
Abstract
Purpose Mental health concerns are common after a workplace injury, particularly amongst those making a compensation claim. Yet there is a lack of research exploring the effect of modifiable elements of the return-to-work process on mental health. The aim of this study is to examine the impact of perceived injustice in the interactions between claim agents and claimants on mental health symptoms in the 12-month following a musculoskeletal (MSK) workplace injury. Methods A cohort of 585 workers compensation claimants in Victoria, Australia were interviewed three times over a 12-month period following a workplace MSK injury. Perceptions of informational and interpersonal justice in claim agent interactions were measured at baseline, and the Kessler Psychological Distress (K6) scale was administered as a measure of mental health at all three timepoints. Path analyses were performed to examine the direct and indirect effects of perceived justice at baseline on concurrent and future mental health, after accounting for confounding variables. Results Each 1-unit increase in perceptions of informational and interpersonal justice, indicating poorer experiences, was associated with an absolute increase of 0.16 and 0.18 in respective K6 mental health score at baseline, indicating poorer mental health on a 5-point scale. In addition, perceived justice indirectly impacted mental health at 6-month and 12-month, through sustained negative impact from baseline as well as increased risk of disagreements between the claim agent and claimant. Conclusions This finding has highlighted the importance of perceived justice in claim agent interactions with claimants in relation to mental health following a work-related MSK injury.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Workplace injuries are a major public health concern. For example, in Australia, workplace injuries resulted in $28.2 billion in direct and indirect costs in 2012/2013, with 85% of these costs related to loss of earnings, borne by the worker and society [1]. In 2015/2016, injury and musculoskeletal (MSK) disorders accounted for 90% of all Australian workers’ compensation claims requiring a week or more off work, totalling 93,890 [2]. These patterns are not unique to Australia and are echoed across most developed economies [3]. To minimise time lost to injury, it is important that return to work and compensation processes are designed to aide and not impede the recovery process, facilitating sustained return to work.
While most of those injured at work recover and return to work as expected, some have a more complex path. One factor important to recovery is mental health. Individuals with physical occupational injuries are at greater risk of developing a mental health problem than those injured in other settings [4]. Further, the prevalence of mental health conditions after a workplace injury is high, with 30–50% meeting screening criteria for depression [5, 6]. Mental health problems following injury can persist for many years and frequently lead to poorer recovery and return to work trajectories [7,8,9,10,11,12]. Research has shown that involvement in a claims settlement process may exacerbate the issue, with those making a claim for their injury demonstrating poorer mental health outcomes than those who do not make a claim [13, 14]. While some research suggests this may be a result of more stressful experiences [15, 16], the elements of the claims process that may be producing stress have not been extensively explored.
One potential element is perceived injustice, or unfairness, in the claims-making process, identified as a strong recurring theme amongst those making claims [17]. Perceived injustice in the claims process can be conceptualised through the four key dimensions of organizational justice: distributive justice, referring to perceived fairness of outcomes; procedural justice, or fairness of the processes that lead to the outcomes; interpersonal or relational justice, perceptions of politeness and respect in interactions; and informational justice, fairness in the provision of information regarding procedures and outcomes [18,19,20,21].
Perceived injustice surrounding the experience of an injury has been associated with prolonged symptoms of post-traumatic stress and depression, and more positive perceptions of organizational justice have been linked to lower risk of poor mental health outcomes [22, 23]. Yet, there is little research exploring the effect of perceptions of justice in the work injury claims process on mental health outcomes. One cross-sectional study found that poor perceptions of procedural justice in the compensation process for those injured at work were associated with poorer mental health [25]. However, this relationship has yet to be examined prospectively, an important distinction since mental health may also impact perceptions of justice. In addition, while perceived unfairness in the procedures and outcomes of a claim may not be easily resolved, respectful, open, and informative interactions between the claim agent and the claimant are modifiable factors that could be targeted to improve health outcomes. Therefore, it is important to examine the effect of perceived justice in the interactions between claim agents and claimants.
This study explores prospectively the effect of interpersonal and informational justice in claim agent interactions on mental health in the first 12 months after an occupational MSK injury. If perceived justice in the claims process is found to impact mental health, this could have significant implications for the ways in which agents manage the claims process and interact with claimants.
