
Abstract
Parents and children with high negative emotionality may be more likely to provide and receive non-supportive contingencies, respectively. However, no study has examined child and parent negative emotionality in the same study and explored whether the link between child and parent negative emotionality may exist in part because of parental emotion socialization. The present study was designed to explore the link between the negative emotionality of mothers and their adolescent children and the potential mechanisms for this similarity. Maternal emotion socialization was explored as a mediator between maternal and adolescent negative emotionality, and between maternal negative emotionality and adolescent internalizing symptoms. Participants were mothers (M age = 30.47) with their children at two time points: preschool (Time 1; M age = 4.55 years old) and adolescence (Time 2; M = 13.73), with 81 boys and 94 girls. Negative emotionality was measured using a questionnaire, with mothers reporting for herself and her child. Maternal emotion socialization was measured by mothers’ self-report of their contingencies to their adolescent child’s negative emotions: 1) Punish; 2) magnify; 3) ignore; 4) override; and 5) support. The results revealed that the maternal punishing of the adolescent’s negative emotions was a mediator between concurrent mother negative emotionality and adolescent negative emotionality, such that higher mother negative emotionality was associated with more punishing, and more punishing was associated with higher adolescent negative emotionality, controlling for previous levels of maternal and child negative emotionality. Furthermore, being supportive of a child’s negative emotions was negatively associated with concurrent levels of adolescent internalizing symptoms, while magnifying a child’s emotions held a marginal positive association, controlling for previous levels of internalizing symptoms. The results highlight the importance of considering maternal emotion socialization strategies, even into adolescence, for a more comprehensive understanding of children’s emotional well-being. The findings have implications for developing and implementing emotion-based parenting interventions.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Many factors contribute to the way that parents interact with their children. Some of these factors relate to the characteristics of the parent, while others are linked to the characteristics of the child. Certain traits or behavioural styles may predispose the parent and the child to react to scenarios in either healthy or unhealthy ways, leading the dyad to develop patterns of behaviour that teach the child long-lasting lessons about their emotions and behaviour. In particular, the emotional well-being of parents and their children has been linked. One way this connection may be maintained is because the emotional disposition of the parent and the child can impact the way that the child is taught about and understands their own emotions. In the present study, the link between parent and child emotional well-being was explored, to better understand how a tendency towards experiencing negative emotions can relate to the parenting behaviour of emotion socialization.
Negative Emotionality is defined as a person’s tendency to react to stressors with strong negative emotions, such as anger, fear or sadness (Rothbart 2011). This emotional reactivity is considered to be a part of temperament, reflecting that it is a dispositional tendency that remains fairly stable from birth until death. Research suggests that negative emotionality is associated with a myriad of problems later in life, especially internalizing problems and symptoms, such as worrying, nervousness, poor self-concept, sadness, loneliness, and somatization symptoms (Klein et al. 2012). Consistent with the stress-diathesis model, Kopala-Sibley and colleagues (2016) provided evidence that children in early to middle childhood with high negative emotionality who are exposed to a traumatic event (e.g., natural disaster) are much more likely to develop psychopathology, such as depression or anxiety, than children who do not have high negative emotionality. Even for those not exposed to an acute event, high negative emotionality ratings during infancy (e.g., Karevold et al. 2009) and preschool (e.g., Dougherty et al. 2011) are predictive of later internalizing symptoms at school age and even during early adolescence. Moreover, a recent longitudinal study by Hagan et al. (2016) showed that negative emotionality in middle to late childhood predicted internalizing symptoms in early adulthood approximately 15 years later, even after controlling for internalizing symptoms in childhood. Taken together, the current literature identifies high negative emotionality in childhood and adolescence as a potential risk factor for future internalizing problems (Klein et al. 2012; Kovacs and Lopez-Duran 2010).
As a component of temperament, negative emotionality is considered to be at least partially genetically or biologically determined. Consequently, it would be expected that parents may pass on their high or low negative emotionality to their biological children. Indeed, research with children aged three to five suggests that mothers and their children tend to be similar in terms of their level of negative emotionality (e.g., Crawford et al. 2011). However, previous studies have shown that although a large part of negative emotionality’s stability throughout life is biologically determined, its variability throughout developmental stages may be attributed to environmental influences, particularly parenting (Propper and Moore 2006). As a result, the similarity in negative emotionality that parents and their children may share may also be due to factors outside of genetics. The negative emotionality of parents and children may influence the way they interact with each other and the type of behaviour they elicit from each other. For example, mothers with higher negative emotionality tend not to possess or show some of the traits that lend themselves to fostering adequate emotional development in children, such as responsiveness (Woodruff-Borden et al. 2002) and nurturance (Metsäpelto and Pulkkinen 2003), and tend to use more harsh parenting practices in general in early childhood samples (e.g., Leung and Slep 2006). In addition, parents of children with high negative emotionality tend to use parenting approaches that further exacerbate their child’s emotion dysregulation, both in middle childhood (Lengua and Kovacs 2005) and early adolescence (Davenport et al. 2011). It is perhaps in these ways that parents and their children with high negative emotionality may maintain it, through the ways that the parent reacts towards their child but also through the ways that their child elicits certain parenting behaviours from them (Moed et al. 2017). The present study was designed to explore how negative emotionality relates to parenting, and how this in turn can play a role in adolescents’ emotional well-being, specifically negative emotionality and internalizing symptoms.
When considering a parent’s role in a child’s healthy emotional development, a critical parenting practice is socialization. Emotion socialization is the process by which parents teach their children to be emotionally competent (Eisenberg et al. 1999). Specifically, socialization can either occur directly, such as when a parent coaches their child in emotional situations, or indirectly, such as when a parent models emotional reactions to stressful situations unintentionally. One area of socialization research that is receiving more attention recently is the direct emotion socialization technique of emotion contingencies. Contingencies refer to the way a parent responds to negative emotions, and these responses can teach children important lessons about experiencing and expressing negative emotions (Jones et al. 2002). According to Tomkins’ Affect theory (Tomkins 1963, 1991), children whose emotions are rewarded and supported, whether they are negative or positive emotions, will have healthier emotional development. O’Neal and Magai (2005) elaborated on Tomkins’ Affect theory, and explored non-supportive responses to negative emotions (i.e., sadness, anger and fear) of pre- and early adolescent children. These non-supportive contingencies included punishing the emotion by providing negative sanctions to the child, magnifying the emotion by matching or exceeding it, ignoring the emotional display, or overriding or minimizing the emotion by dismissing it. O’Neal and Magai (2005) suggest that these non-supportive strategies may teach the child that their parent does not approve of the expression of negative emotions, while the child is not necessarily taught how to cope with their negative emotions (Brand and Klimes-Dougan 2010). Thus, the child may try to reduce their negative emotions in order to garner their parent’s approval, albeit in inappropriate or ineffective ways. In contrast, supportive contingencies, such as comforting the child when they are experiencing a negative emotion, help teach the child that there are ways to deal with negative emotions and that negative emotions are a part of everyday life (see Zeman et al. 2013 for a review).
Emotion socialization strategies have been shown to have a specific impact on emotional well-being in childhood from preschool (e.g., Fabes et al. 2001; Hooper et al. 2018) to middle childhood (e.g., Hurrell et al. 2015; Silk et al. 2011), with non-supportive contingencies being associated with emotional problems and supportive contingencies being associated with better emotional outcomes. However, there is a dearth of research on emotion socialization techniques in adolescence specifically (Zeman et al. 2013). This is unfortunate because adolescence is a critical period in emotional development, as adolescents’ relationships become more complex and authority figures hold them to higher standards (Brand and Klimes-Dougan 2010). In addition, similar to the toddler and preschool age periods, some researchers argue that adolescence is a developmental period that is notable for more frequent and/or more intense negative emotions (e.g., Larson et al. 2002), including depression symptoms (Garber et al. 2002). Furthermore, some research suggests that, following a decline in middle childhood, non-supportive contingencies tend to rise and become more prominent in early adolescence, emphasizing the importance of this time in parents’ and adolescents’ emotional lives (e.g., Eisenberg et al. 1999).
