
Abstract
Can the religious values of an entire geographic area affect the BMI of people living in that same area, even people with different religious values? Although prior research has demonstrated that individual religious characteristics are associated with individual BMI, less is known about how the overall religious context influences BMI. Using multilevel analyses on two waves of the National Study of Youth and Religion merged with county-level variables, this study finds that a county’s higher Catholic population share is associated with lower individual BMI even after controlling for various individual and county-level variables. Surprisingly, this Catholic contextual effect on BMI applies to almost everyone living in a predominantly Catholic county regardless of individual Catholic identity and residential movement across counties. In contrast, county-level conservative Protestant population share is linked with higher BMI. However, this conservative Protestant contextual effect is explained by county-level socioeconomic variables.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
As of 2015, no American state had a prevalence of obesity less than 20% and some states, such as Mississippi and West Virginia, had an obesity prevalence of 35% or greater (Centers for Disease Control and Prevention 2015). These numbers represent a sharp rise when compared to the 11% obesity rate nationwide back in the early 1960s. Worse still, the observed trend is expected to continue as social scientists forecast that by 2030, half of the US adult population will be obese (CDC 2015). Experts note that the prevalence of obesity is attributed to health problems, such as diabetes, heart disease, mortality, and reduced physical function (Ayers et al. 2010).
Considering the onset of a potential public health crisis, social scientists have examined how a major social institution, such as religion, may either facilitate or inhibit the growth of obesity. A focus to study the impact of religious effects on obesity or BMI is needed when one considers that religion is not only a personal matter, such as how one perceives God or interprets religious scriptures, but can also be treated as a dynamic social institution that undeniably produces social forces mobilizing people and powerfully reshapes individual and community outcomes. For instance, followers from different religions hold divergent values on a variety of issues, such as education (e.g., Stroope et al. 2015), marriage (e.g., Hout et al. 2001), and community investment (Beyerlein and Hipp 2005). When a religion’s followers account for a large share of local population, its followers are likely to come into contact with local residents from other religions and eventually transmit their cultural values to the general population of the entire area. Prior studies have suggested that this value transfer might lead to variations in notable outcomes, such as suicide rates (Durkheim 1897) and economic development (Weber 1930), between regions dominated by different religions.
In line with this, the civic community theory makes more specific remarks on how religion may function as a sociocultural force influencing a broad range of individual and social outcomes. The theory argues that more civically engaged religious groups, such as Catholics, tend to believe that a better solution to social ills is social investment and collaborations across group boundaries (Beyerlein and Hipp 2005; Putnam 2000). As a result, individuals in areas with a large presence of those civically engaged religious groups tend to invest more in infrastructure and focus more on the well-being of the whole community. Such cultural emphasis on social activism and this-worldly interest can lead to the creation of a better socioeconomic environment in areas with a large presence of civically engaged religious groups and consequently better health outcomes including lower mortality rates (Blanchard et al. 2008).
In contrast, more conservative religious groups, such as the conservative Protestants, tend to believe that social ills are primarily the result of personal moral failures and warrant corrective measures such as religious redemptions rather than social and secular interventions. Thus, areas with a large presence of conservative Protestants place less emphasis on investment in social infrastructures, thereby leading themselves to a less desirable socioeconomic environment. As a result, communities with a large presence of conservative Protestants and their other-worldly values tend to fare worse on important health outcomes such as mortality rates (Blanchard et al. 2008).
One of the primary interests of this study is to determine the manner in which the religious civic community will influence its BMI. In other words, will the religious civic community influence BMI just like prior studies have found for other health outcomes? Or, will religion mainly affect one’s BMI through individual rather than contextual-level religious characteristics? Unfortunately, with focus on individual-level religious characteristics, most prior research fails to help us answer these questions. Instead, this study has chosen a methodology based on data from wave 3 and wave 4 of the National Study of Youth and Religion (NSYR) merged with county-level variables from the U.S. Census 2000 and the Religious Congregations and Membership Study (RCMS) 2000 to address the unanswered questions. By so doing, this study intends to contribute to a renewed, multilevel understanding of the relationship between religion and BMI.
