
Abstract
The relationship between atheism and health is poorly understood within the Religion/Spirituality–health literature. While the extant literature promotes the idea that Attendance, Prayer, and Religiosity are connected to positive health outcomes, these relationships have not been established when controlling for whether a person is an atheist. Data from the 2008–2012 American General Social Survey (n = 3210) were used to investigate this relationship. Results indicated that atheists experienced Religiosity more negatively than non-atheists. Additionally, results demonstrated that non-belief in God was not related to better or worse perceived global health, suggesting that belief in God is not inherently linked to better reported health.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Predicting Atheists’ Health from Religious/Spiritual Variables
Within the health psychology literature, Religious/Spiritual (R/S) constructs (i.e., Attendance, Prayer, and Religiosity) have been linked to a variety of positive health outcomes (Krause and Hayward 2012; Levin and Chatters 1998; Powell et al. 2003). However, while the general theme of the literature addressing R/S–health is positive, there have been critics who have argued that this relationship is less strong than what is suggested (Sloan and Bagiella 2001). There is merit to this criticism as the literature, among other shortcomings, has largely ignored persons who are traditionally unaffiliated with R/S (Hwang et al. 2011). The extant literature largely describes the effects of R/S on health, but often only does this in terms of religious samples (e.g., Benjamins et al. 2006), which would not apply to persons unaffiliated with religion and/or spirituality. Alternatively, researchers will use general samples to investigate these relationships (e.g., Krause and Hayward; Levin and Chatters); however, these general samples are largely dominated by the religious. Overall, there is a consistent failure to appreciate that persons who are unconnected to R/S may experience R/S constructs differently. This absence of studies is notable particularly in regard to how atheists experience R/S constructs.
In the simplest sense of the word, an “atheist” is a person who does not believe in god(s) (Hwang et al. 2011; O’Brian-Baker and Smith 2009). Because any belief is necessarily a positive position, anyone who would not agree with the statement “I believe in god(s)” is definitionally an atheist. This type of atheism is described as “Negative Atheism”; a person is an atheist simply because he/she lacks belief in god(s). While a lack of belief in god(s) is often confused with the declaration of the non-existence of a god(s), which would be “Positive Atheism,” this tends to be a less inclusive view of what atheism is. Unfortunately, atheism has been equated with being non-religious (Grözinger and Matiaske 2013), non-participation in religious events (Hsaio et al. 2013), and non-belief in an afterlife (Lundh and Radon 1998).
To add to these definitional issues, research treats atheism as a religious affiliation (Hackett 2014), which represents a substantial issue that has largely been ignored by the extant literature. Typically, persons identifying as “atheist” would fall under the “non-religious” category (Social and Aboriginal Statistics Division 2010). However, atheism/theism is a question of belief/non-belief and is not necessarily connected to how a person perceives themselves in relation to a religious group. Persons can identify with any number of religious faiths without having a concomitant belief in god(s). For example, a person may not believe in god(s) but still indicate that he/she is Christian (Hackett). Atheism as a religious affiliation is problematic because it means that religious “groups” are not necessarily exclusive of each other. This is not to suggest that religious affiliation and being an atheist are unrelated topics, but these responses are products of two distinct questions—“Do you believe in god(s)?” (atheist/theist) and “What religion do you identify as being a part of?” (e.g., Christian, Muslim, Hindu). In short, not only is atheism rarely studied in the context of R/S, but when it is studied, the definitional variability makes comparisons extremely problematic.