Consistent with research with children, the available research on adolescents suggests that being non-supportive of negative emotions has harmful consequences. Klimes-Dougan and colleagues (2007) endeavored to discover how parents socialize their adolescents’ emotions in an exploratory study. They found that as adolescents became older, their parents tended to be less supportive and more punitive of their negative emotions. Other researchers have explored the emotional implications of these findings. For example, O’Neal and Magai (2005) reported that non-supportive contingencies, such as punishment or neglecting/ignoring the negative emotion, were associated with higher levels of internalizing and externalizing symptoms in early adolescence. Recent research suggests that adolescents with high levels of depression symptoms are more likely to also experience higher levels of non-supportive parental contingencies, as compared to healthy controls (e.g., Shortt et al. 2016; for a review, see Schwartz et al. 2012). For example, in an observational study, mothers who used more non-supportive contingencies to their adolescent’s fear or sadness, such as acting angry, being rejecting or being self-focused, had children with more internalizing problems and depression symptoms (Hastings et al. 2014). In addition, supportive emotion socialization, such as providing comfort, empathizing, and problem solving was associated with fewer internalizing problems in the same study (Hastings et al. 2014). Taken together, there is some research to suggest that the way a parent responds to his/her adolescent’s negative emotions may have important implications for their emotional well-being.
Considering the biological and environmental influences on negative emotionality and its implications for later psychopathology, the study of negative emotionality is best explored through the lens of developmental psychopathology (Cicchetti and Curtis 2007). This model posits that both the characteristics of the individual, such as negative emotionality, as well as their rearing environment, such as maternal emotion socialization, must be considered in the etiology of psychopathology. In addition to their genetic contribution, it is possible that emotion socialization may be one of the pathways through which parents reinforce their high negative emotionality in their children. Specific to emotion socialization, previous research has shown that mothers with current or histories of poor emotion regulation capabilities or more negative affect are more likely to use non-supportive strategies, such as punishing or neglecting their child’s negative emotions, with children in preschool and early childhood (Fabes et al. 2001; Silk et al. 2011), early to middle childhood (Arellano et al. 2018; Han et al. 2015) and pre-adolescence to adolescence (Buckholdt et al. 2014; Hughes and Gullone 2010). However, recent research has shown no association between higher levels of maternal negative affect (e.g., depression) and non-supportive contingencies with toddlers (Premo and Kiel 2016). It is also possible that children with high negative emotionality may elicit non-supportive contingencies from their parents. Previous research with preschoolers has suggested that children with higher levels of negative emotionality tend to experience higher levels of punishment with regard to their negative emotions (Eisenberg and Fabes 1994). Moreover, an experimental manipulation with undergraduate students showed that tactics that dismiss a young person’s negative emotional experience may in turn intensify their negative emotional reactivity (Shenk and Fruzzetti 2011). Of note, children who are more emotionally labile are more likely to benefit from supportive emotion contingencies and thus reduce their risk of developing behavior problems (Dunsmore et al. 2016).
Current Study
Although there is some research to support that parents and children with high negative emotionality may be more likely to provide and receive non-supportive contingencies respectively, no study has examined child and parent negative emotionality in the same study and explored whether the link between child and parent negative emotionality may exist in part because of parental emotion socialization. The present study was designed to examine the similarity of mother and adolescent negative emotionality, and negative emotionality’s potential contribution to the development of internalizing symptoms. Moreover, the role of maternal emotion socialization, specifically, contingencies to negative emotions, in the emotional well-being of adolescents was explored, controlling for their emotionality earlier in childhood. Given that maternal negative emotionality is associated with harsher parenting practices, including non-supportive contingencies, and that harsher emotion socialization practices are associated with worse socio-emotional functioning, maternal emotion socialization was hypothesized as a psychosocial pathway by which mothers’ and their children’s similar negative emotionality may be partly explained.
This study had three objectives with associated hypotheses. The first objective was to establish the positive concurrent association between mothers’ negative emotionality and both their adolescents’ levels of negative emotionality as well as their adolescents’ internalizing symptoms (Objective #1). The second objective was to evaluate whether maternal contingencies, both non-supportive (i.e., punishing, magnifying, ignoring or overriding their child’s negative emotion) and supportive (i.e., providing comfort and support), mediate the association between maternal negative emotionality and both of the adolescent emotional outcomes (i.e., negative emotionality and internalizing symptoms; Objective #2). Finally, the third objective was to explore whether the mediated relation between maternal negative emotionality and adolescent internalizing symptoms remains after controlling for the mediating effect of adolescent negative emotionality (Objective #3). Based on previous findings in the literature with other age groups and similar constructs, it was hypothesized that mothers’ negative emotionality would be positively associated with adolescent negative emotionality. In addition, mothers with high negative emotionality were hypothesized to be more likely to respond to their child’s negative emotions in a non-supportive manner and less likely to respond in a supportive manner. In turn, non-supportive maternal contingencies were hypothesized to relate to higher adolescent negative emotionality and internalizing symptoms, while supportive maternal contingencies were hypothesized to be associated with lower adolescent negative emotionality and internalizing symptoms.
Methods
Participants
The participants in the current study derive from the original larger longitudinal sample of the Concordia Project. The original recruitment for the Concordia Project was conducted in 1976-77, whereby 4,109 elementary school students in grades 1, 4 and 7 from francophone low-income neighbourhoods in Montreal, Canada were screened (Schwartzman et al. 1985; Serbin et al. 1998; Stack et al. 2015). The present study is composed of original participants, both male and female, who became parents and had a preschool child at the time of recruitment. There were 175 eligible families, with either a father or mother who was an original participant in the 1976 original data collection for the study. All of the objectives were explored using this sub-sample, in which mothers and their preschool-aged children were followed into adolescence. Ethics approval was granted by Concordia University to Serbin, Stack and Schwartzman (Time 1) and to Serbin and Stack (Time 2) for research at each separate time point (i.e., Time 1 [Identification and prediction of risk and resiliency in high-risk preschoolers: An intergenerational study.], and Time 2 [Navigating the transition to adolescence: Predicting continuity vs. discontinuity of risk within a disadvantaged longitudinal sample of children.]). It is worthy to note that although data is available for original male participants at previous time points, data from the father’s perspective, whether he be an original participant or not, was limited. Fathers were asked to complete few if any questionnaires at each time point, and the level of missingness was often very high (e.g., above 70%), particularly for the data required to answer the present study’s research questions. Because of the missing data fathers’ questionnaire data were not included in this study.
With regard to demographic values, the mean age of mothers as of data collection at Time 1 was 30.44 years (SD = 3.35; n = 175). The age at which these mothers had their first child ranged from 16.42 to 36.84, with an average age of 24.86 (SD = 3.39). The marital status of the mothers at Time 1 included single (n = 16; 9.1%), cohabitating (n = 78; 44.6%), married (n = 67; 38.3%), separated (n = 10; 5.7%), divorced (n = 3; 1.7%) and widowed (n = 1; 0.6%). The average number of years of education of the mothers was 11.77 when collected at Time 1; in order to graduate from high school in Quebec, 11 years of education is required. The maximum family prestige score (Standard International Occupational Prestige Scale; Treiman 1977) was an average of 38.41, which could include jobs such as manufacturing laborers (e.g., chemical processors, tobacco preparers, sheet metal workers, etc.), and service workers (e.g., guides, tailors, etc.) At Time 1, the ages of the child participants ranged from 1.96 to 7.46 years and the average age was 4.55 (SD = 1.54). There were 81 boys and 94 girls (n = 175). At Time 2, the age of child participants ranged from 11.64 to 17.26 (M = 13.76, SD = 1.19), with 57 males and 63 females (n = 120). In order to investigate the potential influence of attrition, a series of t-tests were run to determine whether there were differences between retained participants and those who dropped out by Time 2 on study variables and demographic variables at Time 1. No differences were found on study variables at Time 1, on maternal education, maternal age, and on maternal age at the birth of their first child (t = 0.57 to 1.72, p = 0.09 to 0.57, d = 0.09 to 0.29). Mothers who dropped out of the study by Time 2 had lower family prestige (t(170) = 2.08, p = 0.04, d = 0.34), when compared to mothers who participated at Time 2. Therefore, family prestige was controlled where possible. Additional t-tests revealed that mothers increased in years of education (t(143) = 2.23, p = 0.03, d = 0.11), and family prestige (t(84) = 4.73, p < 0.001, d = 0.52) from Time 1 to Time 2.
Measures
Demographic information
Socio-demographic information, such as child’s age and sex and mothers’ level of education in number of years, was collected using the Demographic Information Questionnaire (DIQ). This measure has proven effective in collecting participant demographics, and has been used in past studies of the Concordia Project (e.g., Enns et al. 2015; Martin et al. 2012).
