
Abstract
Introduction
Low birth weight (LBW) is a global issue prevalent in low-income countries. Economic assessments of interventions to reduce this burden are crucial to guide health policies. However, there is a relative scarcity of research that illustrates the magnitude of LBW by country and region to support the design of public policies.
Objective
This study aimed to analyze the temporal trend of fetal growth in newborns in Brazil between 2010 and 2020.
Methods
A time series study was conducted using data from the Live Births Information System (SINASC), which is managed by the Department of Information and Informatics of the Unified Health System (DATASUS) of the Brazilian Ministry of Health. The Prais-Winsten linear model was applied to analyze the annual proportions of LBW. The annual percentage changes (APC) and their respective 95% confidence intervals (95%CI) were calculated. Prevalence rate averages of LBW were calculated and displayed on thematic maps to visualize the evolution dynamics in each Federation Unit (FU).
Results
A total of 31,887,329 women from all Federative Units of Brazil were included in the study from 2010 to 2020. The Southeast region had the largest proportion of participants, with records from 2015 accounting for 9.5% of the total. Among the women in the study, 49.6% were between the ages of 20 and 29, and the majority (75.5%) had between 8 and 12 years of schooling. The newborns of these women were predominantly male (58.8%) and non-white (59.5%). The study found that there was a trend towards stabilization of increasing proportions of LBW in the North, Northeast, and Centre-West regions between 2010 and 2020. In Brazil and other regions, these tendencies remained stable.
Conclusion
To improve living conditions and reduce social inequalities and health inequities, public policies and actions are necessary. Strengthening the Unified Health System (SUS), income transfer programs, quota policies for vulnerable groups, and gender equality measures such as improving access to education for women and the labor sector are among the suggested approaches.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Birth weight is the first weight measured after birth and a crucial indicator of health outcomes later in a child’s life (Cutland et al., 2017; Basel & Singh, 2020; Pereira et al., 2010; Rondó et al., 2008, 2010; Tela et al., 2019), According to the World Health Organization, low birth weight (LBW) refers to a birth weight below 2,500 g, regardless of gestational age (World Health Organization, 2010). LBW is a crucial public health indicator that reflects maternal and neonatal health from nutritional, economic, and healthcare perspectives. Infants with LBW face a higher risk of morbidity and mortality from illness and death soon after birth, as well as non-communicable diseases throughout their lives (Agbozo et al., 2016; Pereira et al., 2010; Rondó et al., 2008, 2010).
It has been established that new-borns with LBW are at a greater risk of developing complications and experiencing death, compared to those with a normal weight, with a 20-fold increase in predisposition (Wardlaw, 2004). LBW may also increase the likelihood of cognitive deficits, motor delays, cerebral palsy, as well as other behavioral and psychological issues (Fan et al., 2013; Basel & Singh 2020; Mathewson et al., 2017). Additionally, the reduction of LBW cases could result in cost savings for households and the health system (Sicuri et al., 2011). Despite government and state efforts to tackle this issue, research on the temporal trends of LBW remains insufficient. A study conducted in Pelotas, Brazil, evaluated trends in prematurity, LBW, and intrauterine growth restriction in three birth cohorts (1982, 1993, and 2004). The study observed a slight increase in the prevalence of LBW, from 9 to 10%, while intrauterine growth restriction decreased from 14.8% in 1982 to 9.4% in 1993, and subsequently increased to 12% in 2004. Additionally, preterm births increased significantly, from 6.3% in 1982 to 14.7% in 2004 (Barros et al., 2008).
A study conducted on the trend of LBW and its determinants in Brazilian capitals between 1996 and 2011 revealed that improved access to education and healthcare reduced the risk of LBW in all regions of Brazil (de Souza Buriol et al., 2016). The study also highlighted the variations in LBW rates and associated factors within and between regions during different stages of demographic, epidemiological, and developmental transition in Brazil (de Souza Buriol et al., 2016). To understand the variation of LBW over time, as well as compare the temporality of LBW (Beraldo et al., 2022; Bernal et al., 2018),furthermore, the study has revealed variations in rates of LBW and related factors within and among regions of Brazil, reflecting shifts in demographics, epidemiology, and development. The aim of our investigation is to analyse the temporal trends in LBW between the years 2000 to 2020 and explore possible determinants of this phenomenon to gain a better understanding of its fluctuations over time.