Like atheism, agnosticism has a variety of definitions and is often perceived as a Religious Identity. Typically, agnostics will either indicate (1) they are unsure if god(s) exist; (2) the nature of god(s) is ultimately unknowable; and/or (3) the existence of god(s) cannot be disproven (Benn 1999). Agnosticism is often presented as a sort of middle ground between atheism and theism, when under closer inspection agnosticism is in fact irrelevant to the atheism/theism binary. Persons who answer the question, “Do you believe in god(s)?” with statements related to knowledge, are not actually responding to the question at hand. A person is able to believe many things without having knowledge that they are correct. For example, a person could indicate that he/she does not believe he/she will get into a car accident during the following week, but this does not mean that he/she is stating with certain knowledge that they will not do so. Because belief and knowledge are different aspects to philosophical positions, it is possible to be an agnostic atheist, a gnostic atheist, an agnostic theist, or a gnostic theist.
The definitions of atheism are relevant to the broader R/S–health research, due in part to how salutary relationships between R/S constructs and health are explained. Occasionally, researchers will account for positive, non-objective health outcomes by suggesting that R/S provides a coherent framework in which to interpret the world (George et al. 2002). The rationale of this explanation is that R/S constructs are associated with better outcomes because Attendance, Prayer, Religiosity, etc. are valued by persons, and these activities therefore provide optimism or comfort. While this may be true, the current literature also assumes that R/S constructs are experienced similarly by persons irrespective of their belief in god(s). This assumption is remarkable as research suggests that atheists attend church less frequently, pray less frequently, and have lower religiosity than their non-atheist counterparts (O’Brian-Baker and Smith 2009). At the very least the differences in these R/S construct levels suggest R/S constructs are valued differently by atheists, probably less so. In a sense, the substantive gap in the literature is a failure to investigate how atheists experience R/S constructs. The default position appears to be that atheists experience R/S constructs similarly to non-atheists; however, this position is untenable with why R/S constructs are reasoned to be beneficial.
Unfortunately, atheism and health is rarely studied despite frequent calls to do so (Galen and Kloet 2011; Hwang et al. 2011; Smith-Stoner 2007). While there has been limited support of the idea that belief is positively associated with some health outcomes (Ekedahl and Wengström 2010; Koenig 1995; Rosmarin et al. 2013), there has been a conspicuous absence of evidence suggesting that a lack of belief is associated with poorer health outcomes. Rather than addressing this issue head-on, researchers will often assume low religiosity is the equivalent of high secularity and will investigate differences between groups on that basis (Hwang et al. 2011). Unfortunately, this does not adequately address atheists as a group and therefore does not clarify the issue at hand. A cursory reading of the literature would suggest that non-belief in god(s) is associated with poorer health, but this relationship is not explicitly tested.
The literature addressing atheists has found varied results. Atheism has been linked to better health outcomes (Buggle et al. 2000; Wilkinson and Coleman 2010), atheism has been unrelated to health (Baker and Cruickshank 2009; Fogel and Ebadi 2011; Horning et al. 2011), and atheism has been linked to poorer health outcomes. In these “poorer health outcomes” situations, atheists fared less well in situations requiring “religious coping” (Baker and Cruickshank 2009) or were less likely to succeed in religiously themed sobriety programs (Humphreys 1997). However, these findings only suggest that some rehabilitation programs may not work for atheists, not that atheism is inherently unhealthy. Overall, the relationship between atheism and health is largely unexplored, and it is unclear as to whether non-belief in god(s) is related to perceived health.
Methods
Data Source
The 1972–2012 American General Social Survey (GSS) cumulative file was accessed through the Inter-University Consortium for Political and Social Research (Smith et al. 2013) (Study Number 34802). The American GSS is a national probability sample of the adult resident population of the USA. These data were chosen due to their representativeness of American citizens and because questions of interest were contained within the dataset.
Participants
To be eligible for participation within the current study, respondents had to answer all relevant items. Respondents answering, “I don’t know” to questions were excluded from analysis in order to maintain the continuous nature of the data. There were no participatory restrictions placed on religious affiliation or age. For further details on the sampling technique, see Smith et al. (2013). Of the described criteria, there were 3427 respondents (1572 males and 1855 females), with the average age of the respondents being 45.63 (SD = 16.33) years. Within this sample, there were 108 Positive Atheists (3.18 % of the entire sample). Of these 108 Positive Atheists, 29 persons identified as being a part of a religious affiliation (26.85 %). Of these 29 persons, 22 persons identified as being a part of a Christian denomination, while the remaining 7 identified as being Jewish. See Table 1 for descriptive statistics. The current study only used pooled data from 2008, 2010, and 2012 to improve statistical power.