Methods
Population and Recruitment
A prospective cohort of workers compensation claimants in Victoria, Australia, was recruited between June 2014 and July 2015. In Victoria, workplace injuries resulting in 10 or more days of absence are eligible for workers’ compensation coverage through Worksafe Victoria (WSV), for 85% of the labour force. The assessment and management of workers’ compensation claims in Victoria is performed by one of five claims agent organisations. The claim agent organisation for an individual worker is determined by the organisation which their employer is insured with. The cohort was recruited through random sampling within the WSV compensation scheme administrative records.
The original cohort (n = 869) included workers seeking compensation for work-related MSK disorders or mental health disorders (Fig. 1). However, in order to examine the effect of perceived justice on comorbid mental health problems among those with a physical injury, only the 678 participants seeking compensation for an MSK disorder were retained. All claimants over the age of 18, with a singular injury in the soft-tissue of the back or upper extremity, resulting in more than 10 days of absence from work were included in the sample. The cohort is described in greater detail elsewhere [26]. Although all workers’ compensation claimants should have at least one interaction with their claim agent, 93 respondents reported having no interactions with their claim agent at the baseline interview and were, therefore, excluded from analyses. We examined if reporting no contact with a claim agent was associated with various demographic, workplace, and health care provider contact characteristics. We did not observe any differences across age, sex, immigration status, workplace size, return to work status at baseline, or time since injury. However, respondents who reported not having contact with their claim agent were also more likely to report not having contact with a health care provider (20% vs. 5% reporting no health care provider contact). After removing these respondents, we had an eligible baseline sample of 585 respondents.

Flow diagram of study sample selection
Data Collection
Interviews were conducted by telephone at baseline, with follow-up interviews 6 months and 12 months after baseline. Data were collected regarding perceived justice in claim agent interactions, disagreements with claim agents, general health and mental health, severity of injury, as well as job and work information and demographic variables.
The median time between date of incapacity, or the first date at which the injured worker could not perform regular duties, and baseline interview for this sample was 110 days (Interquartile range (IQR 89 days to 131 days). The median time since incapacity at the second interview was 326 days (IQR 303 days to 354 days), and 503 days (IQR 480 days to 532 days) at the time three interview.
Of the 585 eligible participants who completed the baseline interview, 432 (73.8%) completed the 6-month interview, and 392 (67.0%) took part at 12 months. Logistic regression analyses were run to examine factors associated with an increased or decreased likelihood of attrition at 6 months or 12 months. Independent variables included time since injury, immigrant status, sex, age, return-to-work (obtained at baseline), mental health (obtained at baseline), injury severity, and perceived interpersonal justice and informational justice. Separate models were run with interpersonal and informational justice given the collinearity between these two measures. Results revealed that younger age was related increased likelihood of loss to follow-up at both time points. Increasing time since injury was associated with increased likelihood of attrition at time 2, while increased injury severity was associated with increase likelihood of attrition at time 3. No relationship was observed between baseline mental health or interpersonal or interactional justice and attrition.
Outcome Variable: Mental Health
Mental health was measured using the six-item Kessler psychological distress scale (K6), administered at baseline, 6 months and 12 months [27]. This scale was designed to screen for serious mental illness (SMI) in the general population and has been validated against World Health Organization (WHO) Composite international Diagnostic Interview Short-Form (CIDI-SF) scales for anxiety and mood disorders [27, 28]. The K6 is used in the Australian National Survey of Mental Health and Well-being [29].
Respondents are asked about the frequency with which they experienced six symptoms in the past 30 days (e.g., “so depressed that nothing could cheer you up”), with answers to each item scored on a 5-point scale ranging from 0 or ‘none of the time’ to 4 or ‘all of the time’. Scores are subsequently summed. A cut-off point of 13 has been used to indicate a serious mental illness and has been found to have a sensitivity of 0.36 and specificity of 0.96 [27]. However, in order to capture greater variation over time, the outcome variable used for analyses was the mean score across the six items, rather than using this cut-point to produce a dichotomous variable where 0 equals the lowest possible score (best mental health) and 4 equals the highest possible score (worse mental health). Internal consistency of the scale in this sample was found to be high (α = 0.91). Scores were not found to have substantial skew or kurtosis.
