
Abstract
Although theoretical studies on Anesthesia Information Management Systems (AIMS) have proved their benefits, much less attention has been paid to researching the actual adoption of AIMS. Only a few studies from the USA and Western Europe have been published up to now. The purpose of this article is to assess the adoption, motivation for, and barriers to, usage of AIMS from the perspective of early Czech adopters of these systems. A questionnaire was used to gather adopters’ views on motivating factors, benefits encountered after introduction and obstacles perceived to adopting AIMS. Data about usage, costs and functionalities of each of the AIMS was obtained using semi-structured telephone interviews prior to sending out the questionnaire. Five AIMS from three different vendors in four academic hospitals (20% of Czech hospitals of this type) were identified. Improved clinical documentation and convenience for anesthesiologists was reported from every site. Lack of funds, however, was identified as the primary barrier to further adoption. The cost of introduction of AIMS per operating room varied between 1000 and 40,000 US dollars. Although the number of AIMS in the Czech Republic is limited, findings suggest that benefits have been experienced on every site. Findings corroborate previous studies from the USA and Western Europe.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In no medical fields other than anesthesia are the vital functions of a patient recorded so frequently and thoroughly. The principles were introduced more than a hundred and twenty years ago by Cushing and Codman [1]. The number of values recorded has risen as physiological principles were understood and new monitoring methods introduced. Fifty years ago, the first attempts emerged at using automatic electronic devices instead of pen and paper to record the anesthesia data [2].
A quantity of studies has already proved that the Automated Anesthesia Record Keeping System (AARKS) decreases the workload of the anesthesiologist [3] and the resulting data is more accurate [4] and much more frequently recorded [5]. Typical concerns were also rebutted since the AARKS does not diminish the anesthesiologist’s attention [6] and even improves his/her position in case of a lawsuit [7].
Using more functions and integration with other components of the hospital information system (HIS), a complex system was born – it is usually known as the Anesthesia Information Management System (AIMS), although the term Perioperative Information Management System is on occasions also used [8]. AIMS facilitates continuity of care from the preoperative to the postoperative phase and clinical decision systems have a measurable effect on the quality of care during anesthesia [9, 10].
However, much fewer studies are available on particular existing AIMS [11]. Also, studies on the actual usage of AIMS are limited to the USA and in part to Western Europe. In the USA at least 44% of American academic hospitals used or were considering using AIMS in 2008 [12], 75% used AIMS in 2014 with 84% adoption expected in 2020 [13]. The only existing European study claims that in 2010 15% of university-affiliated hospitals from twenty-two EU states used or were adopting AIMS [14].
As there is no existing study about AIMS in other European countries, the purpose of this article is to assess the adoption, motivation for, and barriers to, usage of AIMS from the perspective of early Czech adopters of these systems.
Methods
Initially, the main Czech suppliers of anesthesia monitors and ventilators were questioned about the AIMS they have provided or met in a Czech hospital when supplying equipment. Known Czech suppliers of medical information systems were approached with the same queries.
For every identified AIMS installation, a head of the corresponding site was contacted via telephone to provide the name of the physician with the most knowledge of that system or one responsible for running it.
Using a semi-structured telephone interview, firstly the appropriateness of the person questioned was established and then basic information about the AIMS installation was gathered using questions as set out in Table 1.
In the last phase, each physician from the previous phase received a more detailed questionnaire via email. The first part of the questionnaire covered the motivation to introduce AIMS in that hospital and the benefits encountered afterwards. The second part assessed perceived barriers to further adoption of AIMS in the respondent’s hospital and obstacles anticipated in non-adopter hospitals. Both parts took the form of a multiple-choice list, the possible answers being selected in accordance with previous studies [12, 14]. The opportunity to enter one’s own answers was also provided in both parts of the questionnaire. An open question asking, “Why do you think the AIMS development in the Czech Republic is much lower than in other modules of hospital information system?” formed the third part of the questionnaire. Further contact was maintained using e-mail to clarify potential ambiguities and/or problems of interpretation.
