
Abstract
Ethnic identity is an important buffer against drug use among minority youth. However, limited work has examined pathways through which ethnic identity mitigates risk. School-aged youth (N = 34,708; 52 % female) of diverse backgrounds (i.e., African American (n = 5333), Asian (n = 392), Hispanic (n = 662), Multiracial (n = 2129), Native American (n = 474), and White (n = 25718) in grades 4–12 provided data on ethnic identity, drug attitudes, and drug use. After controlling for gender and grade, higher ethnic identity was associated with lower past month drug use for African American, Hispanic, and Multiracial youth. Conversely, high ethnic identity was associated with increased risk for White youth. An indirect pathway between ethnic identity, drug attitudes, and drug use was also found for African American, Hispanic, and Asian youth. Among White youth the path model was also significant, but in the opposite direction. These findings confirm the importance of ethnic identity for most minority youth. Further research is needed to better understand the association between ethnic identity and drug use for Multiracial and Hispanic youth, best ways to facilitate healthy ethnic identity development for minority youth, and how to moderate the risk of identity development for White youth.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Drug use among adolescent populations is a public health concern, as by the time youth reach 12th grade almost 70 % have tried alcohol and almost 50 % have used marijuana (National Institute on Drug Abuse [NIDA] 2014). Moreover, the negative social, mental, and physical health outcomes associated with drug use during this developmental period are considerable. Alcohol use has been linked to increased risk for violent behavior and interpersonal problems (Huang et al. 2001; Shepherd et al. 2006), criminal offenses (Kuhns et al. 2014; White et al. 2002), and alcohol-related injuries (Maio et al. 2000). Similarly, marijuana use is associated with delinquent behavior, risky sexual behavior, impairments in critical thinking and memory, and negative academic performance (Brook et al. 2002; Lynskey and Hall 2000; NIDA 2014; Volkow et al. 2014). Given that a majority of those diagnosed with a substance use disorder report initiating use before the age of 18 (Dennis et al. 2002; Substance Abuse and Mental Health Services Administration [SAMHSA] 2013; SAMHSA, 2014), understanding the factors associated with risk for and protection from alcohol and marijuana use during adolescence is critical for prevention and intervention purposes.
Racial Differences in Drug Use and Consequences
When conceptualizing risk models, it is important to consider disparities in prevalence and outcomes related to use across racial/ethnic groups. In relation to alcohol consumption, lower rates of use, higher rates of abstinence, and later initiation are generally observed among racial/ethnic minority youth compared to their White peers (Clark et al. 2013a; Chen and Jacobson 2012; Johnston et al. 2014; Wallace et al. 2003; Zapolski et al. 2014). Pertaining to marijuana use, recent national reports indicate a rise in the prevalence of use among racial/ethnic minority youth, such that current rates of use are equivalent to or higher than those found among their White peers (Chen and Jacobson 2012; Johnston et al. 2014; Johnson et al. 2015; Wu et al. 2015), with some also finding earlier initiation of marijuana among minority youth (Kosterman et al. 2000).
Notable exceptions to the generalized findings above include Asian American youth, who have lower odds of initiating marijuana use (Kosterman et al. 2000) or of being a current user compared to other racial/ethnic groups (Johnson et al. 2015; Wu et al. 2015). Conversely, Native American youth populations show higher rates of alcohol and marijuana use than youth of other minority groups, and are found to have rates equal or higher than those of White youth (Clark et al. 2013a; Johnson et al. 2015; Wallace et al. 2003; Wu et al. 2015). Higher rates of alcohol and marijuana use have also been reported among Multiracial youth then their monoracial minority peers (Clark et al. 2013a; Johnson et al. 2015; Wu et al. 2015), although mixed findings have been noted in comparison to White peers depending on the biracial subgroups one identifies with (e.g., White-Native American; White-Black; White-Asian; Black-Hispanic; Chavez and Sanchez 2010; Clark et al. 2013a, b).
Yet, regardless of group membership, findings suggest that minority youth experience more drug related problems than White youth. For example, it has been documented that African Americans and Hispanic youth experience more alcohol related problems than their White counterparts, even at equivalent or lower levels of use (Witbrodt et al. 2014; Zapolski et al. 2014). Disparities are also observed in adulthood, with disproportionately higher prevalence of alcohol use disorders among Black and Hispanic adults (Williams et al. 2016). Similar findings have been documented for marijuana use, with greater odds of cannabis use disorders among African American, Hispanic, and Native American youth than Whites (Nguyen and Reuter 2012; Wu et al. 2015, 2011). Hispanic youth are also more likely to be a “hard drug user” (e.g., cocaine, heroin, etc.) as a consequence of cannabis use compared to White, Asian, and African American adolescents (Ellickson and Morton 1999). Interestingly, although Asian youth are less likely to engage in marijuana use compared to their peers, those who do use are at greater risk of illicit drug use than White adolescents (Ellickson and Morton 1999). Thus, gaining a better understanding about risk for and protection for alcohol and marijuana use among these racial/ethnic groups is critical.
Ethnic Identity and Drug Use
Among research examining drug use and consequences among racial/ethnic minority youth, the buffering effect of ethnic identityFootnote 1—a construct that includes clarity and resolution about one’s ethnic background, affect and regard toward one’s ethnic group, and behavioral engagement with one’s ethnic heritage—has received much attention (Phinney 1989, 1990, 2000; Umaña-Taylor et al. 2014). Ethnic identity development is based on social identity theory, and is characterized as a process by which an individual begins to determine who he/she is and integrates different dimensions of their life, including their race or ethnicity, into their identity (Erikson 1968; Phinney 1992). As such, ethnic identity has been shown to begin to solidify during adolescence (Phinney and Chavira 1995; Quintana et al. 2006; Yip et al. 2006), and is thus a critical developmental period to examine its impact on adolescent health outcomes.
The protective effect of ethnic identity has been shown to have both a direct and indirect effect on adolescent health. The indirect effect of ethnic identity has been primarily examined as a mechanism through which the negative effect of exposure to racial discrimination on health outcomes can be mitigated (Sellers et al. 2006). Researchers have also documented a direct protective effect of ethnic identity, independent of stress exposure, on adolescent health. Positive outcomes include the development of a positive self-concept, fewer depressive symptoms and somatic complaints, higher academic motivation, and greater academic achievement (see Rivas-Drake et al. 2014; Smith and Silva 2011). A similar protective effect has also been proposed for drug use, such that adolescents who strongly identify with their ethnic community and culture are speculated to be less vulnerable to risk factors for drug use (Zickler 1999). Numerous findings support this hypothesis demonstrating that a stronger sense of ethnic identity is associated with lower risk for alcohol use and related problems (Caldwell et al. 2004; Marsiglia et al. 2001; Nasim et al. 2007; Yu and Stiffman 2007), marijuana use (e.g., Marsiglia et al. 2004), and drug use more broadly (Smith and Silva 2011).
The most robust effect of ethnic identity of drug use has been observed among African American youth (e.g., Brook et al. 1998; Burlew et al. 2000; Caldwell et al. 2004). Findings have been less consistent among Multiracial youth, with some observing a protective effect of ethnic identity on drug use (e.g., Choi et al. 2006), whereas others have found a null relationship (e.g., James et al. 2000; Marsiglia et al. 2001). Researchers have postulated that these inconsistencies may be due complexities in measuring multiple ethnic identities within a single measure for Multiracial youth (Choi et al. 2006). Moreover, although a majority of studies examining ethnic identity have focused on minority youth, some studies have included White youth. Among such studies, findings have been mixed as to whether ethnic identity is a protective factor (Marsiglia et al. 2004; Prelow et al. 2007) or a risk factor for drug use (Miller-Day and Barnett 2004; Marsiglia et al. 2001) among White youth.