Independent Variables
Interpersonal and Informational Justice
Items addressing perceived justice of the claims process were adapted from those developed for use with a Canadian cohort seeking compensation for a work-related MSK injury [30]. At the baseline interview, respondents were asked about their perceptions of interpersonal and informational justice in their interactions with their current claim agent case-manager. Interpersonal justice in the RTW claim agent interactions were measured using two items addressing the politeness, dignity and respect with which the claim agent communicated (e.g., “treated you in a polite manner”). Informational justice in the RTW claim agent interactions was measured with five items addressing the truthfulness and thoroughness of the information provided (e.g., “provided you with the information you needed”).
Responses for all items for interpersonal and informational justice were measured on a 5-point scale ranging from ‘Strongly Agree’ to ‘Strongly Disagree’. The mean score on items for each of the two constructs was computed and standardized to a 5-point scale, with 1 indicating optimal claim agent performance and 5 indicating the least optimal claim agent performance.
Informational and interpersonal justice have been found to be correlated, but distinct constructs [30, 31]. Internal validity of the two scales has been found to be high, 0.89 for the informational scale, and 0.90 for the interpersonal scale [30]. Both scales have also been found to possess concurrent validity; higher informational and interpersonal justice scores are correlated with lower claim acceptance and longer length of delay in the claim decision, as well as the worker reporting that they had returned to work too soon and that the duration of workplace accommodations they received was too short.
Confirmatory factor analysis (CFA) was undertaken to confirm this factor status and results indicated a model with two separate constructs exhibited better fit to the data than one singular construct. As a result, they were included as separate scales. Internal consistency was also found to be high for both the informational (α = 0.90) and interpersonal (α = 0.89) justice scales in this sample. The correlation between the interpersonal and information justice scales was 0.70.
Disagreement with Claim Agent
During the 6-month interview, respondents were asked if they had had any disagreement about their claim with their claim agent, and whether that disagreement had been resolved. This was asked of all participants, whether or not they had returned to work. It was hypothesised that informational and interpersonal justice may have an indirect effect on subsequent mental health through increasing the likelihood of disagreements with the claim agent. As a result, disagreement with claim agent was included as a mediating variable. The variable used in analysis was coded into three levels, no disagreements, resolved disagreements and unresolved disagreements.
Other Covariates
Other variables were collected at the baseline interview using self-report, including sex, age, whether the individual was an immigrant or born in Australia, union membership, and whether they were living with a domestic partner. Return-to-work status was measured by asking participants whether they had returned to work since injury, for how long, and whether they were currently working, with answers categorised into three groups; no RTW, RTW for < 1 month, and sustained RTW for more than 1 month. Self-rated injury severity was measured on a 5-point scale (very slight to very severe).
Analysis
The initial eligible sample totalled 585 respondents. Of these, 16 respondents were missing 1 or more items within the interpersonal scale, and 70 respondents were missing 1 or more items within the informational scale. Mean scores were imputed for those with a score on at least one item within each scale, an approach recommended by Newman for item-level missingness on the basis that listwise deletion of missing responses is more likely to lead to a biased estimate than imputing values [32]. Only those who responded to at least one item within both the interpersonal and informational scales were retained to maintain the same study sample for both models, this resulted in the removal of two responses. After imputing scores for those with 1 or more items on each scale, the remaining 20 respondents (3.4%) missing all items on the informational or interpersonal scale, or on one or more exogenous covariates were removed, leaving an analytical sample of 565 respondents.
A logistic regression was run with missingness as the outcome, and variables without missing data; time since injury, immigrant status, sex, age and return to work as covariates to determine whether the final sample was representative of those who responded. This revealed that the only variable predictive of missingness was baseline return-to-work status, with those who had returned to work, or had sustained return-to-work being more likely to be missing from the analytical dataset (p = 0.032).
