
Abstract
While metacognitive interventions are gaining attention in the treatment of various mental disorders, a review of the literature showed that the term is often defined poorly and used for a variety of psychotherapeutic approaches that do not necessarily pursue the same goal. We give a summary of three metacognitive interventions which were developed within a sound theoretical framework—metacognitive therapy, metacognitive training, and metacognitively-oriented integrative psychotherapies—and discuss their similarities and distinctive features. We then offer an integrative operational definition of metacognitive interventions as goal-oriented treatments that target metacognitive content, which is characterized by the awareness and understanding of one’s own thoughts and feelings as well as the thoughts and feelings of others. They aim to alleviate disorder-specific and individual symptoms by gaining more flexibility in cognitive processing.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
When John H. Flavell first introduced the term metacognition in 1979 (Flavell 1979) as “knowledge and cognition about cognitive phenomena” (p. 906), he based his concept on findings in developmental psychology regarding our capacity to understand something or someone. In order to understand, we need to appraise the available information correctly which, according to Flavell, requires knowledge about the processes that affect our cognitions. Such metacognitive knowledge helps us to better monitor and control our cognitions, a process closely linked to emotional responses which have further impact on metacognitive processes. In his article, Flavell promotes the idea that metacognitive knowledge can be increased through systematic training. Yet, he describes a training of a recall memory task, which targets rather cognitive than metacognitive functions. This distinction highlights an important difference that we will try to clarify here.
In the last 20 years, the concept of metacognitions was used to further develop psychotherapeutic interventions for mental disorders. A systematic electronic search on metacognitive interventions (for more detailed information see Philipp et al. 2018) showed that the term “metacognition” is often poorly defined or applied loosely when used as a framework for psychological treatments (Wells and Fisher 2011). However, we identified three interventions which offer a sound definition of the term in context of their evidence-based treatments: Metacognitive Therapy as developed by Wells and Matthews (1994), Metacognitive Training by Moritz and Woodward (2007), and metacognitively-oriented approaches which have previously been described as integrative psychotherapies (Hamm et al. 2013), for example Metacognitive Reflection and Insight Therapy by Lysaker and Klion (2017) and Metacognitive Interpersonal Therapy by Dimaggio et al. (2017). Naturally, there is an ongoing discussion between the authors of these interventions about the true meaning of the term “metacognition” and its appropriate implementation within psychological treatments (Capobianco and Wells 2017; Andreou et al. 2018; Solanto et al. 2010; Wells and Fisher 2011; Moritz and Lysaker 2018). Differences in their underlying theoretical frameworks and their diverging lines of argument may add to the confusion about what metacognitive interventions are.
In this contribution, we try to offer a more integrative perspective arguing that—although all three metacognitive interventions differ greatly from one another—the use of the term “metacognitive” is justified within each framework. Therefore, we aim to give a summary of these interventions and discuss their similarities and distinctive features. Moreover, we aim to introduce an operational definition of the term Metacognitive Interventions that may help to better differentiate them from other psychological interventions.
Metacognitive Interventions
Metacognitive Therapy
Based on his experiences in the treatment of patients with generalized anxiety disorder (GAD) and the importance of worry for this disorder (Wells 1995), Wells follows Flavell’s definition as he describes metacognitions as thoughts or beliefs (Wells’ term for knowledge) about cognition and further specifies them as the strategies we use to control our attention and thinking (Wells 2000, 2013). According to Wells and Matthews, mental disorders can be described within a Self-regulatory executive function (S-REF) model (Wells and Matthews 1996), stressing the importance of attentional processes in order to select and process information. The disorder-specific thinking style which regulates information processing is represented in the Cognitive Attentional Syndrome (CAS). The CAS is defined as a result of inflexible metacognitions—the combination of positive (i.e. “worrying is a helpful way of coping”) and negative beliefs (i.e. “thoughts are uncontrollable”) about disorder-specific cognitions. It poses the core symptom of mental disorders because it leads to dysfunctional appraisal of information and negative emotional responses, indicating that more flexibility in metacognitions may reduce bias during information processing.
Wells developed his Metacognitive Therapy as an individual treatment to challenge those inflexible metacognitive beliefs and to modify patients’ S-REF model, especially in order to alleviate their individual CAS in GAD. Metacognitive Therapy was then adapted for the treatment of other disorders (Fisher and Wells 2008; Morrison et al. 2014; Papageorgiou and Wells 2001; Wells et al. 1995; Wells and Sembi 2004) and to group settings (Papageorgiou and Wells 2015). The full intervention often includes techniques that aim to raise inner awareness and increase flexible control over attention, thoughts and strategies: Detached Mindfulness (Wells 2005) and Attention Training (Wells 2007). Both interventions can be administered in combination or independently. Evidence from a meta-analysis with (non-)randomized trials suggests that Metacognitive Therapy is effective in the treatment of patients with anxiety, posttraumatic stress and depression (see Normann et al. 2014; Philipp et al. 2018; Wells 2013 for a summary of evidence).