Survey Items
Demographics
Age (measured on a continuous scale), sex (male/female), real household income (measured on a continuous scale), years of education (measured on a continuous scale), region (New England, Middle Atlantic, Eastern North Atlantic, Western North Atlantic, South Atlantic, Eastern South Atlantic, Mountain, Pacific), marital status (married, widowed, divorced, separated, never married), minority status (white/non-white), and year (2008, 2010, 2012) were all included as covariates.
R/S Constructs
Three items were used to assess different religious behaviors and attitudes. There was a nine-point Attendance item (“How often do you attend religious services?”), a six-point Prayer item (“How often do you pray?”), and a four-point Religiosity item (“To what extent do you consider yourself a religious person?”). For all R/S constructs, higher scores indicated a greater frequency of behavior or greater attitudinal strength. These R/S constructs have been linked to better perceived global health within the extant literature [Attendance (Levin and Markides 1986); Prayer (Harrigan 2011); Religiosity (Levin and Chatters 1998; Mochon et al. 2011)]. The current study will initially investigate the relationship between R/S constructs and global perceived health, and will then focus on whether these relationships are moderated by whether a person is an atheist.
Belief Categories
Belief Categories were derived from the item, “…which statement comes closest to expressing what you believe about God?” [“I don’t believe in God” (Positive Atheists); “I don’t know whether there is a God and I don’t believe there is any way to find out” (Agnostics); “I don’t believe in a personal God, but I do believe in a higher power of some kind” (Deist); “I find myself believing in God some of the time, but not at others” (Weak theist); “While I have doubts, I feel that I do believe in God” (Moderate theist); “I know God exists and I have no doubts about it” (Strong theist)]. Each category of response to this question was included in the regression model to allow for comparisons between dissimilar identities; however, only moderation terms that compared Positive Atheists to persons who were not Positive Atheists (i.e., non-atheists) were of interest to the current study. The term “Positive Atheist” was used as respondents in this category which indicated that they did not believe in God, and would have also indicated some degree of certainty.
Self-Rated Health
The only health indicator available was a single four-point item assessing Self-Rated Health (“Would you say your own health, in general, is excellent, good, fair, or poor?”). Although using a single item to classify Self-Rated Health (SRH) is less than ideal, this approach is consistent with other studies (e.g., Green and Elliot 2010; Krause 2006). This scale was reverse-coded so that higher scores indicated greater health.
Data Analysis
Data were centered to improve interpretability (West et al. 1996), and continuous variables were standardized. Heteroscedastic-consistent error terms were used in assessing predictors within the model (Long and Ervin 2000). Data were weighted with a weighting variable that accounted for the non-response rate (Smith et al. 2013). Data analysis was conducted with Stata 13 using the complex samples module. This approach was used to ensure that estimates of error were accurate. Because of the usage of complex samples, the second value for degrees of freedom for F-statistics represents design degrees of freedom. Sampled strata that only contained single sampling units were dealt with by using scaled values.
Research Questions
The current study investigated the relationship between R/S constructs (Attendance, Prayer, and Religiosity) and Self-Rated Health (SRH) through regression. To this end, hypotheses have been ordered so that they correspond with the regression block that will test that specific hypothesis.
- Block 1:
-
Demographic covariates were entered
- Block 2:
-
R/S constructs were entered
- Block 3:
-
Belief Categories were entered. While the literature has suggested that belief in god(s) is associated with better health outcomes, there has been a lack of corresponding literature suggesting atheism is associated with poorer health outcomes
Hypothesis 1
Given the poor quality of the literature, no hypotheses will be offered in regard to atheism predicting SRH; however, researchers suspect that there will be no differences between Positive Atheists and non-atheists.