Negative emotionality
Children
Mothers completed the Emotionality Activity Sociability Scale (EAS-2; Buss and Plomin 1986) questionnaire at all three time points on behalf of their children. The EAS is a measure of temperament that includes: Emotionality, i.e., the tendency to react to a stressor with strong negative emotions or distress; Activity, i.e., the tendency to be restless or energetic; and Sociability, i.e., the tendency to prefer to be in the company of others rather than alone and to find social interactions rewarding. Only the Emotionality subscale total score, which consists of 5 items, was used in this study. Example items include: “Cries easily”, or “Reacts intensely when upset”. Each item is rated on a likert-type scale from 1 (my child’s behaviour is never like this) to 5 (my child’s behaviour is always like this). Previous research has demonstrated that this measure has good test-retest reliability (e.g., r = 0.82) and internal consistency (e.g., Anthony et al. 2002; Bould et al. 2013; Spence et al. 2013). For the present sample, analyses revealed a Cronbach’s alpha of 0.75 for Time 1, and 0.85 for Time 2.
Mothers
Mothers completed the self-report adult version of the EAS-2 (Buss and Plomin 1984) at Time 1 and Time 2. The total scores for each of the Emotionality subscales, Distress, Anger and Fearfulness, were used (4 items each), and followed the same likert-type scale as described above for the child questionnaire. Sample items include: for Distress, “I frequently get distressed”; for Anger, “I am known as hot-blooded and quick-tempered”; and for Fearfulness, “I am easily frightened”. Previous research has used a total score for Emotionality, thus collapsing across Distress, Anger and Fearfulness, and has found good internal reliability; for example, Laurent and Powers (2007) report a Cronbach’s alpha of .83 for the Emotionality total score. In the present study, the Cronbach’s alpha value for the Emotionality total score was 0.81 and 0.82 for Time 1 and Time 2 respectively.
Child internalizing behavior
Mothers completed the Parent Report Form of the Child Behaviour Checklist (CBCL; Achenbach 1991) at Time 1 and Time 2, which is a questionnaire that is designed to assess a range of behavioural problems in children. Mothers were asked to report whether behavioural descriptions were representative of their child, ranging from 0 (not at all true) to 2 (very true). In the present study, only the Internalizing scale was used, which is composed of 32 items that reflect the Withdrawn, Somatic Complaints, and Anxious/Depressed subscales. This scale was used due to its previous associations with negative emotionality (e.g., Crawford et al. 2011; Shaw et al. 1997). Good short-term test–retest reliability (0.93 for total problems) has been reported for this measure (Achenbach 1991), and previous research has shown high internal consistency reliability (0.90; e.g., Gartstein and Fagot 2003). Note that at Time 1, two different versions of the CBCL were used based on the age group of the child, i.e., under or over 4 years old. The internal consistency for the present sample for the various time points was 0.85 (under 4 years old) and 0.70 (over 4 years old) for Time 1, and 0.84 for Time 2.
Maternal contingencies to child emotions
Mothers completed the Emotions as a Child questionnaire (Magai 1996) at Time 2. The questionnaire, which can be modified to be completed as a self-report by the parent or as child-reported, has been used to assess the techniques used by parents in reaction to their child’s negative emotions (Hastings et al. 2014; Klimes-Dougan et al. 2007; O’Neal and Magai 2005). In the present study, the questionnaire reflected the mother’s self-reported tendency to react to their child’s negative emotions (specifically: sadness, anger and fear) with certain contingencies. It asks mothers to reflect on their reactions to their child’s negative emotional expressions in the past 2 months. Five contingencies to these emotions were identified: (1) Punish (i.e., discouragement of the negative emotional expression via sanctions; e.g., “Gave him/her a disgusted look”); (2) Magnify (i.e., experience and express the negative emotion back to the child; e.g., “Got tearful and cried”); (3) Ignore (i.e., not pay attention to the child’s displays either intentionally or unintentionally; e.g., “Usually didn’t notice”); (4) Override (i.e., minimize their emotional experience; e.g., “Told him/her not to worry”); or (5) Support (i.e., help the child with the problem or with the experience of the emotion itself; e.g., “Helped my child deal with the issue”). Mothers were asked how likely on a likert-type scale of 1 (not at all typical) to 5 (very typical) they were to respond to each of the respective emotions (i.e., sadness, anger, fear) with a series of reactions, with three items per reaction per emotion, totaling 45 items. Internal reliability coefficients of the questionnaire revealed adequate reliability for the present study, with Punish at 0.64, Magnify at 0.77, Ignore at 0.74, Override at 0.79, and Support at 0.88. These reliability coefficients are similar to those found in other studies (e.g. Buckholdt et al. 2009).
Plan of Analysis
Missing data
Due to the participant attrition noted above between the two time points as well as missing data within the variable set, multiple imputation for the 175 families in the current study was conducted. Multiple imputation is a statistical technique commonly used in longitudinal data sets to replace missing data with value estimates, and it is preferred to other missing data techniques such as listwise deletion which drastically reduces sample size and may yield biased parameter estimates (Graham 2009). The results from Little’s MCAR test suggest that data were missing completely at random (χ2(184) = 165.93, p = 0.83). As a result, multiple imputation using Mplus (Muthén and Muthén 2010) was conducted with variables missing less than 35% of their data. Because of the rate of missingness, 100 imputations (i.e., m = 100) were aggregated into one file and the resulting summary file was used in all ensuing analyses (Graham et al. 2007).
Path analyses
Path analyses were conducted using Mplus v. 7.3 (Muthén and Muthén 2017). Two path analyses were conducted which tested the extent to which maternal contingences mediated the effect of maternal negative emotionality and adolescent outcomes.
In the first model, maternal punishment contingency at Time 2 was tested as a mediator of the effect from maternal negative emotionality at Time 2 to adolescent negative emotionality at Time 2. In the second model, adolescent negative emotionality, maternal support contingency, and maternal magnify contingency at Time 2 each individually were tested as mediators of the effect from maternal negative emotionality at Time 2 to adolescent internalizing problems at Time 2. In order to rule out the possibility that the mediation sequence started earlier in the child’s development, maternal negative emotionality at Time 1 was controlled for in both models. Prior levels of the outcomes, and child sex, were also controlled for in both models. Tests of indirect effects were based on bootstrapping procedures (2000 samples) recommended by Preacher and Hayes (2008), using the model indirect command in Mplus. Sensitivity analyses determined the extent to which indirect effects remained statistically significant after accounting for unobserved sources of covariation between mediators and outcomes (Imai et al. 2010). An iterative process was followed where the strength of the unobserved covariance was gradually increased until indirect effects were no longer significant. Sensitivity analyses were conducted via the “mediation” package in R (Tingley et al. 2014), which relies on quasi-bayesian estimation of indirect effects.
Supplemental models included adolescent age (at Time 1 and at Time 2), maternal education, mothers’ age at birth of their first child, and family prestige as additional control variables. Each additional control was investigated in isolation (e.g., one supplemental model included adolescent sex and maternal education as controls, another supplemental model included adolescent sex and family prestige as controls). As an additional supplement to the second model, maternal punishment contingency at Time 2 was added as fourth mediator to determine if it predicted adolescent internalizing problems. Additional supplemental models were explored to determine if results replicated when using full information maximization likelihood (FIML) to handle missing data instead of multiple imputation. Differences in results are noted in the results section.
Results
Descriptive statistics for the predictors can be found in Table 1 and correlations between the predictors can be found in Table 2.
In the first set of path analyses, maternal punishment contingency at Time 2 was entered as a mediator of the concurrent association from maternal negative emotionality at Time 2 to adolescent negative emotionality at Time 2. The model was fully saturated; thus, model fit was perfect. The model accounted for 22% of variance in adolescent negative emotionality at Time 2. The results are presented in Fig. 1.