Methods
This ecological study analyzed the time series of fetal growth and the proportion of live births with LBW in Brazil from 2010 to 2020. The study utilized populational data from the Live Births Information System (SINASC), which is part of the Department of Information and Informatics of the Unified Health System (DATASUS) under the Brazilian Ministry of Health. The data were obtained through the Platform for Data Science Applied to Health (SINASC, 2020).
Study Variables
The outcome of LBW was defined by dichotomously classifying the variable of birth weight as either LBW (< 2500 g) or normal weight (> 2500 g). To calculate the prevalence rate of LBW, the number of new-borns with LBW was divided by the total population of new-borns in the location and year, then multiplied by 100. These rates were calculated for each of the macro-regions of Brazil.
Statistical Analysis
The Prais-Winsten linear regression model was utilized to analyze the temporal trend of annual fetal growth rates, considering the serial autocorrelation, which refers to the dependence of a serial measure on its own values in previous periods. The model generated annual percentage changes (APC) along with their corresponding 95% confidence intervals (95%CI). To visually depict the evolution in each region, averages of LBW prevalence rates were computed and illustrated on thematic maps using QGIS 2.18 software.
The trend of LBW prevalence was interpreted based on the criteria set by Antunes & Cardoso (2015), where an increase (p < 0.05 and positive beta), decrease (p < 0.05 and negative beta), and stability (p ≥ 0.05) were identified. The explanatory variables were explored, and the time series analysis was carried out using Stata version 14.0 (Stata Corp., College Station, United States).
Results
A total of 31,887,329 women from all Federative Units of Brazil were included in the study over the course of several years. The Southeast region had the largest proportion of participants, and records from 2015 accounted for 9.5% of the total. Of the women in the study, 49.6% were between the ages of 20 and 29, and the majority (75.5%) had completed between 8 and 12 years of schooling. The new-borns of these women were predominantly male (58.8%) and non-white. Regarding the Percentage Change in the Period (PCP), the prevalence of LBW in Brazil remained stable from 2010 to 2020, with an average variation of 2.02%. However, significant variations were observed in the North, Northeast, and Midwest regions, where the prevalence increased by 4.74%, 5.82%, and 5.87%, respectively. In the North, the prevalence of LBW increased in all maternal age groups, especially among women under 20, with an increase of 6.53%. In the Northeast and Midwest regions, the prevalence of LBW increased in all maternal age groups, with a greater emphasis on women aged 20 to 29, presenting increases of 5.22% and 5.87%, respectively. (Table 1).
From 2010 to 2020, the yearly percentage variation of the proportion of LBW in all Brazilian Federal Units was equivalent to 0.18%. While the Southeast region saw a decrease of 0.05% in the proportion of LBW, the North, Northeast, and Centre-West regions experienced an increase in this proportion. In the South and Southeast regions, a stationary trend was observed (Table 2).
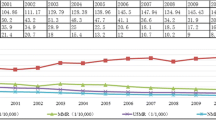
Results shows that there was a low APC in the proportions of LBW in Brazil between 2010 and 2020, with an increase of only 0.18%. However, when the results were disaggregated, it was evident that the Northeast, Midwest, and North regions recorded a slight increase in the prevalence of LBW (Fig. 1). Examining the distribution of the proportions of LBW in all the Federal States over the ten-year period, there was a general stabilization of the trends, although there was variability in behavior both within and between the regions, as well as in the annual percentage variation (APV) of 0.46% in the Southern region and 0.45% in the Northeast and Central-Western regions, as shown in (Fig. 2).