Metacognitive Training
Based on the work by Asher Koriat on the importance of confidence for decision-making (Koriat and Levy-Sadot 1999; Koriat 2002) and supported by their findings about false memories and overconfidence in erroneous judgment in patients with schizophrenia (Moritz and Woodward 2006; Moritz et al. 2017), Moritz and Woodward (2007) suggest that metacognition reflects patients’ awareness of their cognitive biases. According to the authors, typical cognitive biases like jumping to conclusions, overconfidence, or incorrigibility are usually not consciously accessible and thus form the key features of delusional beliefs and positive symptoms. Metacognitive Training aims to improve awareness of these cognitive biases by enhancing patients’ metacognitions, namely their “capacity to think about their thinking” (p. 562) (Moritz et al. 2010) in accordance to Flavell. Originally conceptualized as an eight-module group program, Metacognitive Training aims to modify metacognitions that contribute to cognitive biases indirectly by educating patients about cognitive processes typical for their disorder, their negative consequences, and alternative thinking strategies (Moritz and Woodward 2007; Moritz et al. 2014). The intervention is being continually developed and training programs are available for other mental disorders, taking disorder-specific cognitive biases into account (Hauschildt et al. 2016; Jelinek et al. 2016; Moritz et al. 2017; Schilling et al. 2017; So et al. 2015). It was also adapted into an individual training, allowing for a more intensive and tailored treatment (Andreou et al. 2016), and trainings that put emphasis on social and relational aspects (Moritz et al. 2014; Rocha and Queirós 2013). The effectiveness of Metacognitive Training has been subject to a large number of randomized controlled trials. A meta-analysis with (non-)randomized trials showed a significant alleviation of symptoms in patients with schizophrenia and obsessive–compulsive disorder (see Eichner and Berna 2016; Jiang et al. 2015; Liu et al. 2018; Philipp et al. 2018; van Oosterhout 2015 for a summary of evidence).
Metacognitively-Oriented Integrative Psychotherapies
Focusing on patients’ subjective and intersubjective experiences, a number of psychotherapies have been developed that use metacognition as the ability to understand and make sense of own mental states and the mental states of others (Dimaggio et al. 2010; Lysaker et al. 2011; Salvatore et al. 2012; Semerari et al. 2007; Semerari et al. 2014). They are based on a narrative approach which was introduced by Lysaker and Lysaker (2001) and Dimaggio and Semerari (2001). The authors state that mental disorders, schizophrenia and personality disorders in particular, are characterized by the patients’ inability to construct a coherent personal narrative (Lysaker et al. 2005). Impoverished or disintegrated narratives prevent patients from reflecting on their own mental states and from experiencing the complexity of interpersonal relationships (Dimaggio and Semerari 2001). Following these observations, Semerari et al. (2003) found that there are typical metacognitive deficits for different mental disorders. In psychotherapy, these deficits can be specifically targeted while also taking into account patients’ existing abilities. Metacognitive Interpersonal Therapy aims to identify maladaptive interpersonal schemas, to establish a formulation of functioning, and to help patients to construct an alternative, integrated sense of self and others (Dimaggio et al. 2017; Gordon-King et al. 2018). Metacognitive Reflection and Insight Therapy includes eight integrative principles that aim to improve metacognitive abilities by promoting patients’ reflection on their thoughts, feelings, and challenges, the therapeutic relationship, and the mind of others (Lysaker and Roe 2016; Lysaker et al. 2015; de Jong et al. 2016). Other psychotherapies based on this framework are the Metacognitive-Oriented Social Skills Training (MOSST), a group therapy that promotes patients’ awareness of their mental stated by incorporating elements of social skills training (Ottavi et al. 2014; Inchausti et al. 2017) and Metacognitive Narrative Therapy, an individual therapy that aims to enrich patients’ narratives within five phases of treatment (Bargenquast and Schweitzer 2014). Next to a number of case and qualitative studies testing the effectiveness of metacognitively-oriented integrative psychotherapies (Dimaggio et al. 2017; Gordon-King et al. 2018; Inchausti et al. 2017; de Jong et al. 2016; Lysaker et al. 2005, 2015), which report promising results, there is also one randomized controlled trial (Vohs et al. 2017). Although the study did not find a significant effect for MERIT in alleviating symptoms in patients with early phase psychosis, it showed positive effects for improved insight and reflectiveness (see Philipp et al. 2018 for a more detailed description of evidence).