Standardized regression coefficients for the relationship between maternal negative emotionality (NE) and adolescent negative emotionality (NE) as mediated by maternal emotion socialization contingency punish. Note.N = 175. Standardized results are reported. Child sex was controlled for; only significant associations involving child sex are displayed. The standardized total effect between maternal NE and adolescent NE is in parentheses. *p < 0.05, **p < 0.01 (two-tailed)
The total effect from maternal negative emotionality at Time 2 to adolescent negative emotionality at Time 2 was positive and statistically significant (β = 0.25, p = 0.001). The addition of maternal punishment contingency as a mediator revealed a pattern of associations consistent with partial mediation. Maternal negative emotionality at Time 2 was positively associated with maternal punishment contingency at Time 2 (β = 0.34, p < 0.001), which in turn was positively associated with adolescent negative emotionality at Time 2 (β = 0.26, p < 0.001). The indirect effect was statistically significant (β = 0.09, p = 0.004); approximately 35% of the effect from maternal negative emotionality to adolescent negative emotionality was mediated via maternal punishment contingency. A sensitivity analyses revealed that this indirect effect remained significant until the unobserved correlation between maternal punishment contingency at Time 2 and adolescent negative emotionality at Time 2 exceeded 0.08. The direct effect from maternal negative emotionality at Time 2 to adolescent negative emotionality at Time 2 remained positive and significant (β = 0.16, p = 0.040).
Although maternal negative emotionality at Time 1 was positively related to maternal negative emotionality at Time 2 (β = 0.49, p < 0.001), it was not significantly related to any other study variables at Time 2. Adolescent negative emotionality at Time 1 was positively related to adolescent negative emotionality at Time 2 (β = 0.28, p < 0.001), but it was not significantly related to any other study variables at Time 2. Adolescent sex was not significantly related to any study variables.
Supplemental models revealed that the direct effect from maternal negative emotionality at Time 2 to adolescent negative emotionality at Time 2 became borderline significant in two instances; (a) when family prestige was entered as a control variable (β = 0.14, p = 0.086), and (b) when using unimputed data with FIML (β = 0.19, p = 0.061). All other supplemental models replicated the same pattern of statistically significant associations.
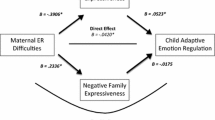
In the second set of path analyses, maternal support contingency, and maternal magnify contingency at Time 2 were together entered as mediators of the concurrent association from maternal negative emotionality at Time 2 to adolescent internalizing problems at Time 2. The model was fully saturated; thus, model fit was perfect. The model accounted for 47% of variance in adolescent internalizing problems at Time 2. The results are presented in Fig. 2.

Standardized regression coefficients for the relationship between the maternal emotion socialization contingencies of magnify and support and adolescent internalizing symptoms, controlling for maternal negative emotionality (NE), child negative emotionality (NE), and previous child internalizing symptoms (depicted in boxes with dashed lines). Note.N = 175. Standardized results are reported. Child sex was controlled for; only significant associations involving child sex are displayed. The standardized total effect between maternal NE and child internalizing is in parentheses. *p < 0.05, **p < 0.01 (two-tailed)
The total effect from maternal negative emotionality at Time 2 to adolescent internalizing problems at Time 2 was positive and statistically significant (β = 0.21, p = 0.007). Of the three mediators tested, only the addition of adolescent negative emotionality revealed an indirect effect which was consistent with full mediation. Maternal negative emotionality at Time 2 was positively associated with adolescent negative emotionality at Time 2 (β = 0.21, p = 0.008), which in turn was positively associated with adolescent internalizing problems at Time 2 (β = 0.49, p < 0.001). The indirect effect was statistically significant (β = 0.10, p = 0.011). A sensitivity analyses revealed that this indirect effect remained significant until the unobserved correlation between adolescent negative emotionality at Time 2 and adolescent internalizing problems at Time 2 exceeded 0.13. In total, approximately 63% of the total effect from maternal negative emotionality at Time 2 to adolescent internalizing problems at Time 2 was mediated, almost entirely by adolescent negative emotionality at Time 2. The model also revealed the presence of direct associations involving maternal magnify and support contingencies at Time 2. Maternal negative emotionality was positively associated with maternal magnify contingency (β = 0.26, p = 0.001), and maternal support contingency was negatively associated with child internalizing problems (β = -0.14, p = 0.012).
Although maternal negative emotionality at Time 1 was positively related to maternal negative emotionality at Time 2 (β = 0.45, p < 0.001), it was not significantly associated with any other study variables at Time 2. Child internalizing problems at Time 1 were positively related to adolescent internalizing problems at Time 2 (β = 0.19, p = 0.001), but were not significantly associated with any other study variables at Time 2. Adolescent sex was positively related to maternal support contingency at Time 2, (β = 0.18, p = 0.017); mothers of females reported higher levels of maternal support contingency at Time 2.
The same pattern of statistically significant associations was maintained when controlling for child age, maternal education, mothers’ age of birth of their first child, and family prestige, and when using FIML to handle missing data. The addition of maternal punishment contingency at Time 2 as a mediator did not influence the presence of significant associations in the model; however, maternal punishment contingency was no longer significantly associated with adolescent internalizing problems, as was previously indicated in Table 2.
Discussion
The developmental psychopathology framework encourages researchers to examine both the personal characteristics that may make a child more vulnerable to psychopathology, such as emotionality, as well as the impact that their parent’s characteristics and rearing practices may have, such as parental emotionality and emotion socialization (Cicchetti and Curtis 2007). In the present study, the link between maternal and adolescent emotionality was examined, and how this association may be mediated by maternal emotion socialization, specifically contingencies. A range of maternal contingencies (i.e., responses to child’s negative emotions) was explored as potential mediators of the association between maternal and adolescent negative emotionality. Further, the roles of emotionality and emotion socialization were explored in relation to maladaptive psychological outcomes, specifically internalizing symptoms in adolescence. Findings are first discussed concerning negative emotionality’s stability and its relation to internalizing symptoms, followed by the mediating role of maternal contingencies.
With regard to the stability of negative emotionality, the results suggest that negative emotionality, a component of temperament, is fairly consistent from preschool to adolescence. The results from the path analysis revealed that previous ratings of child negative emotionality in preschool were associated with adolescent negative emotionality, spanning a total of approximately 10 years between the first and second time point. Although previous research has suggested that negative emotionality is consistent across early developmental periods such as preschool to middle childhood (Bould et al. 2013) or toddlerhood to middle childhood (Neppl et al. 2010), this is one of few recent longitudinal studies to demonstrate the stability of negative emotionality across early to late developmental periods, and the results showed similar effect sizes to those studies with 1–2 years delay between questionnaires (e.g., Sallquist et al. 2009). Further, the results revealed that there is a positive association between adolescent negative emotionality and adolescent internalizing symptoms, controlling for previous ratings of internalizing symptoms at Time 1. This finding further corroborates previous research that suggests that high negative emotionality may be a predisposing or risk factor for internalizing problems (for a review, see Klein et al. 2012).
In order to explore the potential familial contributions to the adolescent’s emotional well-being, the negative emotionality of the mother as well as her emotion socialization practices were explored in relation to her child’s negative emotionality and internalizing problems. The results revealed that maternal negative emotionality was positively associated with adolescent negative emotionality, even after controlling for Time 1 maternal negative emotionality and Time 1 Time 2 child negative emotionality. Overall, path analyses revealed that mothers with high negative emotionality tended to have adolescent children with high negative emotionality. Given previous research associating parent and child negative emotionality (e.g., Crawford et al. 2011; Davenport et al. 2011) and other emotion-related competencies such as emotion regulation (e.g., Buckholdt et al. 2014), the results from this study serve to provide further evidence of the similarity between maternal and child negative emotionality. Although there have been some studies to show this link between parent and child, it is rare that this research is conducted with adolescents. Apart from one study that found a weak correlation between mother’s negative affect and that of her adolescent child (Davenport et al. 2011), the present study is one of the first to examine and demonstrate a significant association between mother and adolescent negative emotionality.