The proportion of LBW (all Brazilian mothers) according to year of notification

Prevalence of LBW in the Brazilian macro-regions in 2010 and 2020
Discussion
Our study reveals that the prevalence of LBW in Brazil has remained stable in recent years. This could be attributed to improved access to healthcare services, increased quality and quantity of prenatal consultations, and better socio-economic conditions, particularly in women’s education and their participation in the labor market (de Souza Buriol et al., 2016). However, despite these improvements, the Southern, South-Wastern, and Centre-West regions continue to exhibit high LBW prevalence rates. It is important to interpret these results cautiously, as these regions are the most developed with better health standards. This paradox is also highlighted in another study by Lima et al. (2013), They refer to this phenomenon as the “low birth weight paradox” where regions with higher socio-economic status have higher rates of LBW (Lima et al., 2013). Another study focusing on LBW trends between 1996 and 1999 showed that the states of Minas Gerais, Rio de Janeiro, São Paulo, and Rio Grande do Sul had the highest LBW rates among all states (Jorge et al., 2001).
Experts attribute this phenomenon to the inadequacy of the SINASC coverage in regions with lower health standards. However, this is not the case today, as the coverage of this system is adequate, and the quality of information has improved, making it a reliable source of data for health research and evaluation. The use of data from this system is crucial for monitoring health inequalities and the quality of care (Garcia & Santana, 2011; Pedraza, 2021; Predebon et al., 2010).
However, these results may be attributed to the improvement in the quality of diagnosis and care for pregnant women, which has enabled the induction of deliveries including caesarean sections. From a public health standpoint, this is a serious problem as it has led to an increase in preterm births and LBW infants, despite a reduction in infant mortality rates. This trend is particularly evident in regions that offer better perinatal health services, while inadequate care and limited access to perinatal technology in disadvantaged areas result in underreporting or misclassification of LBW births (de Andrade et al., 2008; Silva et al., 2005).
The findings concerning the temporal trend of LBW exhibit variations across different regions of Brazil. The North, Northeast, and Centre-West regions show an increasing trend in the proportions of LBW, whereas the trends in the South and Southeast regions remain stationary regardless of the maternal age group. It is important to note that the spatial distribution of LBW rates in the states is related to their location and reflects the social and health inequality experienced throughout the Brazilian territory. The North and Northeast regions historically suffer from restricted access to health services, including adequate prenatal ICU beds and assistance. Additionally, pregnant women in these regions often face socio-economic disadvantages, highlighting Brazil’s social problem situation as a precursor to health inequities, which can lead to various issues during pregnancy, delivery, and in the first days of life, including the development of cognitive skills (Minagawa et al., 2006). Studies conducted across different regions in Brazil indicate that mothers belonging to socially vulnerable groups tend to receive lower quality prenatal care (Coimbra et al., 2003; Gonçalves et al., 2009).
Brazil displays a high level of inequality at the Federal, State, and Municipal levels. This inequality may be attributed to the historical legacy of a socio-economic and political system that prioritizes economic competitiveness over integrality. The healthcare sector is no exception, as our findings indicate that regionalization has a significant impact on the unequal distribution of resources, as evidenced by the setback in the project to provide universal access to the SUS (De Albuquerque et al., 2017).
In this context, it is important to note the political phenomenon that undermines the universal and free project of the SUS, as well as the limitations of other social policies imposed by EC 95/2016 (Igor et al., 2022), and the financialization of social and health policies (Bahia & Scheffer, 2022). These developments have led, on the one hand, to the replacement of policies with beneficial effects, such as the Stork Network for the Maternal and Child Care Network (RAMI), which provided care for pregnant women, and on the other hand, to the discontinuity of universal policies and the commodification of health services (Bahia & Scheffer, 2022), his has widened the gap in access and coverage of services and limited health rights, even at the primary care level. Consequently, Brazil faces significant challenges in achieving the targets set forth in the second sustainable development goal (SDG2), which aims to reduce the incidence of LBW and contribute to the reduction of infant mortality (Brasil, 2022).
Assessing the quality and reliability of secondary data is crucial. In this study, we sourced data from government databases, specifically health information systems, which are widely acknowledged for maintaining high-quality standards. However, the also study presents limitations. For example, since analyses the study uses aggregated data by region or federal unit, we could not identify the individual or familial level factors a associated with LBW, which is relevant information to better support policy planning. Additionally, administrative records may contain errors, and temporal analysis can be sensitive to random fluctuations, affecting the interpretation of changes in the prevalence of low birth weight.
