
Abstract
Case conceptualization is a widely used tool to describe and organize patient information and plan interventions in psychotherapy. Life themes and semi-adaptive plans: Implications of biased beliefs, elicitation, and treatment (LIBET) is a new method for case conceptualization that validates the diathesis-stress model and incorporates elements from the most important theories in the CBT field. LIBET also includes process-based components as maintaining factors of psychological distress, and it is not anchored to a specific kind of psychotherapeutic approach. The LIBET-Questionnaire (LIBET-Q) is a structured interview which helps clinicians achieve a LIBET case conceptualization, co-constructed with patients. The aim of the present study was to validate the process-based section of the LIBET-Q by analyzing its factorial structure, internal consistency, convergent validity, and clinical relevance. A sample of 396 outpatients was recruited to validate the LIBET-Q, which was administered along with interviews and self-report questionnaires to investigate the presence of diagnoses, anxiety, and depression levels and global functioning and wellbeing. Results from both exploratory and confirmatory factor analyses showed a four-factor structure, with adequate consistency and good convergent validity. Process-based elements investigated with the LIBET-Q resulted in identifying different clinical populations. With satisfactory psychometric properties, the LIBET-Q turned out to be a suitable support for case conceptualization and treatment formulation. The independence of the LIBET method from a specific intervention can improve its sharing between clinicians by offering a common frame in which the rationale of every specific technique can be explained.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Case Formulation in Cognitive-Behavioral Therapy
Case formulation is a therapeutic tool that uses a psychological theory to describe a patient’s functioning and symptomatology in an understandable way (Bucci et al., 2016). The type of formulation used in psychotherapy is linked to a specific theory regarding the origins and development of psychological distress (Ruggiero et al., 2018). Every single approach conceptualizes different aspects as relevant, for instance feelings, thoughts, or the impact of life events, and it provides its specific hypothesis to a patient’s functioning (Johnstone & Dallos, 2013). Moreover, case conceptualization is also useful in planning treatment and interventions based on identified psychological processes (Johnstone et al., 2011). Easden and Kazantzis (2017) reviewed case conceptualization in cognitive-behavioral therapy (CBT) and found three levels of conceptualization: First, a situation-level conceptualization in which patients can identify antecedents, thoughts, feelings, and consequences of a specific stressful event (Padesky & Mooney, 1990). A second type is focused on a list of problems, which underlines a patient’s goals and priorities for treatment (Persons, 1989). Finally, comprehensive conceptualization formats aim to identify core self-beliefs or self-schemata that are responsible for a patient’s distress among a wide range of different situations (Beck, 2011). Some of these comprehensive conceptualization formats can include developmental or attachment features, along with etiological elements, perpetuating factors, and the patient’s resources (Kazantzis et al., 2017; Kuyken et al., 2008). Even if there are peculiar differences, almost all the case conceptualization processes follow some common steps: (1) describe clinical information; (2) infer and organize observed information; and (3) apply a formulation to the case, and revise it when necessary (Eells, 2007).
Behaviorism conceptualizes individuals’ problems using functional analysis, which is defined as the identification of important, controllable, causal functional relationships applicable to specified behaviors for an individual (Haynes et al., 1993). The emphasis on components that can be controlled helps clinicians plan an intervention that addresses changeable variables in a clinically useful way (Gresham, 1985).
In CBT, case conceptualization is based on the diathesis-stress model, proposed by Meehl (1962) to explain schizophrenia’s etiology. Beck et al. (1979) applied this model to cognitive therapy for depression by conceptualizing an individual’s distress as the result of negative core beliefs about self, world and future that lead to misinterpretation of everyday events. Core beliefs are thought responsible for negative emotions and dysfunctional coping strategies by inducing incorrect assumptions and negative automatic thoughts. Case conceptualization in Beck’s (2011) approach is a hierarchical organization of these three-level thoughts and self-declared rules: automatic thoughts, conditional assumptions, and core beliefs. In the same period, Ellis (1962) proposed a different cognitive model, called rational emotive behavior therapy (REBT). REBT is focused on the disputing of irrational beliefs that cause unhealthy emotions (Ellis, 1994). In REBT, case conceptualization is focused on a specific event (situation-level formulation) and activating events (A), the system of belief (B), emotional and behavioral consequences (C), disputation (D), new effects (E), and new feelings (F) in the ABCDEF model, which is the principal tool to analyze and modify unpleasant situations (DiGiuseppe et al., 2013). So, even if the CBT panorama at the beginning of its development was not so complex, several case conceptualizations already existed, with commonalities and differences (Kuyken et al., 2005). Many other theorists followed Beck and Ellis by structuring their own formats for case conceptualization (i.e., Lazarus, 1976; Mahoney, 1974; Mansell et al., 2008; Meichenbaum, 1977). The previously mentioned Easden and Kazantzis (2017) review revealed that there are several ways to conceptualize a patient’s situation, but there is no significant data about which kind of conceptualization is the most efficient.
REBT or DBT conceptualizations are used to address an entire session to the conceptualization process, and it is planned for every single session, at least in the first part of therapy (DiGiuseppe et al., 2013; Linehan, 2015). Other therapies focus the case conceptualization on a few central aspects that are measured and monitored (i.e., psychological flexibility, or metacognitive control).
Given the central role of case conceptualization in CBT, a complete and simple tool to analyze patients’ situations is necessary to record data and give feedback to patients. It would be useful to engage patients in a cooperative relationship, in line with the collaborative empiricism approach, one of the core elements in CBT (Easden & Kazantzis, 2017). The onset of different case conceptualization models has led to a fragmentation in the field that compromises clinicians’ ability to share information and understand colleagues’ therapeutic choices (Eells, 2007). This lack of common language implies critical issues in exchanging information, fixation on one’s theoretic perspective and, consequently, difficulties in sharing new evidence (Ridley et al., 2017). Moreover, a new kind of case conceptualization must consider metacognitive elements, which are distinguished aspects in several CBT recent approaches (i.e., Wells, 2008). LIBET model can be a comprehensive tool for case conceptualization, cross every single approach that stands under CBT umbrella.
