
Abstract
Objective To compare the duration of financial compensation and the occurrence of a second episode of compensation of workers with occupational back pain who first sought three types of healthcare providers. Methods We analyzed data from a cohort of 5511 workers who received compensation from the Workplace Safety and Insurance Board for back pain in 2005. Multivariable Cox models controlling for relevant covariables were performed to compare the duration of financial compensation for the patients of each of the three types of first healthcare providers. Logistic regression was used to compare the occurrence of a second episode of compensation over the 2-year follow-up period. Results Compared with the workers who first saw a physician (reference), those who first saw a chiropractor experienced shorter first episodes of 100 % wage compensation (adjusted hazard ratio [HR] = 1.20 [1.10–1.31], P value < 0.001), and the workers who first saw a physiotherapist experienced a longer episode of 100 % compensation (adjusted HR = 0.84 [0.71–0.98], P value = 0.028) during the first 149 days of compensation. The odds of having a second episode of financial compensation were higher among the workers who first consulted a physiotherapist (OR = 1.49 [1.02–2.19], P value = 0.040) rather than a physician (reference). Conclusion The type of healthcare provider first visited for back pain is a determinant of the duration of financial compensation during the first 5 months. Chiropractic patients experience the shortest duration of compensation, and physiotherapy patients experience the longest. These differences raise concerns regarding the use of physiotherapists as gatekeepers for the worker’s compensation system. Further investigation is required to understand the between-provider differences.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
According to the 2010 Global Burden of Disease study, back pain causes more years of life with disability (YLD) than any of the other 291 conditions studied [1]. It also ranks sixth for the overall burden [1]. The point prevalence of back pain is estimated at approximately 9 %, and its lifetime prevalence is near 85 % [2, 3]. Back pain is the most common occupational injury in Canada and the United States [4, 5]. The Workplace Safety and Insurance Board (WSIB) of Ontario considers low back pain a high-impact claim responsible for 20 % of all lost time claims [6], and the Quebec’s Commission de la Santé et de la Sécurité du Travail paid approximately $540.5 million for vertebral conditions in 2008 [7].
In Canada, the provincial workers’ compensation boards provide financial support, medical assistance and rehabilitation to workers suffering from occupational injuries. Most provincial boards provide direct access to physicians and chiropractors. The exception is Quebec, where physicians are the sole gatekeepers of the workers’ compensation system [8]. In January 2004, the WSIB expanded direct access to physiotherapists and registered nurses (extended class) [9].
The Regulated Health Profession Act in Ontario (and the Physiotherapy Act) has allowed physiotherapists (outside of a public hospital) to assess and treat patients without a referral from a physician since 1991. Even after those policy changes went into effect, many private and quasi-public insurers continued to require a physician referral. A previous study concluded that delayed access to physiotherapy was a predictor of an increased duration of WSIB benefits [10] and that direct access to physiotherapy was associated with positive patient outcomes [11]. The evaluation of the WSIB Acute Low Back Injury Program of Care (ALBI) revealed that physiotherapists saw patients at a much later date after their injury than physicians or chiropractors did [12]; often, the first visit was so late that the patient was not eligible for treatment within the ALBI recommendation (at the time, patients were required to access care within 28 days after their injury). Those findings influenced the WSIB policy change.
The diagnostic and therapeutic tools for back pain differ among healthcare providers: physicians can prescribe medication and diagnostic imaging; chiropractors can prescribe X-rays but no medication; and physiotherapists cannot prescribe diagnostic imaging or medication. Therefore, it is possible that a patient who initially consults a physiotherapist or a chiropractor will be referred to a medical environment for complementary imaging or drug prescriptions. This situation could lead to a duplication of consultations, which could prolong the rehabilitation process. To develop the best first-line care possible, it is important to investigate whether these new providers have an impact on the return to work after an injury. In Washington, nurse practitioners as attending providers had disability and cost outcomes similar to those of physicians [13], and workers who first saw a chiropractor were less likely to become chronically work disabled [14]. The objective of the current study was to compare the duration of financial compensation and the occurrence of a second episode of compensation for back pain among patients seen by three types of first healthcare providers (physicians, chiropractors, and physiotherapist) in the context of the Ontario workers’ compensation board.
Methods
Study Design
The study analyzed data of a cohort of Ontarian workers who received at least 1 day of financial compensation from the Workplace Safety and Insurance Board (WSIB) between January 1 and June 30, 2005, for uncomplicated back pain, based on historical WSIB records. Each worker had a 2-year follow-up after the accident date. This historical cohort was initially assembled to build a prediction model for time on benefits [15, 16]. The recruitment period was chosen to match that of a smaller prospective cohort (the readiness to return to work (R-RTW) cohort [16, 17]) used to investigate the predictors of return to work status for musculoskeletal disorders. The University of Montreal Health Research Ethics Board approved this study (12-129-CERES-D).