- Block 4 (stepwise regression):
-
Moderator terms for Attendance, Prayer, and Religiosity were entered into the regression mode
Hypothesis 2
Significant moderation terms will be negative. This will support the contention that Positive Atheists (the reference group for these regression models) will experience R/S constructs more negatively than non-atheists.
Hypothesis 3
When compared on the highest levels for any moderated R/S construct, Positive Atheists are predicted to report poorer SRH than non-atheists (this is a one-tailed hypothesis). This would support the contention that Positive Atheists experience high levels of R/S constructs less positively than non-atheists.
Hypothesis 4
When compared on the Positive Atheist average for any moderated R/S construct, Positive Atheists are predicted to report comparable SRH to non-atheists (this is a one-tailed hypothesis). This would suggest that Positive Atheists reporting low levels of R/S constructs have similar SRH compared to other Belief Categories.
Results
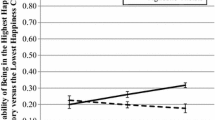
Self-Rated Health (SRH) was regressed on covariates in Block 1 F(19, 300) = 17.66, p < .001, R 2 = .109. Religious/Spiritual constructs were entered in Block 2, ΔR 2 = .007 F(3, 300) = 6.52, p < .001, R 2 = .116. Results indicated that Attendance positively predicted SRH, t = 3.91, p < .001, 95 % CI (0.05, 0.16). However, neither Prayer nor Religiosity predicted SRH. Self-Rated Health was regressed on Belief Categories in Block 3, t = 0.49, p = .783. Results indicated that would suggest that being a Positive Atheist was not associated with poorer global health than any other comparison group. This was consistent with the expectations expressed in Hypothesis 1. A stepwise regression block was used in Block 4, ΔR 2 = .002, R 2 = .119. Positive Atheists experienced Religiosity more negatively than non-atheists (i.e., all other Belief Categories), t = −3.32, p < .001, 95 % CI (−0.56, −0.14) (see Fig. 1). While not all R/S constructs were moderated by Belief Categories, this finding were still consistent with Hypothesis 2; Religiosity was experienced more negatively by Positive Atheists than by non-atheists (see Table 2 for regression model).

Religiosity predicting Self-Rated Health for positive atheists error bars represent 95 % confidence intervals. For aesthetic purposes, the line representing group “Not Positive Atheists” depicts the average of the coefficients for the belief category groups in Block 4
While confirmation of Hypothesis 2 established that Religiosity was more negatively experienced by Positive Atheists than by non-atheists, this would not necessarily mean that Positive Atheists reporting high levels of Religiosity would be less healthy than non-atheists reporting the same levels of Religiosity. However, with the inclusion of Block 4, being a Positive Atheist was associated with poorer SRH when compared to every other Belief Category (supporting Hypothesis 3). In other words, Positive Atheists were less healthy than Agnostics, Deists, Weak theists, Moderate theists, and Strong theists. However, because the Religiosity variable had been centered at the national average of Religiosity, this result is initially misleading. When Religiosity was re-centered at the average level for Positive Atheists, group differences disappeared (supporting Hypothesis 4). In other words, Positive Atheists reported lower health than Agnostics, Deists, Weak theists, Moderate theists, and Strong theists, but only when Positive Atheists reported atypically high levels of Religiosity. When Positive Atheists displayed “typical” levels of Religiosity (i.e., extremely low levels of Religiosity), there were no differences between Positive Atheists and any other Belief Category.