The LIBET Method as a Tool for Case Conceptualization and Treatment Formulation
Life themes and semi‐adaptive plans: Implications of biased beliefs, elicitation, and treatment (LIBET) is a CBT case formulation method grounded on Beck’s diathesis–stress model which aims to develop its bidimensional arrangement of core beliefs and coping strategies by including in it developmental and processual aspects. In the LIBET method: (1) core beliefs are expanded to general life themes because they include not only biased cognition but also the developmental roots of emotional vulnerability perceived as mental states of focused attention to emotional sensitivities, represented as verbalizable core self-beliefs in consciousness and accompanied by painful somatic and emotional perceptions influenced by painful or even dangerous experiences during personal development that left some of the primary emotional needs of the individual unsatisfied (Bandura, 1977, 1988; Beck, 2011; Bruner, 1973; Capo et al., 2010; Capo & Mancini, 2008; Csikszentmihalyi & Beattie, 1979; Di Fini & Veglia, 2019; Dodet, 2010; Frankl, 2006; Guidano & Liotti, 1983; Jaspers, 1971; Lorenzini & Sassaroli, 1995; Markus, 1977; Neisser, 1967; Panksepp & Watt, 2011; Schore, 2012a, 2012b; Wells, 2008); and (2) coping strategies are expanded to semi-adaptive behavioral plans because they are conceptualized as behavioral patterns that are initially characterized by a form of adaptability only subsequently compromised in unhealthy, rigid applications of functional developmental habits (Young et al., 2003), such as anxious safety behaviors (Salkovskis, 1991; Thwaites & Freeston, 2005), compulsive controls (Salkovskis, 1985), and aggressive or rewarding strategies, including desire-thinking, anger rumination, impulsive behaviors, and dependent behaviors (Critchfield et al., 2008; DiGiuseppe & Tafrate, 2007; Martin & Dahlen, 2005; Spada et al., 2013). These strategies are adopted even at the cost of giving up significant areas of personal development. In the long term, therefore, “semi-adaptive plans” hinder personal development and, beyond a certain level of dysfunctionality, may lead to emotional disorders.
The LIBET method remains grounded in the mainstream CBT framework because these two additional developmental and processual expansions of the classical bidimensional arrangement in core beliefs and coping strategies of CBT were already present in Beck’s model: The idea that dysfunctional self-beliefs are rooted in the personal development of the patient existed in the CBT stress-diathesis model as developmental emotional vulnerability (Beck, 1976, 2008; Beck & Bredemeier, 2016; Clark & Beck, 2010; Dobson et al., 2018) and was called “relevant childhood data” in the cognitive conceptualization diagram, which is the classical CBT case formulation procedure (Beck, 2011). It was also present in other cognitive approaches that cultivated this aspect, such as those by Bannister and Fransella (1971), Feixas and Miró (1993), Guidano (1987, 1991), Guidano and Liotti (1983), Lorenzini and Sassaroli (1995), Mahoney (1974, 1991, 2003), Neimeyer (2009), Neimeyer and Mahoney (1995), and Winter and Viney (2005). Overall, the LIBET method expands but does not betray the CBT case formulation model by conceptualizing it not only in terms of cognitive contents regarding core self-beliefs and coping strategies, but also including a developmental dimension that justifies the mental representability and verbalizability of emotional vulnerability in terms of core self-beliefs; it also includes a process dimension that justifies the rigidification of coping strategies in dysfunctional behaviors (Sassaroli et al., 2021).
In addition, the LIBET method promotes the integration of processual aspects into CBT, as proposed by Hayes and Hofmann (2018) in their process-based CBT model. Again, the importance of process components had already been identified in CBT models, such as by Aaron Beck himself when he described the “circle of fear” (Beck et al., 1985), or when he claimed the possibility of going beyond beliefs (Beck, 1996); similarly, Ellis had his seminal concept of “secondary ABC,” which was a forerunner of metacognitive concepts (DiGiuseppe et al., 2013; Sassaroli et al., 2005). The LIBET method attempts to integrate these process principles into the classical CBT diathesis-stress model by assuming that developmental vulnerability is not sufficient to determine the disorder but, if managed in a flexible way by individuals, can result in only temporary discomfort and not in negative core self-beliefs and dysfunctional coping strategies.
The LIBET method includes five process variables: (1) the intolerability and (2) conditioning referred to the life theme, and (3) the conditioning, (4) utility, and (5) uncontrollability about the semi-adaptive plan. Their definitions include: (1) The evaluation of intolerability of the theme modifies the value attributed to it as a mental experience and therefore can rigidify the system in a defensive perspective, both in preventive and reactive terms. The experience of intolerability can become worrying, an obligation to keep the attention focused on the pain itself; (2) conditioning of the life theme means that its experience is evaluated as pivotal for making decisions. It is an indication of how protection from the experience of the life theme is a priority for the individual and becomes a discriminating element for them to organize their daily and long-term choices; (3) the conditioning process about plans refers to the perceived level of interference of semi-adaptive plans in daily life. An increase in this scale can denote awareness about the dysfunctionality of the repertory adopted to avoid life themes; (4) the necessity of the semi-adaptive plan means that it is evaluated as required to protect the person from the life theme. This process organizes the system resources for the planning, activation, and suspension of actions (i.e., cognitive, such as worry, or behavioral, such as withdrawal) by following internal signals—whether they be bodily or cognitive—associated with the life theme; (5) the fifth and final metacognitive regulation variable is the uncontrollability of semi-adaptive plans. Different expressions underlie this perspective: “It’s just the way I am”, or “it is my nature”. The most studied processes of this kind are beliefs about the uncontrollability of worry and one’s behavior (for a review, see Wells, 2013). In line with the description proposed by Flavell (1979), which defined metacognitive knowledge as “that segment of your (a child’s, an adult’s) stored world knowledge that has to do with people as cognitive creatures and with their diverse cognitive tasks, goals, actions, and experiences” (p. 906), processes included in the LIBET method can be also defined as metacognitive processes.
The present study aimed to validate the processual component of the LIBET method. To achieve this goal, the LIBET-Questionnaire (LIBET-Q) was developed based on a previous validation of the LIBET method (Sassaroli et al., 2021). The LIBET-Q is composed of two sections: The first section is a qualitative investigation about the patient’s themes and plans, based on qualitative analyses of assessment sessions’ transcripts (see Sassaroli et al.). The second section is a list of 18 items, rated on visual analogue scales, which investigate the patient’s processes about themes and plans in terms of conditioning, pain, utility, and perceived control perceived per themes and plans. To validate the LIBET-Q, the sequent aims were explored using: (1) both exploratory and confirmatory factor analyses; (2) psychometric properties, such as internal consistency; (3) convergent validity with other measures; and (4) LIBET-Q profiles for different clinical populations (i.e., the absence/presence of comorbidities).