The current research was also designed to expand and contribute to the literature by exploring a potential mechanism by which mothers may reinforce high negative emotionality in their adolescent children. Specifically, this was explored via contingencies, a form of emotion socialization that involves the parental response to emotions. A total of five contingencies were examined as potential mediators. In general, non-supportive responses have been positively associated with more difficulty coping with anger and sadness (Sanders et al. 2015), and high negative affect in children (Eisenberg and Fabes 1994), and more depression symptoms in adolescents (Shortt et al. 2016). The only contingency that was found to be associated with both maternal and adolescent negative emotionality was the punish contingency. Specifically, the punish contingency acted as a mediator between maternal and adolescent negative emotionality, such that mothers who experienced higher levels of negative emotionality were more likely to use the punish contingency, and adolescents who received the punish contingency more often tended to have higher levels of negative emotionality. The punish contingency specifically includes behaviours such as giving a disgusted look, being condescending or mocking, and giving a tangible behavioural punishment, in response to their adolescent expressing a negative emotion. By responding in this non-supportive way, the expression of negative emotions is treated as something to be ignored or denied and as something harmful or undesired as opposed to an opportunity to learn and grow from (Schwartz et al. 2012). This type of responding provides children with fewer opportunities to learn how to deal with these emotions in an appropriate way (Buck 1984). Instead, non-supportive or harsh reactions may be laying the foundation for maladaptive reactions such as thought suppression or other avoidant coping (Krause et al. 2003; Wenzlaff and Eisenberg 1998) which in turn increases the likelihood of distress (e.g., Brenner and Salovey 1997). Moreover, the adolescent may begin to associate sanctions and negative consequences with their negative emotions, further contributing to their emotional distress in already stressful situations. Conversely, there is also the possibility that high levels of emotional distress from the adolescent tends to elicit negative emotions from their parent (e.g., Kim et al. 2001) which in turn may make non-supportive socialization tactics, such as punishment, more likely. However, observational research with adolescents suggests that the mother characteristics, such as her awareness of her own emotions, may be a much better predictor than child characteristics, such as child negative emotionality, in the circumvention of non-supportive socialization strategies (Yap et al. 2008).
Results from the mediation analyses suggest that mothers with higher negative emotionality were more likely to use the punish contingency than mothers with lower levels of negative emotionality. This is well-supported by previous research, which suggests that mothers who tend to use parenting practices, including emotion socialization, which is harsh or punitive have emotional capabilities that are somehow compromised, such as being high in negative emotionality (Leung and Slep 2006), having a history of depression (Silk et al. 2011) or anxiety (Arellano et al. 2018), or having poor emotion regulation (Buckholdt et al. 2014). In further mediation analyses, it was revealed that the punish contingency was no longer associated directly with internalizing problems when adolescent negative emotionality was taken into account. These results suggest that punishing negative emotions leads to higher levels of emotional distress in adolescents, which can then lead to higher levels of internalizing symptoms. The findings therefore support the potential precursor or predisposing role of negative emotionality in internalizing problems (Klein et al. 2012). It is suggested that having higher negative emotionality places a greater strain on a child’s ability to regulate their emotions in day-to-day life, and therefore these high negative emotionality children may be more likely to have failures in their regulatory abilities, potentially manifesting as internalizing problems (Yap et al. 2007).
As reported in the second model, the magnify contingency was also associated with higher maternal negative emotionality. This contingency is characterized by the mother matching her child’s distress with her own similar emotional reaction. Therefore, it should follow that mothers with higher negative emotionality in general may be less able to contain their own emotional distress in response to their children’s. Interestingly, magnify could not be included as a potential mediator in the first model because its association with negative emotionality became statistically nonsignificant when the punish contingency was also in the model. This may be because responding to anger with magnify is similar to the act of the punish contingency according to factor analyses, in that matching an adolescent’s angry expression with anger or aggression (e.g., yelling) may likely be perceived as a form of punishment (Klimes-Dougan et al. 2007). Indeed, the magnification of anger specifically has been associated with detrimental outcomes such as externalizing behaviour, whereas the magnification of sadness or fear does not share that association (O’Neal and Magai 2005). However, the implications of magnifying sadness or fear remain unclear. Although mirroring sadness or fear could be problematic as the parent’s distress may interfere with their ability to properly coach their child through the negative emotion (Moed et al. 2015), it could also be potentially perceived as validating by the adolescent in that their emotional concerns are being heard and understood. Although only marginally significant, the magnify contingency was positively associated with internalizing symptoms. Considering that this association remained statistically significant even when controlling for the punish contingency, whereas the punish contingency was not statistically significant, it is possible that the variance associated with internalizing symptoms relates to the reactions to sadness and fear, and not anger as described above. Potentially, children of mothers who respond to their sadness or fear with their own similar reactions are creating the space for the child to also show their emotions regularly. However, because magnification does not involve the use of coaching techniques, it is possible that these children may be more likely to feel comfortable expressing their sadness and fear to their mothers, but have few resources to cope with these emotions on a daily basis.
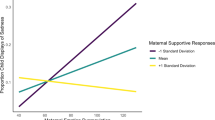
With respect to helpful emotion socialization techniques, the support contingency was directly negatively associated with internalizing symptoms. Specifically, more support, in the form of comforting or problem solving with the child, was associated with fewer internalizing symptoms. Interestingly, this contingency was not associated with adolescent negative emotionality. This may reflect the fact that providing support and comfort may help to improve day-to-day coping with such things as worries, somatization, and self-defeating beliefs, but may not help reduce the intensity and frequency with which adolescents react to stressors or crises with strong negative emotions. Improving an adolescent’s emotional reactivity, as in the spur of the moment reactions, may pose as a serious challenge to parents, even if they are responding supportively. Supportive reactions do not necessarily entail strategies to increase emotional distress tolerance or soothe the emotion instantly. Instead, they provide the adolescent with problem-solving strategies and a safe space to express their emotions and thoughts. This may help the child to process their emotions in a gradual manner that overall leads to less worrying, rumination, and somatization, even if their gut reactions remain intense (e.g., Bronstein et al. 1993). In a sense, they may feel more comfortable to feel and display negative emotions intensely, knowing that their mother has shown them consistently that negative emotions fade away with comforting and soothing and that they will receive the scaffolding necessary to solve their problems.
By understanding one of the potential mechanisms at play in the transfer of negative emotionality, it is possible to intervene to protect parents and adolescents alike. For example, Tuning in to Teens (TINT; Kehoe et al. 2014) is an emotion socialization training program for parents which has proven to be effective in a community sample. In addition to emotion coaching skills, the program teaches parents how to deal with their own emotions in the moment, such as through meditation and mindfulness-based skills. Considering that the results from the current study showed that parental emotional distress is associated with the use of maladaptive techniques, such as the punish contingency, it may be particularly helpful to teach parents skills that allow them to regulate their emotions in the midst of their adolescent’s emotional crisis, in order to ultimately respond in a way that will be helpful and supportive. Future programs may also emphasize the harmfulness of punishing negative emotions, potentially prioritizing the dramatic reduction of this particular technique above all other non-supportive techniques.
Although the current research contributed to the literature in a number of ways, there are some limitations that would be best attended to in the context of future studies. The measures for the study were exclusively self-report for the maternal measures and mother-report for the adolescent measures, raising the issue of the single-rater effect. Although maternal reports for emotionality and internalizing symptoms have been shown to be valid and reliable (e.g., Rothbart and Bates 2006; Sallquist et al. 2009), a combination of reporters, such as a teacher, father/partner, or the adolescent him/herself could have added to the understanding of the adolescent’s behavioural and emotional experience (e.g., Keiley et al. 2003). In addition, the use of maternal self-report on the contingencies may have led to some biased reporting, as mothers may have intuited which responses would be seen as maladaptive. Future studies could use observational data and coding systems as well as the corroboration from the child in conjunction with the self-report questionnaire data in order to have a more objective and broader view of the mother’s responses. It also should be noted that, because previous levels of the outcomes were controlled for, the results could potentially be interpreted as the effects associated with change in those outcomes. In addition, the results concerning the link between emotional well-being and maternal socialization were limited to concurrent associations, as the maternal socialization variable was not available at the earlier time point. Future studies may use longitudinal methods to control for past and present maternal socialization techniques to establish the power of the socialization strategy at that moment and further argue for its role in transmission via prospective relations (Bridgett et al. 2015). Longitudinal designs in studies could help to answer questions about how mothers may modify their techniques as their children age and whether specific techniques are particularly harmful or beneficial for a child’s psychosocial well-being depending on their age.