Study Population
A simple random sample of 6500 out of a total of 18,974 claims was selected from all of the lost-time claims related to uncomplicated back pain that had an accident date during the recruitment period. We added 157 back pain subjects from the R-RTW cohort who were not randomly selected. We then excluded 1146 subjects because they did not have the main outcome of interest (100 % wage compensation; n = 413) or they had missing (n = 420) or aberrant data (n = 304) for the main independent variable. We excluded workers who initially sought treatment from a nurse because of their low number (n = 9). Our final sample comprised 5511 injured workers. More details regarding the selection process were reported in a previous article [18].
Source of Data
Following a work injury, the employer must report the injury to the WSIB within 3 days via their form containing: worker identification, details of the injury, earnings details, and claim information. The healthcare provider must complete their form when a patient’s injury is related to work, and workers may submit their form if they are concerned that the employer did not send theirs or if they incur expenses related to the injury. The worker form includes general information and the injury details while the healthcare provider form contains the following sections: patient and employer information, billing, incident dates and details sections, clinical information, treatment plan and return to work information. The WSIB cannot adjudicate the claim if too much information is missing; consequently, form submission rates are high (worker = 76.8 %, employer = 99.1 % and healthcare provider = 90.9 %), and the rate of missing information is low. In order to complete this project, relevant WSIB data from the claim file; the healthcare billing database; and the imaged files of the forms completed by the employers, workers and healthcare providers were extracted and assembled by an experienced programmer-analyst at the Institute for Work and Health (IWH). Information from the forms for the first 100 claims was independently collected from the imaged files by two extractors, and their agreement was high (98 %) [15]. Therefore, only one extractor per claim was used for the remaining claims. When the employer and the worker provided divergent information, the worker’s information was prioritized.
Description of the Study Variables
Independent Variable
The type of first healthcare provider seen was determined using data from the healthcare billing database and the healthcare provider form(s). We selected the first billing associated with a chiropractor (DC), a physician (MD, regardless of specialty), or a physiotherapist (PT) for each claim. When the date of the service provided was prior to the accident (n = 283), we either chose to correct an obvious data transcription error (i.e., the inversion of day and month) or to select the first billing after the accident date. We selected the first date on the first healthcare provider form for each claim. Dates preceding the accident (n = 287) were replaced with another date from the same form (the assessment, treatment or signature date) when available or were marked as missing. The first date and the associated provider from either the billing or the form were then selected. If two different providers were recorded on the same day (n = 96), the one who completed the healthcare provider form was considered the first healthcare provider.
Dependent Variables
Three outcomes were analyzed: the duration of the first episode of 100 % wage compensation, the duration of the first episode of any wage compensation (full or partial) and the occurrence of a second episode of compensation for the same claim during the follow-up period. We considered that a second episode of compensation occurred when the worker received income compensation (full or partial) after the end of the first episode of any wage compensation. The outcomes were obtained from the compensation administrative database for 2 years after the accident date.
Covariables
Socio-demographic factors: age at time of injury, sex and annual gross income were extracted from the claim file. The preferred language of communication was obtained from the employer and/or worker form (% of agreement = 100 %). The French and English languages were combined as they demonstrated a similar association with our dependent variables. The postal code from the claim file was converted into the community size and the urban/rural indicator using the postal code conversion file [19].
Work-related factors: we used information from the claim file to determine the job tenure, national occupational code (NOC), the sector of economic activity (Statistics Canada 1980 Standard Industrial Classification [SIC-80] [20]) and the number of employees in the company. The number of employees was dichotomized into 20 or fewer and more than 20 employees because small companies do not have the same re-employment obligations as larger ones [21]. The NOC from the claim file was converted into the physical demands of the job (manual, non-manual and mixed work) using an exposure matrix [22, 23]. The employer and worker’s forms contained information about union membership (% of agreement = 96.3 %). The employer also specified the availability of early return to work programs on their form and whether they doubted that the injury was related to work. We considered this answer as an indicator of an adversarial relationship with the employer.
Injury-related factors: the claim file contained information about previous lost time claim(s), the part of the body affected and the nature of the injury. We categorized the affected body part into four anatomical regions and the nature of the injury into least-severe cases (non-specific backache) and more-severe case (disc disorders, sciatica, herniated lumbar disc, radiculitis) based on a previously used classification [24, 25]. The worker’s and employer’s forms specifically asked whether the worker had had a similar injury in the past (% of agreement = 78.4 %). The healthcare provider form contained information about task limitations. Because different versions of the healthcare provider form were used during the study period, we grouped the ability to use public transportation, the ability to operate a motor vehicle and other specified task limitations together under “any task limitations” to combine the information from the different versions of the form. More details regarding the construction of these variables have been reported elsewhere [18].