Three exploratory analyses were conducted that investigated subgroups. The goal of the exploratory analysis was to determine whether other Belief Categories (i.e., Agnostics, Deists, Weak theists, Moderate theists, and Strong theists) also reported experiencing Religiosity differently than other Belief Categories. For this follow-up analysis, Positive Atheists were removed from population of consideration. No other Belief Category was found to moderate the experience of Religiosity, which suggests that only Positive Atheists experienced increased Religiosity differently. Interestingly, this would indicate that Strong theists did not experience Religiosity more positively than other Belief Categories. The second exploratory analysis compared Positive Atheists who reported the lowest levels of Religiosity against non-atheists who reported the highest level of Religiosity. When entered into the regression model, Positive Atheism was not predictive of SRH, t = 1.18, p = .240, 95 % CI (−0.23, 0.90), which would suggest that Positive Atheists of low Religiosity and non-atheists reporting high Religiosity, did not differ in terms of SRH. Interesting, Attendance remained a positive predictor of SRH and was not moderated by whether a person was a Positive Atheist. To investigate the idea that Attendance was linked to better health even in Positive Atheists, a follow-up analysis was conducted. When only considering Positive Atheists, Attendance, t = 1.13, p = .260, 95 % CI (−0.16, 0.57) was a non-significant predictor of SRH, while Religiosity continued to be a negative predictor of SRH. Overall, these findings are supportive of the idea that R/S constructs are experienced differently by Positive Atheists.
Discussion
While the R/S–health literature is vast, there have been a very limited number of studies addressing the relationship between atheism and health. The findings from the current study varied, but centered on the idea that R/S was experienced differently by atheists. Positive Atheists experience Religiosity more negatively than their non-atheist counterparts; which appears to be the first time a finding like this has been described within the literature. Secondary findings suggested that Positive Atheists experienced Religiosity more negatively than every other Belief Categories. Moreover, Positive Atheists reporting the lowest level of Religiosity and non-atheists reporting the highest level of Religiosity did not differ in terms of SRH. Finally, tertiary findings emerged from the descriptive statistics section of the Methods sections; approximately one quarter of persons who indicated that they did not believe in God also indicated that they were religious.
Although studies occasionally describe a positive relationship between R/S constructs and health, there has not been any concerted effort within the literature to determine whether R/S constructs are uniformly beneficial. The extant literature has consistently failed to explore whether the salutary relationship between R/S constructs and health is moderated by what a person values. Even basic consideration of religious affiliation is absent from the literature, which is surprising given that questions related to religious affiliation are often collected as part of national surveys related to health (e.g., Krause 2006; Krause and Hayward 2006; Levin and Chatters 1998). In the current study, evidence was provided that while Religiosity was a nonsignificant predictor of SRH in a general sample, it was actually a significant negative predictor of health for Positive Atheists.
While previous research has suggested belief in God is positively predictive of health outcomes in clinical settings (e.g., Rosmarin et al. 2013), this finding was not replicated within this general study. The findings seemed to indicate that Belief Categories (i.e., Positive Atheist, Agnostics, Deists, Weak theists, Moderate theists, and Strong theists) were generally unrelated to reported global health. This nonsignificant result is supportive of the idea that belief in God is not inherently linked to better health. Additionally, given that there was adequate power to find even a small effect, this null finding is unlikely to be the product of Type II error. In general, it appears that non-belief in God is not associated with any type of health penalty, nor was agnosticism or deism.
Consistent with the research hypothesis, the only time in which being a Positive Atheist was associated with poorer SRH is when Positive Atheists displayed atypically high levels of Religiosity. This finding is of note because it confirms two related ideas. The first is that Positive Atheists do not experience Religiosity in the same way as non-atheists do. The second is that not only do Positive Atheists experience Religiosity differently, they experience Religiosity more negatively. Positive Atheists reporting higher Religiosity did not report a concomitant increase in health, which would be expected if Religiosity were to be unconditionally associated with better health. When Positive Atheists did report the highest level of Religiosity, this was associated with dramatically lower levels of SRH. In fact, when Positive Atheists reported the highest level of Religiosity, they reported lower health than Agnostics, Deists, Weak theists, Moderate theists, and Strong theists. In general, Positive Atheists reported poorer health than every other Belief Category—but only when Positive Atheists reported an atypically high level of Religiosity. When Positive Atheists with low Religiosity were compared against non-atheists with high Religiosity, there were no differences between the groups. These findings are supportive of the contention that valuation (or lack thereof) likely plays a role in explaining why Religiosity predicts health.