Despite these inconsistencies, overall, the protective effect of ethnic identity on drug use has been well established for the majority of racial groups; however, less work has been conducted on understanding the mechanisms through which ethnic identity operates (Neblett et al. 2012). Unger (2011) proposed a theoretical model on the role of cultural identity—a broader term to encompass ethnic identity, as well as membership with others based on shared traits, interests, knowledge, or behaviors—on adolescent health outcomes. Specifically, it was posited that a causal pathway between cultural identity and health-related behaviors was mediated by several cognitive processes, including adoption of cultural values, which was defined as attitudes, beliefs, priorities, and behaviors emphasized, encouraged, and viewed as desirable by the group (McElroy and Jezewski 2000). There is empirical support for the relationship between cultural values and drug use. Unger et al. (2002) found that filial piety was related to lower drug use among a multiethnic sample of California adolescents, due to internalizing the cultural values of piety and being more inclined to obey parental rules regarding drug use. Similarly, a study among Asian American and Hispanic youth found a negative association between values of politeness and respect for adults with tobacco use (Unger et al. 2006). It was posited that lower youth drug use was observed among these studies due to youth’s internalization of the cultural groups values, which in turn influenced their decision to engage in the health behaviors.
In light of this theoretical model, a related potential mechanism through which ethnic identity may protect youth against drug use is through the development of anti-drug attitudes that are congruent with the cultural groups’ attitudes and beliefs regarding drug use (Belgrave et al. 1994, 1997; Unger 2011). There is empirical evidence to support the positive association between ethnic identity and anti-drug attitudes, for African American (Wallace and Fisher 2007; Belgrave et al. 2000; Burlew et al. 2000; Corneille and Belgrave 2007; Townsend and Belgrave 2000; Rivas-Drake et al. 2014), Hispanic, and Native American youth (Holley et al. 2006; Marsiglia et al. 2004; Kulis et al. 2002; Rivas-Drake et al. 2014). We postulate that this effect may be due to more conservative norms and beliefs regarding drug use within these cultural groups. For African Americans, more negative beliefs regarding alcohol use have been documented among both parents and youth compared to their White counterparts (Zapolski et al. 2014). Additionally, African American youth report more disapproval of cannabis use compared to their White counterparts (Wu et al. 2015). Similar cultural norms have been documented for Asian Americans and Hispanics, with a national study among youth 12–17 finding that Asian-Americans were approximately twice as likely as Whites to report personal, parental, or close friend disapproval of cannabis use, and Hispanic youth reporting more parental disapproval of cannabis use compared to their White peers (Wu et al. 2015).
Given the positive association between ethnic identity and drug use attitudes and the positive association between drug attitudes and use (Best et al. 2000; Wright et al. 2016), it is plausible that ethnic identity may influence risk for drug use indirectly through drug use attitudes. However, to our knowledge, no study has examined a path model between ethnic identity, drug attitudes, and drug use. Understanding this pathway is important, as it will provide clarity on the underlying mechanisms through which ethnic identity buffers drug use risk and whether this relationship is found among youth of various racial/ethnic backgrounds. The results from this study can also be used to inform drug preventative programing on best practices to reduce drug use and drug use cognitions among adolescent populations.
Current Study and Hypotheses
The current study will examine the indirect effect of drug attitudes on the relationship between ethnic identity and drug use among 34,708 adolescents between 4th and 12th grade. Given mixed findings on the effect of ethnic identity on drug use among White and Multiracial youth, as well as limited available data on the effect ethnic identity has on drug attitudes among minority populations, the current study will add to existing literature by examining these relationships among a diverse sample of youth who self-identify as either African American, Native American, Asian, Hispanic, Multiracial, or White.
The primary goal of the current study is to establish whether the pathway between ethnic identity, drug use attitudes, and drug use exists among each racial/ethnic group. We hypothesize that higher ethnic identity will predict lower drug use across all ethnic groups, with the exception of White and Multiracial youth, in which a null effect will be found. Similar to the direct effect of ethnic identity on drug use, we hypothesize that higher ethnic identity will predict lower drug attitudes for all groups except White and Multiracial youth. Conversely, given the strong association between drug attitudes and drug use found in the literature (Best et al. 2000; Wright et al. 2016), we hypothesize a significant positive relationship between the two factors for all groups. Lastly, given no previous studies documenting the pathway between ethnic identity, drug attitudes, and drug use, we hypothesize the indirect path will be found but have no a priori hypotheses as to whether the effect will be observed for all groups.
Methods
Participants and Procedures
The current study involves participants drawn from a 5-wave parent study examining school and health behavior outcomes among students between fourth and twelfth grade. As approved by the University IRB, participants were sampled from 159 schools (21 school districts) in a large Midwestern county. Informed consent forms were sent home to parents of potential participants. Signed consent forms were obtained from 50 % of parents (approximately 12,000 per year). Retention rates for waves 2 through 5 were modest with approximately half of the participants (45.3 %) completing more than one wave of data (see Barnes et al. 2009, for further information about the parent study).
For the current study, all participants who provided data on the study variables of interest at a minimum of one data point were retained, for a final sample size of 34,708 youth. Among this sample, the majority of the participants self-identified as White (71.8 %), followed by African American (16.8 %), Multiracial (6.1 %), Hispanic (1.9 %), Native American (1.5 %), and Asian (1.1 %). Participants were equally divided based on gender (52 % female), and on average the students were in seventh grade (SD = 1.96) at the first wave of data collection.
Measures
Demographic information
Participants were asked to indicate their gender, grade, birthdate, and racial/ethnic background (i.e., African American, Native American, Asian, Hispanic, Multiracial, White, and Other). All participants were included in the study, except for those who identified their race as Other.
Ethnic identity
The Multi-group Ethnic Identity Measure (MEIM; Roberts et al. 1999) was used as a measure of ethnic identity that could be utilized across racial/ethnic groups. The MEIM is a 12-item scale designed to measure two components of ethnic identity: exploration and affirmation. Sample items from each subscale include, “In order to learn more about my ethnic background, I have often talked to other people about my ethnic group” for the exploration subscale and “I feel good about my cultural or ethnic background” for the affirmation subscale. Items were rated on a 4-point Likert scale, with responses ranging from 1 (strongly disagree) to 4 (strongly agree). A composite score based on all 12 MEIM items was used for the current study. The scale had high internal consistency across all waves of data collection for each racial/ethnic group (α = .88 for African American, .91 for Asian American, .91 for Hispanic, .91 for Multiracial, .91 for Native American, and .88 for White), which is consistent with previous literature with reliability ranging from .81–.92 (Ponterotto et al. 2003).
Drug use attitudes
The drug use attitude measure was adapted from items included in various national studies conducted among youth (e.g., Monitoring the Future, Youth Risk Behavior Surveillance Survey (YRBSS)). Participants were asked to indicate how harmful they thought it was to “drink alcohol occasionally” and “use marijuana” on a 3-point Likert scale ranging from 1 (very bad for you) to 3 (not very bad for you). Reponses were summed into a “drug attitudes” scale with higher scores indicating less harmful attitudes regarding drug use. There was adequate internal consistency across all waves of data collection for each racial/ethnic group (α = .76 for African American, .75 for Asian American, .78 for Hispanic, .74 for Multiracial, .78 for Native American, and .73 for White).
Drug use
The drug use measure was also adapted from items included in various national studies conducted among youth (e.g., Monitoring the Future, YRBSS). Participants were asked to indicate how many days in the past 30 days had they “had at least one drink of alcohol,” and “used marijuana.” Responses choices were provided on a 7-point Likert scale, with 1 (0-days), 2 (1 or 2 days), 3 (3–5 days), 4 (6–9 days), 5 (10–19 days), 6 (20–29 days), and 7 (everyday). Reponses were summed for a “drug use” scale. There was high internal consistency across all waves of data collection for each racial/ethnic group (α = .81 for African American, .91 for Asian American, .88 for Hispanic, .87 for Multiracial, .91 for Native American, and .89 for White).