Use of health services: the number of days between the accident date and the first healthcare consultation was calculated to control for the timing of the first consultation.
Analysis
Most of the covariables had low levels (<5 %) of missing data, and only 3.5 % of all values were missing. Only, the following variables had more than 5 % of missing values: job tenure (28.5 %), sector of economic activity (19.0 %), employer’s doubt that the injury was work-related (13.3 %), restricted use of public transportation (11.8 %) or a motor vehicle (11.3 %), any task limitations (10.2 %), and the availability of an early return to work program (6.9 %). We assumed that data were missing at random because Little’s missing completely at random test was significant (Chi squared = 44.5, df = 27, P = 0.018) and because we did not find a clear pattern of missing values. To fill in the variables with missing values we applied multiple imputations by using Markov Chain Monte Carlo simulations. We generated twenty different imputed data sets. In order to respect the 100-parameter limit in SPSS, the sector of economic activity and the community size were not used as predictors. The imputation used all the others available variables as predictors. The analysis were performed in every imputed data sets and the pooled estimates were generated by using Rubin’s algorithms [26].
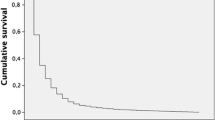
We conducted two models of multivariable survival analyses (Cox model) to compare the duration of financial compensation for back pain (dependent variable) for the three types of first healthcare providers (independent variable). We created a multivariable logistic regression model to compare the occurrence of a second episode of compensation (dependent variable) between the three types of first healthcare providers (independent variable). Bivariable analyses (survival analysis or logistic regression) between the dependent variables and all the other variables were conducted prior to data imputation. To control for confounding variables, an initial model was built that included all of the individual characteristics and health behaviors with a P < 0.25 or less in the bivariable analysis [27]. We formed a reduced model by removing the covariates with the largest P values one by one until all of the variables had a P < 0.25 according to the Wald test (confirmed with the likelihood ratio test). Excluded or non-included variables were reintroduced one at a time. Variables were left in the model if they were significant (P < 0.25) or if they caused a change of 15 % or more in the main regression coefficient. The linearity assumption of continuous variables was assessed graphically and collinearity was assessed by using variance inflation factor. Assumptions of non-informative censoring were found satisfactory. We tested the proportional hazard assumption by introducing an interaction term with a time-dependent covariate and found that the hazards of the three healthcare providers were not proportional. After analyzing the Kaplan–Meier survival curves for the three types of healthcare providers (Figs. 1, 2), we decided to treat the type of first healthcare provider as a time-dependent variable. Therefore, we created two Heaviside functions for the effect of the first healthcare provider (0–149 and 150–730 days).

Kaplan–Meier survival curves for the first episode of 100 % wage compensation by the first healthcare provider

Kaplan–Meier survival curves for the first episode of any wage compensation by the first healthcare provider
We excluded the 163 subjects that did not ended their first episodes of compensation by the end of the follow-up period prior to building the logistic regression model that compared the occurrence of a second episode of income compensation for the same claim (dependent variable) across the three types of first healthcare providers (independent variable) using the same modeling strategy to control for confounding. The linearity assumption of continuous variables was assessed graphically. All comparisons were considered statistically significant at P < 0.05. We performed all analyses using SPSS for Mac (version 22.0, IBM Corporation, Armonk, NY, USA).
Results
Of the 5511 compensated workers included in the sample, 85.3 % first saw a medical doctor (n = 4710), 11.4 % (n = 627) first saw a chiropractor, and 3.2 % (n = 174) first saw a physiotherapist. The median numbers of days of the first episode of full wage compensation were 7.0 (95 % confidence interval (CI) 5.8–8.2), 8.0 (95 % CI 7.5–8.5) and 19.0 (95 % CI 15.5–22.5) for the workers who first consulted chiropractors, physicians and physiotherapists, respectively. When the partial wage compensation associated with a gradual return to work was included, the median number of days of the first episode of any wage compensation were 8.0 (95 % CI 6.6–9.4), 10.0 (95 % CI 9.5–10.0) and 25.0 (95 % CI 20.3–29.7) for the workers who first consulted chiropractors, physicians and physiotherapists, respectively. Among the workers who completed their first episode of any wage compensation during the follow-up, 15.0 % (n = 92) of the chiropractic care seekers, 16.2 % (n = 738) of the physician care seekers and 23.7 % (n = 40) of the physiotherapist care seekers had a second compensation episode. The complete characteristics of the analyzed sample are reported elsewhere [18].