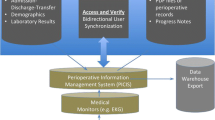
The whole process of acquiring data is depicted in Fig. 1.

Process of acquiring data for the study
Results
Initial response from Czech suppliers was obtained in all cases, and in every identified AIMS installation the responsible physician was identified and reached and his view (via phone and email in the second part) was obtained. Thus, it was possible to achieve a 100% response rate.
As a result of the initial enquiry a total of five installations of three different AIMS products were identified in four different Czech hospitals. Each of the hospitals can be defined as an academic hospital. One of the hospitals uses two different AIMS, one in general anesthesia, the other in cardiac anesthesia (it is not unusual that in some academic hospitals in the Czech Republic specialized anesthesia care is not part of the general anesthesia department). Each of the hospitals with AIMS has a full spectrum of HIS modules (e.g. clinical, radiology, laboratory, etc.)
Three installations of Centricity Anesthesia (GE), one of Metavision (IMDSoft) and one of FONS Enterprise (Stapro Pardubice – a local Czech supplier of medical information systems) were identified. More detailed information on each of the AIMS is set out in Table 2 – the different hospitals are described as Sites 1 to 4 (with denominations “Site 2A” and “Site 2B” describing the hospital with two different AIMS installed.
There are some 130 acute-care hospitals in the Czech Republic. About twenty of these can be seen as academic hospitals, since they are either an integral part of a medical faculty or have at least close ties to one. Only four of these hospitals have AIMS installed, and therefore only 20% of Czech academic hospitals have already adopted AIMS already.
When evaluating the actual usage from Table 2, four of the five sites use AIMS regularly with 90% or more physicians using AIMS when the Operating room (OR) is equipped. Only at Site 2B is the usage just limited (in fact, the only person using it is the responder, whilst other physicians have remained with the paper version).
The estimated cost varies from 1000 US dollars per OR at Site 2A (where Metavision software was installed in intensive care unit and for extension to OR the procurement of an all-in-one PC was all that was needed) to 40,000 US dollars in the case of GE Centricity Anesthesia in Sites 2B and 3 (where the system was acquired alongside other equipment).
Connected equipment varies from site to site. None of the systems are much integrated into HIS structures. Also, none of the AIMS have clinical decision support installed. AIMS at Sites 2B and 3 do not have an option to edit the stored data.
Motivating factors for introducing AIMS and actual benefits observed by the responders after introduction are set out in Table 3, with site descriptions corresponding to Table 2. The respondent from Site 1 added the benefit, “We encountered the possibility of further using acquired data and the anesthesiologist now has more time for the patient”. The respondent from Site 2B added the comment, “We acquired the system in a package alongside the anesthesia equipment, we did not have any say in its purchase”.
Perceived barriers to the further adoption of AIMS in the respondent’s hospital and the obstacles he/she anticipates in the non-adopter hospitals are set out in Table 4, with site descriptions again corresponding to Table 2. The respondent from Site 2A added the claim, “Established suppliers of IT are hindering the introduction of new and more functional solutions” and “Heads of anesthesia departments have no understanding of new technologies due to their age”. The respondent from Site 2B added the claim, “Anesthesiologists are not willing to learn the system and do not comprehend that it will save them time once they are proficient with it”.
The respondents give reasons for thinking that AIMS adoption in the Czech Republic is on a much lower scale than that of other HIS modules. These can be rephrased as follows:
AIMS is perceived as less important than other modules of HIS (Site 1, Site 4)
There are no financial incentives from payers of the health care system to introduce and use AIMS (Site 2A, Site 3)
Voluntary use of AIMS is not an option, only its compulsory use (enforcement by the authorities or the law) would make a difference (Site 2B, Site 3)
Discussion
Established 20% adoption of AIMS in Czech academic hospitals roughly corresponds to the known data from other EU countries from 2010 (15%) [14] – sadly no newer data is available. Nevertheless one can expect further development, as in the USA with expected adoption of 84% in 2020 [13].