To help understand the relationships, and potential overlap between items on the K6 and our independent variables, we conducted a confirmatory factor analysis including items from each of these measures. This analysis demonstrated that the K6 scale items measured a distinct construct to perceived informational and interpersonal justice items, which suggests that these are three distinct constructs (results not shown, available upon request).
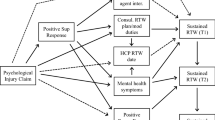
A path modeling approach was undertaken to estimate the direct effect of interpersonal and informational justice on mental health at baseline, 6 months and 12 months, as well as their indirect effects on mental health at 6 months and 12 months via mental health at baseline, and disagreements with claim agent reported at 6 months. These hypothesised effects are displayed in Fig. 2.

Conceptual model
Two separate path models were fit for interpersonal and informational justice. Both models adjusted for the effect of union membership, being born in Australia, living with a partner, injury severity, sex, age, return to work and time between injury and baseline interview. On the Kessler scale, 99.1% of respondents completed all six items at baseline, with 0.9% missing 5 or fewer items, 1.4% missing 5 or fewer items at 6 months and 0.5% missing 5 or fewer items at 12 months. Scores were imputed for these respondents. The full Information Maximum Likelihood estimation method was used to ensure the inclusion of the remaining respondents who did not answer any of the items on endogenous variables, including mental health at all three timepoints and disagreements with claim agent.
Model fit was assessed using goodness of fit indices including the model Chi square, the Bentler Comparative Fit Index (CFI) and the Root Mean Square Error of Approximation (RMSEA). Relationships with estimates close to 0 were removed to improve model fit. Data preparation and descriptive analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC) and path analyses were run using Mplus version 8 (Muthen & Muthen, Los Angeles, CA).
Finally, secondary analyses were undertaken to examine the effect of interpersonal and informational justice on the likelihood of reaching the threshold of 13 on the K6 scale at any of the three interviews, indicating a likely serious mental illness. Two separate logistic regressions were run using serious mental illness as the binary outcome, with either impersonal or informational justice, alongside union membership, being born in Australia, living with a partner, injury severity, sex, age, return to work and time between injury and baseline interview as covariates.
Results
Table 1 presents demographic, work and injury characteristics of the sample. Overall, 55.6% of the sample were male, the mean age was 43.8 years and 72.9% were born in Australia. By the first interview, 76.5% of the sample had attempted or sustained return to work. Severity of injury at the time of occurrence was self-rated as severe or very severe by 75.4% of the sample.
Table 2 describes the findings pertaining to organizational justice, disagreements with claim agent and mental health variables. The vast majority of the sample agreed or strongly agreed with interpersonal justice items, indicating that the claim agent case manager treated them in a polite manner (92.5%) and with dignity and respect (91.3%). Agreement with informational justice items was slightly lower, ranging from 89.0% agreeing or strongly agreeing that their claim agent was open and truthful in their communications, to 73.4% agreeing or strongly agreeing that the claim agent explained the RTW process carefully and completely. Overall, 25.2% reported having a disagreement with their claim agent between the time of their injury and the 6-month interview, and only 10.8% in total reported that this disagreement had been resolved.
Across the sample, K6 mental health scores improved slightly over time. The mean of all mean K6 mental health scores, where 0 is complete absence of symptoms and 4 is highly prevalent symptoms was 1.3 (SD = 1.1) at baseline interview, 1.1 (SD = 1.1) at the 6-month interview and 1.0 (SD = 1.0) at the 12-month interview.
Table 3 presents total, direct and indirect effect estimates for the organizational justice scales on mental health at baseline, 6 months and 12 months. After adjusting for the effect of covariates, both interpersonal and informational justice had a significant direct effect on mental health at baseline: a 1-unit increase in interpersonal and informational justice scores were associated with an absolute increase of 0.16 and 0.18 in respective K6 mental health score.
However, baseline organizational justice had only an indirect effect on mental health at follow-up: a 1-unit increase in interpersonal and informational justice were associated with a 0.15 and 0.16 respective increase in K6 mental health score at 6 months and a 0.12 and 0.14 respective increase at 12 months. These effects were entirely mediated, with poorer perceived justice leading to worse mental health scores at baseline and increased likelihood of disagreements with the claim agent at 6 months, which were subsequently related to poorer mental health at 6 months and 12 months.