Bivariable Results
The results of the bivariable analyses between the workers’ characteristics and the study outcomes are presented in Tables 1 and 2.
Kaplan–Meier Survival Curves
The Kaplan–Meier survival curves for the duration of the first episode of 100 % wage compensation and the duration of the first episode of any wage compensation according to the three types of healthcare providers are presented in Figs. 1 and 2. Up to 150 days post-injury, the curves are regular and distinct in both figures. Physiotherapists showed the longest duration of compensation, and chiropractors showed the shortest. After 150 days, the three curves cross and demonstrate a similar trajectory until the end of the follow-up period (730 days). Few events occurred after 150 days among the chiropractic (n = 20) and physiotherapy (n = 10) groups.
Multivariable Results
Our three final multivariable models are presented in Tables 1 and 2. We report the pooled estimates from the multiple imputations. All the HRs and ORs obtained from the listwise analysis (not reported) were within 10 % of the variation of the reported pooled estimates.
Over the first 149 days, the workers who first sought care from a chiropractor had a significantly greater hazard of ending their compensation episode compared with the workers who first consulted a physician (100 % wage compensation: HR = 1.20 [1.10–1.31], P value ≤ 0.001; any wage HR = 1.19 [1.09–1.30], P value ≤ 0.001) and those who first consulted a physiotherapist had a significantly lower hazard of ending their compensation episode (100 % wage compensation: HR = 0.84 [0.71–0.98], P value = 0.028; any wage HR = 0.79 [0.68–0.93], P value = 0.005). From 150 to 730 days, few events occurred among the chiropractic and physiotherapy groups, and the type of first healthcare provider was not a significant predictor of termination of the first compensation episode during this time period. Both of our final multivariable Cox models that assessed the duration of the first episode of compensation controlled for sex, age, language, job tenure, union membership, employer’s doubts regarding the work-relatedness of the injury, the physical demands of the job, gross earnings, the availability of an early return to work program, number of employees at the company, previous similar injury, any task limitations, the nature of the injury, the body part affected and the time interval between the accident and the first healthcare consultation.
The workers who first sought care from a physiotherapist had significantly higher odds of having a second episode of compensation compared with the workers who first consulted a physician (OR = 1.49 [1.02–2.18], P value = 0.038). The workers who first sought care from a chiropractor did not have significantly different odds of having a second episode of compensation compared with the workers who first consulted a physician (OR = 0.83 [0.65–1.06], P value = 0.135). Our final multivariable logistic regression model that assessed the occurrence of a second compensation episode controlled for sex, age, community size, language, union membership, employer’s doubts regarding the work-relatedness of the injury, physical demands, gross earnings, previous similar injury, previous 100 % wage compensation, the nature of the injury and the body part affected.
Discussion
Summary of Main Findings
The type of first healthcare provider was a significant predictor of the duration of the first episode of compensation only during the first 5 months of compensation. When compared with medical doctors, chiropractors were associated with shorter durations of compensation and physiotherapists with longer ones. Physiotherapists were also associated with higher odds of a second episode of financial compensation.
Consistency with the Findings of Other Studies
Several randomized controlled trials have compared the effectiveness of medical, chiropractic and physiotherapy care for back pain among the general population, and the results did not clearly favor any type of care in terms of pain and functional status [28–35]. Reviews and a recent observational study of occupational back pain failed to clarify whether one type of care was more effective or cost effective [36–38]. Most of the previous studies considered the main or exclusive healthcare provider. There is, however, a distinction between the “main” healthcare provider and the “first” provider. In fact, the first provider will not be the main provider in approximately 50 % of cases [39–42]. Few studies have investigated the impact of the first healthcare provider. The cohort study of American workers with back pain conducted by Turner et al. [14] found that the first healthcare provider was one of the main predictors of work disability after a year. In accordance with our findings, workers who first sought chiropractic care were less likely to be work-disabled after 1 year compared with workers who first sought other types of medical care [14]. Regarding physiotherapy care, a recent review concluded that direct access to physiotherapy care was associated with better patient outcomes compared with referred physiotherapy care [11]. We did not retrieve any study that directly compared physiotherapy care with other types of first healthcare providers in the context of occupational back pain, probably because most workers’ compensation systems still require a referral for physiotherapy. However, a study comparing primary physiotherapy care with usual emergency department care concluded that physiotherapy care leads to a prolonged time before patients return to their usual activities [43].
According to previous studies, back pain care provided by physiotherapists and chiropractors adheres more closely to guidelines (reduced use of diagnostic imaging, surgery and opioids) than medical care does [44–46]. Our findings partly support that finding because 75.9 % of the workers seeking chiropractic care did not seek an additional type of care within the first month [18]. However, 58.6 % of workers who first consulted a physiotherapist also sought medical care within the first month [18]. At the time of our study, physiotherapists could not prescribe medication or diagnostic imaging, which might explain this additional use of medical services. Additionally, direct access to physiotherapy for injured workers was only in place for a year at the time of our study, and physiotherapists were probably not familiar with the workers’ compensation system.