Data Analyses
To test for group differences on the study variables, one-way ANOVA models were estimated and tested for each of the study variables (i.e., ethnic identity, drug attitudes, drug use) based on racial group membership. If significant differences were observed, Tukey HSD (Honestly Significant Difference) post-hoc analyses were conducted to test specific group differences. These preliminary analyses were conducted in SPSS (version 24). A path model approach was used to test the within-person effect of ethnic identity on adolescent drug use attitudes and past 30-day drug, controlling for gender and grade. As these data were hierarchical—that is repeated measurements of ethnic identity, drug attitudes, and drug use taken at every time point (Level 1) were nested within school (Level 2). We used a two-level multilevel analysis approach, as the interclass correlation coefficients (ICC) were .056 for ethnic identity, .33 for drug use, and .34 for drug use attitudes, indicating that school membership had a significant effect on drug use outcomes. All models were conducted using ml_mediation in Stata (version 13.0), and engaged a random intercept (Krull and MacKinnon 2001). The significance of the indirect, direct, and total effects, and the standard errors and confidence intervals were generated, using a n = 500 bootstrap procedure. All available data were used for the study analyses, with no data imputed. The pathways between ethnic identity, drug attitudes, and drug use were conducted within each wave of data collection. Analyses are also stratified by race in order to examine the study hypothesis as to whether these effects are found for each group.
Results
Group Differences on Study Variables
Prior to conducting the path modeling, we examined descriptive statistics and mean differences between racial/ethnic groups on the study variables. Based on a one-way ANOVA, participants differed in their ratings of ethnic identity F(6, 34,871) = 268.10, p < .001, drug attitudes F(6, 34,875) = 71.64, p < .001, and drug use F(6, 34,874) = 12.89, p < .001. Specifically, findings indicated significantly higher rates of ethnic identity for African Americans than other racial/ethnic groups, except Asian Americans. Conversely, White youth reported significantly lower ethnic identity than all other racial/ethnic groups. Related to drug beliefs, African Americans reported stronger beliefs that drug use was harmful compared to the other racial/ethnic groups, although they were not statistically different from Asian youth. Conversely, Hispanic youth reported the strongest beliefs that drug use was not harmful compared to youth of other racial/ethnic groups. As for drug use, Hispanic youth reported statistically greater use than all other groups, except for Native American youth. Refer to Table 1 for more details on mean differences across racial/ethnic groups.
A correlation matrix was also constructed to assess the association between the study variables across all waves of data collection (Table 2). Because gender is dichotomous, correlations between these two variables are point-biseral coefficients. Correlations with grade are Spearman correlations and the remaining correlations are Pearson correlations. Ethnic identity was negatively correlated with drug attitudes and use (r = −.142 and −.127, p < .001, respectively). Drug attitudes and drug use were also positively correlated (r = .505, p < .001). Gender and grade differences were observed. Females reported stronger ethnic identity (r = .069, p < .001) and lower drug attitudes (r = −.025, p < .001) and drug use (r = −.047, p < .001) than males. Older youth reported lower ethnic identity (r = −.080, p < .001), lower perceived harms of drug use (r = .402, p < .001) and greater drug use (r = .295, p < .001) than younger participants
Path Model: Ethnic Identity, Drug Attitudes, and Drug Use
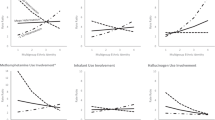
Multilevel path models were estimated to test the hypothesized direct protective effect of ethnic identity on past-month drug use and whether the pathway operated indirectly through drug attitudes for each racial/ethnic group. Given the significant correlation between gender and grade on ethnic identity, drug attitudes, and drug use, they were controlled for within the path models. Findings indicated that higher ethnic identity was directly associated with lower drug use for African American (β = −7.46, p < .001), Hispanic (β = −3.21, p = .001), and Multiracial (β = −5.92, p < .001) youth. A null effect was found for Asian American (β = −1.76, p = .078) and Native American (β = −1.88, p = .06) youth. For White youth, the opposite relationship was observed, with greater ethnic identity associated with higher drug use (β = 6.95, p < .001). The direct effect of ethnic identity on drug attitudes was only observed for a subset of youth, with higher ethnic identity associated with more negative drug attitudes for African American (β = −6.42, p < .001), Asian (β = −3.10, p = .002), and Hispanic (β = −2.62, p = .009) youth. For White youth, the opposite relationship was observed, with greater ethnic identity associated with higher drug attitudes (β = 3.14, p = .002). A null relationship was observed for Multiracial (β = −1.08, p = .279) and Native American (β = −1.59, p = .111) youth.
When assessing the path model including drug attitudes, the protective effect of ethnic identity on past month drug use through attitudes was significant for African American (b = −4.31, 95 % Boot CI = −.14, −.05), Hispanic (b = −2.63, 95 % Boot CI = −.31, −.05), and Asian (b = −2.25, 95 % Boot CI = −.49, −.03) youth. Among White youth the path model was also significant, but in the opposite direction (b = 2.62, 95 % Boot CI = .00, .003). These pathways accounted for 36.7 % of the variance in drug use for African American youth, 42.3 % of the variance for Hispanic youth, 91.9 % of variance for Asian youth, and 20.1 % of the variance for White youth. See Table 3 and Fig. 1 for all path coefficients.

Depiction of structural model representing the pathways to drug use among African American, Asian American, Hispanic American, and White youth based on ethnic identity development and drug attitudes. Not included in the figure, for ease of presentation, are disturbance terms and error terms. *p < .05, **p < .01, ***p < .001
Discussion
Prior research has documented that ethnic identity development is protective against drug use among youth, with a particularly robust effect found for African American youth (e.g., Burlew et al. 2000; Caldwell et al. 2004). However, little attention has been given to the mechanism through which ethnic identity influences drug use. Thus, the current study aimed to be the first, to date, to examine whether the buffering of ethnic identity on drug use (i.e., alcohol and marijuana use) operated indirectly through drug attitudes among a diverse sample of youth. Overall our findings were consistent with previous literature in that ethnic identity appears to be protective broadly speaking for racial/ethnic minority youth. However, the impact of ethnic identity on drug use through changes in drug attitudes was only observed among African American, Asian, and Hispanic youth.
Among these three minority groups, the amount of variance accounted for also varied, such that 36.7 % of the variance was accounted for among African American youth, 42.3 % of the variance accounted for among Hispanic youth, and 91.9 % of variance accounted for among Asian youth. Although statistical equivalence between racial/ethnic groups was not hypothesized or tested, these findings indicate that the indirect pathway may be particularly strong for Asian youth, suggesting that changing drug use attitudes may be the primary process through which ethnic identity development reduces drug use vulnerability among this group of youth. However, for African American and Hispanic youth, although ethnic identity had a significant impact on drug attitudes and use, other factors may also mediate this relationship. Future studies should examine additional mediating factors such as self-esteem (Bracey et al. 2004; Smith et al. 1999; Umaña-Taylor 2004), beliefs regarding normative behavior (Unger 2011), and peer influences (Ford and Hill 2012).
A significant indirect effect between ethnic identity, drug attitudes, and drug use was not observed for Native American and Multiracial youth, which is consistent with a broader body of research documenting a null effect between ethnic identity and drug use among these subgroups of youth (James et al. 2000; Markstrom et al. 2011; Marsiglia et al. 2001; Whitesell et al. 2014). Potential explanations for this finding may include the complexity in measuring ethnic identity and the social norms of use within Native American and Multiracial communities. For example, Markstrom (2011) proposed a multifaceted model for Native American ethnic identity that include domains outside of those measured by the MEIM, such as connection to land and spirituality. Additionally, when the overall construct of ethnic identity has been disaggregated, differing effects on drug outcomes have been found, such that Native Americans with a stronger sense of ethnic pride displayed more antidrug attitudes while ethnic behavior was unrelated to attitudes towards drugs (Kulis et al. 2002). Thus, further research is needed to understand the unique components of ethnic identity development specific for Native American youth and how varying dimensions of ethnic identity impact drug outcomes among this subgroup of youth.