In both models, disagreements with the claim agent, measured at 6 months, was found to have a small direct effect on mental health at 6 months, and a small indirect effect on mental health at 12 months. Having a disagreement compared to no disagreement and having an unresolved disagreement in comparison to a resolved disagreement, was associated with a 0.16 and 0.15 respective increase in K6 mental health scores at 6 months, in the interpersonal and informational models. The indirect effect on K6 mental health at 12 months was 0.09 and 0.08, via increasing K6 mental health scores at 6 months.
The Chi square test of model fit was significant at the 95% level for both models, indicating that the model may not be a good fit to the data. However, both path models presented good fit compared with a null model, with CFI > 0.95 and residual fit-based indices also indicated good fit, with root mean square RMSEA < 0.03.
Secondary analyses revealed that a 1-unit increased in informational and interpersonal justice were associated with a 27.5% (95% CI 6.8–52.2%, p = 0.007) and 19.5% (95% CI − 1 to 44.2%, p = 0.06) increased odds of reaching the threshold for a serious mental illness at any of the three interviews.
Discussion
While there is a body of literature linking workplace injuries and claim-making processes with poor mental health [4, 13, 14], there is a paucity of research exploring why this relationship might exist and how the workplace injury compensation system could be adapted to minimize risk of mental illness. This study found that one potentially modifiable factor impacting mental health after a workplace injury is perceived injustice in the interactions between claim agents and claimants.
Perceived justice in interactions with claim agents shortly after injury was found to be associated with mental health for those with work-related MSK disorders. While poorer perceptions of justice did not directly impact long-term mental health, they were associated with poorer mental health at baseline, and this association was sustained at 6 and 12 months. Perceived injustice was also associated with increased likelihood of disagreements between the claim agent and claimant, which subsequently had a negative association with longer term mental health. Although the association between perceived justice and mental health appears to be relatively modest, secondary analyses revealed that each respective 1-unit increase in the informational and interpersonal justice variables is associated with a 28% and 20% increase, respectively, in the odds of serious mental illness (defined as a K6 score of 13 and above).
These findings build upon the extensive evidence of poor mental health outcomes amongst those involved in a workers’ compensation claim, adding to the growing evidence that perceived injustice surrounding the experience of a compensated work-related injury may be one factor contributing to worse mental health among this injury population [22,23,24]. Further, this study extends previous work on the association between perceived injustice within the claims process and mental health in three important ways: by measuring the individual effect of interpersonal and informational justice, by demonstrating the long-term nature of this effect and finally by revealing the pathways through which this effect may occur [25].
The findings of this study have implications for service delivery models among workers’ compensation claimants. Given we observed that negative perceptions of claim agent fairness and communication were associated with an increased odds of mental health conditions, it would seem beneficial to ensure the training of claim agents includes ways to enhance perceptions of fairness, and thoroughness and clarity of the information provided to claimants. It should be noted that while over 90% of respondents agreed that their claim agent was polite and treated them with dignity and respect, more than a quarter did not believe that they explained the claims process carefully or completely, with just under a quarter expressing that their claim agent did not consider their specific needs when communicating with them. As a result, careful and considerate provision of information are target areas for improvement.
Some of the strengths of this study include the use of established measures of organizational justice, and the longitudinal study design, following claimants over a period of 12 months after injury to examine longer-term outcomes. In addition, the inclusion of disagreements between the claimant and the claim agent in the analytical model contributes to a fuller understanding of how perceptions of justice may impact long-term mental health.