Method
Item Development
Items were generated by G. C., G. M. R., and S. S., based on their theorization of the metacognitive components of LIBET case conceptualization. The items were developed to assess two principal areas, including (1) metacognitive processes about life themes and (2) metacognitive processes about life plans. Processes about life themes were divided into two domains: intolerability (i.e., It is intolerable) and conditioning (i.e., It influences my self-realization). Processes about plans are of three different types: conditioning (i.e., They influence my choices in life), utility (i.e., They are useful to reach my goals), and uncontrollability (i.e., I can modify these strategies). The focus selected on metacognitive processes arises from the recent studies about metacognitive beliefs (Wells, 2008). In the self-regulation executive function model, Wells (2000) analyzed the role of metacognition in triggering maladaptive thinking styles and, subsequently, maintaining emotional distress. This perspective was integrated into the LIBET method, by applying metacognitive processes not only to thinking styles, but also to personal themes and plans. Moreover, the LIBET method acknowledges metacognitive processes as the results of childhood experiences that greatly affect individual emotional and cognitive development (Pournaghash-Tehrani & Feizabadi, 2009). Every item was assessed on a visual analogue scale whose length was 10 cm, and only three items that referred to alternative strategies had reverse scores. The LIBET-Q has a total of 18 items; six refer to life themes (LTs), and 12 refer to life plans (LPs). The scoring procedure consisted of summing items LT1, LT2, and LT3 to obtain a total score for the “Conditioning about theme” subscale, and items LT4, LT5, and LT6 were summed to achieve a score for “Intolerability.” For the second part, items that had to be added were: LP1, LP2, LP3, and LP4 for the “Conditioning about plans” subscale, and items LP5, LP6, LP7, and LP8 for the “Utility” subscale. Finally, items LP9(r), LP10(r), LP11(r), and LP12 were summed for the “Uncontrollability” subscale.
Participants
A total of 396 participants (44.4% males, 55.6% females) aged between 18 and 71 (M = 34.82, SD = 10.32) were recruited for this study. Demographic and clinical information are reported in Table 1. The Research Ethics Committee of the Sigmund Freud University of Vienna approved the study (Ref. ECHVDR6DBGUCQ589682). To compare exploratory and confirmatory factor analyses, participants were randomly grouped into two samples. Table 1 shows sociodemographic features and diagnoses of the groups. The LIBET-Q was developed to reach a sufficient comprehension and sharing of patients’ symptoms and vulnerabilities, so a clinical sample was considered the most adequate to validate it. This choice was in line with the previous article about LIBET-Q validation (Sassaroli et al., 2021).
Procedure
Participants were recruited from 2017 to 2022 at the Studi Cognitivi Clinical and Research Center in Modena, Italy. They accessed the clinic asking for help for mental health problems such as anxiety, depression, or relational troubles. After the first session with a senior clinician, they were asked to attend two sessions of psychodiagnostic assessment with psychotherapists of the Psychodiagnostics Assessment Group (PAG). Each therapist in the PAG had at least 4 years of training in CBT and followed a 2-h training in administering the LIBET-Q. A. O. was a psychotherapist and supervisor of the PAG during recruitment.
During the first session, the interviewer administered the Structured Clinical Interview for DSM-5, Clinical Version (SCID-5-CV). Throughout the second assessment session, the interviewer administered the Structured Clinical Interview for DSM-5, Personality Disorders (SCID-5-PD) and the LIBET-Q. At the end of this session, the interviewer described research projects of the center and asked for participation. After informed consent was obtained, the data referring to the participant were anonymized and then included in a database. If participants did not give their consent, assessment went on as usual. Participation in the research did not change the assessment procedure of the clinic but simply allowed the interviewer to use anonymized data for research purposes.
Materials
Life Themes and Semi-adaptive Plans: Implications of Biased Beliefs, Elicitation, and Treatment-Questionnaire (LIBET-Q)
The LIBET-Q is a structured interview composed of two sections. Section “Case Formulation in Cognitive-Behavioral Therapy” contains a familiarization item and two multiple-choice questions. The first question is about LTs (life themes). Patients are asked to choose three words that describe their most negative mental states. The second question is about LPs (life plans), and patients are asked to select three strategies that they use more often when they are emotionally activated. The validation data for Sect. “Case Formulation in Cognitive-Behavioral Therapy” can be found in a previous article (Sassaroli et al., 2021). Section “The LIBET Method as a Tool for Case Conceptualization and Treatment Formulation” is aimed at identifying patients’ beliefs and processes about their LTs and plans, and it is composed of 18 items. The final version of the LIBET-Q is included in Supplementary Information.
Structured Clinical Interview for DSM-5, Personality Disorder (SCID-5-PD)
The SCID-5-PD is a structured interview to assess personality disorders according to DSM-5 criteria. The interview is usually preceded by a 119-item questionnaire that is a screening tool to help clinicians in selecting personality traits for deep investigation. SCID-5-PD administration can last from 60 to 120 min. The categorical PD diagnoses obtained from the SCID-5-PD showed good inter-rater reliability in an Italian sample (median κ value = 0.89, SD = 0.11; Somma et al., 2017).
Structured Clinical Interview for DSM-5, Clinical Version (SCID-5-CV)
The SCID-5-CV is a structured interview that investigates several categories of diagnoses based on the DSM-5, such as mood disorders, addictions, eating disorders, bipolar, related disorders, and others. Its administration usually takes 45–90 min (Shabani et al., 2021).
Beck Anxiety Inventory (BAI)
The BAI (Beck et al., 1988) is a self-report questionnaire composed of 21 items rated on a 4-point Likert scale. It aims to assess state anxiety by asking people to indicate the frequency of symptoms during the prior week. Scores range from 0 to 63, and a total score above 7 indicates significant levels of anxiety. The Italian version of the BAI showed good internal consistency, with a Cronbach’s α of 0.87 (Sica & Ghisi, 2007).
Beck Depression Inventory II (BDI-II)
The BDI-II (Beck & Steer, 1993) is a widely used measure of depression. It is a self-report questionnaire of 21 items rated on a 4-point Likert scale. It assesses depressive symptoms from the prior two weeks. Total scores range from 0 to 63, and a score of 10 or above means the presence of depressive symptoms. The Italian version of the BDI-II possesses good psychometric properties (Cronbach’s α = 0.80; Sica & Ghisi, 2007).
Clinical Outcomes in Routine Evaluation, Outcomes Measure (CORE-OM)
The CORE-OM (Evans et al., 2000) consists of 34 items rated on a 5-point Likert scale. Items investigate four areas: subjective wellbeing, problems/symptoms, life functioning, and risk of harming oneself and others. Respondents are asked to give answers by thinking about the prior 7 days. An Italian validation of the CORE-OM showed good internal consistency, with a Cronbach’s α index > 0.90 for the total score and > 0.70 for each domain (Palmieri et al., 2009).
Statistics
First, an inspection of the distribution of data was executed to assess their normality. No missing data were allowed in order to perform confirmatory factor analyses using AMOS (Version 27). The entire sample was randomly split into two subsamples to perform exploratory and confirmatory factor analyses. The exploratory factor analysis (EFA) with principal components method was performed on Sample 1 (n = 189) to verify the number of latent variables. The Keiser-Meyer-Olkin (KMO) test evaluated the adequacy of sample size; Bartlett’s sphericity test was used to test inter-correlations between items. Factor extraction was based on eigenvalues, keeping any factor with an eigenvalue of 1.0 or higher. An oblique rotation (Promax) was chosen to admit a correlation between factors. A confirmatory factor analysis (CFA) was then performed on Sample 2 (n = 207), comparing different goodness of fit indices. The root-mean-square-residual error of approximation (RMSEA) is considered a good index of fit with values less than 0.80 (Browne & Cudeck, 1993). The comparative fit index (CFI) with a value equal or greater than 0.90 represents a “good fit” index, such as the Tucker-Lewis index (TLI) (Oppo et al., 2019).