The measurement of ethnic identity for Multiracial youth may also vary from traditional measures. While the MEIM has been found to be a valid tool among adolescent populations, with high internal consistency found across racial/ethnic groups, the use of the total score may not be measuring the intended construct for Multiracial youth. Researchers assert that a fully realized positive identity for Multiracial youth consists of an additional step of accepting all parts of their identity, a step that is not represented in the MEIM (Neblett et al. 2012). Thus, further work is needed in the area of measurement development to ensure that ethnic identity measures are capturing all the components experienced in developing ethnic identity for Multiracial. However, after addressing measurement issues, it is possible that higher ethnic identity may actually increase pro-drug norms for these groups, as researchers have noted lower odds of personal, parental, and close friend disapproval of cannabis use among Multiracial youth (Wu et al. 2015) and greater perceived normative use of drugs among Native Americans compared to other racial/ethnic groups (Swaim et al. 2013).
For White youth, high ethnic identity was not protective against drug use, but was associated with higher risk for pro-drug attitudes and drug use. Other studies have also found a similar effect for ethnic identity among this subpopulation of youth (Miller-Day and Barnett 2004; Marsiglia et al. 2001). It may be the case that due to lower perceived disapproval of drug use (Wu et al. 2015) and more permissive views about alcohol particularly among White parents compared to other racial/ethnic groups (James and Johnson 1996; Peterson et al. 1994), a stronger connection with White identity may increase use among this subgroup of youth. As reported by Miller-Day and Barnett (2004), White youth within their study who reported a strong connection with their ethnicity also professed a desire to be similar to others, reported personal norms favorable to drug use, and reported greater drug use.
There are also two other factors that may help explain mixed findings in the literature on the impact of ethnic identity on drug use outcomes among White youth—heterogeneity within the group and contact with racial/ethnic minority youth. First, some individuals who identity as White develop attachments with specific ethnic groups, such as German, British, or Italian ancestry (McDermott 2015; Torkelson and Hartmann 2010) and thus may develop their ethnic identity based on these identifications. It is plausible that the effect of ethnic identity on drug use outcomes may vary based on the specific ethnic group a White youth identifies with. Further work is needed to test this hypothesis. Secondly, we speculate that the level of contact White youth have with racial/ethnic minority may impact not only their own ethnic identity development (Fisher et al. 2014; Hartigan 1999; French et al. 2000; McKinney 2006; Morris 2006; Peterson and Hamrick 2009), but also their views on drug use and drug use behaviors. Specifically, Morris (2006) found that White individuals with limited contact with those of other racial backgrounds are more prone to experience the “invisibility of Whiteness” which can contribute to a lack of understanding of what it means to be White and in turn what it means to explore or affirm one’s White identity. However, White individuals who are surrounded by racial/ethnic minorities are more aware of their race/ethnicity and are more inclined to acknowledge and develop their own racial/ethnic identity (Morris 2006). Moreover, being a numeric minority has also been shown to alter drug use behaviors, such that White youth are less likely to use when their social context is primarily composed of non-White peers (Su and Supple 2016; Seffrin 2012). More research is needed to disentangle the relationship between ethnic identity and drug use among White adolescents based on family ethnic origin and social context.
Limitations
Although the current study provides useful data related to an understudied area of research, several limitations must also be noted and taken into consideration when interpreting these results. First, researchers have noted that these inconsistent findings in the literature related to the relationship between ethnic identity and drug use may be due to a number of factors including variation in the meaning of ethnic identity across different groups, as well as variations in the measurement of ethnic identity across studies (Fuller-Rowell et al. 2012; Smith and Silva 2011; Ponterotto and Park-Taylor 2007). Our study did not explore whether there was a differentiation between the ethnic identity participants indicated on the demographic form and how they may have identified themselves when completing the ethnic identity measure. Additionally, we utilized the MEIM composite score of ethnic identity and although there is a breath of research qualifying the validity of the measurement, as well as findings of high internal consistency of the measure for each racial/ethnic group, there are some who suggest use of the MEIM subscales (Ponterotto et al. 2003). We used the composite due to limited research examining the impact of ethnic identity on drug attitudes and drug use among a large sample of diverse youth. Subsequent studies may further examine these relationships based on MEIM subscales, as well as examine variations in the assessment of ethnic identity, particularly for Native American and Multiracial youth. Third, although we used a longitudinal dataset, due to a limited number of youth with consecutive data points, analyses were run cross-sectionally within time-point. Thus, we cannot confirm the temporal ordering of our findings. Further longitudinal research is needed to confirm these proposed pathways.
Future Research
To our knowledge, this is the first study to examine the indirect effect of drug attitudes on the relationship between ethnic identity and drug use among a diverse sample of youth. Implications from this study can be used to inform drug use prevention programming. Specifically, given the strong association that drug attitudes has on drug use (Best et al. 2000; Wright et al. 2016), interventions that work to reduce positive beliefs regarding drugs can have a long-lasting effect on drug use among adolescents. Based on our finding, addressing drug use attitudes can be done through including aspects of ethnic identity development in existing programs, particularly for Asian American youth. For African American and Hispanic youth, although ethnic identity was associated with decreased drug use though reduction of drug attitudes, a little over half of variance remained unexplained in our model. Thus, additional factors, such as self-esteem (Bracey et al. 2004), beliefs regarding normative behavior (Unger 2011), and peer influences (Ford and Hill 2012) should be explored. Moreover, for Hispanic youth, disentangling the impact of ethnic identity from level of acculturation may also be critical, as it has been documented that a lack of acculturation or maintenance of the norms, beliefs and practices of one’s culture of origin is protective against drug use for youth, whereas assimilating to mainstream society is harmful (Lara et al. 2005; Salas-Wright et al. 2015; Savage and Mezuk 2014; Szapocznik et al. 2007; Thai et al. 2010; Wright et al. 2016). Future research should explore the incremental predictability of acculturation status vs. level of ethnic identity development on both drug attitudes and drug use. Interestingly, the path model between ethnic identity, drug attitudes, and drug use was not found among self-identified Native American or Multiracial youth. The factors identified above may also serve to be particularly critical mechanisms given the lack of support for drug attitudes within our model.
The current study also paves the way for additional research questions, such as understanding antecedents to the development of ethnic identity, as well as moderators that impact the strength of the relationship between ethnic identity and mediating variables (i.e., drug attitudes, self-esteem). For example, it is plausible that ethnic identity development is facilitated through contextual factors within a youth’s home environment, such as interactions with parents and educators, through which youth are provided massages regarding self-worth and their identity (e.g., Douglass and Umaña-Taylor 2015; Gonzalez et al. 2014; Holcomb-McCoy 2005; Peck et al. 2014). For example, studies have shown that parental communication (i.e., racial/ethnic socialization) is associated with stronger ethnic identity and self-esteem (Hughes et al. 2006, 2009; Peck et al. 2014), which may in turn lower risk for drug use (Szapocznik et al. 2007). Additional attention can also be placed on gaining a better understanding of the messages regarding ethnic identity through the media (Adams-Bass et al. 2014; Leavitt et al. 2015; Martin 2008), and its impact on drug use and health outcomes. Religiosity may serve as an important contextual factor that may both mediate and moderate the effect of ethnic identity on drug attitudes, as researchers have documented that youth with closer cultural ties to a religion that frowns upon drug use, report more harmful views of drug use (Ford and Hill 2012) and less drug use (Ford and Hill 2012; Kelly et al. 2015; Wallace et al. 2007).