One potential limitation of the current work is that mental health and perceived justice were measured concurrently at baseline, and we lack information on pre-existing mental health conditions, meaning reverse causality may be an issue. We cannot establish whether mental health problems created issues with claim agent interactions, or if mental health problems may have changed perceptions of these interactions. However, a confirmatory factor analysis did reveal that the K6 and the two measures of perceived justice represented three distinct constructs, meaning there was not conceptual overlap. Further, to explore the potential for reverse causality, we conducted a sub-analysis to examine if baseline mental health is associated with time two assessment of claim agent interactions, for those respondents still in contact with their claim agent between the baseline and time two interview. The results of this analysis suggest that previous mental health is not associated with perceptions of claim agent interactions, and therefore may not be a confounder in the relationship between claim agent performance and future mental health (details available on request). Additionally, even if pre-existing mental health problems among claimants did increase the likelihood of poorer interactions with claim agents, this does not minimize the importance of these findings, since poor interactions with those who are already experiencing a mental illness may still exacerbate symptoms and delay recovery. Another limitation is that those who had returned to work by baseline interview had higher odds of being missing from the analytical sample, therefore the results may not be representative of this group. However, since only 20 respondents (3.4%) were excluded, it is unlikely that this difference would impact the results to a large extent. Finally, since the majority of claimants in this sample had returned to work prior to their first interview, the results may not be generalizable to those who have greater difficulty in returning to work.
In conclusion, this study has highlighted the importance of fair, open, and respectful communications, and the provision of clear and thorough information to claimants with work-related injuries. High quality randomized control trials are required to establish the benefit of increased perceived justice in claim agent interactions on mental health, amongst those with and without pre-existing serious mental illness.
References
Safework Australia. The cost of work-related injury and illness for Australian employers, workers and the community: 2012–13. Safework Australia. 2015. https://www.safeworkaustralia.gov.au/system/files/documents/1702/cost-of-work-related-injury-and-disease-2012-13.docx.pdf. Accessed 20 Sept 2018.
Safework Australia. Australian workers’ compensation statistics 2015–16. Safework Australia. 2016. https://www.safeworkaustralia.gov.au/system/files/documents/1801/awcs_2015-16_report-20171023_v3_0.pdf. Accessed 20 Sept 2018.
Takala J, Hämäläinen P, Saarela KL, et al. Global estimates of the burden of injury and illness at work in 2012. J Occup Environ Hyg. 2014;11(5):326–337.
Kim J. Depression as a psychosocial consequence of occupational injury in the US working population: findings from the medical expenditure panel survey. BMC Public Health. 2013;13(1):303.
Carnide N, Franche RL, Hogg-Johnson S, et al. Course of depressive symptoms following a workplace injury: a 12-month follow-up update. J Occup Rehabil. 2016;26(2):204–215.
Keogh JP, Nuwayhid I, Gordon JL, et al. The impact of occupational injury on injured worker and family: outcomes of upper extremity cumulative trauma disorders in Maryland workers. Am J Ind Med. 2000;38(5):498–506.
Chin WS, Shiao JSC, Liao SC, et al. Depressive, anxiety and post-traumatic stress disorders at six years after occupational injuries. Eur Arch Psychiatry Clin Neurosci. 2017;267(6):507–516.
Corbiere M, Sullivan MJL, Stanish WD, et al. Pain and depression in injured workers and their return to work: a longitudinal study. Can J Behav Sci. 2007;39(1):23–31.
Dong XS, Wang X, Largay JA, et al. Long-term health outcomes of work-related injuries among construction workers-findings from the National Longitudinal Survey of Youth. Am J Ind Med. 2015;58(3):308–318.
Dozois DJA, Dobson KS, Wong M, et al. Factors associated with rehabilitation outcome in patients with low back pain (LBP): prediction of employment outcome at 9-month follow-up. Rehabil Psychol. 1995;40(4):243–259.
Kendrick D, Dhiman P, Kellezi B, et al. Psychological morbidity and return to work after injury: multicentre cohort study. Br J Gen Pract. 2017;67(661):e555–e564.
Lötters F, Franche RL, Hogg-Johnson S, et al. The prognostic value of depressive symptoms, fear-avoidance, and self-efficacy for duration of lost-time benefits in workers with musculoskeletal disorders. Occup Environ Med. 2006;63(12):794–801.
Elbers NA, Hulst L, Cuijpers P, et al. Do compensation processes imipair mental health? A meta-analysis. Injury. 2013;44(5):674–683.