Similarities and Distinctive Features Between Metacognitive Interventions
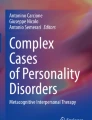
Although the three conceptualizations of metacognitive interventions differ in their theoretical and clinical background, they all share a meta-level of cognition on which we may control, regulate, and reflect on our thoughts and therefore, are able to affect our emotions and behavior. The essential features of the described treatments are summarized in Fig. 1.

Overview of metacognitive interventions
Similar to Wells, who understands Metacognitive Therapy as an extension of Cognitive Behavioral Therapy (CBT) (Hofmann and Asmundson 2008), Moritz encourages to administer Metacognitive Training in addition to individual psychotherapy as it may facilitate talking about symptoms more directly (Moritz et al. 2014). Both authors promote an indirect treatment approach that aims to modify metacognitive content instead of cognitions—inflexible metacognitive beliefs in Metacognitive Therapy and cognitive biases in Metacognitive Training. Even though both interventions work with elements of psychoeducation, psychoeducation seems to be of more importance in Metacognitive Training. The combination of psychoeducation and training sessions targets cognitive processes by raising patients’ awareness of their inflexible thinking biases. In Metacognitive Therapy, the focus is on challenging patients’ negative and positive metacognitive beliefs. Because one key element is the formulation of the patient’s problem based on an individual metacognitive model, Metacognitive Therapy might be more tailored to patients’ needs than Metacognitive Training. Yet, in MCT +, an individual illness model is established beforehand (Moritz et al. 2011). Furthermore, both approaches consider the disorder-specific adaptation of their single components – CAS for Metacognitive Therapy and specific cognitive biases in Metacognitive Training – more effective than using generic models or modules.
Metacognitively-oriented integrative psychotherapies seem to focus less on the symptom level of the disorder, but promote personal growth by developing an integrated sense of self through enriching patients’ narratives. Although Metacognitive Training educates patients in Theory of Mind and trains them in social situations, intersubjective experiences play a more essential role in metacognitively-oriented integrative psychotherapies, as understanding the other’s mind is a basic metacognitive ability in their conceptualization (Lysaker et al. 2011; Semerari et al. 2003). Moreover, these psychotherapies aim to improve social relationships and symptoms in patients with personality disorders and schizophrenia, whereas Metacognitive Training explicitly targets positive symptoms in patients with schizophrenia.
Conceptual Distinction from Other Psychological Interventions
All three presented interventions are manual-based interventions specifically targeting metacognitive content. In addition to their primary focus, they can be distinguished from traditional psychotherapies and other psychological interventions by taking a closer look at their specific therapeutic elements (Dickerson and Lehman 2011).
Some of the interventions in CBT may include metacognitive elements. Yet, in these interventions, such as internet-delivered CBT for depression and generalized anxiety disorder (iCBT) (Newby et al. 2014), CBT for psychosis (CBTp) (Menon et al. 2017), or Rational Emotive Behavior Therapy (REBT, Ellis and Dryden 2007) metacognitive elements are not the core component but only part of a more comprehensive treatment. Compared to earlier versions of Metacognitive Training, recent developments of the program include more cognitive elements, which might shift the focus of the training towards a CBT approach. Still, a large proportion of the training deals with metacognitive content (Andreou et al. 2018).
Although Metacognitive Therapy includes Detached Mindfulness and Attention Training Technique—approaches, which promote a state of self-awareness and aim to ameliorate selective attention in terms of CAS, respectively—it differs from therapies like Mindfulness-Based Cognitive Therapy (MBCT, Segal et al. 2013) and Acceptance and Commitment Therapy (ACT, A-Tjak et al. 2015). Other than these third waves therapies, metacognitive interventions generate a model of illness, are goal-oriented, educate patients about their symptoms, and promote alternative strategies (Dickerson and Lehman 2011; Wells et al. 2009). On the other hand, Metacognitively-oriented integrative psychotherapies can be described as third wave therapies as they incorporate elements of psychodynamic, cognitive behavioral, humanistic and recovery-focused interventions (Gordon-King et al. 2018; Lysaker and Roe 2016). Nevertheless the emphasis on patients’ metacognitive abilities also allows for a classification independent from third wave therapies.