Literature Review
In a study of this nature, a good starting point is the question: What socio-demographic factors predict body mass index, BMI? In social science research, great efforts have been made to better answer this question. Some prior studies suggest that BMI is associated with health behaviors, such as drinking and smoking (e.g., Kim et al. 2003); socioeconomic status, such as education and income (BeLue et al. 2009); race and ethnicity (e.g., Cossrow and Falkner 2004); residential location, such as living in the South (CDC 2015); and the bodyweights of one’s close social ties (e.g., Christakis and Fowler 2007).
When it comes to the sociology of religion, prior research has also found some interesting connections between individual religious characteristics and BMI. In a nationally representative sample of US adults, Ferraro (1998) points out that dedicated religious practices such as active church participation, reading religious books, and being exposed to religious media bear a positive relationship with obesity and a negative one with being thin. The author suggests that instead of functioning as a public health venue promoting a healthy diet among the congregants, many American religious institutions support and promote the social tolerance of people who are overweight or obese. Meanwhile, these same institutions pay more institutional attention and effort to the deviancy of substance use, such as alcohol and tobacco, rather than gluttony. This phenomenon, according to the author, may potentially increase the chance of becoming overweight or obese among the religiously active (Ferraro 1998).
According to Kim et al. (2003), religious practice is no longer a robust predictor of BMI once individual health behaviors, such as drinking and smoking, are considered. Although the Kim study may have challenged Ferraro’s findings, to some extent, this mediating effect of substance use on religious practice and BMI may also confirm what Ferraro speculates—an overemphasis on preventing substance abuse combined with a consequent lack of effort in reinforcing healthy eating habits that may contribute to heavier body weight among the religious. Kim et al.’s finding is later confirmed by a large-scale study of US adults. The study indicates that after considering individual health behavior and socioeconomic status, regular attendance at religious services is no longer significantly related to one’s weight status (Gillum 2006).
Besides individual religiosity, individual religious affiliation has also been found to be an important and reliable predictor of BMI. Kim et al. (2003) show that, although the individual religiosity effect on BMI may be explained by health behaviors, the denominational effect on BMI remains robust: conservative Protestant men have a significantly higher BMI compared to men with no religion. Using a more sophisticated evaluation of the Protestant denomination, Cline and Ferraro (2006) find that, in the case of women, affiliation with the Baptist denomination is associated with higher BMI. Significant denominational variations in BMI have also been found in Australia where, in general, a Christian affiliation is tied to a higher BMI (Kortt and Dollery 2014) and in England where men with a Christian or Sikh affiliation have a higher BMI than men without a religious affiliation (Lycett 2015).
Despite these interesting findings, our knowledge of the interaction between religion and BMI at the macro-level remains limited to bivariate associations (e.g., Ferraro 1998). Still, some interesting religion-based questions regarding effects on BMI can be raised. Two such questions are: (1) What happens to an individual’s BMI when a person lives in an area with a large religious following that is known to be linked with a higher BMI? (2) When it comes to BMI, will a religious denomination’s BMI characteristics influence nonmembers who happen to share the same geographic space?
To better understand how contextual-level religion may influence important individual and social outcomes, consider the civic community theory. The theory suggests that religion is a group property whose influence is diffusive, that is, it affects the entire community. Specifically, the civic community theory argues that when a community has a prevalence of religious values emphasizing saving the world through active social investment and community collaborations, such a community may produce a social environment that features more positive individual and social outcomes (Beyerlein and Hipp 2005), such as lower mortality rates (Blanchard et al. 2008) and lower crime rates (Ulmer and Harris 2013). Prior research has shown that Catholics tend to embrace so-called civically engaging values. For example, in his encyclical, Pope John Paul II has argued that it is important for Catholics to resolve social ills through active social interventions and more equitable economic development (Pope John Paul II 1988). When an area has a large presence of Catholics with a high regard for civic values, one may expect that such an area tends to invest more on its infrastructures and the well-being of its residents. As a result, people living in that community may benefit from its more enabling social environment.