Conclusion
The results have helped deepen the understanding of maternal emotion socialization practices and their implications for adolescent emotional health. Within the framework of the developmental psychopathology model, underscoring the importance of exploring both child and parent characteristics as well as the rearing environment was attempted to obtain a more complete understanding of a child’s emotional well-being (Calkins et al. 2013; Cichetti and Curtis 2007). The findings concerning antecedents of the punish contingency, specifically high maternal negative emotionality, contribute to knowledge of the contextual factors that place certain parents at-risk for maladaptive practices. Kovan et al. (2009) have emphasized the need to further explore how and why parents may use certain emotion socialization practices over others, as this will help intervention researchers identify at-risk groups who may need extra assistance in reducing and eliminating these behaviours. In addition, adolescent outcomes of emotion socialization techniques were examined, which is rare in the literature. The findings from the present study demonstrate the importance of socialization’s role on temperamental constructs such as negative emotionality in addition to psychopathological symptoms measures such as internalizing behaviours. The results provide evidence that an adolescent’s distress can potentially be worsened with non-supportive emotion socialization techniques, such as punishing negative emotions, whereas supportive reactions can be potentially helpful in reducing internalizing symptoms. Taken together, the study highlighted the importance of studying parental emotion socialization practices beyond childhood and into adolescence in order to best understand how to support adolescents’ emotional well-being. Furthermore, this study identifies specific directions for further investigation in the development of interventions for families who are emotionally at-risk.
References
Achenbach, T. M. (1991). Manual for the child behavior checklist/ 4–18 and 1991 profile. Burlington, VT: University of Vermont.
Anthony, J. L., Lonigan, C. J., Hooe, E. S., & Phillips, B. M. (2002). An affect-based, hierarchical model of temperament and its relations with internalizing symptomatology. Journal of Clinical Child and Adolescent Psychology, 31, 480–490. https://doi.org/10.1207/S15374424JCCP3104_7.
Arellano, B., Gramszlo, C., & Woodruff-Borden, J. (2018). Parental reactions to children’s negative affect: the moderating role of parental GAD. Journal of Anxiety Disorders, 53, 22–29. https://doi.org/10.1016/j.janxdis.2017.10.006.
Bould, H., Joinson, C., Sterne, J., & Araya, R. (2013). The emotionality activity sociability temperament survey: factor analysis and temporal stability in a longitudinal cohort. Personality and Individual Differences, 54(5), 628–633. https://doi.org/10.1016/j.paid.2012.11.010.
Brand, A. E., & Klimes-Dougan, B. (2010). Emotion socialization in adolescence: the roles of mothers and fathers. New Directions for Child and Adolescent Development, 128, 85–100. https://doi.org/10.1002/cd.270.
Brenner, E. M., & Salovey, P. (1997). Emotion regulation during childhood: developmental, interpersonal, and individual considerations. In P. Salovey & D. J. Sluyter (Eds.), Emotional development and emotional intelligence: Educational implications (pp. 168–192). New York, NY: Basic Books.
Bridgett, D. J., Burt, N. M., Edwards, E. S., & Deater-Deckard, K. (2015). Intergenerational transmission of self-regulation: A multidisciplinary review and integrative conceptual framework. Psychological Bulletin, 141(3), 602–654. https://doi.org/10.1037/a0038662.
Bronstein, P., Fitzgerald, M., Briones, M., Pieniadz, J., & D’Ari, A. (1993). Family emotional expressiveness as a predictor of early adolescent social and psychological adjustment. The Journal of Early Adolescence, 13(4), 448–471. https://doi.org/10.1177/0272431693013004006.
Buck, R. (1984). The communication of emotion. New York, NY: Guilford Press.
Buckholdt, K. E., Parra, G. R., & Jobe-Shields, L. (2009). Emotion regulation as a mediator of the relation between emotion socialization and deliberate self-harm. American Journal of Orthopsychiatry, 79, 482–490. https://doi.org/10.1037/a0016735.
Buckholdt, K. E., Parra, G. R., & Jobe-Shields, L. (2014). Intergenerational transmission of emotion dysregulation through parental invalidation of emotions: Implications for adolescent internalizing and externalizing behaviors. Journal of Child and family Studies, 23(2), 324–332. https://doi.org/10.1007/s10826-013-9768-4.
Buss, A. H., & Plomin, R. (1984). Temperament: early developing personality traits. Hillsdale, NJ: Lawrence Erlbaum.
Buss, A. H., & Plomin, R. (1986). The EAS approach to temperament. In R. Plomin & J. Dunn (Eds.), The study of temperament: Changes, continuities, and challenges (pp. 67–79). Hillsdale, NJ: Lawrence Erlbaum Associates, Inc.
Calkins, S. D., Propper, C., & Mills-Koonce, W. R. (2013). A biopsychosocial perspective on parenting and developmental psychopathology. Development and Psychopathology, 25, 1399–1414. https://doi.org/10.1017/S0954579413000680.
Cicchetti, D., & Curtis, W. J. (2007). Multilevel perspectives on pathways to resilient functioning. Development and Psychopathology, 19, 627–629. https://doi.org/10.1017/S0954579407000314.
Crawford, N. A., Schrock, M., & Woodruff-Borden, J. (2011). Child internalizing symptoms: contributions of child temperament, maternal negative affect, and family functioning. Child Psychiatry and Human Development, 42, 53–64. https://doi.org/10.1007/s10578-010-0202-5.
Davenport, E., Yap, M. B., Simmons, J. G., Sheeber, L. B., & Allen, N. B. (2011). Maternal and adolescent temperament as predictors of maternal affective behavior during mother–adolescent interactions. Journal of Adolescence, 34(5), 829–839. https://doi.org/10.1016/j.adolescence.2011.02.003.
Dougherty, L. R., Bufferd, S. J., Carlson, G. A., Dyson, M., Olino, T. M., Durbin, C. E., & Klein, D. N. (2011). Preschoolers’ observed temperament and psychiatric disorders assessed with a parent diagnostic interview. Journal of Clinical Child & Adolescent Psychology, 40(2), 295–306. https://doi.org/10.1080/15374416.2011.546046.
Dunsmore, J. C., Booker, J. A., Ollendick, T. H., & Greene, R. W. (2016). Emotion socialization in the context of risk and psychopathology: Maternal emotion coaching predicts better treatment outcomes for emotionally labile children with oppositional defiant disorder. Social Development, 25(1), 8–26. https://doi.org/10.1111/sode.12109.
Eisenberg, N., & Fabes, R. A. (1994). Mothers’ reactions to children’s negative emotions: relations to children’s temperament and anger behavior. Merrill Palmer Quarterly, 40, 138–156.
Eisenberg, N., Fabes, R. A., Shepard, S. A., Guthrie, I. K., Murphy, B. C., & Reiser, M. (1999). Parental reactions to children’s negative emotions: Longitudinal relations to quality of children’s social functioning. Child Development, 70, 513–534.https://0-doi-org.mercury.concordia.ca/10.1111/1467-8624.00037.
Enns, L. N., Barrieau, L. E., Stack, D. M., Serbin, L. A., Ledingham, J. E., & Schwartzman, A. E. (2015). Verbal and nonverbal communication in at-risk mother-child dyads: implications for relationship quality and developing positive social behaviors in middle-childhood. European Journal of Developmental Psychology, 13(1), 1–19. https://doi.org/10.1080/17405629.2015.1049153.
Fabes, R. A., Leonard, S. A., Kupanoff, K., & Martin, C. L. (2001). Parental coping with children’s negative emotions: relations with children’s emotional and social responding. Child Development, 72(3), 907–920. https://doi.org/10.1111/1467-8624.00323.
Garber, J., Keiley, M. K., & Martin, N. C. (2002). Developmental trajectories of adolescents’ depressive symptoms: predictors of change. Journal of Consulting and Clinical Psychology, 70(1), 79–95. https://doi.org/10.1037/0022-006X.70.1.79.
Gartstein, M. A., & Fagot, B. I. (2003). Parental depression, parenting and family adjustment, and child effortful control: explaining externalizing behaviors for preschool children. Journal of Applied Developmental Psychology, 24(2), 143–177. https://doi.org/10.1016/S0193-3973(03)00043-1.
Graham, J. W. (2009). Missing data analysis: making it work in the real world. Annual Review of Psychology, 60, 549–576. https://doi.org/10.1146/annurev.psych.58.110405.085530.
Graham, J. W., Olchowski, A. E., & Gilreath, T. D. (2007). How many imputations are really needed? Some practical clarifications of Multiple Imputation Theory. Prevention Science, 8, 206–213. https://doi.org/10.1007/s11121-007-0070-9.
Hagan, M. J., Luecken, L. J., Modecki, K. L., Sandler, I. N., & Wolchik, S. A. (2016). Childhood negative emotionality predicts biobehavioral dysregulation fifteen years later. Emotion ( Washington, D C ), 16(6), 877–885. https://doi.org/10.1037/emo0000161.