The large proportion of metacognitive elements in Cognitive Remediation Training (CRT) programs like COGPACK® (Marker 2003; Moritz et al. 2015) or Computerized Interactive Remediation of Cognition Training for Schizophrenia (CIRCuiTS, Cella et al. 2016) make it necessary to distinguish them from metacognitive interventions. CRT aims to improve neuropsychological functioning in patients by using exercises with explicit instructions and learning strategies. Therefore, they target cognitive content. Metacognitive interventions, on the other hand, need to go beyond simple skill or strategy training (Dawson et al. 2014; Moro et al. 2015) or self-management skills (Solanto et al. 2010; Wells and Fisher 2011) which have been proven effective in patients with other deficits. In Metacognitive Training, CRT plays a rather secondary role and is applied in the context of cognitive biases, on which patients reflect with a therapist. Metacognitive interventions can be distinguished from Cognitive Bias Modification (CBM) interventions for the same reasons. They aim to reduce cognitive bias directly and thus focus on training tasks (Jones and Sharpe 2017).
Conclusion
The three metacognitive interventions that we describe and compare in this article differ greatly in their theoretical groundwork, their definition of metacognition and, accordingly, their clinical implications. Each of the interventions focuses on different aspects of metacognition, depending on the goal they want to achieve in the treatment of mental disorders. Metacognitive Training focuses on patients’ awareness that there is a meta-level of cognition and fosters their capacity to acknowledge this through training. This assumption appears to be immanent in Metacognitive Therapy, which emphasizes the role of metacognition in selecting and processing information and challenges patients’ inflexible thoughts. Metacognitively-oriented integrative psychotherapies add the interpersonal perspective to the patients’ ability to reflect on own mental states and its relevance in order to develop and integrated sense of self and others.
Consistent with these considerations, metacognitive interventions can be defined as treatments that explicitly target metacognitive content—characterized by the awareness and understanding of one’s thoughts and feelings as well as the thoughts and feelings of others—as the key element. These interventions are also goal-oriented and aim to alleviate disorder-specific and individual symptoms by specifically enhancing metacognitive capacities in order to gain more flexibility in the attention, monitoring, control, and regulation of cognitive processes. Because of the different concepts of metacognition promoted in each of these interventions, they all pursue different goals in the treatment of mental disorders which does not make them mutually exclusive but offers valuable contribution in the field of clinical psychology and psychotherapy when applied to the appropriate group of patients and clinical setting.
With our operating definition, we aim to facilitate identifying therapeutic approaches which share theoretical backgrounds and pursue the same goals as the metacognitive interventions described above. Thereby, we hope to contribute to more clarity in clinical and academic exchange.
References
Andreou, C., Balzan, R. P., Jelinek, L., & Moritz, S. (2018). Letter to the Editor: Metacognitive training and metacognitive therapy. A reply to Lora Capobianco and Adrian Wells. Journal of Behavior Therapy and Experimental Psychiatry. https://doi.org/10.1016/j.jbtep.2018.01.006.
Andreou, C., Wittekind, C. E., Fieker, M., Heitz, U., Veckenstedt, R., Bohn, F., et al. (2016). Individualized metacognitive therapy for delusions: A randomized controlled rater-blind study. Journal of Behavior Therapy and Experimental Psychiatry,56, 144–151. https://doi.org/10.1016/j.jbtep.2016.11.013.
A-Tjak, J. G. L., Davis, M. L., Morina, N., Powers, M. B., Smits, J. A. J., & Emmelkamp, P. M. G. (2015). A meta-analysis of the efficacy of acceptance and commitment therapy for clinically relevant mental and physical health problems. Psychotherapy and Psychosomatics,84, 30–36. https://doi.org/10.1159/000365764.
Bargenquast, R., & Schweitzer, R. (2014). Metacognitive narrative psychotherapy for people diagnosed with schizophrenia: An outline of a principle-based treatment manual. Psychosis,6, 155–165. https://doi.org/10.1080/17522439.2012.753935.
Capobianco, L., & Wells, A. (2017). Letter to the editor: Metacognitive therapy or metacognitive training: What’s in a name? Journal of Behavior Therapy and Experimental Psychiatry. https://doi.org/10.1016/j.jbtep.2017.12.003.
Cella, M., Reeder, C., & Wykes, T. (2016). Group cognitive remediation for schizophrenia: Exploring the role of therapist support and metacognition. Psychology and Psychotherapy,89, 1–14. https://doi.org/10.1111/papt.12062.
Dawson, D., Richardson, J., Troyer, A., Binns, M., Clark, A., Polatajko, H., et al. (2014). An occupation-based strategy training approach to managing age-related executive changes: A pilot randomized controlled trial. Clinical Rehabilitation,28, 118–127. https://doi.org/10.1177/0269215513492541.
de Jong, S., van Donkersgoed, R., Pijnenborg, G. H. M., & Lysaker, P. H. (2016). Metacognitive reflection and insight therapy (MERIT) with a patient with severe symptoms of disorganization. Journal of Clinical Psychology,72, 164–174. https://doi.org/10.1002/jclp.22249.