Last, given the novelty of the current study, our goal was to test whether a pathway between ethnic identity, drug attitudes, and drug use existed for each racial/ethnic group, rather than attempt to compare the strength of the associations across groups. Future studies can build off of this work to empirically test whether the impact of ethnic identity on drug attitudes and drug use, or any of the other mediating variables proposed above, function statistically different across racial/ethnic groups. This work may provide support for indicated or tailored intervention programs for specific racial/ethnic groups. Additionally, future studies can build off of this work to examine whether there is a critical age during which ethnic identity is the most impactful on drug use outcomes, which would provide support for implementing intervention programming among particular age cohorts of youth (i.e., interventions tailored to elementary school vs. middle or high school students).
Conclusion
In sum, the current study contributes to the literature on adolescents’ drug use vulnerability by examining the relationships between ethnic identity development, drug use attitudes, and drug use among a large diverse sample of school-aged youth. Results documented a protective effect of ethnic identity on drug use through drug attitudes for Asian, African American, and Hispanic youth, while at the same time uncovering ethnic identity as a risk factor for White youth. Moreover, no effect of ethnic identity on drug use attitudes and subsequent use was found for Native American and Multiracial youth. Given that ethnic identity development is a critical developmental milestone for youth, as it helps determine who they are and how best to integrate different dimensions of themselves into their daily life (Erikson 1968; Phinney 1992), more research is needed to understand how best to conceptualize and facilitate development of ethnic identity for minority youth and moderate the risk of identity development for White youth. Ultimately, such advances in the field on understanding ethnic identity and its impact on drug use can be utilized in intervention efforts among adolescent populations and aid in the reduction of ethnic/racial disparities in drug use outcomes.
Notes
Scholars have noted that the term ethnic identity and racial identity represent very similar constructs at the level of lived experiences (Cross and Cross 2008; Markus 2008), and although they are not synonymous terms (Burlew et al. 2000; Phinney and Ong 2007), scholars have proposed combining them into one unifying construct (Rivas-Drake et al. 2014; Umaña-Taylor et al. 2014). Although some research, primarily those focused on African American sample, use the term racial identity, for ease of presentation, we use the term ethnic identity for all racial/ethnic groups.
Reference
Adams-Bass, V. N., Stevenson, H. C., & Kotzin, D. S. (2014). Measuring the meaning of black media stereotypes and their relationship to the racial identity, black history knowledge, and racial socialization of African American youth. Journal of Black Studies, 45(5), 367–395. doi:10.1177/0021934714530396.
Barnes, J., Almerigi, J., & Hsu, W.W. (2009). Coordinated community assessment: Data from the Coordinated Community Student Survey. http://cerc.msu.edu/research/pastprojects.aspx.
Belgrave, F., Brome, D., & Hampton, C. (2000). The contribution of Africentric values and racial identity to the prediction of drug knowledge, attitudes and use among African American youth. Journal of Black Psychology, 26, 386–401.
Belgrave, F., Cherry, V., & Cunningham, D. (1994). The influence of Africentric values, self-esteem, and Black identity on drug attitudes among African American fifth graders: A preliminary study. Journal of Black Psychology, 20, 143–156.
Belgrave, F. Z., Townsend, T. G., Cherry, V. R., & Cunningham, D. M. (1997). The influence of an Africentric worldview and demographic variables on drug knowledge, attitudes, and use among African American youth. Journal of Community Psychology, 25(5), 421–433.
Best, D., Rawaf, S., Rowley, J., Floyd, K., Manning, V., & Strang, J. (2000). Drinking and smoking as concurrent predictors of illicit drug use and positive drug attitudes in adolescents. Drug and Alcohol Dependence, 60(3), 319–321.
Bracey, J. R., Ba´maca, M. Y., & Umana-Taylor, A. J. (2004). Examining ethnic identity and self-esteem among biracial and monoracial adolescents. Journal of Youth and Adolescence, 33(2), 123–132. doi:10.1023/B:JOYO.0000013424.93635.68.
Brook, J., Balka, E., Brook, D., Win, P., & Gursen, M. (1998). Drug use among African Americans: Ethnic identity as a protective factor. Psychological Reports, 83, 1427–1446.
Brook, J. S., Adams, R. E., Balka, E. B., & Johnson, E. (2002). Early adolescent marijuana use: Risks for the transition to young adulthood. Psychological Medicine, 32(01), 79–91.
Burlew, K., Neely, D., Johnson, C., Hucks, T. C., Purnell, B., & Butler, J., et al. (2000). Drug attitudes, racial identity, and alcohol use among African American adolescents. Journal of Black Psychology, 26(4), 402–420. doi:10.1177/0095798400026004004.
Caldwell, C. H., Sellers, R. M., Bernat, D. H., & Zimmerman, M. A. (2004). Racial identity, parental support, and alcohol use in a sample of academically at-risk African American high school students. American Journal of Community Psychology, 34, 71–81. doi:10.1023/ B:AJCP.0000040147.69287.f7.
Chavez, G. F., & Sanchez, D. T. (2010). A clearer picture of multiracial substance use: Rates and correlates of alcohol and tobacco use in multiracial adolescents and adults. Race and Social Problems, 2(1), 1–18. doi:10.1007/s12552-010-9023-1.
Chen, P., & Jacobson, K. C. (2012). Developmental trajectories of substance use from early adolescence to young adulthood: Gender and racial/ethnic differences. Journal of Adolescent Health, 50(2), 154–163. doi:10.1016/j.jadohealth.2011.05.013.
Choi, Y., Harachi, T. W., Gillmore, M. R., & Catalano, R. F. (2006). Are multiracial adolescents at greater risk? Comparisons of rates, patterns, and correlates of substance use and violence between monoracial and multiracial adolescents. American Journal of Orthopsychiatry, 76(1), 86.
Clark, T. T., Doyle, O., & Clincy, A. (2013a). Age of first cigarette, alcohol, and marijuana use among US biracial/ethnic youth: A population-based study. Addictive Behaviors, 38(9), 2450–2454.
Clark, T. T., Nguyen, A. B., & Kropko, J. (2013b). Epidemiology of drug use among biracial/ethnic youth and young adults: Results from a U.S. population-based survey. Journal of Psychoactive Drugs, 45(2), 99–111. doi:10.1080/02791072.2013.785804.
Corneille, M. A., & Belgrave, F. Z. (2007). Ethnic identity, neighborhood risk, and adolescent drug and sex attitudes and refusal efficacy: The urban African American girls’ experience. Journal of Drug Education, 37(2), 177–190. doi:10.2190/UJ17-34J7-U306-2822.
Cross, W. E., & Cross, T. B. (2008). Theory, research, and models. In S. M. Quintana, & C. McKown (Eds.), Handbook of race, racism, and the developing child (pp. 154–181). Hoboken, NJ: Wiley.
Dennis, M., Babor, T. F., Roebuck, C., & Donaldson, J. (2002). Changing the focus: The case for recognizing and treating cannabis use disorders. Addiction, 97(s1), 4–15.
Douglass, S., & Umaña-Taylor, A. J. (2015). Development of ethnic–racial identity among Latino adolescents and the role of family. Journal of Applied Developmental Psychology, 41, 90–98. doi:10.1016/j.appdev.2015.09.002.
Ellickson, P. L., & Morton, S. C. (1999). Identifying adolescents at risk for hard drug use: Racial/ethnic variations. Journal of Adolescent Health, 25(6), 382–395.
Erikson, E. (1968). Identity: Youth and crisis. New York, NY: Norton.
Fisher, S., Reynolds, J., Hsu, W., Barnes-Najor, J., & Tyler, K. (2014). Examining multiracial youth in context: Ethnic identity and mental health outcomes. Journal of Youth and Adolescence, 43(10), 1688–1699. doi:10.1007/s10964-014-0163-2.
French, S. E., Seidman, E., Allen, L., & Aber, J. L. (2000). Racial/ethnic identity, congruence with the social context, and the transition to high school. Journal of Adolescent Research, 15(5), 587–602. doi:10.1177/0743558400155004.
Fuller-Rowell, T. E., Cogburn, C. D., Brodish, A. B., Peck, S. C., Malanchuk, O., & Eccles, J. S. (2012). Racial discrimination and substance use: Longitudinal associations and identity moderators. Journal of Behavioral Medicine, 35(6), 581–590. doi:10.1007/s10865-011-9388-7.