Based on the civic community theory and prior research, it might be possible that when an area has a significant presence of Catholics with their strong civic values, that area may develop a more desirable social environment, thereby leading to lower BMIs for all residents living in that area. Therefore, this study hypothesizes that:
H1
There is a negative relationship between county-level Catholic population share and individual BMI
In contrast, when a community is suffused with religious values that define many social problems as personal, moral issues, such a community may turn to personal religious redemptions rather than social, secular remedies for solutions. Consequently, such a community may invest less in its social infrastructure as social problems are perceived to be the result of personal moral crises rather than a shortage of resources and enabling factors within the community. One religious denomination whose behavior resembles such a scenario is that of the conservative Protestants. Their religious teachings and values tend to direct one to fervent religious devotions and to other-worldly pursuits (Beyerlein and Hipp 2005). When a community has a prevalence of such cultural and religious values, one may expect less investment being made to improve the community and a resulting social environment which oftentimes is linked with undesirable outcomes, such as higher mortality rates (Blanchard et al. 2008) and higher violent crime rates (Desmond et al. 2010).
Thus, based on civic community theory, it might be possible that when an area has a significant presence of conservative Protestants with their inherent cultural values, that area may develop a less desirable social environment which leads to higher BMIs for its residents. Therefore, this study hypothesizes that:
H2
There is a positive relationship between county-level conservative Protestant population share and individual BMI.
By using nationally representative panel data (NSYR) merged with county-level data from the U.S. census and the Religious Congregational Membership Survey (RCMS), this study will be able to better assess whether individual-level or contextual-level religious composition accounts for the simple associations that have sometimes been found between religious variables and BMI.
Methods
The data in this study come from three sources, namely wave 3 (2008) and wave 4 (2012) of the National Study of Youth and Religion (NSYR), the U.S. Census 2000, and the Religious Congregations and Memberships Study (RCMS) 2000. The NSYR is a nationally representative telephone survey of 3290 youth whose major purpose is to explore the religious and spiritual life of America’s youth as well as their political, social, and cultural attitudes as they transition from adolescence into adulthood (Smith 2008; Smith and Pearce 2003, 2005).
The NSYR panel data feature a multi-wave arrangement. Wave 1 of the NSYR was conducted in 2003, when the respondents were aged 13–17. For each teen respondent, a parent was also interviewed concerning the family environment in which the teen respondent grew up. Wave 2 of the NSYR was conducted in 2005 when the respondents were aged 16–20. The NSYR also has wave 3 (2008) and wave 4 (2012) survey data which capture the respondents’ life during formal adulthood. Because body mass index (BMI) data are only available in the wave 3 and wave 4 subsets of the NSYR data, this study will use these two wave sets for analyses.
Although the NSYR data provide a great deal of religious and delinquency measures which serve the purposes of this study, it originally did not contain any contextual-level data. With permission from the principal investigators of the NSYR, the NSYR data were merged with the county-level U.S. Census 2000 data and the county-level data in the Religious Congregations and Membership Study (RCMS) 2000 so that a multilevel approach for using the NSYR data is now possible.
The RCMS 2000 contains data on the number of congregations and adherents (official members with or without children in a given denomination) for participating religious groups in each county of the USA (Grammich et al. 2012). The RCMS contains data on most denominations, especially the larger denominations, and thus, the RCMS data include most, but not all, religious adherents in each county. From the RCMS data, one can calculate a variety of important religious contextual measures, such as rates of adherence per 1000 population in a county for all denominations combined, for each specific denomination considered separately, and for each of several groupings of similar denominations as described below.