Murgatroyd DF, Casey PP, Cameron ID, et al. The effect of financial compensation on health outcomes following musculoskeletal injury: systematic review. PLoS ONE. 2015;10(2):e0117597.
Grant GM, O’Donnell ML, Spittal MJ, et al. Relationship between stressfulness of claiming for injury compensation and long-term recovery: a prospective cohort study. JAMA Psychiatry. 2014;71(4):446–453.
O’Donnell ML, Grant G, Alkemade N, et al. Compensation seeking and disability after injury: the role of compensation-related stress and mental health. J Clin Psychiatry. 2015;76(8):e1000–e1005.
Murgatroyd DF, Cameron ID, Harris IA. Understanding the effect of compensation on recovery from severe motor vehicle crash injuries: a qualitative study. Inj Prev. 2011;17(4):222–227.
Adams JS. Inequity in social exchange. In: Berkowitz L, editor. Advances in experimental social psychology, vol. 2. New York: Academic Press; 1965. p. 267–299.
Thibaut JW, Walker L. Procedural justice: a psychological analysis. Hillsdale: L. Erlbaum Associates; 1975.
Bies RJ, Moag JF. Interactional justice: communication criteria of fairness. In: Lewicki RJ, Sheppard BH, Bazerman MH, editors. Research on negotiations in organizations, vol. 1. Greenwich: JAI Press; 1986. pp. 43–55.
Greenberg J. Organizational justice: yesterday, today, and tomorrow. J Manag. 1990;16(2):399–432.
Ndjaboué R, Brisson C, Vézina M. Organisational justice and mental health: a systematic review of prospective studies. Occ Environ Med. 2012;69(10):694–700.
Scott W, Trost Z, Milioto M, et al. Barriers to change in depressive symptoms after multidisciplinary rehabilitation for whiplash: the role of perceived injustice. Clin J Pain. 2015;31(2):145–151.
Sullivan MJL, Thibault P, Simmonds MJ, et al. Pain, perceived injustice and the persistence of post-traumatic stress symptoms during the course of rehabilitation for whiplash injuries. Pain. 2009;145(3):325–331.
Ioannou L, Braaf S, Cameron P, et al. Compensation system experience at 12 months after road or workplace injury in Victoria, Australia. Psychol Inj Law. 2016;9(4):376–389.
Dimitriadis C, LaMontagne AD, Lilley R, et al. Cohort profile: workers’ compensation in a changing Australian labour market: the return to work (RTW) study. BMJ Open. 2017;7(11):e016366.
Kessler RC, Barker PR, Colpe LJ, et al. Screening for serious mental illness in the general population. Arch Gen Psychiatry. 2003;60(2):184–189.
Furukawa TA, Kessler RC, Slade T, et al. The performance of the K6 and K10 screening scales for psychological distress in the Australian National Survey of Mental Health and Well-Being. Psychol Med. 2003;33(2):357–362.
Slade T, Grove R, Burgess P. Kessler psychological distress scale: normative data from the 2007 Australian National Survey of Mental Health and Wellbeing. Aust N Z J Psychiatry. 2011;45(4):308–316.
Franche RL, Severin CN, Lee H, et al. Perceived justice of compensation process for return-to-work: development and validation of a scale. Psychol Inj Law. 2009;2(3):225–237.
Colquitt JA. On the dimensionality of organizational justice: a construct validation of a measure. J Appl Psychol. 2001;86(3):386–400.
Newman DA. Missing data: five practical guidelines. Org Res Methods. 2014;17(4):372–411.
Acknowledgements
This study was supported through a Linkage Grant through the Australian Research Council (Grant # LP130100091). Peter Smith was supported by a Discovery Early Career Research Award, and is currently supported through a Research Chair in Gender, Work and Health from the Canadian Institutes of Health Research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the Monash University Human Research Ethics Committee.
Informed Consent
Written informed consent was obtained from all patients included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Orchard, C., Carnide, N. & Smith, P. How Does Perceived Fairness in the Workers’ Compensation Claims Process Affect Mental Health Following a Workplace Injury?. J Occup Rehabil 30, 40–48 (2020). https://doi.org/10.1007/s10926-019-09844-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10926-019-09844-3