Internal coherence was tested on the entire sample (n = 396) and analyzed for each of the four factors resulting from the EFAs and CFAs. Item analyses were run using adjusted item-total correlations. Cronbach’s alpha was used to test internal coherence. The decrease of Cronbach’s alpha was inspected for all items, referring to their factor. Concurrent validity was also tested on the entire sample using correlational analyses with other measures of depression (BDI-II), anxiety (BAI), and outcomes indicators (CORE-OM). Finally, an Analysis of Variance (ANOVA) with Bonferroni correction was performed to analyze differences in LIBET-Q scores between different clinical population groups.
Statistics were performed using IBM’s SPSS (Version 27) for descriptives, EFA, internal coherence, concurrent validity, and analyses of variance. CFAs were conducted using the AMOS macro for SPSS.
Results
Descriptive Statistics
Tables 1 and 2 show sociodemographic and clinical features of the samples. Table 1 lists all diagnoses obtained by the SCID-5-CV and SCID-5-PD interviews and comorbidities in samples 1 and 2. Differences between the two samples were tested with chi-squared tests, which confirmed the equality between samples for each variable. Table 2 shows means and standard deviations of the self-report questionnaires and 18 original items on the LIBET-Q. An inspection of kurtosis and skewness was accomplished to verify the normality of distribution, and all values were approximately between − 1 and 1. A Student’s t-test was performed to assess differences between samples. In two cases (LT6 and LP2), significant differences emerged. The effect sizes with Cohen’s d were then examined, and its values were found acceptable (LT6, d = 0.33; LP2, d = 0.28).
LIBET-Q Factorial Structure
Exploratory Factor Analysis (EFA)
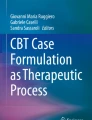
For the 18 items of the LIBET-Q tested, the KMO test was, 83, which is a good index of non-unique covariance among items. Bartlett’s test of sphericity was significant (χ2 = 2781.91, df = 14, p < 0.001), so factor analysis with orthogonal rotation (Promax) was performed. Four factors (conditioning, utility, painfulness, and alternative strategies) were extracted, accounting for 61.37% of the variance. Because of the cross-loading of item LP12 on both factor 1 (0.32) and 3 (0.55), the EFA was replicated excluding item LP12. The four- factor structure was confirmed, and explained variance increased to 63.43%. Factor 1, labelled Interference/Irrelevance, accounted for 29.44% of the total explained variance; Factor 2, Necessity/Option, accounted for 17.23%; Factor 3, Dangerous/Unpleasant, accounted for 9.54%; and Factor 4, Presence/Absence of alternative strategies, accounted for 7.22%. This structure was also confirmed by inspections of scree plots (Fig. 1). Item LP12 (I am required to act these behaviors) was then removed from further analyses. Table 3 shows the results of the item-factor loadings. Promax rotation allowed for inter-correlations: Among emerging factors, only Factor 1 (Interference/Irrelevance) and Factor 3 (Dangerous/Unpleasant) resulted in a significant relationship (0.49).

Screeplot exploratory factor analysis
Confirmatory Factor Analysis (CFA)
A CFA was run on Sample 2 (n = 207). Different goodness of fit indices were used and compared to identify the most adequate model for the LIBET-Q. Model 1 was designed according to the authors’ theorization, which resulted in five domains (corresponding to five processes): two referred to LTs (life themes) (conditioning and painfulness), and three referred to plans (conditioning, utility, alternative strategies). Model 2 was calculated from the first tested EFA, with four factors and 18 items included. Model 3 was constituted from the same four factors of Model 2, but without item LP12. Model 3 was the best model according to the goodness of fit indices considered (Table 4). Figure 2 shows the factor structure of the LIBET-Q.

Confirmatory factor analysis of LIBET-Q
Psychometric Properties of the LIBET-Q
Internal Consistency
Internal consistency for each factor was evaluated with Cronbach’s α, analyzing both samples 1 and 2 and the entire sample. Results are presented in Table 5. Considering the entire sample, Cronbach’s α was good for each factor (Factor 1: Interference/Irrelevance, Cronbach’s α = 0.87; Factor 2: Necessity/Option, Cronbach’s α = 0.83; Factor 3: Dangerous/Unpleasant, Cronbach’s α = 0.76; Factor 4: Presence/Absence of alternative strategies, Cronbach’s α = 0.68).
Convergent Validity
Convergent validity of the LIBET-Q was assessed via correlations with other measures. Results using Pearson’s coefficient are shown in Table 6. Every LIBET-Q factor was significantly correlated with all other measures, except for Factor 2 (Necessity/Option), which was not correlated with anxiety or self/other damage risk measured with the CORE-OM. Higher values of correlation were found for factors 1 and 3 (Interference/Irrelevance, Dangerous/Unpleasant). A closer look into these correlations was performed to understand if one of the four factors was more linked to subjective distress. We calculated percentiles of BDI-II items and then analyzed correlations again. Results showed that Factor 2 (Necessity/Option) had a negative correlation with depression (r = -0.14, p < 0.01). Factor 1 (Interference/Irrelevance) had a strong positive correlation (r = 0.43, p < 0.001), like Factor 3 (Dangerous/Unpleasant, r = 0.35, p < 0.001). Factor 4 (Presence/Absence of alternative strategies) had a significant, albeit lower, positive correlation with depression (r = 0.26, p < 0.001).
Profiling Patients with LIBET-Q Items
An ANOVA with Bonferroni correction (significant value considered 0.05) was performed to identify commonalities and differences in LIBET-Q values between different clinical population groups. Thus, we split our sample into four groups: patients without diagnosis; patients with one or more diagnoses obtained with the SCID-5-CV; patients with one or more personality disorder(s); and patients with comorbidities between at least one personality disorder (PD) and other disorder(s). Results from the ANOVA revealed significant differences in distribution for Interference/Irrelevance (F = 16.997; df = 3; p = 0.000; η2 = 0.072), Dangerous/Unpleasant (F = 10.134; df = 3; p = 0.000; η2 = 0.115), and Presence/Absence of alternative strategies (F = 4.572; df = 3; p = 0.004; η2 = 0.034), but not for Necessity/Option (F = 0.124; df = 3; p = 0.946; η2 = 0.001). A Bonferroni correction was performed to analyze differences between groups more specifically. Figure 3 shows means and standard errors for each group considered. Factor 1 (Interference/Irrelevance) was significantly different between patients without a diagnosis and patients with at least one diagnosis from the SCID-5-CV. However, Interference/Irrelevance did not change for patients with a PD. Factor 2 (Necessity/Option) did not change between groups. Factor 3 (Dangerous/Unpleasant) reflected differences between patients without diagnoses and patients with at least one diagnosis from the SCID-5-CV, but not with patients diagnosed with a PD. Factor 4 (Presence/Absence of alternative strategies) underlined differences only between patients with both a diagnosis from the SCID-5-CV and a PD and patients without diagnoses. No differences between the other groups were found.

