P., Erausquin, J. T., & Bartlett, R. (2018). Trajectories of risk behaviors across adolescence and young adulthood: the role of race and ethnicity. Addictive Behaviors, 76, 1–7.
Pirkis, J. E., Irwin, C. E., Brindis, C. D., Sawyer, M. G., Friestad, C., Biehl, M., & Patton, G. C. (2003). Receipt of psychological or emotional counseling by suicidal adolescents. Pediatrics, 111(4), e388–e393.
Ram, N., & Grimm, K. J. (2009). Methods and measures: growth mixture modeling: a method for identifying differences in longitudinal change among unobserved groups. International Journal of Behavioral Development, 33(6), 565–576.
SAS Institute. (2012). SAS. Cary, NC: SAS Institute.
Séguin, M., Beauchamp, G., Robert, M., DiMambro, M., & Turecki, G. (2014). Developmental model of suicide trajectories. The British Journal of Psychiatry, 205(2), 120–126. https://doi.org/10.1192/bjp.bp.113.139949.
Sellers, R. M., Copeland‐Linder, N., Martin, P. P., & Lewis, R. L. (2006). Racial Identity Matters: the relationship between racial discrimination and psychological functioning in african american adolescents. Journal of Research on Adolescence, 16(2), 187–216. https://doi.org/10.1111/j.1532-7795.2006.00128.x.
Smedley, B. D., Myers, H. F., & Harrell, S. P. (1993). Minority-status stresses and the college adjustment of ethnic minority freshmen. The Journal of Higher Education, 64(4), 434–452. https://doi.org/10.2307/2960051.
Stack, S., & Wasserman, I. (2005). Race and method of suicide: culture and opportunity. Archives of Suicide Research: Official Journal of the International Academy for Suicide Research, 9(1), 57–68. https://doi.org/10.1080/13811110590512949.
Stevenson, H. C., Davis, G. Y., Herrero-Taylor, T., & Morris, R. (2003). Boys, not men: hypervulnerability in African American youth. In Playing with anger: teaching coping skills to African American boys through athletics and culture (3–20).
Substance Use and Mental Health Services Administration. (2014). Results from the 2013 National Survey on Drug Use and Health: mental health findings (NSDUH Series H-49). Rockville, MD: Substance Abuse and Mental Health Services, 2014. http://www.samhsa.gov/data/sites/default/files/NSDUHmhfr2013/NSDUHmhfr2013.pdf. (No. HHS Publication No. (SMA) 14-4887).
Supple, A. (2013). Ethnic, gender, and age differences in adolescent nonfatal suicide behaviors. Death Studies, 37, 830–847. https://doi.org/10.1080/07481187.2012.699909.
Walker, R. L., Wingate, L. R., Obasi, E. M., & Joiner, T. E. (2008). An empirical investigation of acculturative stress and ethnic identity as moderators for depression and suicidal ideation in college students. Cultural Diversity & Ethnic Minority Psychology, 14(1), 75–82. https://doi.org/10.1037/1099-9809.14.1.75.
Xu, J. (2017). QuickStats: average number of deaths from motor vehicle injuries, suicide, and homicide, by day of the week — National Vital Statistics System, United States, 2015. MMWR, 66. https://doi.org/10.15585/mmwr.mm6622a5.
Acknowledgements
This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill, and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. Special acknowledgment is due Ronald R. Rindfuss and Barbara Entwisle for assistance in the original design. Information on how to obtain the Add Health data files is available on the Add Health website (http://www.cpc.unc.edu/addhealth). No direct support was received from grant P01-HD31921 for this analysis.
Authors’ Contributions
J.T.E conceptualized data analysis, summarized relevant extant empirical and theoretical research, interpreted results, and led the writing and revision of the manuscript; T.P.M. participated in the design, performed statistical analyses, participated in the interpretation of data, drafted the methods section of the manuscript, and participated in revisions; R.B. summarized relevant extant empirical and theoretical research, contributed to interpretation of results, drafted the discussion section, and participated in revisions; E.P. conceptualized data analysis, contributed to the introduction/background on theory, and participated in revisions. All authors read and approved the final manuscript.
Data Sharing and Declaration
The data that support the findings of this study are available from Add Health, a program project at the University of North Carolina at Chapel Hill. Restrictions apply to the availability of these data, which were used under license for the current study. Information on how to obtain the Add Health data files is available on the Add Health website (http://www.cpc.unc.edu/addhealth).
Funding
The authors received no funding support for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
ll procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Erausquin, J.T., McCoy, T.P., Bartlett, R. et al. Trajectories of Suicide Ideation and Attempts from Early Adolescence to Mid-Adulthood: Associations with Race/Ethnicity. J Youth Adolescence 48, 1796–1805 (2019). https://doi.org/10.1007/s10964-019-01074-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-019-01074-3