Dickerson, F. B., & Lehman, A. F. (2011). Evidence-based psychotherapy for schizophrenia: 2011 update. The Journal of Nervous and Mental Disease,199, 520–526. https://doi.org/10.1097/NMD.0b013e318225ee78.
Dimaggio, G., Salvatore, G., MacBeth, A., Ottavi, P., Buonocore, L., & Popolo, R. (2017). Metacognitive interpersonal therapy for personality disorders: A case study series. Journal of Contemporary Psychotherapy,47, 11–21. https://doi.org/10.1007/s10879-016-9342-7.
Dimaggio, G., Salvatore, G., Nicolò, G., Fiore, D., & Procacci, M. (2010). Enhancing mental state understanding in the over-constricted personality disorder with metacognitive interpersonal therapy. In G. Dimaggio & P. H. Lysaker (Eds.), Metacognition and severe adult mental disorders: From basic research to treatment (pp. 247–268). London: Routledge.
Dimaggio, G., & Semerari, A. (2001). Psychopathological narrative forms. Journal of Constructivist Psychology,14, 1–23. https://doi.org/10.1080/107205301451335.
Eichner, C., & Berna, F. (2016). Acceptance and efficacy of Metacognitive Training (MCT) on positive symptoms and delusions in patients with schizophrenia: A meta-analysis taking into account important moderators. Schizophrenia Bulletin,42, 952–962. https://doi.org/10.1093/schbul/sbv225.
Ellis, A., & Dryden, W. (2007). The Practice of Rational Emotive Behavior Therapy (2nd ed.). New York, NY: Springer Publishing Company.
Fisher, P. L., & Wells, A. (2008). Metacognitive therapy for obsessive–compulsive disorder: A case series. Journal of Behavior Therapy and Experimental Psychiatry,39, 117–132. https://doi.org/10.1016/j.jbtep.2006.12.001.
Flavell, J. H. (1979). Metacognition and cognitive monitoring: A new area of cognitive-developmental inquiry. American Psychologist,34, 906–911. https://doi.org/10.1037//0003-066X.34.10.906.
Gordon-King, K., Schweitzer, R. D., & Dimaggio, G. (2018). Metacognitive interpersonal therapy for personality disorders featuring emotional inhibition: A multiple baseline case series. The Journal of Nervous and Mental Disease. https://doi.org/10.1097/NMD.0000000000000789.
Hamm, J. A., Hasson-Ohayon, I., Kukla, M., & Lysaker, P. H. (2013). Individual psychotherapy for schizophrenia: Trends and developments in the wake of the recovery movement. Psychology Research and Behavior Management,6, 45–54. https://doi.org/10.2147/PRBM.S47891.
Hauschildt, M., Schröder, J., & Moritz, S. (2016). Randomized-controlled trial on a novel (meta-)cognitive self-help approach for obsessive-compulsive disorder (“myMCT”). Journal of Obsessive-Compulsive and Related Disorders,10, 26–34. https://doi.org/10.1016/j.jocrd.2016.04.010.
Hofmann, S. G., & Asmundson, G. J. G. (2008). Acceptance and mindfulness-based therapy: New wave or old hat? Clinical Psychology Review,28, 1–16. https://doi.org/10.1016/j.cpr.2007.09.003.
Inchausti, F., García-Poveda, N. V., Ballesteros-Prados, A., Fonseca-Pedrero, E., Ortuño-Sierra, J., Sánchez-Reales, S., et al. (2017). A pilot study on feasibility, acceptance and effectiveness of metacognitive-oriented social skills training in schizophrenia. BMC Psychiatry,17, 217. https://doi.org/10.1186/s12888-017-1378-z.
Jelinek, L., Hauschildt, M., Wittekind, C. E., Schneider, B. C., Kriston, L., & Moritz, S. (2016). Efficacy of metacognitive training for depression: A randomized controlled trial. Psychotherapy and Psychosomatics,85, 231–234. https://doi.org/10.1159/000443699.
Jiang, J., Zhang, L., Zhu, Z., Li, W., & Li, C. (2015). Metacognitive Training for schizophrenia: A systematic review. Shanghai Archives of Psychiatry,27, 149–157. https://doi.org/10.11919/j.issn.1002-0829.215065.
Jones, E. B., & Sharpe, L. (2017). Cognitive bias modification: A review of meta-analyses. Journal of Affective Disorders,223, 175–183. https://doi.org/10.1016/j.jad.2017.07.034.
Koriat, A. (2002). Metacognition research: An interim report. In T. J. Perfect & B. L. Schwartz (Eds.), Applied metacognition (pp. 261–286). Cambridge: Cambridge University Press.