Han, Z. R., Qian, J., Gao, M., & Dong, J. (2015). Emotion socialization mechanisms linking Chinese fathers’, mothers’, and children’s emotion regulation: a moderated mediation model. Journal of Child and family Studies, 24(12), 3570–3579. https://doi.org/10.1007/s10826-015-0158-y.
Hastings, P. D., Klimes-Dougan, B., Kendziora, K. T., Brand, A., & Zahn-Waxler, C. (2014). Regulating sadness and fear from outside and within: mothers’ emotion socialization and adolescents’ parasympathetic regulation predict the development of internalizing difficulties. Development and Psychopathology, 26(4 Pt 2), 1369–1384. https://doi.org/10.1017/S0954579414001084.
Hughes, E. K., & Gullone, E. (2010). Parent emotion socialisation practices and their associations with personality and emotion regulation. Personality and Individual Differences, 49(7), 694–699. https://doi.org/10.1016/j.paid.2010.05.042.
Hooper, E. G., Wu, Q., Ku, S., Gerhardt, M., & Feng, X. (2018). Maternal emotion socialization and child outcomes among African Americans and European Americans. Journal of Child &Family Studies, 27(6), 1870–1880.
Hurrell, K. E., Hudson, J. L., & Schniering, C. A. (2015). Parental reactions to children’s negative emotions: relationships with emotion regulation in children with an anxiety disorder. Journal of Anxiety Disorders, 29, 72–82. https://doi.org/10.1016/j.janxdis.2014.10.008.
Imai, K., Keele, L., & Tingley, D. (2010). A general approach to causal mediation analysis. Psychological Methods, 15(4), 309–334.
Jones, S., Eisenberg, N., Fabes, R. A., & MacKinnon, D. P. (2002). Parents’ reactions to elementary school children’s negative emotions: relations to social and emotional functioning at school. Merrill-Palmer Quarterly, 48(2), 133–159. https://doi.org/10.1353/mpq.2002.0007.
Karevold, E., Røysamb, E., Ystrom, E., & Mathiesen, K. S. (2009). Predictors and pathways from infancy to symptoms of anxiety and depression in early adolescence. Developmental Psychology, 45(4), 1051–1060. https://doi.org/10.1037/a0016123.
Kehoe, C. E., Havighurst, S. S., & Harley, A. E. (2014). Tuning in to teens: improving parent emotion socialization to reduce youth internalizing difficulties. Social Development, 23(2), 413–431. https://doi.org/10.1111/sode.12060.
Keiley, M., Lofthouse, N., Bates, J., Dodge, K., & Pettit, G. (2003). Differential risks of covarying and pure components in mother and teacher reports of externalizing and internalizing behavior across ages 5 to 14. Journal of Abnormal Child Psychology, 31, 267–284.
Kim, K. J., Conger, R. D., Lorenz, F. O., & Elder, Jr., G. H. (2001). Parent–adolescent reciprocity in negative affect and its relation to early adult social development. Developmental Psychology, 37(6), 775–790. https://doi.org/10.1037//0012-1649.37.6.775.
Klein, D. N., Dyson, M. W., Kujawa, A. J., & Kotov, R. (2012). Temperament and internalizing disorders. In M. Zentner & R. L. Shiner (Eds.), Handbook of temperament (pp. 541–561). New York, NY: The Guilford Press.
Klimes-Dougan, B., Brand, A. E., Zahn-Waxler, C., Usher, B., Hastings, P. D., Kendziora, K., & Garside, R. B. (2007). Parental emotion socialization in adolescence: Differences in sex, age and problem status. Social Development, 16(2), 326–342. https://doi.org/10.1111/j.1467-9507.2007.00387.x.
Kopala-Sibley, D. C., Danzig, A. P., Kotov, R., Bromet, E. J., Carlson, G. A., & Olino, T. M., et al. (2016). Negative emotionality and its facets moderate the effects of exposure to hurricane sandy on children’s postdisaster depression and anxiety symptoms. Journal of Abnormal Psychology, 125(4), 471–481. https://doi.org/10.1037/abn0000152.
Kovacs, M., & Lopez-Duran, N. (2010). Prodromal symptoms and atypical affectivity as predictors of major depression in juveniles: implications for prevention. Journal of Child Psychology and Psychiatry, 51, 472–496. https://doi.org/10.1111/j.1469-7610.2010.02230.x.
Kovan, N. M., Chung, A. L., & Sroufe, L. A. (2009). The intergenerational continuity of observed early parenting: A prospective, longitudinal study. Developmental Psychology, 45(5), 1205–1213. https://doi.org/10.1037/a0016542.
Krause, E. D., Mendelson, T., & Lynch, T. R. (2003). Childhood emotional invalidation and adult psychological distress: the mediating role of emotional inhibition. Child Abuse & Neglect, 27(2), 199–213. 10.1016/S0145-2134(02)00536-7.
Larson, R. W., Moneta, G., Richards, M. H., & Wilson, S. (2002). Continuity, stability, and change in daily emotional experience across adolescence. Child Development, 73(4), 1151–1165. https://doi.org/10.1111/1467-8624.00464.
Laurent, H., & Powers, S. (2007). Emotion regulation in emerging adult couples: Temperament, attachment, and HPA response to conflict. Biological Psychology, 76, 61–71. https://doi.org/10.1016/j.biopsycho.2007.06.002.
Lengua, L. J., & Kovacs, E. A. (2005). Bidirectional associations between temperament and parenting and the prediction of adjustment problems in middle childhood. Journal of Applied Developmental Psychology, 26(1), 21–38. https://doi.org/10.1016/j.appdev.2004.10.001.
Leung, D. W., & Slep, A. M. S. (2006). Predicting inept discipline: the role of parental depressive symptoms, anger, and attributions. Journal of Consulting and Clinical Psychology, 74(3), 524–534. https://doi.org/10.1037/0022-006X.74.3.524.
Magai, C. (1996). Emotions as a Child: Adult Version. Brooklyn, NY: Long Island University.
Martin, J. P., Stack, D. M., Serbin, L. A., Ledingham, J., & Schwartzman, A. E. (2012). Social problem solving in high-risk mother–child dyads: an intergenerational study. Social Development, 21(1), 47–67. https://doi.org/10.1111/j.1467-9507.2011.00600.x.
Metsäpelto, R. L., & Pulkkinen, L. (2003). Personality traits and parenting: neuroticism, extraversion, and openness to experience as discriminative factors. European Journal of Personality, 17, 59–78. https://doi.org/10.1002/per.468.
Moed, A., Dix, T., Anderson, E. R., & Greene, S. M. (2017). Expressing negative emotions to children: mothers’ aversion sensitivity and children’s adjustment. Journal of Family Psychology, 31(2), 224–233. https://doi.org/10.1037/fam0000239.
Moed, A., Gershoff, E. T., Eisenberg, N., Hofer, C., Losoya, S., Spinrad, T. L., & Liew, J. (2015). Parent–adolescent conflict as sequences of reciprocal negative emotion: links with conflict resolution and adolescents’ behavior problems. Journal of Youth and Adolescence, 44(8), 1607–1622. https://doi.org/10.1007/s10964-014-0209-5.
Muthén, B. O., & Muthén, L. K. (2010). Mplus (Version 6.00) [Computer software]. Los Angeles: Muthén & Muthén.
Muthén, B. O., & Muthén, L. K. (2017). Mplus (Version 7.3) [Computer software]. Los Angeles, CA: Muthén & Muthén.
Neppl, T. K., Donnellan, M. B., Scaramella, L. V., Widaman, K. F., Spilman, S. K., Ontai, L. L., & Conger, R. D. (2010). Differential stability of temperament and personality from toddlerhood to middle childhood. Journal of Research in Personality, 44(3), 386–396. https://doi.org/10.1016/j.jrp.2010.04.004.
O’Neal, C. R., & Magai, C. (2005). Do parents respond in different ways when children feel different emotions? The emotional context of parenting. Development and Psychopathology, 17, 467–487. https://doi.org/10.1017/S0954579405050224.
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40, 879–891.
Premo, J. E., & Kiel, E. J. (2016). Maternal depressive symptoms, toddler emotion regulation, and subsequent emotion socialization. Journal of Family Psychology, 30(2), 276–285. https://doi.org/10.1037/fam0000165.