Differences between groups
Discussion
The LIBET-Q is a feasible instrument aimed to investigate the LIBET conceptualization of a patient’s situation. The first part of the LIBET-Q revealed a three-themes, three-plans structure (Sassaroli et al., 2021). The present study aimed to validate the second part of the LIBET-Q, which analyses the metacognitive processes about LTs (life themes) and LPs (life plans). Originally, the authors identified two metacognitive processes that referred to themes (conditioning and painfulness) and three that referred to plans (conditioning, utility, and alternative strategies). Both exploratory and CFAs confirmed a four-factor model, with conditioning about themes and about plans collapsed into one single factor. Taken together, the four factors explained 63.43% of the variance. Goodness of fit indexes confirmed the adequacy of the model. The loading of each item on the corresponding factor represented good construct validity. This four-factor model is in line with the metacognitive prospect of psychological distress (Wells, 2008).
The scoring procedure was slightly changed from the original version: item LP12 (I am required to act these behaviors) was not included, and future versions of the LIBET-Q will not report it. Moreover, the original subscales “Conditioning about themes” and “Conditioning about plans” must be summed and considered as a total score. From a clinical perspective, it can be useful to independently contemplate the amount of conditioning perceived from LTs and LPs to both explain more specifically causes and maintaining factors of distress to patients and plan therapeutic interventions aimed to reduce symptoms. However, our data did not discriminate regarding the content of items, and, from a theoretical point of view, present findings support the process-based theorization (Ruggiero, 2011).
The results (partially) confirm the five original variables. These variables characterize LIBET-monitoring in terms of the process of the course of therapy, and they definitively establish the LIBET therapeutic “contract” and the work alliance between patient and therapist in a LIBET-method framework. This is a contract that encourages the patient to work on the interference and danger perceived from the LT and on the necessity, interference, and absence of alternative strategies linked to the semi-adaptive LP. Based on this contract, the therapeutic intervention agenda can be discussed, and its rationale justified. For this purpose, a re-definition of processes was determined: Conditioning was modified on the Interference/Irrelevance (I/I) axis, painfulness on the Dangerous/Unpleasant (D/U) axis, utility on the Necessity/Option (N/O) axis, and uncontrollability on the Presence/Absence of alternative strategies (P/A) axis. This new way to consider metacognitive processes allows clinicians to openly share with patients not only the case conceptualization but also the therapeutic formulation by underlining the justification and direction for the recommended therapeutic intervention.
Correlation between LIBET-Q factors and other measures (i.e., CORE-OM subscales) suggests the importance of metacognitive processes. Almost all the LIBET-Q factors correlated with depression, anxiety, and global wellbeing. The I/O and D/U axes had the highest correlation: In line with results mentioned above, these factors could reflect the symptomatic status of patients.
Metacognitive processes investigated with the LIBET-Q can also identify patients’ profiles and help clinicians improve their understanding of patients’ awareness of their situation. The same level of conditioning is perceived by the group of patients without diagnoses and patients with a PD but without other disorders. The ego-syntonic nature of PD can explain this phenomenon: ego-syntonicity implies consistency between personality functioning and goals and/or self-concepts (Hart et al., 2018). Our data corroborated the importance of perceived distress as an indicator of insight, necessary to discuss one’s functioning; this is in line with previous findings for obsessive–compulsive disorder (Summerfeldt, 2007), but more studies are necessary to explore ego-dystonic symptoms among other disorders. Also, the D/U factor distinguished between people with at least one disorder diagnosed with the SCID-5-CV. Items which loaded on this factor were specifically referred to as LTs; those considered as interfering and dangerous can cause distress, which people attempt to manage with plans. Usually, LPs are effective in the short term, or in absence of high-risk situations, like exposure to events that trigger LT-related beliefs or feelings (Sassaroli et al., 2016). When long-term disadvantages of plans are perceived, or plans come out as inadequate because of environmental changes that affect its closeness to a LT, the D/U scale increased towards the “dangerous” side of the factor (Ruggiero & Sassaroli, 2012). The N/O factor is composed of items referring to plans, and this measurement did not change between groups. This can be explained by the nature of our study design, which saw data collected at a clinical center. People that ask for help could be conscious about their plans’ limits, even if their distress is not diagnosable. The process measured by P/A of alternative strategies factor discriminated between subjects with both a diagnosis from the SCID-5-CV and a PD and people without diagnoses. The concurrent presence of two (or more) diagnoses in different psychopathological areas could alter the ability to access different ways of coping with distress (Thase, 1996). The ability of the LIBET processes investigated to discriminate between different clinical populations underlines the role of metacognition as a possible superordinate construct, independent from a specific diagnosis and strictly linked to ideas about self and one’s functioning (Harvey et al., 2004).
Having a valid and reliable instrument to measure these processes is significant for different reasons. First, during assessment, the LIBET-Q can help clinicians discriminate levels of metacognitive awareness perceived by patients. An increase in one or more factors can suggest which kinds of clinical problems are present. Second, the LIBET-Q can identify one or more areas to address during therapy, such as the need to increase a patient’s ability to find alternative strategies. These goals can be achieved with different therapeutic approaches because the LIBET model is aimed to reveal problems, related goals, and possibilities, and it is not anchored to a specific treatment (Ruggiero & Sassaroli, 2012). Moreover, the LIBET-Q can overcome a limit which is common to most case conceptualization tools: the need to collect and organize several relevant episodes prior to being able to share a consistent formulation (Eells, 2007).
Granted, the present study has limitations. Factor 4 (P/A of alternative strategies) includes an item (LP9, I feel free to do something different) whose removal can increase the Cronbach’s alpha. The choice to keep the element in the instrument is linked to the low number of items and the limited relevance of consistency gain. Because of the archival nature of data collection, the present study did not use measures to investigate divergent validity, which could have explained the specificity of elements assessed with the LIBET-Q. The clinical sample was chosen to first-off validate the LIBET-Q with the population it was made for. However, the heterogeneity of the diagnoses detected in our samples implies challenges in clearly analyzing relations between LIBET components and psychopathological elements. Moreover, the comparison with a non-clinical group could better explain the specificity of patients in LIBET conceptualizations. To achieve this goal, future studies might conduct analyses with non-clinical samples to better investigate commonalities and differences. Other studies might include the exploration of the possibility of better representing the process approach also in item descriptions by joining questions about plans and themes in fewer elements referring more explicitly to metacognition. Moreover, item-response techniques could be implemented in data analyses to deeply investigate the role of specific metacognitive components. A longitudinal study with the LIBET-Q would have to be conducted to verify the sensitivity of the instrument to a patient’s changes during therapy, and to explore if there would be any differences in metacognitive process. Finally, a LIBET-Q therapist-report version could be created and administered to evaluate commonalities and differences between patients’ and clinicians’ perspectives on LTs and metacognitive processes. Also, it might be useful to see if the patients’ and clinicians’ versions of the LIBET-Q show differences at the beginning of the treatment, and how many sessions are necessary to fit them together conceptualizations. This could be achieved also with the LIBET-Q, and it could reflect a measure of working alliance.