It is noteworthy that Attendance remained a positive predictor of Self-Rated Health (SRH) and was not experienced differently by Positive Atheists. While this finding could be interpreted as being supportive of the idea that Attendance has a positive relationship with SRH for Positive Atheists, caution would be urged within this interpretation. One of the benefits associated with Attendance is higher levels of social support (Horning et al. 2011), which was not controlled for within the current study. Therefore, it is unclear from the current study whether Attendance promoted SRH, or whether Attendance promoted social support which in turn promoted SRH.
Within the introduction, it was noted that treating atheism as a religious affiliation produces substantial conceptual issues. Because of these issues, there has been recognition that the General Social Survey may inadequately capture the diversity the “religiously unaffiliated” (Woodberry et al. 2012), although whether this will lead to substantive changes is unknown. In the current study, 26.85 % of the Positive Atheists included within the study, indicated that they belonged to a religious denomination. While this figure represents a small percentage of various religious groups, it represents a non-negligible proportion of Positive Atheists. In other words, a minority of persons who would be counted as “religious” within much of the current literature are classifiable as “atheists” using the current study’s definition. Frustratingly, being able to assess Positive Atheism [believing there is no god(s)] or Negative Atheism [not believing in god(s)] would be relatively easy to assess [e.g., “Do you believe there is no god(s)?” or “Do you believe in god(s)?”], and would therefore be easy to effect change. However, these data are infrequently gathered and are therefore difficult to use to inform the current discussion.
Determining the number of atheists by asking about what a person believes, which is the approach used in this study, is a superior approach to asking a person to identify as being an atheist. Persons perceive atheism to be any number of things and may even identify as atheist without understanding what the label means (Hwang et al. 2011; Woodberry et al. 2012). Because of the wide-ranging definitional issues, persons may identify as being an atheist but may also indicate that they believe in god(s) or some “higher power” (Hackett 2014). Additionally, persons are reluctant to identify as atheists because of stigma associated with the label “atheist” (Hwang et al.). In the current study, persons who were identified as Positive Atheists may not have self-identified as being atheists. However, this underscores a critical point in the current study: A person’s belief is what predicted their experience of R/S constructs, not necessarily how he/she identified. Overall, the argument against using atheism as a religious affiliation is not merely one of semantics; it is one of practical consequences as well.
Ultimately, the decision to assess atheism as a question of belief rather than one of identity reduces to an important philosophical question. Is the research better served by determining how many persons identify as “atheist,” or is the research better served by determining how many persons do not believe in god(s)? Given the range of conceptualizations that “atheism” invokes, it is suggested that collecting data on belief may be more worthwhile. This would be a relatively simple change to enact and would help inform the national discussion on the relationship between atheism and health.
Limitations and Future Directions
A limitation to the current study was the restricted number of health outcomes. The only health outcome assessed was Self-Rated Health (SRH), which was a single-item indicator of subjective well-being. While other research within the R/S–health field has used similar items, it is desirable to investigate a wider range of health outcomes. Ideally, both subjective and objective health outcomes would be investigated. The limited number of health outcomes was the product of using archival data. However, given that the General Social Survey was a representative national sample of Americans, these limitations were arguably worthwhile.
In the future, researchers should consider the role of R/S identities as moderators for the experience of R/S constructs. The assumption that Positive Atheists would experience R/S constructs the same as the religious or spiritual is at best, religious privileging. In closing, while R/S constructs are likely related to a variety of positive health outcomes, it would appear that these relationships are nuanced by questions of belief. It would be to the benefit of the field as a whole to address which group memberships affect the experience of R/S constructs. In short, while the R/S–health literature is enormous, there is much work to be done to refine the body of findings.