Measurements
Focal Dependent and Independent Variables
The dependent variable used in the study is body mass index (BMI) whose values are available in wave 3 and wave 4 of the NSYR. The mean BMI in wave 3 is 24.74 which, according to the BMI categories of the National Institute of Health, is interpreted as close to being overweight (BMI ≥ 25). The mean BMI in wave 4 is 26.79, a value which falls into the overweight category. Due to the positive skewness of the BMI scores in both waves, the BMI scores are log transformed in both waves; this operation reduces skewness significantly.
The key independent variables selected in the study are the log-transformed adherence rate of religious denominations per 1000 population of a county calculated from the RCMS 2000 data for the counties in which each NSYR respondent lives. The classification of denominations was done in ways that parallel the classification technique used in the popular Steensland et al. (2000) classification of denomination in the US General Social Survey. Although in the early analyses all kinds of denominational population share were analyzed, only the conservative Protestant and Catholic population share variables have been selected due to their statistically significant main relationships with the BMI-dependent variable. Thus, in the analyses that follow, the study will focus only on these two key independent variables. Because these population share variables have substantial positive skewness, the natural logs of the conservative Protestant and Catholic population share variables will be taken for all analyses.
Control Variables
This study controls for a variety of variables which, as prior research suggests, may influence BMI. These control variables can be broadly categorized into individual-level controls and county-level controls. The individual-level controls capture the religious and demographic profiles of the youth, while the county-level controls are mostly enlightened by prior research which suggests that some contextual-level socioeconomic characteristics may deeply impact individual conformity and deviance (e.g., Leventhal et al. 2009). Table 1 provides a brief summary of the number of cases, mean, standard deviation, and minimum and maximum value for each control variable. In addition, the principal component analysis (PCA) was conducted to reduce the number of control variables which resulted in one principal component on personal religiosity, one principal component on substance use, and three principal components on county-level socioeconomic environment. Table 2 presents the details of PCA analyses including item loadings, eigenvalues, and proportion variance for each principal component.
Plan of Analysis
The respondents in the survey data are clustered in counties, a feature that requires the adoption of mixed-effect modeling. This approach allows lower level parameters to randomly vary across higher level units. In particular, this study uses a three-level multilevel modeling approach, a form of mixed-effect modeling that clusters the time (age) effect within each individual respondent, and the individual effect within the same county. Equations used at each level of the three-level model are provided. To simplify the process of data presentation and its interpretation, only one variable from each level is included in the equations below: one variable at level 1 (time), age \(a_{1ij}\), one variable at level 2 (individual), individual Catholic identity \(X_{01j} ,\) and one variable at level 3 (county), the Catholic population share \(W_{001}\) to predict the outcome variable BMI \(y_{tij}\).
Combined equation:
Level 1 (time) equation:
Level 2 (individual) equation:
Level 3 (county) equation:
where \(y_{tij}\) is BMI of ith individual in jth county at age t and the intercept of grand mean BMI \(\varUpsilon_{000}\) now represents a mean BMI level differs across each individual and each county. After this operation, the variances and residual then become level specific, with \(e_{tij}\) being the variance within individual, \(r_{0ij}\) being the variance between individuals, and \(\mu_{00j}\) being the variance between counties.
All data preparation and model analyses are conducted in Stata 15. Before performing the main analyses, multiple imputation is conducted to handle the missing data by creating five additional samples for a completed dataset based on the chained multiple imputation method. The latter is preferred whenever large samples have missing values across several variables of different types (Azur et al. 2011). The so-called mi estimate applies the combination rules to analyze the imputed full samples in all subsequent models that would be otherwise biased due to sample inflation. This method allows the estimation of parameters as the average of coefficients from the imputed datasets and calculates standard errors based on the degree to which the coefficient estimates vary across the imputations.
Results
Table 1 presents the descriptive statistics of the variables. These include the number of individuals, mean, standard deviation, and the range of the response categories. The mean age in wave 3 is 20.02, and it increases to 25.47 in wave 4. Using values presented in the BMI categories of the National Institute of Health, 13.91% of the respondents in the study were found to be obese (BMI ≥ 30) in wave 3. In wave 4, this figure rises to 25.15%. Meanwhile, the share of respondents who are classified as having “normal weight” drops from 57.07% to 45.09% between the two waves.