Ford, J. A., & Hill, T. D. (2012). Religiosity and adolescent substance use: Evidence from the national survey on drug use and health. Substance Use & Misuse, 47(7), 787–798. doi:10.3109/10826084.2012.667489.
Gonzalez, L. M., Eades, M. P., & Supple, A. J. (2014). School community engaging with immigrant youth: Incorporating personal/social development and ethnic identity development. The School Community Journal, 24(1), 99–117.
Hartigan, J. (1999). Racial situations: Class predicaments of whiteness in Detroit. Princeton, NJ: Princeton University Press.
Holcomb-McCoy, C. (2005). Ethnic identity development in early adolescence: Implications and recommendations for middle school counselors. Professional School Counseling, 9(2), 120–127. doi:10.5330/prsc.9.2.21q8m2724r545414.
Holley, L. C., Kulis, S., Marsiglia, F. F., & Keith, V. M. (2006). Ethnicity versus ethnic identity: What predicts substance use norms and behaviors? Journal of Social Work Practice in the Addictions, 6(3), 53–79. doi:10.1300/ J160v06n03_06.
Huang, B., White, H. R., Kosterman, R., Catalano, R. F., & Hawkins, J. D. (2001). Developmental associations between alcohol and interpersonal aggression during adolescence. Journal of Research in Crime and Delinquency, 38(1), 64–83. doi:10.1177/0022427801038001004.
Hughes, D., Rodriguez, J., Smith, E. P., Johnson, D. J., Stevenson, H. C., & Spicer, P. (2006). Parents’ ethnic-racial socialization practices: A review of research and directions for future study. Developmental Psychology, 42(5), 747 doi:10.1037/0012-1649.42.5.747.
Hughes, D., Witherspoon, D., Rivas-Drake, D., & West-Bey, N. (2009). Received ethnic–racial socialization messages and youths’ academic and behavioral outcomes: Examining the mediating role of ethnic identity and self-esteem. Cultural Diversity and Ethnic Minority Psychology, 15(2), 112–124. doi:10.1037/a0015509.
James, S. H., & Johnson, S. L. (1996). Doing drugs: Patterns of African American addiction. Austin, TX: University of Texas Press.
James, W. H., Kim, G. K., & Armijo, E. (2000). The influence of ethnic identity on drug use among ethnic minority adolescents. Journal of Drug Education, 30(3), 265–280.
Johnson, R. M., Fairman, B., Gilreath, T., Xuan, Z., Rothman, E. F., Parnham, T., & Furr-Holden, C. D. M. (2015). Past 15-year trends in adolescent marijuana use: Differences by race/ethnicity and sex. Drug and Alcohol Dependence, 155, 8–15. doi:10.1016/j.drugalcdep.2015.08.025.
Johnston, L. D., O’Malley, P. M., Bachman, J. G., Schulenberg, J. E., & Miech, R. A. (2014). Monitoring the future national survey results on drug use, 1975–2013, vol. I, secondary school students. Ann Arbor, MI: Institute for Social Research, The University of Michigan. http://www.monitoringthefuture.org/pubs/monographs/mtf-vol1_2013.pdf.
Kelly, P. E., Polanin, J. R., Jang, S. J., & Johnson, B. R. (2015). Religion, delinquency, and drug use: A meta-analysis. Criminal Justice Review, 40(4), 505–523.
Kosterman, R., Hawkins, J. D., Guo, J., Catalano, R. F., & Abbott, R. D. (2000). The dynamics of alcohol and marijuana initiation: Patterns and predictors of first use in adolescence. American Journal of Public Health, 90(3), 360–366.
Krull, J. L., & MacKinnon, D. P. (2001). Multilevel modeling of individual and group level mediated effects. Multivariate Behavioral Research, 36(2), 249–277.
Kuhns, J. B., Exum, M. L., Clodfelter, T. A., & Bottia, M. C. (2014). The prevalence of alcohol-involved homicide offending a meta-analytic review. Homicide Studies, 18(3), 251–270. doi:10.1177/1088767913493629.
Kulis, S., Napoli, M., & Marsiglia, F. F. (2002). Ethnic pride, biculturalism, and drug use norms of urban American Indian adolescents. Social Work Research, 26(2), 101–112.
Lara, M., Gamboa, C., Kahramanian, M. I., Morales, L. S., & Hayes Bautista, D. E. (2005). Acculturation and Latino health in the United States: A review of the literature and its sociopolitical context. Annual Review of Public Health, 26, 367–397.
Leavitt, P. A., Covarrubias, R., Perez, Y. A., & Fryberg, S. A. (2015). “Frozen in time”: The impact of Native American media representations on identity and self‐understanding. Journal of Social Issues, 71(1), 39–53. doi:10.1111/josi.12095.
Lynskey, M., & Hall, W. (2000). The effects of adolescent cannabis use on educational attainment: A review. Addiction, 95(11), 1621–1630. doi:10.1080/09652140020000867.
Maio, R. F., Shope, J. T., Blow, F. C., Copeland, L. A., Gregor, M. A., & Brockmann, L. M., et al. (2000). Adolescent injury in the emergency department: Opportunity for alcohol interventions? Annals of Emergency Medicine, 35(3), 252–257. doi:10.1067/mem.2000.104300.
Markstrom, C. A. (2011). Identity formation of American Indian adolescents: Local, national, and global considerations. Journal of Research on Adolescence, 21(2), 519–535. doi:10.1111/j.1532-7795.2010.00690.x.
Markstrom, C. A., Whitesell, N. R., & Galliher, R. V. (2011). Ethnic identity and mental health among American Indian and Alaska Native adolescents. In M. C. Sarche, P. Spicer, P. Farrell, & H. E. Fitzgerald (Eds.), American Indian and Alaska Native children and mental health: Development, context, prevention, and treatment (pp. 101–131). Denver, CO: Praeger.
Markus, H. R. (2008). Pride, prejudice and ambivalence: Toward a unified theory of race and ethnicity. American Psychologist, 63, 651–670.
Marsiglia, F. F., Kulis, S., & Hecht, M. L. (2001). Ethnic labels and ethnic identity as predictors of drug use among middle school students in the Southwest. Journal of Research on Adolescence, 11(1), 21–48.
Marsiglia, F. F., Kulis, S., Hecht, M. L., & Sills, S. (2004). Ethnicity and ethnic identity as predictors of drug norms and drug use among preadolescents in the US Southwest. Substance Use & Misuse, 39, 1061–1094.
Martin, A. C. (2008). Television media as a potential negative factor in the racial identity development of African American youth. Academic Psychiatry, 32(4), 338–342. doi:10.1176/appi.ap.32.4.338.
McDermott, M. (2015). Color-blind and color-visible identity among American whites. American Behavioral Scientist, 59, 1452-1473. doi:10.1177/002764214566501.
McElroy, A., & Jezewski, M. A. (2000). Cultural variation in the experience of health and illness. In Albrecht, G., Fitzpatrick, R., Scrimshaw, S. C. (Eds). The handbook of social studies in health and medicine (pp. 191-209). Thousand Oaks, CA: Sage Publications.
McKinney, K. D. (2006). “I Really felt white”: Turning points in whiteness through interracial contact. Social Identities, 12(2), 167–185. doi:10.1080/13504630600583361.
Miller-Day, M., & Barnett, J. M. (2004). “I’m not a druggie”: Adolescents’ ethnicity and (erroneous) beliefs about drug use norms. Health Communication, 16(2), 207–228. doi:10.1207/S15327027HC1602_5.
Morris, E. W. (2006). An unexpected minority: White kids in an urban school. New Brunswick, NJ: Rutgers University Press.