Strengths and Limitations
The large sample size of this study enabled us to perform our multivariable modeling with sufficient statistical power during the first 150 days. Because few events occurred after 150 days, our modeling of the impact of the first healthcare provider during that period is less robust. The addition of information from the employee, employer and healthcare provider forms to the data routinely collected by the WSIB provided us with many potential confounders to consider. We combined the information from two different sources (the healthcare billing database and the healthcare provider form) to determine the type of first healthcare provider, thus limiting misclassification.
The information that we used was collected by the WSIB for administrative purposes; therefore, its psychometric proprieties have not been assessed. When comparing the outcomes of different types of healthcare providers in an observational study, it is essential to consider the possibility of confounding by indication. We used several variables to determine the needs of the injured workers. We specifically used two dichotomized variables to control for the burden of back pain: injury severity and task limitations. Without knowing how these variables compared to established functional status questionnaires, it is impossible to completely rule out confounding by indication. We found that the workers who sought chiropractic care experienced shorter durations of compensation. Most previous studies found that medical patients had more severe pain, disability, comorbidity and lower general health status than chiropractic patients [39, 44, 47–53]. If our analysis contains residual confounding, the real difference between the types of provider might be diminished. We also found that the physiotherapy patients experienced longer compensation durations and more second episodes of compensation. In order to attenuate the associations we measured, physiotherapy patients should experience more severe back pain in a way that was not captured by our analysis. While increased pain among physiotherapy patients is always a possibility, we believe this is unlikely because the physiotherapy patients experienced a longer time interval between the injury and the first consultation [18]. Usually, patients with more severe injuries will seek immediate medical care at an emergency room [54]. Additionally, the physiotherapy patients were more likely to seek an additional type of care, which has previously been associated with longer compensation durations [55, 56].
Since a relatively small percentage of workers who first saw a physiotherapist (3.2 %) was included 1 year after the policy change, it is possible that our analysis captured early adopter of the new policy and that the association between first consulting a physiotherapist and the compensation duration now differ from the ones assessed in 2005. Generalizations of our findings to other jurisdictions should be performed with caution since it was hypothesized that the compensation policy might have a greater influence than the type of care sought [38].
Recommendations for Futures Research
Further investigations should be conducted for a better understanding of why patients who initially seek physiotherapy care experience longer compensation durations. The factors that influence the decision to seek physiotherapy as the first source of care should be better understood. The process of care that follows the initial type of care should also be evaluated. Because a differential use of additional health services was observed, the trajectory of care might also be an important predictor of the compensation duration.
Conclusion
The type of first healthcare provider sought for occupational back pain was associated with the duration of compensation over the first 5 months. The chiropractic patients experienced the shortest compensation duration, and the physiotherapy patients experienced the longest. The physiotherapy patients were also more likely to experience a second episode of compensation. Our results raised concerns regarding the use of physiotherapists as gatekeepers of Ontario’s worker’s compensation system. Further investigations should be conducted to better understand the reasons behind the observed differences between the three types of first healthcare providers.
Abbreviations
- ALBI:
-
Acute low back pain injury program of care
- ANOVA:
-
Analysis of variance
- CI:
-
Confidence interval
- DC:
-
Doctor of chiropractic
- HR:
-
Hazard ratio
- IRSST:
-
Institut de Recherche en Santé Sécurité au Travail
- IWH:
-
Institute for Work and Health
- MD:
-
Medical doctor
- NOC:
-
National occupational code
- OR:
-
Odds ratio
- PT:
-
Physiotherapist
- ROC:
-
Receiver operating characteristics
- R-RTW:
-
Readiness to return to work
- SD:
-
Standard deviation
- SIC-80:
-
Standard international classification 1980
- WSIB:
-
Workplace Safety and Insurance Board
References
Hoy D, March L, Brooks P, Blyth F, Woolf A, Bain C, et al. The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. 2014;73(6):968–74. doi:10.1136/annrheumdis-2013-204428.
Schmidt CO, Raspe H, Pfingsten M, Hasenbring M, Basler HD, Eich W, et al. Back pain in the German adult population: prevalence, severity, and sociodemographic correlates in a multiregional survey. Spine. 2007;32(18):2005–11. doi:10.1097/BRS.0b013e318133fad8 (Phila Pa 1976).
Cassidy JD, Carroll LJ, Côté P. The Saskatchewan health and back pain survey: the prevalence of low back pain and related disability in Saskatchewan adults. Spine. 1998;23(17):1860–6.