Overall, the LIBET-Q, as a whole with its two sections, appears to be a feasible measure for case conceptualization. Being a brief tool, it gathers a lot of information. It can easily reveal a negative mental status (in terms of LTs) and provide semi-adaptive strategies to deal with them in an immediate way, through the use of multiple-choice items with verbal triggers. After this investigation, the clinician can guide the patient to an exploration of pathological elements, which can be described as “maladaptive metacognitive processes.” During treatment, the second section of the LIBET-Q can be re-administered to suggest to patients any modifications of their metacognitive processes by using the bipolar axis explanation. Also, an unwillingness to modify processes can reveal resistances or vulnerabilities that can be addressed to increase the odds of a satisfying therapy outcome.
Data Availability
The data that support the findings of this study are not openly available due to reasons of sensitivity. Located in controlled-access data storage at the Studi Cognitivi Clinical and Research Centre, the data are available from the corresponding author upon reasonable request.
References
Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84, 191–215. https://doi.org/10.1037/0033-295X.84.2.191
Bandura, A. (1988). Self-efficacy conception of anxiety. Anxiety and self-focused attention (pp. 89–110). Routledge.
Bannister, D., & Fransella, F. (1971). Inquiring man: The psychology of personal constructs (3rd ed.). Penguin.
Beck, A. T. (1976). Cognitive therapies and emotional disorders. International Universities Press.
Beck, A. T. (1996). Beyond belief: A theory of modes, personality, and psychopathology. In P. M. Salkovskis (Ed.), Frontiers of cognitive therapy (pp. 1–26). The Guilford Press.
Beck, A. T. (2008). The evolution of the cognitive model of depression and its neurobiological correlates. American Journal of Psychiatry, 165(8), 969–977. https://doi.org/10.1176/appi.ajp.2008.08050721
Beck, A. T., & Bredemeier, K. (2016). A unified model of depression: Integrating clinical, cognitive, biological, and evolutionary perspectives. Clinical Psychological Science, 4, 596–619. https://doi.org/10.1177/2167702616628523
Beck, A. T., Emery, G., & Greenberg, R. L. (1985). Anxiety disorders and phobias: A cognitive perspective. Basic Books.
Beck, A. T., Epstein, N., Brown, G., & Steer, R. A. (1988). An inventory for measuring clinical anxiety: Psychometric properties. Journal of Consulting and Clinical Psychology, 56, 893–897. https://doi.org/10.1037/0022-006X.56.6.893
Beck, A. T., Rush, A. J., Shaw, B. F., & Emery, G. (1979). Cognitive therapy of depression. Guilford Press.
Beck, A. T., & Steer, R. A. (1993). Manual for the Beck depression inventory. The Psychological Corporation.
Beck, J. S. (2011). Cognitive behavior therapy: Basics and beyond. Guilford Publications.
Browne, M. W., & Cudeck, R. (1993). Alternative ways of assessing model fit. In K. A. Bollen & J. S. Long (Eds.), Testing structural equation models (pp. 136–162). Sage Publications.
Bruner, J. (1973). Going beyond the information given. Norton.
Bucci, S., French, L., & Berry, K. (2016). Measures assessing the quality of case conceptualization: A systematic review. Journal of Clinical Psychology, 72(6), 517–33. https://doi.org/10.1002/jclp.22280
Capo, R., & Mancini, F. (2008). Scopi terminali, temi di vita e psicopatologia [Terminal goals, life themes and psychopathology]. In C. Perdighe & F. Mancini (Eds.), Elementi di Psicoterapia Cognitiva: II edizione [Elements of cognitive psychotherapy: second edition] (pp. 39–68). Fioriti.
Capo, R., Mancini, F., & Barcaccia, B. (2010). Temi di vita e psicopatologia [Life themes and psychopathology]. In A. Pacciolla & F. Mancini (Eds.), Cognitivismo Esistenziale: Dal Significato del Sintomo al Significato della Vita [Existential cognitivism: From the meaning of the symptom to the meaning of life] (pp. 202–226). Franco Angeli.
Clark, D. A., & Beck, A. T. (2010). Cognitive therapy of anxiety disorders: Science and practice. Guilford Press.
Critchfield, K. L., Levy, K. N., Clarkin, J. F., & Kernberg, O. F. (2008). The relational context of aggression in borderline personality disorder: Using adult attachment style to predict forms of hostility. Journal of Clinical Psychology, 64, 67–82. https://doi.org/10.1002/jclp.20434
Csikszentmihalyi, M., & Beattie, O. V. (1979). Life themes: A theoretical and empirical exploration of their origins and effects. Journal of Humanistic Psychology, 19, 45–63.
Di Fini, G., & Veglia, F. (2019). Life themes and attachment system in the narrative self-construction: Direct and indirect indicators. Frontiers in Psychology, 10, 1393–1406. https://doi.org/10.3389/fpsyg.2019.01393
DiGiuseppe, R. A., DiGiuseppe, R., Doyle, K. A., Dryden, W., & Backx, W. (2013). A practitioner’s guide to rational-emotive behavior therapy. Oxford University Press.
DiGiuseppe, R., & Tafrate, R. C. (2007). Understanding anger disorders. Oxford University Press.
Dobson, K. S., Poole, J. C., & Beck, J. S. (2018). The fundamental cognitive model. In R. L. Lehay (Ed.), Science and practice in cognitive therapy: Foundations, mechanisms, and applications (pp. 29–47). Guilford Publications.
Dodet, M. (2010). Self meaning e tema di vita [Self meaning and life theme]. In A. Pacciolla & F. Mancini (Eds.), Cognitivismo Esistenziale: Dal Significato del Sintomo al Significato della Vita [Existential cognitivism: From the meaning of the symptom to the meaning of life] (pp. 148–169). Franco Angeli.
Easden, M. H., & Kazantzis, N. (2017). Case conceptualization research in cognitive behavior therapy: A state of the science review. Journal of Clinical Psychology, 74(3), 356–384. https://doi.org/10.1002/jclp.22516
Eells, T. D. (2007). Handbook of psychotherapy case formulation. Guilford Press.