Nasim, A., Belgrave, F. Z., Jagers, R. J., Wilson, K. D., & Owens, K. (2007). The moderating effects of culture on peer deviance and alcohol use among high-risk African-American adolescents. Journal of Drug Education, 37(3), 335–363. doi:10.2190/DE.37.3.g.
National Institute on Drug Abuse (2014). Monitoring the future study: Trends in the prevalence of various drugs. http://www.drugabuse.gov/trends-statistics/monitoringfuture/monitoring-future-study-trends-in-prevalence-various-drugs.
Neblett, E. W., Rivas‐Drake, D., & Umaña‐Taylor, A. J. (2012). The promise of racial and ethnic protective factors in promoting ethnic minority youth development. Child Development Perspectives, 6(3), 295–303.
Nguyen, H., & Reuter, P. (2012). How risky is marijuana possession? Considering the role of age, race, and gender. Crime & Delinquency, 58(6), 879–910. doi:10.1177/0011128712461122.
Peck, S. C., Brodish, A. B., Malanchuk, O., Banerjee, M., & Eccles, J. S. (2014). Racial/ethnic socialization and identity development in Black families: The role of parent and youth reports. Developmental Psychology, 50(7), 1897–1909. doi:10.1037/a0036800.
Peterson, R. D., & Hamrick, F. A. (2009). White, male, and “minority”: Racial consciousness among White male undergraduates attending a historically black university. The Journal of Higher Education, 80(1), 34–58. doi:10.1353/jhe.0.0036.
Peterson, P. L., Hawkins, J. D., Abbott, R. D., & Catalano, R. F. (1994). Disentangling the effects of parental drinking, family management, and parental alcohol norms on current drinking by black and white adolescents. Journal of Research on Adolescence, 4(2), 203–227.
Phinney, J. S. (1989). Stages of ethnic identity development in minority group adolescents. Journal of Early Adolescence, 9(1-2), 34–49. doi:10.1177/0272431689091004.
Phinney, J. S. (1990). Ethnic identity in adolescents and adults: Review of research. Psychological Bulletin, 108, 499–514. doi:10.1037/0033-2909.108.3.499.
Phinney, J. S. (1992). The multigroup ethnic identity measure a new scale for use with diverse groups. Journal of Adolescent Research, 7(2), 156–176.
Phinney, J. S. (2000). Ethnic and racial identity: Ethnic identity. In A. E. Kazdin (Ed.), Encyclopedia of psychology (Vol. 3, pp. 254–259). Washington, DC: American Psychological Association. doi:10.1037/10518-122.
Phinney, J., & Chavira, V. (1995). Parental ethnic socialization and adolescent coping with problems related to ethnicity. Journal Research on Adolescent, 5, 31–53.
Phinney, J. S., & Ong, A. D. (2007). Conceptualization and measurement of ethnic identity: Current status and future directions. Journal of Counseling Psychology, 54, 271–281.
Ponterotto, J. G., Gretchen, D., Utsey, S. O., Stracuzzi, T., & Saya, R. (2003). The multigroup ethnic identity measure (MEIM): Psychometric review and further validity testing. Educational and Psychological Measurement, 63(3), 502–515. doi:10.1177/0013164403063003010.
Ponterotto, J., & Park-Taylor, J. (2007). Racial and ethnic identity theory, measurement, and research in counseling psychology: Present status and future directions. Journal of Counseling Psychology, 54(3), 282–294. doi:10.1037/0022-0167.54.3.282.
Prelow, H. M., Bowman, M. A., & Weaver, S. R. (2007). Predictors of psychosocial well-being in urban African American and European American youth: The role of ecological factors. Journal of Youth and Adolescence, 36(4), 543–553.
Quintana, S. M., Aboud, F. E., Chao, R. K., Contreras-Grau, J., Cross, W. E., Hudley, C., Hughes, D., Liben, L. S., Nelson-Le Gall, S., & Vietze, D. L. (2006). Race, ethnicity, and culture in child development: Contemporary research and future directions. Child Development, 77, 1129–1141. doi:10.1111/j.1467-8624.2006.00951.x.
Rivas-Drake, D., Seaton, E. K., Markstrom, C., Quintana, S., Syed, M., & Lee, R. M., et al. (2014). Ethnic and racial identity in adolescence: Implications for psychosocial, academic, and health outcomes. Child Development, 85(1), 40–57. doi:10.1111/cdev.12200.
Roberts, R. E., Phinney, J. S., Masse, L. C., Chen, Y. R., Roberts, C. R., & Romero, A. (1999). The structure of ethnic identity of young adolescents from diverse ethnocultural groups. The Journal of Early Adolescence, 19, 301–322. doi:10.1177/0272431699019003001.
Salas-Wright, C. P., Lee, S., Vaughn, M. G., Jang, Y., & Sanglang, C. C. (2015). Acculturative heterogeneity among Asian/Pacific Islanders in the United States: Associations with DSM mental and substance use disorders. American Journal of Orthopsychiatry, 85(4), 362–370. doi:10.1037/ort0000042.
Savage, J. E., & Mezuk, B. (2014). Psychosocial and contextual determinants of alcohol and drug use disorders in the National Latino and Asian American Study. Drug and Alcohol Dependence, 139, 71–78. doi:10.1016/j.drugalcdep.2014.03.011.
Seffrin, P. (2012). Alcohol use among black and white adolescents: Exploring the influence of interracial friendship, the racial composition of peer groups, and communities. The Sociological Quarterly, 53(4), 610–635. doi:10.1111/j.1533-8525.2012.01244.x.
Sellers, R. M., Copeland‐Linder, N., Martin, P. P., & Lewis, R. H. (2006). Racial identity matters: The relationship between racial discrimination and psychological functioning in African American adolescents. Journal of Research on Adolescence, 16(2), 187–216.
Shepherd, J. P., Sutherland, I., & Newcombe, R. G. (2006). Relations between alcohol, violence and victimization in adolescence. Journal of Adolescence, 29(4), 539–553. doi:10.1016/j.adolescence.2006.06.005.
Smith, T. B., & Silva, L. (2011). Ethnic identity and personal well-being of people of color: A meta-analysis. Journal of Counseling Psychology, 58, 42–60.
Smith, E. P., Walker, K., Fields, L., Brookins, C. C., & Seay, R. C. (1999). Ethnic identity and its relationship to self-esteem, perceived efficacy and prosocial attitudes in early adolescence. Journal of Adolescence, 22(6), 867–880. doi:10.1006/jado.1999.0281.
Su, J., & Supple, A. J. (2016). School substance use norms and racial composition moderate parental and peer influences on adolescent substance use. American Journal of Community Psychology, 57, 280–290. doi:10.1002/ajcp.12043.
Substance Abuse and Mental Health Services Administration [SAMHSA]. (2013). Results from the 2012 National Survey on Drug Use and Health: Summary of National Findings. NSDUH Series H-46, HHS Publication No. (SMA) 13-4795. Rockville, MD: Substance Abuse and Mental Health Services Administration.
Substance Abuse and Mental Health Services Administration [SAMHSA], Center for Behavioral Health Statistics and Quality. (2014). The TEDS Report: Age of Substance Use Initiation among Treatment Admissions Aged 18 to 30. Rockville, MD: Substance Abuse and Mental Health Services Administration. Retrieved from http://www.samhsa.gov/data/sites/default/files/WebFiles_TEDS_SR142_AgeatInit_07-10-14/TEDS-SR142-AgeatInit-2014.pdf
Szapocznik, J., Prado, G., Burlew, A. K., Williams, R. A., & Santisteban, D. A. (2007). Drug abuse in African American and Hispanic adolescents: Culture, development, and behavior. Annual Review of Clinical Psychology, 3, 77–105.
Swaim, R. C., Stanley, L. R., & Beauvais, F. (2013). The normative environment for substance use among American Indian students and white students attending schools on or near reservations. American Journal of Orthopsychiatry, 83(2-3), 422.