References
Baker, P., & Cruickshank, J. (2009). I am happy in my faith: The influence of religious affiliation, saliency, and practice on depressive symptoms and treatment preference. Mental Health, Religion and Culture, 12, 339–357. doi:10.1080/13674670902725108.
Benjamins, M. R., Trinitapolli, J., & Ellison, C. G. (2006). Religious attendance, health maintenance beliefs, and mammography utilization: Findings from a nationwide survey of Presbyterian women. Journal for the Scientific Study of Religion, 45, 597–607. doi:10.1111/j.1468-5906.2006.00330.x.
Benn, P. (1999). Some uncertainties about agnosticism. International Journal for Philosophy of Religion, 46, 171–188.
Buggle, F., Bister, D., Nohe, G., Scheider, W., & Uhmann, K. (2000). Are atheists more depressed than religious people? Free Inquiry, 20(4), 50–54.
Ekedahl, M. A., & Wengström, Y. Y. (2010). Caritas, spirituality and religiosity in nurses’ coping. European Journal of Cancer Care, 19, 530–537. doi:10.1111/j.1365-2354.2009.01089.x.
Fogel, J., & Ebadi, C. (2011). Religious categories and the human papillomavirus (HPV) vaccine: Attitudes, intentions, and behaviors regarding vaccination. Journal Of Medical Marketing, 11, 303–311. doi:10.1177/1745790411428232.
Galen, L., & Kloet, J. D. (2011). Mental well-being in the religious and the non-religious: Evidence for a curvilinear relationship. Mental Health, Religion and Culture, 14, 673–689. doi:10.1080/13674676.2010.510829.
George, L. K., Ellison, C. G., & Larson, D. B. (2002). Explaining the relationship between religious involvement and health. Psychological Inquiry, 13, 190–200.
Green, M., & Elliott, M. (2010). Religion, health, and psychological well-being. Journal of Religion and Health, 49, 149–163. doi:10.1007/s10943-009-9242-1.
Grözinger, G., & Matiaske, W. (2013). The direct and indirect impact of religion on well-being in Germany. Social Indicators Research, 116, 373–387. doi:10.1007/s11205-013-0308-9.
Hackett, C. (2014). Seven things to consider when measuring religious identity. Religion, 44, 396–413. doi:10.1080/0048721X.2014.903647.
Harrigan, J. T. (2011). Health promoting habits for people who pray for their health. Journal of Religion and Health, 50, 602–607. doi:10.1007/s10943-009-9293-3.
Horning, S. M., Davis, H. P., Stirrat, M., & Cornwell, R. (2011). Atheistic, agnostic, and religious older adults on well-being and coping behaviors. Journal of Aging Studies, 25, 177–188. doi:10.1016/j.jaging.2010.08.022.
Hsiao, Y., Chiang, Y., Lee, H., & Han, C. (2013). Psychometric testing of the properties of the spiritual health scale short form. Journal of Clinical Nursing, 22, 2981–2990. doi:10.1111/jocn.12410.
Humphreys, K. (1997). Clinicians’ referral and matching of substance abuse patients to self-help groups after treatment. Psychiatric Services, 48, 1445–1449.
Hwang, K., Hammer, J., & Cragun, R. (2011). Extending religion-health research to secular minorities: issues and concerns. Journal of Religion and Health, 50(3), 608–622. doi:10.1007/s10943-009-9296-0.
Koenig, H. G. (1995). Religion and older men in prison. International Journal of Geriatric Psychiatry, 10, 219–230.
Krause, N. (2006). Gratitude toward god, stress, and health in late life. Research on Aging, 28, 163–183. doi:10.1177/0164027505284048.