Conclusion
The research findings demonstrate that LBW rates exhibit a spatial and temporal distribution that is unevenly dispersed across Brazil. The unequal distribution of LBW rates reflects the health and socioeconomic conditions prevalent in various Brazilian states. Historically, public policies have ignored social and spatial dynamics, resulting in capitalist dynamics that marginalize areas lacking adequate infrastructure and qualified labor, thereby adversely affecting people’s health and life. Based on our observation that more developed regions of the country exhibit higher LBW rates, we conclude that the availability and utilization of healthcare services are critical factors in reducing infant mortality and increasing LBW rates. Therefore, to improve the population’s living conditions, public policies and actions aimed at reducing health inequalities and inequities are imperative. This may include strengthening the Unified Health System (SUS), implementing income transfer programs, adopting quota policies for vulnerable groups, and promoting gender equity in access to education and the labor market.
Data Availability
The data, codebook, and analytic code described in the manuscript will be made available upon request.
References
Agbozo, F., Abubakari, A., Der, J., & Jahn, A. (2016). Prevalence of low birth weight, macrosomia and stillbirth and their relationship to associated maternal risk factors in Hohoe Municipality. Ghana Midwifery, 40, 200–206. https://doi.org/10.1016/j.midw.2016.06.016.
Antunes J. L. F., & Cardoso, M. R. A. (2015). Uso da análise de séries temporais em estudos epidemiológicos. Epidemiologia, Serviço e Saúde. Brasília, DF, 24(3), 565–576. https://doi.org/10.5123/S1679-49742015000300024.
Bahia, L., & Scheffer, M. (2022). Financeirização na saúde. Cadernos De Saúde Pública, 38(Suppl 2), e00119722. https://doi.org/10.1590/0102-311XPT119722.
Barros, F. C., Victora, C. G., Matijasevich, A., Santos, I. S., Horta, B. L., Silveira, M. F., & Barros, A. J. D. (2008). Preterm births, low birth weight, and intrauterine growth restriction in three birth cohorts in Southern Brazil: 1982, 1993 and 2004. Cadernos De Saude Publica, 24(Suppl 3(SUPPL.3). https://doi.org/10.1590/S0102-311X2008001500004.
Basel, K. C. A., P. L., & Singh, S. (2020). Low birth weight and its associated risk factors: Health facility-based case-control study. Plos One, 15(6), e0234907. https://doi.org/10.1371/journal.pone.0234907.
Beraldo, F. C., Vaz, I. M. F., & Naves, M. M. V. (2022). Nutrição, atividade física e obesidade em adultos: aspectos atuais e recomendações para prevenção e tratamento. 14(1), 57–62. http://rmmg.org/artigo/detalhes/1521.
Bernal, J. L., Cummins, S., & Gasparrini, A. (2018). The use of controls in interrupted time series studies of public health interventions. International Journal of Epidemiology, 47(6). https://doi.org/10.1093/ije/dyy135.
Brasil (2022). Índice de Desenvolvimento Sustentável das Cidades Brasileiras. https://idsc.cidadessustentaveis.org.br/map/indicators/baixo-peso-ao-nascer.
Coimbra, L. C., Silva, A. A. M., Mochel, E. G., Alves, M. T. S. S. B., Ribeiro, V. S., Aragão, V. M. F., & Bettiol, H. (2003). Fatores Associados à inadequação do uso Da assistência pré-natal. Revista De Saúde Pública, 37, 456–462. https://doi.org/10.1590/S0034-89102003000400010.
Cutland, C. L., Lackritz, E. M., Mallett-Moore, T., Bardají, A., Chandrasekaran, R., Lahariya, C., Nisar, M. I., Tapia, M. D., Pathirana, J., Kochhar, S., & Muñoz, F. M. (2017). Low birth weight: Case definition & guidelines for data collection, analysis, and presentation of maternal immunization safety data. Vaccine, 35(48), 6492–6500. https://doi.org/10.1016/j.vaccine.2017.01.049.