Propper, C., & Moore, G. A. (2006). The influence of parenting on infant emotionality: a multi-level psychobiological perspective. Developmental Review, 26(4), 427–460. https://doi.org/10.1016/j.dr.2006.06.003.
Rothbart, M. K. (2011). Becoming who we are: temperament and personality in development. New York, NY: Guilford Press.
Rothbart, M. K., & Bates, J. E. (2006). Temperament. In W. Damon, R. Lerner & N. Eisenberg (Eds.), Handbook of child psychology: Vol. 3. Social, emotional, and personality development. 6th edn. (pp. 99–166). New York, NY: Wiley.
Sallquist, J. V., Eisenberg, N., Spinrad, T. L., Reiser, M., Hofer, C., & Liew, J., et al. (2009). Positive and negative emotionality: trajectories across six years and relations with social competence. Emotion (Washington, DC), 9(1), 15–28. https://doi.org/10.1037/a0013970.Positive.
Sanders, W., Zeman, J., Poon, J., & Miller, R. (2015). Child regulation of negative emotions and depressive symptoms: the moderating role of parental emotion socialization. Journal of Child and family Studies, 24(2), 402–415. https://doi.org/10.1007/s10826-013-9850-y.
Schwartz, O., Sheeber, L., Dudgeon, P., & Allen, N. (2012). Emotion socialization within the family environment and adolescent depression. Clinical Psychology Review, 32(6), 447–453. https://doi.org/10.1016/j.cpr.2012.05.002.
Schwartzman, A. E., Ledingham, J. E., & Serbin, L. A. (1985). Identification of children at risk for adult schizophrenia: A longitudinal study. Applied Psychology, 34(3), 363–379. https://doi.org/10.1111/j.1464-0597.1985.tb01333.x.
Serbin, L. A., Cooperman, J. M., Peters, P. L., Lehoux, P. M., Stack, D. M., & Schwartzman, A. E. (1998). Intergenerational transfer of psychosocial risk in women with childhood histories of aggression, withdrawal, or aggression and withdrawal. Developmental Psychology, 34(6), 1246–1262. https://doi.org/10.1037/0012-1649.34.6.1246.
Shaw, D., Keenan, K., Vondra, J. I., Delliquadri, E., & Giovannelli, J. (1998). Antecedents of preschool children’s internalizing problems: A longitudinal study of low-income families. Journal of the American Academy of Child and Adolescent Psychiatry, 36, 1760–1767. https://doi.org/10.1097/00004583-199712000-00025.
Shenk, C. E., & Fruzzetti, A. E. (2011). The impact of validating and invalidating responses on emotional reactivity. Journal of Social and Clinical Psychology, 30(2), 163–183. https://doi.org/10.1521/jscp.2011.30.2.163.
Shortt, J. W., Katz, L. F., Allen, N. B., Leve, C., Davis, B., & Sheeber, L. B. (2016). Emotion socialization in the context of risk and psychopathology: mother and father socialization of anger and sadness in adolescents with depressive disorder. Social Development, 25(1), 27–46. https://doi.org/10.1111/sode.12138.
Silk, J. S., Shaw, D. S., Prout, J. T., O’Rourke, F., Lane, T. J., & Kovacs, M. (2011). Socialization of emotion and offspring internalizing symptoms in mothers with childhood-onset depression. Journal of Applied Developmental Psychology, 32(3), 127–136. https://doi.org/10.1016/j.appdev.2011.02.001.
Spence, R., Owens, M., & Goodyer, I. (2013). The longitudinal psychometric properties of the EAS temperament survey in adolescence. Journal of Personality Assessment, 95(6), 633–639. https://doi.org/10.1080/00223891.2013.819513.
Stack, D. M., Serbin, L. A., Mantis, I., & Kingdon, D. (2015). Breaking the cycle of adversity in vulnerable children and families: a thirty-five year study of at-risk lower income families. International Journal for Family Research and Policy, 1(1), 31–56.
Tingley, D., Yamamoto, T., Hirose, K., Keele, L., & Imai, K. (2014). Mediation: R package for casual mediation analysis. Journal of Statistical Software, 59(5), 1–38.
Tomkins, S. S. (1963). Affect, imagery, consciousness: Vol. 2. Negative affects. New York, NY: Springer.
Tomkins, S. S. (1991). Affect, imagery, consciousness: Vol. 3. Anger and fear. New York, NY: Springer.
Treiman, D. J. (1977). Occupational prestige in comparative perspective. New York, NY: Academic Press.
Wenzlaff, R. M., & Eisenberg, A. R. (1998). Parental restrictiveness of negative emotions: sowing the seeds of thought suppression. Psychological Inquiry, 9(4), 310–313. https://doi.org/10.1207/s15327965pli0904_15.
Woodruff-Borden, J., Morrow, C., Bourland, S., & Cambron, S. (2002). The behavior of anxious parents: examining mechanisms of transmission of anxiety from parent to child. Journal of Clinical Child and Adolescent Psychology, 31(3), 364–374. https://doi.org/10.1207/S15374424JCCP3103_08.
Yap, M., Allen, N., & Sheeber, L. (2007). Using an emotion regulation framework to understand the role of temperament and family processes in risk for adolescent depressive disorders. Clinical Child and Family Psychology Review, 10(2), 180–196. https://doi.org/10.1007/s10567-006-0014-0.
Yap, M. B. H., Allen, N. B., Leve, C., & Katz, L. F. (2008). Maternal meta-emotion philosophy and socialization of adolescent affect: the moderating role of adolescent temperament. Journal of Family Psychology, 22(5), 688–700. https://doi.org/10.1037/a0013104.
Zeman, J., Cassano, M., & Adrian, M. C. (2013). Socialization influences on children’s and adolescents’ emotional self-regulation processes: a developmental psychopathology perspective. In K. C. Barrett, N. A. Fox, G. A. Morgan, D. J. Fidler & L. A. Daunhauer (Eds.), Handbook of self-regulatory processes in development: New directions and international perspectives (pp. 79–106). New York, NY: Psychology Press.
Acknowledgements
This research was conducted by authors at the Department of Psychology and Centre for Research in Human Development (CRDH), Concordia University. The research described in this article was partially supported by grants from Fonds Québécois de la Recherche sur la Société et la Culture (FQRSC), currently, Fonds de Recherche du Québec—Société et Culture (FRQSC); 6 investigators including Serbin, Stack, Schwartzman), and the Social Sciences and Humanities Research Council of Canada (SSHRC) awarded to Dale M. Stack and Lisa A. Serbin, and Canadian Institutes of Health Research, Child & Youth Mental Health and Well-Being (Health Canada), as well as support from Concordia University and CRDH awarded to Serbin, Stack and Schwartzman. The Concordia Project originated in 1976 under the direction of Jane Ledingham and Alex E. Schwartzman. The intergenerational project is currently directed by Lisa A. Serbin and Dale M. Stack. We extend our gratitude to Catherine Delisle and Joelle Bélisle-Cuillerier for their help in the final preparation of the manuscript. We also wish to thank Claude Senneville and the Concordia Project team for their assistance in data management and collection. Finally, we are most indebted to the participants in the study.
Authors’ Contributions
C.B. conceived of the design and interpretation of the data and drafted the manuscript. D.M.S. conceived of the study and participated in the design and coordination of the study, as well as participated in the interpretation and drafting of the manuscript. D.J.D. re-analyzed the data according to reviewer specifications and wrote portions of the manuscript related to analyses and results. L.A.S. conceived of the study and participated in the design and coordination of the study. All authors read and approved the final manuscript.
Funding
The funding sources for this research were awarded from Health Canada (6070-10-5/9515) and the Social Sciences and Humanities Research Council of Canada (410-2005-1599), and Fonds Québécois de la Recherche sur la Société et la Culture (2005-SE-96123) and these are gratefully acknowledged.
Data Sharing and Declaration
This manuscript’s data will not be deposited.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
The authors received ethical approval for all research reported in the present study.
Informed Consent
Informed consent was received from all participants.
Rights and permissions
About this article

Cite this article
Briscoe, C., Stack, D.M., Dickson, D.J. et al. Maternal Emotion Socialization Mediates the Relationship between Maternal and Adolescent Negative Emotionality. J Youth Adolescence 48, 495–509 (2019). https://doi.org/10.1007/s10964-018-0945-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-018-0945-z