Ellis, A. (1962). Reason and emotion in psychotherapy. Lyle Stuart.
Ellis, A. (1994). Reason and emotion in psychotherapy: Revised and updated. Kensington Publishers.
Evans, C., Mellor-Clark, J., Margison, F., Barkham, M., McGrath, G., Connell, J., & Audin, K. (2000). CORE: Clinical outcomes in routine evaluation. Journal of Mental Health, 9(3), 247–255. https://doi.org/10.1080/713680250
Feixas, G., & Miró, M. (1993). Aproximaciones ala Psicoterapia una Introducción a los Tratamientos Psicológicos [Approaches to psychotherapy. An introduction to psychological treatments]. Paidós.
Flavell, J. (1979). Metacognition and cognitive monitoring: A new area of cognitive-developmental inquiry. American Psychologist, 34(10), 906–911. https://doi.org/10.1037/0003-066X.34.10.906
Frankl, V. (2006). Man’s search for meaning. An introduction to logotherapy. Originally published in 1946. Beacon Press.
Gresham, F. (1985). Behavior disorder assessment: Conceptual, definitional and practical considerations. School Psychology Review, 14, 495–509.
Guidano, V. F. (1987). Complexity of the Self. Guilford Press.
Guidano, V. F. (1991). The self in process: Toward a post-rationalist cognitive therapy. Guilford Press.
Guidano, V., & Liotti, G. (1983). Cognitive processes and emotional disorders: A structural approach to psychotherapy. Guilford Press.
Hart, W., Tortoriello, G. K., & Richardson, K. (2018). Are personality disorder traits ego-syntonic or ego-dystonic? Revisiting the issue by considering functionality. Journal of Research in Personality, 76, 124–128. https://doi.org/10.1016/j.jrp.2018.08.001
Harvey, A. G., Watkins, E., & Mansell, W. (2004). Cognitive behavioural processes across psychological disorders: A transdiagnostic approach to research and treatment. Oxford University Press.
Hayes, S. C., & Hofmann, S. G. (Eds.). (2018). Process-based CBT: The science and core clinical competencies of cognitive behavioral therapy. New Harbinger Publications.
Haynes, S. N., Spain, E. H., & Oliveira, J. (1993). Identifying causal relations in clinical assessment. Psychological Assessment, 5, 281–291. https://doi.org/10.1037/1040-3590.5.3.281
Jaspers, K. (1971). Philosophy of existence. University of Pennsylvania Press.
Johnstone, L., & Dallos, R. (2013). Formulation in psychology and psychotherapy: Making sense of people’s problems. Routledge.
Johnstone, L., Whomsley, S., Cole, S., & Oliver, N. (2011). Good practice guidelines on the use of psychological formulation. British Psychological Society. https://doi.org/10.53841/bpsrep.2011.rep100
Kazantzis, N., Dattilio, F. M., & Dobson, K. S. (2017). The therapeutic relationship in cognitive behavior therapy: A clinician’s guide to the heart and soul of effective practice. Guilford Publications.
Kukyen, W., Padesky, C., & Dudley, R. (2008). The science and practice of case conceptualization. Behavioural and Cognitive Psychotherapy, 36(6), 757–768. https://doi.org/10.1017/S1352465808004815
Kuyken, W., Fothergill, C. D., Musa, M., & Chadwick, P. (2005). The reliability and quality of cognitive case formulation. Behaviour Research and Therapy, 43, 1187–1201. https://doi.org/10.1016/j.brat.2004.08.007
Lazarus, A. (1976). Multi-modal behavior therapy. Springer.
Linehan, M. M. (2015). DBT® skills training: Manuale [DBT® skills training: Manual]. Raffaello Cortina.
Lorenzini, R., & Sassaroli, S. (1995). Attaccamento, Conoscenza e Disturbi di Personalità [Attachment, knowledge and personality disorders]. Raffaello Cortina Editore.
Mahoney, M. J. (1974). Cognition and behavior modification. Ballinger.
Mahoney, M. J. (1991). Human Change process. Basic Books.
Mahoney, M. J. (2003). Constructive psychotherapy: A practical guide. Guilford Press.
Mansell, W., Harvey, A., Watkins, E. R., & Shafran, R. (2008). Cognitive behavioral processes across psychological disorders: A review of the utility and validity of the transdiagnostic approach. International Journal of Cognitive Therapy, 1(3), 181–191. https://doi.org/10.1680/ijct.2008.1.3.181
Markus, H. (1977). Self-schemata and processing information about the self. Journal of Personality and Social Psychology, 35, 63–78. https://doi.org/10.1037/0022-3514.35.2.63
Martin, R. C., & Dahlen, E. R. (2005). Cognitive emotion regulation in the prediction of depression, anxiety, stress, and anger. Personality and Individual Differences, 39, 1249–1260. https://doi.org/10.1016/j.paid.2005.06.004
Meehl, P. E. (1962). Schizotaxia, schizotypy, schizophrenia. American Psychologist, 17(12), 827–838. https://doi.org/10.1037/h0041029
Meichenbaum, D. H. (1977). Cognitive behavior modification. Plenum Press.
Neimeyer, R. A. (2009). Constructivist psychotherapy. Routledge.
Neimeyer, R. A., & Mahoney, M. J. (Eds.). (1995). Constructivism in psychotherapy. American Psychological Association.
Neisser, U. (1967). Cognitive psychology. Prentice-Hall.
Oppo, A., Prevedini, A. B., Dell’Orco, F., Dordoni, P., Presti, G., Gillanders, D. T., & Moderato, P. (2019). Fusione e Defusione. Adattamento e proprietà psicometriche della versione italiana del cognitive fusion questionnaire (I-CFQ) [Fusion and defusion. Adaptation and psychometric properties of the Italian version of the cognitive fusion questionnaire (I-CFQ)]. Psicoterapia Cognitiva e Comportamentale, 25(1), 53–73.
Padesky, C. A., & Mooney, K. (1990). Clinical tip: Presenting the cognitive model to clients. International Cognitive Therapy Newsletter, 6, 13–14.
Palmieri, G., Evans, C., Hansen, V., Brancaleoni, G., Ferrari, S., Porcelli, P., Reitano, F., & Rigatelli, M. (2009). Validation of the Italian version of the clinical outcomes in routine evaluation outcome measure (CORE-OM). Clinical Psychology & Psychotherapy: An International Journal of Theory & Practice, 16(5), 444–449. https://doi.org/10.1002/cpp.646
Panksepp, J., & Watt, D. (2011). Why does depression hurt? Ancestral primary-process separation-distress (PANIC/GRIEF) and diminished brain reward (SEEKING) processes in the genesis of depressive affect. Psychiatry Interpersonal & Biological Processes, 74(1), 5–13. https://doi.org/10.1521/psyc.2011.74.1.5
Persons, J. B. (1989). Cognitive therapy in practice: A case formulation approach. W W Norton & Co.