De Albuquerque, M. V., Viana, A. L., De d’Ávila, L. D., Ferreira, M. P., Fusaro, E. R., & Iozzi, F. L. (2017). Regional health inequalities: Changes observed in Brazil from 2000–2016. Ciência & Saúde Coletiva, 22(4), 1055–1064. https://doi.org/10.1590/1413-81232017224.26862016.
de Andrade, C. L. T., Szwarcwald, C. L., & de Castilho, E. A. (2008). Baixo peso Ao Nascer no Brasil De Acordo com as informações sobre nascidos vivos do Ministério Da Saúde, 2005. Cadernos De Saúde Pública, 24(11), 2564–2572. https://doi.org/10.1590/S0102-311X2008001100011.
de Souza Buriol, V. C., Hirakata, V., Goldani, M. Z., & da Silva, C. H. (2016). Temporal evolution of the risk factors associated with low birth weight rates in Brazilian capitals (1996–2011). Population Health Metrics, 2016 14:1(1), 1–10. https://doi.org/10.1186/S12963-016-0086-0. 14.
Fan, R. G., Portuguez, M. W., & Nunes, M. L. (2013). Cognition, behavior and social competence of preterm low birth weight children at school age. Clinics, 68(7), 915–921. https://doi.org/10.6061/clinics/2013(07)05.
Garcia, L. P., & Santana, L. R. (2011). Evolução das desigualdades socioeconômicas na mortalidade infantil no Brasil, 1993–2008. Ciência & Saúde Coletiva, 16(9), 3717–3728. https://doi.org/10.1590/S1413-81232011001000009.
Gonçalves, C. V., Cesar, J. A., & Mendoza-Sassi, R. A. (2009). Qualidade E eqüidade na assistência à Gestante: Um estudo de base populacional no sul do Brasil. Cadernos De Saúde Pública, 25(11), 2507–2516. https://doi.org/10.1590/S0102-311X2009001100020.
Igor, R., Oliveira, S., Aparecida, M., & Ferreira, S. (2022). A Emenda Constitucional n° 95/2016 e as Implicações para os Recursos da Assistência Estudantil do IFRN. FINEDUCA - Revista de Financiamento Da Educação, 12. https://doi.org/10.22491/2236-5907109019.
Jorge, M. H. P., de Gotlieb, M., S. L. D., & Laurenti, R. (2001). A saúde no Brasil: análise do período 1996 a 1999. A saúde no Brasil: análise do período 1996 a 1999, 237. https://pesquisa.bvsalud.org/portal/resource/essiqueira/biblio-935933.
Lima, M. C. B., de Oliveira, M., de Lyra, G. S., de Roncalli, C., A. G., & Ferreira, M. A. F. (2013). A desigualdade espacial do Baixo Peso Ao Nascer no Brasil. Ciência & Saúde Coletiva, 18, 2443–2452. https://doi.org/10.1590/S1413-81232013000800029.
Mathewson, K. J., Chow, C. H. T., Dobson, K. G., Pope, E. I., Schmidt, L. A., & Van Lieshout, R. J. (2017). Mental health of extremely low birth weight survivors: A systematic review and meta-analysis. Psychological Bulletin, 143(4), 347–383. https://doi.org/10.1037/BUL0000091.
Minagawa, A. T., Biagoline, R. E. M., Fujimori, E., de Oliveira, I. M. V., de Moreira, A. P. C. A., & Ortega, L. D. S. (2006). Baixo peso Ao Nascer E condições maternas no pré-natal. Revista Da Escola De Enfermagem Da USP, 40(4), 548–554. https://doi.org/10.1590/S0080-62342006000400014.
Pedraza, D. F. (2021). Sistema De informações sobre nascidos vivos: uma análise da qualidade com base na Literatura. Cadernos Saúde Coletiva, 29(1), 143–152. https://doi.org/10.1590/1414-462x202129010106.
Pereira, J. A., Rondó, P. H. C., Lemos, J. O., Pacheco de Souza, J. M., & Dias, R. S. C. (2010). The influence of birthweight on arterial blood pressure of children. Clinical Nutrition, 29(3), 337–340. https://doi.org/10.1016/J.CLNU.2010.01.005.