Deyo RA, Mirza SK, Martin BI. Back pain prevalence and visit rates: estimates from U.S. national surveys, 2002. Spine. 2006;31(23):2724–7. doi:10.1097/01.brs.0000244618.06877.cd (Phila Pa 1976).
Leroux I, Dionne CE, Bourbonnais R, Brisson C. Prevalence of musculoskeletal pain and associated factors in the Quebec working population. Int Arch Occup Environ Health. 2005;78(5):379–86. doi:10.1007/s00420-004-0578-2.
WSIB. By the numbers: 2013 WSIB statistical report. Toronto, ON: Workplace Safety and Insurance Board. http://www.wsibstatistics.ca. Accessed 3 Aug 2014.
Lamarche D, Veilleux F, Provencher J, Boucher P. Statistiques sur les affections vertébrales 2005–2008. Québec; QC: Commission de la santé et de la sécurité du travail du Québec2009 Contract No.: ISBN: 978-2-550-56793-6.
Loi sur les accidents du travail et les maladies professionnelles (LATMP). L.R.Q., c. A-3.001 (1985).
WSIB. Un plus grand choix de professionels de la santé pour les travailleurs blessés ou malades. Bull Polit. 2004;17(1):3.
McIntosh G, Frank J, Hogg-Johnson S, Bombardier C, Hall H. Prognostic factors for time receiving workers’ compensation benefits in a cohort of patients with low back pain. Spine. 2000;25(2):147–57 (Phila Pa 1976).
Ojha HA, Snyder RS, Davenport TE. Direct access compared with referred physical therapy episodes of care: a systematic review. Phys Ther. 2014;94(1):14–30. doi:10.2522/ptj.20130096.
Gregory AW, Pentland W. Program of care for acute low back injuries: one-year evaluation report. Maitland Consulting Inc.; 2004.
Sears JM, Wickizer TM, Franklin GM, Cheadle AD, Berkowitz B. Nurse practitioners as attending providers for injured workers: evaluating the effect of role expansion on disability and costs. Med Care. 2007;45(12):1154–61. doi:10.1097/MLR.0b013e3181468e8c.
Turner JA, Franklin G, Fulton-Kehoe D, Sheppard L, Stover B, Wu R, et al. ISSLS prize winner: early predictors of chronic work disability: a prospective, population-based study of workers with back injuries. Spine. 2008;33(25):2809–18. doi:10.1097/BRS.0b013e31817df7a7 (Phila Pa 1976).
Steenstra IA, Busse JW, Tolusso D, Davilmar A, Lee H, Furlan AD, et al. Predicting time on prolonged benefits for injured workers with acute back pain. J Occup Rehabil. 2015;25(2):267–78. doi:10.1007/s10926-014-9534-5.
Steenstra IA, Franche RL, Furlan AD, Amick B 3rd, Hogg-Johnson S. The added value of collecting information on pain experience when predicting time on benefits for injured workers with back pain. J Occup Rehabil. 2015;. doi:10.1007/s10926-015-9592-3.
Bultmann U, Franche RL, Hogg-Johnson S, Cote P, Lee H, Severin C, et al. Health status, work limitations, and return-to-work trajectories in injured workers with musculoskeletal disorders. Qual Life Res. 2007;16(7):1167–78. doi:10.1007/s11136-007-9229-x.
Blanchette M-A. Première ligne de soins pour les travailleurs atteints de rachialgie occupationnelle: étude du délai de consultation et du premier fournisseur de services de santé [Ph.D. thesis by articles]: Université de Montréal. 2016.
Wilkins R. PCCF+ version 4G user’s guide: automated geographic coding based on the statistics Canada postal code conversion files. Health Analysis and Measurement Group. Statistics Canada, 64 pp. 2006.
Statistics Canada. Standard industrial classification—establishments (SIC-E) 1980. Statistics Canada. 2014. http://www23.statcan.gc.ca/imdb/p3VD.pl?Function=getVD&TVD=53446. Accessed 12 Aug 2015.
WSIB. Operational policy: responsibilities of the workplace parties in work reintegration. 2011.
Hébert F, Duguay P, Massicotte P, Levy M. Révision des catégories professionnelles utilisées dans les études de l’IRSST portant sur les indicateurs quinquennaux de lésions professionnelles. Montréal: IRSST1996 Contract No.: Études et recherches/Guide technique R-137.
Duguay P, Boucher A, Busque M, Prud’homme P, Vergara D. Lésions professionnelles indemnisées au Québec en 2005–2007: profil statistique par industrie-catégorie professionnelle. Études et recherches/Rapport R-749 Montréal: IRSST. 2012;202.