Table 3 contains the multilevel analytical results of the Catholic population share on BMI using four models. A brief summary of the results from each model is presented. Model 1, the null model, shows that level 1 ICC has a value of 39%, meaning that 39% of the variance in BMI is the result of intra-individual changes over time, while the remaining 61% is due to the variance between individuals. As is in all other models, the ICC value at the county level is too small to be even rounded to the second decimal. This outcome is due to the nature of the survey where the number of counties is often greater than the number of individuals as individuals may move across counties between waves.
Model 2 in Table 3 includes the log-transformed Catholic population share per 1000 county residents. The result shows that the Catholic population share bears a negative and statistically significant relationship with BMI (p < 0.001). In other words, when a county has a higher adherence rate of residents belonging to the Catholic denomination, a young adult living there is more likely to have a lower BMI. Model 3 includes the values of variables dealing with “between individual variation.” The results show that even when all three individual-level categories are considered, Catholic population share remains statistically significant. Surprisingly, the individual-level religious identity variables are statistically insignificant, an outcome that may run contrary to prior research. In fact, it might suggest that in past studies what appeared to be an individual-level effect of religious identity was really a contextual-level effect of living in a subculture associated with a particular religious influence.
As for other individual-level control variables, higher individual religiosity, more substance usage, being female, white, having higher educational attainment, and coming from higher income families, are associated with a lower BMI. In contrast, variables like being married, older, and having moved across counties between waves are related to a higher BMI. Based on these findings, one can raise the question: Can county-level variables mediate the effect of Catholic population share on BMI? To answer the question, consider that when county-level socioeconomic variables are included in model 4, the relationship between Catholic population share and BMI remains robust. That is, a higher Catholic population share in a county is associated with a lower BMI for young adults living there. Therefore, hypothesis 1 is supported.
However, one can also ask: Is this Catholic contextual effect on BMI only applicable to Catholics living in a predominantly Catholic county? In addition, what would happen to people who moved across counties between survey waves? Does the Catholic contextual effect on BMI only apply to residents who had always lived in a predominantly Catholic county between survey waves? To answer these questions, two cross-level interactions were created and analyzed: one is a cross-level interaction between Catholic population share and individual Catholic identity and the other is a cross-level interaction between Catholic population share and inter-county residential change. Neither of these cross-level interactions are statistically significant in the full model, meaning that the Catholic contextual effect on BMI applies to almost all county residents regardless of one’s (non-) Catholic identity or inter-county residential changes between waves. To save space, results of the cross-level interaction analyses are not included in this document but are available upon request.
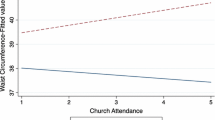
The models in Table 3 show that the Catholic population share has a relationship with BMI that is statistically significant. But how large is this effect? Given that the Catholic population share has been transformed by taking the natural log, the regression coefficient is hard to interpret in any intuitive way. Thus, this study calculates how many centiles the predicted value of the dependent variable (\(\hat{y}\)) has changed when the independent variable, Catholic population share, changes from its 10th percentile to the 90th percentile. If the log-based Catholic population share in a county changes from 3.41 (the 10th percentile) to 5.99 (the 90th percentile) and all other variables are kept at their mean values, a young adult’s BMI value is shown to decrease from 3.24 (the 56th percentile of the distribution of the predicted values of BMI) to 3.21 (the 46th percentile)—a 10 percentile decrease. A visual illustration of this behavior is presented in Fig. 1.