Koriat, A., & Levy-Sadot, R. (1999). Processes underlying metacognitive judgments: Information-based and experience-based monitoring of one’s own knowledge. In S. Chaiken & Y. Trope (Eds.), Dual process theories in social psychology (pp. 483–502). New York: Guilford.
Liu, Y.-C., Tang, C.-C., Hung, T.-T., Tsai, P.-C., & Lin, M.-F. (2018). The efficacy of Metacognitive Training for delusions in patients with schizophrenia: A meta-analysis of randomized controlled trials informs evidence-based practice. Worldviews on Evidence-Based Nursing,15, 130–139. https://doi.org/10.1111/wvn.12282.
Lysaker, P. H., Buck, K. D., Carcione, A., Procacci, M., Salvatore, G., Nicolò, G., et al. (2011). Addressing metacognitive capacity for self reflection in the psychotherapy for schizophrenia: A conceptual model of the key tasks and processes. Psychology and Psychotherapy,84, 58–69. https://doi.org/10.1348/147608310x520436.
Lysaker, P. H., Davis, L. W., Eckert, G. J., Strasburger, A. M., Hunter, N. L., & Buck, K. D. (2005). Changes in narrative structure and content in schizophrenia in long term individual psychotherapy: A single case study. Clinical Psychology and Psychotherapy,12, 406–416. https://doi.org/10.1002/cpp.457.
Lysaker, P. H., & Klion, R. E. (2017). Recovery, meaning-making, and severe mental illness: A comprehensive guide to metacognitive reflection and insight therapy (1st ed.). New York, NY: Routledge.
Lysaker, P. H., Kukla, M., Belanger, E., White, D. A., Buck, K. D., Luther, L., et al. (2015). Individual psychotherapy and changes in self-experience in schizophrenia: A qualitative comparison of patients in metacognitively focused and supportive psychotherapy. Psychiatry,78, 305–316. https://doi.org/10.1080/00332747.2015.1063916.
Lysaker, P. H., & Lysaker, J. T. (2001). Psychosis and the disintegration of dialogical self-structure: Problems posed by schizophrenia for the maintenance of dialogue. British Journal of Medical Psychology,74, 23–33.
Lysaker, P. H., & Roe, D. (2016). Integrative psychotherapy for schizophrenia: Its potential for a central role in recovery oriented treatment. Journal of Clinical Psychology,72, 117–122. https://doi.org/10.1002/jclp.22246.
Marker, K. (2003). COGPACK. Ladenburg: Marker Software.
Menon, M., Balzan, R. P., Harper-Romeo, K., Kumar, D., Anderson, D., Moritz, S., et al. (2017). Psychosocial approaches in the treatment of psychosis: Cognitive behaviour therapy for psychosis (CBTp) and metacognitive training (MCT). Clinical Schizophrenia and Related Psychoses,11(3), 156–163.
Moritz, S., Andreou, C., Schneider, B. C., Wittekind, C. E., Menon, M., Balzan, R. P., et al. (2014). Sowing the seeds of doubt: A narrative review on metacognitive training in schizophrenia. Clinical Psychology Review,34, 358–366. https://doi.org/10.1016/j.cpr.2014.04.004.
Moritz, S., Lüdtke, T., Pfuhl, G., Balzan, R., & Andreou, C. (2017). Liberale Akzeptanz als kognitiver Mechanismus bei Psychose: Eine 2-Stufen-Theorie der Pathogenese schizophrener Positivsymptome. Verhaltenstherapie,27, 108–118. https://doi.org/10.1159/000464256.
Moritz, S., & Lysaker, P. H. (2018). Metacognition–what did James H. Flavell really say and the implications for the conceptualization and design of metacognitive interventions. Schizophrenia Research. https://doi.org/10.1016/j.schres.2018.06.001.
Moritz, S., Thoering, T., Kühn, S., Willenborg, B., Westermann, S., & Nagel, M. (2015). Metacognition-augmented cognitive remediation training reduces jumping to conclusions and overconfidence but not neurocognitive deficits in psychosis. Frontiers in Psychology,6, 1048. https://doi.org/10.3389/fpsyg.2015.01048.
Moritz, S., Veckenstedt, R., Randjbar, S., Vitzthum, F., & Woodward, T. S. (2011). Antipsychotic treatment beyond antipsychotics: Metacognitive intervention for schizophrenia patients improves delusional symptoms. Psychological Medicine,41, 1823–1832. https://doi.org/10.1017/S0033291710002618.
Moritz, S., Vitzthum, F., Randjbar, S., Veckenstedt, R., & Woodward, T. S. (2010). Detecting and defusing cognitive traps: Metacognitive intervention in schizophrenia. Current Opinion in Psychiatry,23, 561–569. https://doi.org/10.1097/YCO.0b013e32833d16a8.