Dasinger LK, Krause N, Deegan LJ, Brand RJ, Rudolph L. Physical workplace factors and return to work after compensated low back injury: a disability phase-specific analysis. J Occup Environ Med. 2000;42(3):323–33.
Sinnott P. Administrative delays and chronic disability in patients with acute occupational low back injury. J Occup Environ Med. 2009;51(6):690–9. doi:10.1097/JOM.0b013e3181a033b5.
Rubin DB. Multiple imputation for nonresponse in surveys. Wiley; 2004.
Vittinghoff E, Glidden DV, Shiboski SC, McCulloch CE. Predictor selection. Regression methods in biostatistics. Berlin: Springer; 2012. p. 395–429.
Cherkin DC, Deyo RA, Battie M, Street J, Barlow W. A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for the treatment of patients with low back pain. N Engl J Med. 1998;339(15):1021–9. doi:10.1056/nejm199810083391502.
Hurwitz EL, Morgenstern H, Harber P, Kominski GF, Belin TR, Yu F, et al. A randomized trial of medical care with and without physical therapy and chiropractic care with and without physical modalities for patients with low back pain: 6-month follow-up outcomes from the UCLA low back pain study. Spine. 2002;27(20):2193–204. doi:10.1097/01.brs.0000029253.40547.84 (Phila Pa 1976).
Hurwitz EL, Morgenstern H, Kominski GF, Yu F, Chiang LM. A randomized trial of chiropractic and medical care for patients with low back pain: eighteen-month follow-up outcomes from the UCLA low back pain study. Spine. 2006;31(6):611–21. doi:10.1097/01.brs.0000202559.41193.b2 (Phila Pa 1976; discussion 22).
Meade TW, Dyer S, Browne W, Frank AO. Randomised comparison of chiropractic and hospital outpatient management for low back pain: results from extended follow up. BMJ. 1995;311(7001):349–51.
Meade TW, Dyer S, Browne W, Townsend J, Frank AO. Low back pain of mechanical origin: randomised comparison of chiropractic and hospital outpatient treatment. BMJ. 1990;300(6737):1431–7.
Petersen T, Larsen K, Nordsteen J, Olsen S, Fournier G, Jacobsen S. The McKenzie method compared with manipulation when used adjunctive to information and advice in low back pain patients presenting with centralization or peripheralization: a randomized controlled trial. Spine. 2011;36(24):1999–2010. doi:10.1097/BRS.0b013e318201ee8e (Phila Pa 1976).
Skargren EI, Carlsson PG, Oberg BE. One-year follow-up comparison of the cost and effectiveness of chiropractic and physiotherapy as primary management for back pain. Subgroup analysis, recurrence, and additional health care utilization. Spine. 1998;23(17):1875–83 (Phila Pa 1976; discussion 84).
Skargren EI, Oberg BE, Carlsson PG, Gade M. Cost and effectiveness analysis of chiropractic and physiotherapy treatment for low back and neck pain. Six-month follow-up. Spine. 1997;22(18):2167–77 (Phila Pa 1976).
Baldwin ML, Cote P, Frank JW, Johnson WG. Cost-effectiveness studies of medical and chiropractic care for occupational low back pain. A critical review of the literature. Spine J. 2001;1(2):138–47. doi:10.1016/S1529-9430(01)00016-X.
Brown A, Angus D, Chen S, Tang Z, Milne S, Pfaff J et al. Costs and outcomes of chiropractic treatment for low back pain (structured abstract). Health Technology Assessment Database 2005.
Butler RJ, Johnson WG. Adjusting rehabilitation costs and benefits for health capital: the case of low back occupational injuries. J Occup Rehabil. 2010;20(1):90–103. doi:10.1007/s10926-009-9206-z.
Cote P, Cassidy JD, Carroll L. The treatment of neck and low back pain: who seeks care? who goes where? Med Care. 2001;39(9):956–67.
Wasiak R, Pransky GS, Atlas SJ. Who’s in charge? Challenges in evaluating quality of primary care treatment for low back pain. J Eval Clin Pract. 2008;14(6):961–8. doi:10.1111/j.1365-2753.2007.00890.x.
Hurwitz EL, Chiang LM. A comparative analysis of chiropractic and general practitioner patients in North America: findings from the joint Canada/United States Survey of Health, 2002–03. BMC Health Serv Res. 2006;6:49. doi:10.1186/1472-6963-6-49.
Cote P, Baldwin ML, Johnson WG. Early patterns of care for occupational back pain. Spine. 2005;30(5):581–7. doi:10.1097/01.brs.0000154613.17511.dd (Phila Pa 1976).