Predicted changes in BMI by changes in Catholic population share
Table 4 presents the multilevel analytical results of the conservative Protestant population share on BMI. Four models having the same order and format as shown in Table 3 analysis are used. Model 1 in Table 4 is the null model whose interpretations are the same as those for mode l in Table 3. Model 2 only includes the county-level conservative Protestant population share. The results indicate a phenomenon that is opposite to that found for Catholics, that is, a higher adherence rate of conservative Protestants in a county leads to a higher BMI (p < 0.001).
Model 3 incorporates individual-level demographic variables and religious characteristics. The inclusion of individual-level controls almost explains the conservative Protestant contextual effect on BMI. Similar to the Catholic context, in model 3, some demographic characteristics, such as gender, race, age, parent income, education, and inter-county residential change, are significantly related to BMI. Also similar to model 3 in Table 3, individual religious identity cannot be used to predict BMI. County-level controls are included in model 4 considering the potential mediating effects of county-level census variables. The results suggest a mediating effect of county-level characteristics on the conservative Protestant population share–BMI connection: when county-level socioeconomic variables are controlled, conservative Protestant population share becomes insignificant. Therefore, hypothesis 2 is rejected.
Conclusions and Discussion
In this study, individual-level data are merged with the national census and county-level religious membership data to explore the relationship between religious context and BMI of the young adults. This is one of the few studies that have ever used a multilevel analytical approach to look into the relationship between religion and BMI. The findings in this study reveal that county-level conservative Protestant population share has a statistically significant main effect on individual BMI: one tends to develop higher BMI when living in a predominantly conservative Protestant county. However, such a conservative Protestant contextual effect on BMI is explained by county-level socioeconomic characteristics. This phenomenon echoes one of the key arguments in the civic community theory—the conservative Protestant other-worldly cultural orientation is tied to less developed socioeconomic conditions which might translate into undesirable individual and social outcomes in areas with a large presence of conservative Protestants (Beyerlein and Hipp 2005; Blanchard et al. 2008; Desmond et al. 2010).
In contrast to the BMI-increasing effect from a higher county-level conservative Protestant population share, when a county has a higher share of its residents affiliated with Catholicism, young adults living in that county, regardless of religious identity and residential change status, tend to develop a lower BMI. This phenomenon is, to some extent, consistent with what Durkheim (1897) and Weber (1930) have argued in their classic works: religion is more than a set of individual theological beliefs and practices limited to the followers of some religion. Rather, it is a social phenomenon that carries with it values and norms that may broadly affect people in the general society.
This robust Catholic contextual effect on BMI breathes some fresh air into prior studies which predominantly cite deleterious religious effects that contribute to higher BMI or more prevalent obesity (e.g., Cline and Ferraro 2006; Ferraro 1998; Kortt and Dollery 2014). In addition, the multilevel analyses employed in this study serve to highlight an important fallacy that prior research was unable to address. For instance, Ferraro (1998) finds that states with a higher percentage of Baptists are more likely to have a higher rate of obesity. Without knowing the relationship between individual-level BMI and religious affiliation, one might be tempted to erroneously conclude that Baptism is associated with higher obesity rates. However, it is possible that the positive correlation between state-level Baptist population share and obesity rate is in fact due to the higher obesity rates among residents who are not Baptists but happen to live in a more Baptist-populated state. Thus, by using multilevel analyses and controlling for variables at both the individual and contextual levels, this study is able to rule out possible ecological fallacies (Morgenstern 1995, 2008) and enrich our knowledge of interconnections between socially relevant issues like religion and BMI.
What may explain the Catholic contextual effect on BMI? A closer look at model 4 in Table 3 reveals that when county-level socioeconomic variables are controlled, Catholic population share becomes less statistically significant than in prior models. Thus, it might be possible that some uncontrolled variable(s) at the county level could further explain the Catholic contextual effect on BMI. Perhaps, in line with the civic community theory noted above, the civically engaged cultural perspective from the Catholic denomination may lead to more investment in public health infrastructure, such as higher public health resources per capita—variables that are not directly available in the data but may in fact contribute to lower BMI for residents in an area. A brief look into this possible scenario by controlling workforce employed in professional fields and median household income measures that might indicate county-level conditions of public health resources fail to explain the robust Catholic contextual effect. Considering the somewhat limited scope of the available data, the findings of the study showing a robust effect of Catholic context on BMI remain an interesting puzzle and call for future research.