Predebon, K. M., Mathias, T. A., de Aidar, F., T., & Rodrigues, A. L. (2010). Desigualdade sócio-espacial expressa por indicadores do Sistema De Informações Sobre Nascidos Vivos (SINASC). Cadernos De Saúde Pública, 26(8), 1583–1594. https://doi.org/10.1590/S0102-311X2010000800012.
Rondó, P. H. C., Lemos, J. O., Pereira, J. A., Oliveira, J. M., & Innocente, L. R. (2008). Relationship between birthweight and arterial elasticity in childhood. Clinical Science (London England: 1979), 115(10), 317–326. https://doi.org/10.1042/CS20070420.
Rondó, P. H. C., Lemos, J. O., Pereira, J. A., Oliveira, R. G., Freire, M. B. S., & Sonsin, P. B. (2010). The relationship between birth weight and insulin resistance in childhood. The British Journal of Nutrition, 103(3), 386–392. https://doi.org/10.1017/S000711450999184X.
Sicuri, E., Bardají, A., Sigauque, B., Maixenchs, M., Nhacolo, A., Nhalungo, D., Macete, E., Alonso, P. L., & Menéndez, C. (2011). Costs Associated with Low Birth Weight in a rural area of Southern Mozambique. Plos One, 6(12), e28744. https://doi.org/10.1371/journal.pone.0028744.
Silva, L. R., da, Christoffel, M. M., & de Souza, K. V. (2005). História, conquistas e perspectivas no cuidado à Mulher E à criança. Texto & Contexto - Enfermagem, 14(4), 585–593. https://doi.org/10.1590/S0104-07072005000400016.
Sistema de Informações sobre Nascidos Vivos (SINASC): Plataforma de Ciência de Dados aplicada à Saúde (PCDaS) | PCDaS. SINASC, & Fiocruz (2020). https://pcdas.icict.fiocruz.br/conjunto-de-dados/sistema-de-informacao-sobre-nascidos-vivos/.
Tela, F. G., Bezabih, A. M., & Adhanu, A. K. (2019). Effect of pregnancy weight gain on infant birth weight among mothers attending antenatal care from private clinics in Mekelle City, Northern Ethiopia: A facility based follow-up study. Plos One, 14(3). https://doi.org/10.1371/JOURNAL.PONE.0212424.
Wardlaw, T. M. (2004). Low Birthweight: Country, Regional and Global Estimates. UNICEF. https://books.google.com.br/books?id=ciHZ-RTA3lQC.
World Health Organization (2010, January). P07 Disorders related to short gestation and low birth weight, not elsewhere classified. Nternational Classification of Diseases and Related Health Problems. https://scholar.google.com/scholar_lookup?title=Disorders+related+to+short+gestation+and+low+birth+weight,+not+elsewhere+classified&publication_year=2016&.
Funding
The project was done with no specific support.
Author information
Authors and Affiliations
Contributions
A.V., A.R.M.G., and M.M. designed the study. A.V., I.W.O.A., and R.F.O. collected data and built the database. A.V., I.W.O.A., and L.A. outlined the analytical strategy. A.V., S.P.X., L.A., R.F.O., and I.W.O.A. performed the statistical analyses, interpreted the results, and drafted the manuscript. M.M., P.R., A.R.M.G., A.F., L.A., S.P.X., and M.D.V. interpreted the results and provided critical feedback on the manuscript. P.H.R., A.F., and L.A. reviewed the manuscript. All authors approved the final version of the manuscript and agreed to be responsible for all aspects of the work.
Corresponding author
Ethics declarations
Conflict of Interest Disclosures
The authors have no conflicts of interest relevant to this article to disclose.
Ethical Issue
According to Resolution n. 466/2012 of the National Research Ethics Commission of the National Health Council of Brazil, informed consent and approval by the Research Ethics Committee are not required.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Victor, A., Aguiar, I.W.O., Flores-Ortiz, R. et al. Social Inequalities in Child Development: Analysis of Low-Birth-Weight Trends in Brazil, 2010–2020. J of Prevention 45, 545–555 (2024). https://doi.org/10.1007/s10935-024-00768-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10935-024-00768-0