Moritz, S., & Woodward, T. S. (2006). Metacognitive control over false memories: A key determinant of delusional thinking. Current Psychiatry Reports,8, 184–190.
Moritz, S., & Woodward, T. S. (2007). Metacognitive training for schizophrenia patients (MCT): A pilot study on feasibility, treatment adherence, and subjective efficacy. The German Journal of Psychiatry,10(3), 69–78.
Moro, V., Condoleo, M. T., Valbusa, V., Broggio, E., Moretto, G., & Gambina, G. (2015). Cognitive stimulation of executive functions in mild cognitive impairment: Specific efficacy and impact in memory. American Journal of Alzheimer’s Disease and other Dementias,30, 153–164. https://doi.org/10.1177/1533317514539542.
Morrison, A. P., Pyle, M., Chapman, N., French, P., Parker, S. K., & Wells, A. (2014). Metacognitive therapy in people with a schizophrenia spectrum diagnosis and medication resistant symptoms: A feasibility study. Journal of Behavior Therapy and Experimental Psychiatry,45, 280–284. https://doi.org/10.1016/j.jbtep.2013.11.003.
Newby, J. M., Williams, A. D., & Andrews, G. (2014). Reductions in negative repetitive thinking and metacognitive beliefs during transdiagnostic internet cognitive behavioural therapy (iCBT) for mixed anxiety and depression. Behaviour Research and Therapy,59, 52–60. https://doi.org/10.1016/j.brat.2014.05.009.
Normann, N., van Emmerik, A. A. P., & Morina, N. (2014). The efficacy of Metacognitive Therapy for anxiety and depression: A meta-analytic review. Depression and Anxiety,31, 402–411. https://doi.org/10.1002/da.22273.
Ottavi, P., D’Alia, D., Lysaker, P., Kent, J., Popolo, R., Salvatore, G., et al. (2014). Metacognition-oriented social skills training for individuals with long-term schizophrenia: Methodology and clinical illustration. Clinical Psychology and Psychotherapy,21, 465–473. https://doi.org/10.1002/cpp.1850.
Papageorgiou, C., & Wells, A. (2001). Metacognitive beliefs about rumination in recurrent major depression. Cognitive and Behavioral Practice,8, 160–164. https://doi.org/10.1016/S1077-7229(01)80021-3.
Papageorgiou, C., & Wells, A. (2015). Group metacognitive therapy for severe antidepressant and CBT resistant depression: A baseline-controlled trial. Cognitive Therapy and Research,39, 14–22. https://doi.org/10.1007/s10608-014-9632-x.
Philipp, R., Kriston, L., Lanio, J., Kühne, F., Härter, M., Moritz, S., et al. (2018). Effectiveness of metacognitive interventions for mental disorders in adults–A systematic review and meta-analysis (METACOG). Clinical Psychology and Psychotherapy,26, 227–240. https://doi.org/10.1002/cpp.2345.
Rocha, N. B. F., & Queirós, C. (2013). Metacognitive and social cognition training (MSCT) in schizophrenia: A preliminary efficacy study. Schizophrenia Research,150, 64–68. https://doi.org/10.1016/j.schres.2013.07.057.
Salvatore, G., Lysaker, P. H., Gumley, A., Popolo, R., Mari, J., & Dimaggio, G. (2012). Out of illness experience: Metacognition-oriented therapy for promoting self-awareness in individuals with psychosis. American Journal of Psychotherapy,66(1), 85–106.
Schilling, L., Moritz, S., Kriston, L., Krieger, M., & Nagel, M. (2017). Efficacy of metacognitive training for patients with borderline personality disorder: Preliminary results. Psychiatry Research. https://doi.org/10.1016/j.psychres.2017.09.024.
Segal, Z. V., Williams, J. M. G., & Teasdale, J. D. (2013). Mindfulness-based cognitive therapy for depression: A new approach to preventing relapse (2nd ed.). New York, NY: The Guilford Press.
Semerari, A., Carcione, A., Dimaggio, G., Falcone, M., Nicolò, G., Procacci, M., et al. (2003). How to evaluate metacognitive functioning in psychotherapy? The metacognition assessment scale and its applications. Clinical Psychology and Psychotherapy,10, 238–261. https://doi.org/10.1002/cpp.362.
Semerari, A., Carcione, A., Dimaggio, G., Nicolò, G., & Procacci, M. (2007). Understanding minds: Different functions and different disorders? The contribution of psychotherapy research. Psychotherapy Research,17, 106–119. https://doi.org/10.1080/10503300500536953.