Another limitation of the study is worthwhile noting. The NSYR data only cover adolescents and young adults. It does not include individuals from other age groups, especially senior citizens whose long-held religious experience and physical conditions may be dramatically different from those of the young adults. If availability of these data can be found, it is proposed that future research be initiated with a focus into how religious context might influence BMI and other important health outcomes of people in the different age groups.
Despite the limitations cited, this study serves as one of the pioneering studies that feature a multilevel approach to explore the relationship between religious context, an often neglected yet important aspect of religion, and BMI, a hotly debated public health issue. The key findings of the study suggest that the sociological aspects of religion should be more than simply studying the implications of individual religiosity, such as how one worships the higher power or reads the scriptures. Rather, it should also look into the ways in which religious cultural values impact the functions of a community and how the impact might eventually affect important life outcomes of residents within the broader community. The study also underscores the importance of looking into variations between different kinds of religious context. Because prior research dealing with religious context tends to conceptualize religious context as aggregated religiosity, such as mean church attendance rates of a geographic unit, it neglects the cultural and value variations between geographic units dominated by different kinds of religious tradition (e.g., Bahr and Hoffman 2008).
In summary, using advanced statistics on classic sociological thoughts, this study strives to avoid some of the shortcomings of prior research and seeks to contribute to this understudied, yet important, subfield in the sociology of religion and health.
References
Ayers, J., Irvin, V., Park, H., Hovell, M., Hofstetter, C., Song, Y., et al. (2010). Can religion help prevent obesity? Religious messages and prevalence of being overweight or obese among Korean women in California. Journal for the Scientific Study of Religion, 49, 536–549.
Azur, M., Stuart, E., Frangakis, C., & Leaf, P. (2011). Multiple imputation by chained equations: What is it and how does it work? International Journal of Methods in Psychiatric Research, 20, 40–49.
Bahr, S. J., & Hoffmann, J. P. (2008). Religiosity, peers, and adolescent drug use. Journal of Drug Issues, 8(3), 743–770.
BeLue, R., Francis, L., Rollins, B., & Colaco, B. (2009). One size does not fit all: Identifying risk profiles for overweight in adolescent population subsets. Journal for Adolescent Health, 45, 517–524.
Beyerlein, K., & Hipp, J. (2005). Social capital, too much of a good thing? American religious traditions and community crime. Social Forces, 84, 995–1013.
Blanchard, T., Bartkowski, J., Matthews, T., & Kerley, K. (2008). Faith, morality and mortality: The ecological impact of religion on population health. Social Forces, 86, 1591–1620.
Centers for Disease Control and Prevention. (2015). Prevalence of obesity among adults and youth: United States, 2011–2014. Retrieved 15 January, 2018, from https://www.cdc.gov/obesity/data/adult.html.
Christakis, N., & Fowler, J. (2007). The spread of obesity in a large social network over 32 years. The New England Journal of Medicine, 357, 370–379.
Cline, K., & Ferraro, K. (2006). Does religion increase the prevalence and incidence of obesity in adulthood? Journal for the Scientific Study of Religion, 45, 269–281.
Cossrow, N., & Falkner, B. (2004). Race/ethnic issues in obesity and obesity-related comorbidities. Journal of Clinical Endocrinology and Metabolism, 89, 2590–2594.
Desmond, S., Kikuchi, G., & Morgan, K. (2010). Congregations and crime: Is the spatial distribution of congregations associated with neighborhood crime rates? Journal for the Scientific Study of Religion, 49, 37–55.
Durkheim, E. (1897). Suicide: A study in sociology. New York: The Free Press.
Ferraro, K. (1998). Firm believers? Religion, body weight, and well-being. Review of Religious Research, 39, 224–244.