Thai, N. D., Connell, C. M., & Tebes, J. K. (2010). Substance use among Asian American adolescents: Influence of race, ethnicity, and acculturation in the context of key risk and protective factors. Asian American Journal of Psychology, 1(4), 261–274. doi:10.1037/a0021703.
Torkelson, J., & Hartmann, D. (2010). White ethnicity in twenty-first-century America: Findings from a new national survey. Ethnic and Racial Studies, 33(8), 1310–1331.
Townsend, T. G., & Belgrave, F. Z. (2000). The impact of personal identity and racial identity on drug attitudes and use among African American children. Journal of Black Psychology, 26(4), 421–436. doi:10.1177/0095798400026004005.
Umaña-Taylor, A. J. (2004). Ethnic identity and self-esteem: Examining the role of social context. Journal of Adolescence, 27(2), 139–146.
Umaña‐Taylor, A. J., Quintana, S. M., Lee, R. M., Cross, W. E., Rivas‐Drake, D., & Schwartz, S. J., et al. (2014). Ethnic and racial identity during adolescence and into young adulthood: An integrated conceptualization. Child Development, 85(1), 21–39. doi:10.1111/cdev.12196.
Unger, J. B. (2011). Cultural identity and public health. In S. J. Schwartz, K. Luyckx, V. L. Vignoles, S. J. Schwartz, K. Luyckx, V. L. Vignoles (Eds.), Handbook of identity theory and research (vols. 1 and 2) (pp. 811–825). New York, NY: Springer Science + Business Media. doi:10.1007/978-1-4419-7988-9_34.
Unger, J. B., Ritt-Olson, A., Teran, L., Huang, T., Hoffman, B. R., & Palmer, P. (2002). Cultural values and substance use in a multiethnic sample of California adolescents. Addiction Research & Theory, 10(3), 257–279. doi:10.1080/16066350211869.
Unger, J. B., Shakib, S., Gallaher, P., & Ritt-Olson, A. (2006). Cultural/interpersonal values and smoking in an ethnically diverse sample of Southern California adolescents. Journal of Cultural Diversity, 13(1), 55–63.
Volkow, N. D., Baler, R. D., Compton, W. M., & Weiss, S. R. (2014). Adverse health effects of marijuana use. New England Journal of Medicine, 370(23), 2219–2227. doi:10.1056/NEJMra1402309.
Wallace, J. J., Yamaguchi, R., Bachman, J. G., O’Malley, P. M., Schulenberg, J. E., & Johnston, L. D. (2007). Religiosity and adolescent substance use: The role of individual and contextual influences. Social Problems, 54(2), 308–327. doi:10.1525/sp.2007.54.2.308.
Wallace, J. M., Bachman, J. G., O’Malley, P. M., Schulenberg, J. E., Cooper, S. M., & Johnston, L. D. (2003). Gender and ethnic differences in smoking, drinking, and illicit drug use among American 8th, 10th, and 12th grade students, 1976-2000. Addiction, 98, 225–234. doi:10.1046/j.1360-0443.2003.00282.x.
Wallace, S. A., & Fisher, C. B. (2007). Substance use attitudes among urban black adolescents: The role of parent, peer, and cultural factors. Journal of Youth and Adolescence, 36(4), 441–451.
White, H. R., Tice, P. C., Loeber, R., & Stouthamer-Loeber, M. (2002). Illegal acts committed by adolescents under the influence of alcohol and drugs. Journal of Research in Crime and Delinquency, 39(2), 131–152. doi:10.1177/002242780203900201.
Whitesell, N. R., Asdigian, N. L., Kaufman, C. E., Crow, C. B., Shangreau, C., & Keane, E. M., et al. (2014). Trajectories of substance use among young American Indian adolescents: Patterns and predictors. Journal of Youth and Adolescence, 43(3), 437–453.
Williams, E. C., Gupta, S., Rubinsky, A. D., Jones‐Webb, R., Bensley, K. M., & Young, J. P., et al. (2016). Racial/ethnic differences in the prevalence of clinically recognized alcohol use disorders among patients from the U.S. Veterans Health Administration. Alcoholism: Clinical And Experimental Research, 40(2), 359–366. doi:10.1111/acer.12950.
Witbrodt, J., Mulia, N., Zemore, S. E., & Kerr, W. C. (2014). Racial/ethnic disparities in alcohol‐related problems: Differences by gender and level of heavy drinking. Alcoholism: Clinical and Experimental Research, 38(6), 1662–1670.
Wright, E. M., Fagan, A. A., & Pinchevsky, G. M. (2016). Penny for your thoughts? The protective effect of youths’ attitudes against drug use in high-risk communities. Youth Violence And Juvenile Justice, 14(2), 110–129. doi:10.1177/1541204014562074.
Wu, L. T., Swartz, M. S., Brady, K. T., Hoyle, R. H., & Workgroup, N. A. (2015). Perceived cannabis use norms and cannabis use among adolescents in the United States. Journal of Psychiatric Research, 64, 79–87. doi:10.1016/j.jpsychires.2015.02.022.
Wu, L. T., Woody, G. E., Yang, C., Pan, J. J., & Blazer, D. G. (2011). Racial/ethnic variations in substance-related disorders among adolescents in the United States. Archives of General Psychiatry, 68(11), 1176–1185. doi:10.1001/archgenpsychiatry.2011.120.
Yip, T., Seaton, E. K., & Sellers, R. M. (2006). African American racial identity across the lifespan: Identity status, identity content, and depressive symptoms. Child Development, 77, 1504–1517. doi:10.1111/j.1467-8624.2006.00950.x.
Yu, M., & Stiffman, A. R. (2007). Culture and environment as predictors of alcohol abuse/dependence symptoms in American Indian youths. Addictive Behaviors, 32(10), 2253–2259. doi:10.1016/j.addbeh.2007.01.008.
Zapolski, T. C. B., Pedersen, S. L., McCarthy, D. M., & Smith, G. T. (2014). Less drinking, yet more problems: Understanding African American drinking and related problems. Psychological Bulletin, 140(1), 188–223. doi:10.1037/a0032113.
Zickler, P. (1999). Ethnic identification and cultural ties may help prevent drug use. NIDA Notes, 14(3), 7–9. http://archives.drugabuse.gov/NIDA_Notes/NNVol14N3/Ethnic.html.
Funding
This research was supported by NIH award KL2TR001106 to A. Shekhar and Tamika Zapolski and by NIH award DA05312 to Sycarah Fisher. Writing of the manuscript was supported by NIH/NIDA award R25DA035163 to Tamika Zapolski.
Authors’ Contributions
The contribution of each author is as follows: TZ conceived of the study, participated in its design, conducted statistical analysis, interpretation of data, drafting of the manuscript, and coordinated writing components for co-authors; SF participated in the study design, and contributed to drafting of the manuscript and editing; DB contributed to drafting the manuscript and editing; DH participated in the study design, conducted primary statistical analyses, drafting of the manuscript, and editing; JB participated in the design and coordination of the parent study, worked with community partners to develop the measurement plan, conducted data collection and processing, and participated in manuscript editing. All authors have given final approval of the version to be published.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Compliance with Ethical Standards
The authors do not have any interests or activities that might be interpreted as influencing the research submitted, and this study was conducted in accordance with APA ethical standards. This research has not been presented at a conference and is not under consideration for publication with any other journals.
Ethical Approval
Data collected for this study has been approved by the Institutional Review Board/ethnics committee at Michigan State University and the research has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Informed Consent
All participants in the study provided informed assent, with informed consent provided by their legal guardian.
Conflict of Interest
The authors declare that they have no competing interests.
Rights and permissions
About this article

Cite this article
Zapolski, T.C.B., Fisher, S., Banks, D.E. et al. Examining the Protective Effect of Ethnic Identity on Drug Attitudes and Use Among a Diverse Youth Population. J Youth Adolescence 46, 1702–1715 (2017). https://doi.org/10.1007/s10964-016-0605-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-016-0605-0