Semerari, A., Colle, L., Pellecchia, G., Buccione, I., Carcione, A., Dimaggio, G., et al. (2014). Metacognitive dysfunctions in personality disorders: Correlations with disorder severity and personality styles. Journal of Personality Disorders,28, 751–766. https://doi.org/10.1521/pedi_2014_28_137.
So, S. H.-W., Chan, A. P., Chong, C. S.-Y., Wong, M. H.-M., Lo, W. T.-L., Chung, D. W.-S., et al. (2015). Metacognitive training for delusions (MCTd): Effectiveness on data-gathering and belief flexibility in a Chinese sample. Frontiers in Psychology,6, 730. https://doi.org/10.3389/fpsyg.2015.00730.
Solanto, M. V., Marks, D. J., Wasserstein, J., Mitchell, K., Abikoff, H., Alvir, J. M. J., et al. (2010). Efficacy of meta-cognitive therapy for adult ADHD. The American Journal of Psychiatry,167, 958–968. https://doi.org/10.1176/appi.ajp.2009.09081123.
van Oosterhout, B., Smit, F., Krabbendam, L., Castelein, S., Staring, A. B. P., & van der Gaag, M. (2015). Metacognitive Training for schizophrenia spectrum patients: A meta-analysis on outcome studies. Psychological Medicine,46, 47–57. https://doi.org/10.1017/S0033291715001105.
Vohs, J. L., Leonhardt, B. L., James, A. V., Francis, M. M., Breier, A., Mehdiyoun, N., et al. (2017). Metacognitive reflection and insight therapy for early psychosis: A preliminary study of a novel integrative psychotherapy. Schizophrenia Research. https://doi.org/10.1016/j.schres.2017.10.041.
Wells, A. (1995). Meta-cognition and worry: A cognitive model of generalized anxiety disorder. Behavioural and Cognitive Psychotherapy,23, 301–320.
Wells, A. (2000). Emotional disorders and metaacognition: Innovative cognitive therapy. Chichester: Wiley.
Wells, A. (2005). Detached Mindfulness in cognitive therapy: A metacognitive analysis and ten techniques. Journal of Rational-Emotive and Cognitive-Behavior Therapy,23, 337–355. https://doi.org/10.1007/s10942-005-0018-6.
Wells, A. (2007). The attention training technique: The attention training technique: Theory, effects, and a metacognitive hypothesis on auditory hallucinations. Cognitive and Behavioral Practice,14, 134–138. https://doi.org/10.1016/j.cbpra.2006.01.010.
Wells, A. (2013). Advances in metacognitive therapy. International Journal of Cognitive Therapy,6, 186–201. https://doi.org/10.1521/ijct.2013.6.2.186.
Wells, A., Clarke, D. M., Salkovskis, P., Ludgate, J., Hackmann, A., & Gelder, M. (1995). Social phobia: The role of in-situation safety behaviors in maintaining anxiety and negative beliefs. Behavior Therapy,26, 153–161.
Wells, A., & Fisher, P. L. (2011). Meta-cognitive therapy without metacognition: A case of ADHD. The American Journal of Psychiatry,168, 327–328. https://doi.org/10.1176/appi.ajp.2010.1010150r.
Wells, A., Fisher, P. L., Myers, S., Wheatley, J., Patel, T., & Brewin, C. R. (2009). Metacognitive therapy in recurrent and persistent depression: A multiple-baseline study of a new treatment. Cognitive Therapy and Research,33, 291–300. https://doi.org/10.1007/s10608-007-9178-2.
Wells, A., & Matthews, G. (1994). Attention and emotion: A clinical perspective. Hove: Lawrence Erlbaum.
Wells, A., & Matthews, G. (1996). Modelling cognition in emotional disorder: The S-REF model. Behaviour Research and Therapy,34, 881–888. https://doi.org/10.1016/S0005-7967(96)00050-2.
Wells, A., & Sembi, S. (2004). Metacognitive therapy for PTSD: A preliminary investigation of a new brief treatment. Journal of Behavior Therapy and Experimental Psychiatry,35, 307–318. https://doi.org/10.1016/j.jbtep.2004.07.001.
Acknowledgements
We thank Steffen Moritz for his notes on Metacognitive Training and the reviewers for their notes on earlier drafts of the manuscript.
Funding
This work was funded by the German Federal Ministry of Education and Research (Grant Number 01KG1511).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
LK participated in trials of the Metacognitive Training as independent statistician. All other authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Philipp, R., Kriston, L., Kühne, F. et al. Concepts of Metacognition in the Treatment of Patients with Mental Disorders. J Rat-Emo Cognitive-Behav Ther 38, 173–183 (2020). https://doi.org/10.1007/s10942-019-00333-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10942-019-00333-3