Krause, N., & Hayward, R. R. (2012). Humility, lifetime trauma, and change in religious doubt among older adults. Journal of Religion and Health, 51, 1002–1016. doi:10.1007/s10943-012-9576-y.
Levin, J. S., & Chatters, L. M. (1998). Religion, health, and psychological well-being in older adults: Findings from three national surveys. Journal of Aging and Health, 10, 504–531. doi:10.1177/089826439801000406.
Levin, J. S., & Markides, K. S. (1986). Religious attendance and subjective health. Journal for the Scientific Study of Religion, 25, 31–40.
Long, J. S., & Ervin, L. H. (2000). Using heteroscedasticity consistent standard errors in the linear regression model. The American Statistician, 54, 217–224.
Lundh, L., & Radon, V. (1998). Death anxiety as a function of belief in an afterlife: A comparison between a questionnaire measure and a Stroop measure of death anxiety. Personality and Individual Differences, 25, 487–494.
Mochon, D., Norton, M., & Ariely, D. (2011). Who benefits from religion? Social Indicators Research, 101(1), 1–15. doi:10.1007/s11205-010-9637-0.
O’Brian-Baker, J., & Smith, B. (2009). None too simple: Examining issues of religious nonbelief and nonbelonging in the United States. Journal for the Scientific Study of Religion, 48, 719–733.
Powell, L. H., Shahabi, L., & Thoresen, C. E. (2003). Religion and spirituality. American Psychologist, 58, 36–52. doi:10.1037/0003-066X.58.1.36.
Rosmarin, D. H., Bigda-Peyton, J. S., Kertz, S. J., Smith, N., & Rauch, T. B. (2013). A test of faith in god and treatment: The relationship of belief in god to psychiatric treatment outcomes. Journal of Affective Disorders, 146, 441–446. doi:10.1016/j.jad.2012.08.030.
Sloan, R. P., & Bagiella, E. (2001). Claims about religious involvement and health outcomes. Annals of Behavioural Medicine, 24, 14–21.
Smith, T. W., Hout, M., & Marsden, P. V. (2013). General Social Survey, (1972–2012) [Cumulative File]. 427 ICPSR34802-v1. Storrs, CT: Roper Center for Public Opinion Research, University of Connecticut / 428 Ann Arbor, MI: Inter-university Consortium for Political and Social Research [distributors], 2013-09-429 11. http://doi.org.qe2aproxy.mun.ca/10.3886/ICPSR34802.v1.
Smith-Stoner, M. (2007). End-of-life preferences for atheists. Journal of Palliative Medicine, 10, 923–928. doi:10.1089/jpm.2006.0197.
Social and Aboriginal Statistics Division. (2010). General Social Survey cycle 22: Social networks public use microfile documentation and user’s guide. [Catalogue no. 12M0022G]. Retrieved http://qe2a-proxy.mun.ca/Login?url=http://equinox2.uwo.ca/EN/BasicSearch.asp
West, S. G., Aiken, L. S., & Krull, J. L. (1996). Experimental personality designs: Analyzing categorical by continuous variable interactions. Journal of Personality, 64, 1–48. doi:10.1111/j.1467-6494.1996.tb00813.x.
Wilkinson, P. J., & Coleman, P. G. (2010). Strong beliefs and coping in old age: A case-based comparison of atheism and religious faith. Ageing and Society, 30, 337–361. doi:10.1017/S0144686X09990353.
Woodberry, R. D., Park, J. Z., Kellstedt, L. A., Regnerus, M. D., & Steensland, B. (2012). The measure of American religious traditions: Theoretical and measurement considerations. Social Forces, 91, 65–73. doi:10.1093/sf/sos121.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Speed, D., Fowler, K. What’s God Got to Do with It? How Religiosity Predicts Atheists’ Health. J Relig Health 55, 296–308 (2016). https://doi.org/10.1007/s10943-015-0083-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10943-015-0083-9