Pournaghash-Tehrani, S., & Feizabadi, Z. (2009). Predictability of physical and psychological violence by early adverse childhood experiences. Journal of Family Violence, 24, 417–422. https://doi.org/10.1007/s10896-009-9245-4
Ridley, C. R., Jeffrey, C. E., & Roberson, R. B., 3rd. (2017). Case mis-conceptualization in psychological treatment: An enduring clinical problem. Journal of Clinical Psychology, 73(4), 359–375. https://doi.org/10.1002/jclp.22354
Ruggiero, G. M. (2011). Terapia cognitiva: Una Storia Critica [Cognitive psychotherapy: A critical history]. Raffaello Cortina.
Ruggiero, G. M., Caselli, G., & Sassaroli, S. (2018). Laicizzare la relazione terapeutica in psicoterapia cognitivo-comportamentale: La formulazione condivisa del caso [Secularising the therapeutic relationship in cognitive behavioural therapy: Shared case formulation]. Psicoterapia Cognitiva e Comportamentale, 24, 203–222.
Ruggiero, G. M., & Sassaroli, S. (2012). Il Colloquio in Psicoterapia Cognitiva: Tecnica e Pratica Clinica [The cognitive psychotherapy session: Clinical technique and practice]. Raffaello Cortina.
Salkovskis, P. M. (1985). Obsessive-compulsive problems: A cognitive-behavioural analysis. Behaviour Research and Therapy, 23, 571–583. https://doi.org/10.1016/0005-7967(85)90105-6
Salkovskis, P. M. (1991). The importance of behaviour in the maintenance of anxiety and panic: A cognitive account. Behavioural Psychotherapy, 19, 6–19. https://doi.org/10.1017/S0141347300011472
Sassaroli, S., Caselli, G., Mansueto, G., Palmieri, S., Pepe, A., Veronese, G., & Ruggiero, G. M. (2021). Validating the diathesis-stress model based case conceptualization procedure in cognitive behavioral therapies: The LIBET (life themes and semi-adaptive plans: Implications of biased beliefs, elicitation, and treatment) procedure. Journal of Rational-Emotive & Cognitive-Behavior Therapy, 40(3), 527–565. https://doi.org/10.1007/s10942-021-00421-3
Sassaroli, S., Caselli, G., & Ruggiero, G. M. (2016). A clinical cognitive model of verification and case conceptualisation: Life themes and plans implications of biased beliefs: Elicitation and treatment (LIBET). Psicoterapia Cognitiva e Comportamentale, 22(2), 183–197.
Sassaroli, S., Lorenzini, R., & Ruggiero, G. M. (2005). Kellian invalidation, attachment and the construct of “control.” In D. A. Winter & L. L. Viney (Eds.), Personal construct psychotherapy. Advances in theory, practice and research (pp. 34–42). Whurr Publishers.
Schore, A. N. (2012a). The science of the art of psychotherapy. Norton & Company Inc.
Schore, A. N. (2012). Bowlby’s environment of evolutionary adaptedness. Recent studies on the interpersonal neurobiology of attachment and emotional development. In D. Narvaez, J. Panksepp, A. N. Schore, & T. R. Gleason (Eds.), Evolution, early experience and human development from research to practice (pp. 31–73). Oxford University Press.
Shabani, A., Masoumian, S., Zamirinejad, S., Hejri, M., Pirmorad, T., & Yaghmaeezadeh, H. (2021). Psychometric properties of structured clinical interview for DSM-5 disorders-clinician version (SCID-5-CV). Brain and Behavior, 11(5), e01894. https://doi.org/10.1002/brb3.1894
Sica, C., & Ghisi, M. (2007). The Italian versions of the Beck anxiety inventory and the Beck depression inventory-II: Psychometric properties and discriminant power. In M. A. Lange (Ed.), Leading-edge psychological tests and testing research (pp. 27–50). Nova Science Publishers.
Somma, A., Borroni, S., Maffei, C., Besson, E., Garbini, A., Granozio, S., Limuti, B., Perego, G., Pietrobon, A., Rugi, C., Turano, E., & Fossati, A. (2017). Inter-rater reliability of the Italian translation of the structured clinical interview for DSM-5 personality disorders (SCID-5-PD): A study on consecutively admitted clinical adult participants. Journal of Psychopathology, 23(3), 105–111.
Spada, M. M., Caselli, G., & Wells, A. (2013). A triphasic metacognitive formulation of problem drinking. Clinical Psychology & Psychotherapy, 20(6), 494–500. https://doi.org/10.1002/cpp.1791
Summerfeldt, L. J. (2007). Treating Incompleteness, ordering, and arranging concerns. In M. M. Antony, C. Purdon, & L. J. Summerfeldt (Eds.), Psychological treatment of obsessive-compulsive disorder: Fundamentals and beyond (pp. 187–207). American Psychological Association.
Thase, M. E. (1996). The role of Axis II comorbidity in the management of patients with treatment-resistant depression. Psychiatric Clinics of North America, 19(2), 287–309. https://doi.org/10.1016/s0193-953x(05)70289-6
Thwaites, R., & Freeston, M. H. (2005). Safety-seeking behaviours: Fact or function? How can we clinically differentiate between safety behaviours and adaptive coping strategies across anxiety disorders? Behavioural and Cognitive Psychotherapy, 33(2), 177–188. https://doi.org/10.1017/S1352465804001985
Wells, A. (2000). Emotional disorders and metacognition: Innovative cognitive therapy. Wiley.
Wells, A. (2008). Metacognitive therapy for anxiety and depression. Guilford Press.
Wells, A. (2013). Metacognitive therapy. In K. T. Mueser, J. D. Gottlieb, & S. Gingerich (Eds.), Social skills and problem-solving training. The Wiley handbook of cognitive behavioral therapy (pp. 243–272). Wiley.
Winter, D. A., & Viney, L. L. (Eds.). (2005). Personal Construct psychotherapy. Advances in theory, practice and research. Whurr Publishers.
Young, J. E., Klosko, J. S., & Weishaar, M. (2003). Schema therapy: A practitioner’s guide. Guilford.
Funding
This research received no specific grant from any funding agency.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors report no conflicts of interest.
Ethical Approval
Ethical approval for the study was granted by the Sigmund Freud University Ethics Commission (Ref. ECHVDR6DBGUCQ589682), and all participants provided written informed consent.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Offredi, A., Oppo, A., Ruggiero, G.M. et al. Validation of Process-Based Components of the LIBET-Q: An Innovative Instrument for Case Conceptualization. J Rat-Emo Cognitive-Behav Ther (2024). https://doi.org/10.1007/s10942-024-00542-5
Accepted:
Published:
DOI: https://doi.org/10.1007/s10942-024-00542-5