Richardson B, Shepstone L, Poland F, Mugford M, Finlayson B, Clemence N. Randomised controlled trial and cost consequences study comparing initial physiotherapy assessment and management with routine practice for selected patients in an accident and emergency department of an acute hospital. Emerg Med J EMJ. 2005;22(2):87–92. doi:10.1136/emj.2003.012294.
Fritz JM, Kim J, Dorius J. Importance of the type of provider seen to begin health care for a new episode low back pain: associations with future utilization and costs. J Eval Clin Pract. 2015. doi:10.1111/jep.12464.
Allen H, Wright M, Craig T, Mardekian J, Cheung R, Sanchez R, et al. Tracking low back problems in a major self-insured workforce: toward improvement in the patient’s journey. J Occup Environ Med. 2014;56(6):604–20. doi:10.1097/jom.0000000000000210.
Amorin-Woods LG, Beck RW, Parkin-Smith GF, Lougheed J, Bremner AP. Adherence to clinical practice guidelines among three primary contact professions: a best evidence synthesis of the literature for the management of acute and subacute low back pain. J Can Chiropr Assoc. 2014;58(3):220–37.
Lim KL, Jacobs P, Klarenbach S. A population-based analysis of healthcare utilization of persons with back disorders: results from the Canadian Community Health Survey 2000–2001. Spine. 2006;31(2):212–8 (Phila Pa 1976).
Plenet A, Gourmelen J, Chastang JF, Ozguler A, Lanoe JL, Leclerc A. Seeking care for lower back pain in the French population aged from 30 to 69: the results of the 2002–2003 Decennale Sante survey. Ann Phys Rehabil Med. 2010;53(4):224–31. doi:10.1016/j.rehab.2010.03.006 (31–8).
Nyiendo J, Haas M, Goldberg B, Sexton G. Patient characteristics and physicians’ practice activities for patients with chronic low back pain: a practice-based study of primary care and chiropractic physicians. J Manipulative Physiol Ther. 2001;24(2):92–100. doi:10.1067/mmt.2001.112565.
Sharma R, Haas M, Stano M. Patient attitudes, insurance, and other determinants of self-referral to medical and chiropractic physicians. Am J Public Health. 2003;93(12):2111–7.
Cote P, Hogg-Johnson S, Cassidy JD, Carroll L, Frank JW, Bombardier C. Initial patterns of clinical care and recovery from whiplash injuries: a population-based cohort study. Arch Intern Med. 2005;165(19):2257–63. doi:10.1001/archinte.165.19.2257.
Hurwitz EL, Morgenstern H. The effects of comorbidity and other factors on medical versus chiropractic care for back problems. Spine. 1997;22(19):2254–63 (Phila Pa 1976; discussion 63–4).
Hestbaek L, Munck A, Hartvigsen L, Jarbol DE, Sondergaard J, Kongsted A. Low back pain in primary care: a description of 1250 patients with low back pain in danish general and chiropractic practice. Int J Fam Med. 2014;2014:106102. doi:10.1155/2014/106102.
Kosny A, Maceachen E, Ferrier S, Chambers L. The role of health care providers in long term and complicated workers’ compensation claims. J Occup Rehabil. 2011;21(4):582–90. doi:10.1007/s10926-011-9307-3.
Cote P, Hogg-Johnson S, Cassidy JD, Carroll L, Frank JW, Bombardier C. Early aggressive care and delayed recovery from whiplash: isolated finding or reproducible result? Arthritis Rheum. 2007;57(5):861–8. doi:10.1002/art.22775.
Cote P, Soklaridis S. Does early management of whiplash-associated disorders assist or impede recovery? Spine. 2011;36(25 Suppl):S275–9. doi:10.1097/BRS.0b013e3182388d32 (Phila Pa 1976).
Acknowledgments
The authors thank Ashleigh Burnet and many others from the WSIB for facilitating access to data. M. A. Blanchette is currently supported by a Ph.D. fellowship from the Canadian Institutes for Health Research (CIHR) and previously received Ph.D. Grants from both the Quebec Chiropractic Foundation and the CIHR strategic training program in transdisciplinary research on public health intervention (4P). The data extraction was funded through a grant from the WSIB Research Advisory Committee. Dr. Hogg-Johnson reports grants from Workplace Safety & Insurance Board Research Advisory Council, during the conduct of the study; grants from Ontario Ministry of Labour, outside the submitted work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare they have no other conflict of interest.
Rights and permissions
About this article

Cite this article
Blanchette, MA., Rivard, M., Dionne, C.E. et al. Association Between the Type of First Healthcare Provider and the Duration of Financial Compensation for Occupational Back Pain. J Occup Rehabil 27, 382–392 (2017). https://doi.org/10.1007/s10926-016-9667-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10926-016-9667-9