Gillum, R. (2006). Frequency of attendance at religious services, overweight, and obesity in American men and women: The third National Health and Nutrition Examination Survey. Annals of Epidemiology, 16, 655–660.
Grammich, C., Hadaway, K., Houseal, R., Jones, D., Krindatch, A., Stanley, R., & Taylor, R. (2012). 2010 U.S. religion census: Religious congregations and membership study. Retrieved 15 January, 2018, from http://www.thearda.com/Archive/Files/Descriptions/RCMSCY10.asp.
Hout, M., Greeley, A., & Wilde, M. J. (2001). The demographic imperative in religious change in the United States. The American Journal of Sociology, 107, 468–500.
John Paul II, Pope. (1988). Encyclical Letter Sollicitudo Rei Socialis of the Supreme Pontiff, John Paul II, to the Bishops, Priests, Religious Families, Sons and Daughters of the Church and All People of Good Will for the Twentieth Anniversary of Populorum Progressio. Washington, D.C.: Office of Publishing and Promotion Services, United States Catholic Conference.
Kim, K., Sobal, J., & Wethington, E. (2003). Religion and body weight. International Journal of Obesity, 27, 469–477.
Kortt, M., & Dollery, B. (2014). Religion and BMI in Australia. Journal of Religion and Health, 53, 217–228.
Leventhal, T., Dupéré, V., & Brooks-Gunn, J. (2009). Neighborhood influences on adolescent development. In R. Lerner & L. Steinberg (Eds.), Handbook of adolescent psychology (3rd ed., pp. 411–443). Hoboken, NJ: Wiley.
Lycett, D. (2015). The association of religious affiliation and body mass index (BMI): An analysis from the health survey for England. Journal of Religion and Health, 54, 2249–2267.
Morgenstern, H. (1995). Ecologic studies in epidemiology: Concepts, principles, and methods. Annual Review of Public Health, 16, 61–81.
Morgenstern, H. (2008). Ecological studies. In K. J. Rothman, T. L. Lash, & S. Greenland (Eds.), Modern epidemiology (pp. 511–531). Philadelphia, PA: Lippincott Williams and Wilkins.
Putnam, R. D. (2000). Bowling alone: The collapse and revival of American community. New York: Simon & Schuster.
Smith, C. (2008). The national study of youth and religion wave 3. Retrieved 15 January, 2018, from http://www.thearda.com/Archive/NSYR.asp.
Smith, C., & Pearce, L. (2003). The national study of youth and religion wave 1. Retrieved 15 January, 2018, from http://www.thearda.com/Archive/NSYR.asp.
Smith, C., & Pearce, L. (2005). The national study of youth and religion wave 2. Retrieved 15 January, 2018, from http://www.thearda.com/Archive/NSYR.asp.
Steensland, B., Robinson, L., Wilcox, W., Park, J., Regnerus, M., & Woodberry, R. (2000). The measure of American religion: Toward improving the state of the art. Social Forces, 79, 291–318.
Stroope, S., Franzen, A. B., & Uecker, J. E. (2015). Social context and college completion in the United States: The role of congregational biblical literalism. Sociological Perspectives, 58, 120–137.
Ulmer, J. T., & Harris, C. T. (2013). Race and the religious contexts of violence: Linking religion and White, Black, and Latino violent crime. The Sociological Quarterly, 54, 610–646.
Weber, M. (1930). The Protestant ethic and the spirit of capitalism. New York: Scribner.
Acknowledgements
This study uses data from the National Study of Youth and Religion, a research project designed by Christian Smith, of the Department of Sociology at the University of Notre Dame, and generously funded by the Lilly Endowment Inc. of Indianapolis, IN.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Nie, F. Body Mass Index in Religious Contexts: Exploring the Multilevel Influences of Religion. J Relig Health 60, 1160–1178 (2021). https://doi.org/10.1007/s10943-019-00844-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10943-019-00844-4