Figures obtained in this study (from 1000 USD to 40,000 USD per OR) differ significantly from commonly reported sums of 4000 to 10,000 US dollars per OR [15]. The higher costs observed might be explained by low implementation in a multi-OR environment, since only in Site 1 is AIMS implemented in all existing OR.
There are not many integrated functions between AIMS and other HIS structures in the Czech Republic. Therefore, all these AIMS can be perceived to be more like AARKS, since none of the systems can facilitate the continuity of care. Also, AIMS in the Czech Republic lacks the clinical decision support already present in other systems [16]. Nevertheless, the huge usage in most of the sites shows the staff benefits from existing AIMS.
Two of the five existing AIMS in the Czech Republic do not have an option to edit the stored data – some AIMS in other states also lack this function [17]. This might be seen as a negative factor by users and decrease their willingness to use the system. Indeed, this could be one of the reasons why AIMS is not widely used in Site 2B.
Apart from the respondent from Site 2B all the others were motivated by envisaged improved clinical documentation and convenience for anesthesiologists. These factors materialized into observed benefits at all sites including Site 2B, and improved patient care was observed at three sites after AIMS adoption. This is in accordance with general findings in the literature [3, 6, 18, 19].
The responder at Site 2A also observed cost savings, cost benefits and increased patient throughput. Such findings have already been reported [20, 21].
At least some benefits, then, have evidently been observed at every site. The motivations to introduce, and benefits from introducing AIMS do not differ significantly from previous studies [12, 22].
As to the barriers, most responders feel the lack of funds to be the primary problem, but the anesthesiologists’ reluctance to use new technologies and their lack of understanding of possible benefits is also mentioned. Such observations are also further corroborated in answers to the final question. Ironically, this reluctance might best be affected by actually using the system, since according to the literature anesthesiologists’ opinions change when they actually have the opportunity to use such a system [23].
The suggestion of mandatory usage of AIMS might be a novelty, since as far as I know no such measure has been employed in any other country. However, proposing incentives to introduce AIMS might be a possibility, as in the USA under the Health Information Technology for Economic and Clinical Health Act [24].
It is highly probable that it was possible to identify all facilities using AIMS in the Czech Republic. However, since there are only five AIMS, this factor poses the greatest limitation of the study and results of this survey should be viewed accordingly. Also, at every site only a single physician (albeit the most skilled one) was questioned. Even so, this is one of the few studies on AIMS in Europe ever to take place and might well up to now be the only study carried out outside Western Europe. Hopefully it might prompt more research in this area and facilitate wider introduction of AIMS farther afield than just in the Czech Republic.
Conclusion
This study identified adoption of five different AIMS from three different vendors in four different academic hospitals in the Czech Republic, i.e. circa 20% of this type of facility in the Czech Republic. AIMS vary according to their functions, the equipment connected, and the price paid. Advanced functions of AIMS are limited, and no clinical support decision functions are implemented in any of the AIMS which have been adopted.
As seen from the adopters’ perspective, the motivations for introduction, the obstacles perceived to adoption, and the actual benefits observed afterwards do not differ significantly from previous findings in the literature. Some of the responders feel that incentives should be introduced to facilitate wider introduction of AIMS.
Abbreviations
- AARKS:
-
Automated Anesthesia Record Keeping System
- HIS:
-
Hospital Information System
- AIMS:
-
Anesthesia Information Management System
- OR:
-
Operating room
References
Sundararaman, L. V., and Desai, S. P., The Anesthesia Records of Harvey Cushing and Ernest Codman. Anesth. Analg. 126:322–329, 2018. https://doi.org/10.1213/ANE.0000000000002576.
Daub, D., Destunis, S., Halbach, M., vom Hövel, R., and Kalff, G., First experiences with a documentation system via display terminals. Acta Anaesthesiol. Belg. 23(Suppl):200–204, 1975.
Edsall, D. W., Deshane, P., Giles, C., Dick, D., Sloan, B., and Farrow, J., Computerized patient anesthesia records: Less time and better quality than manually produced anesthesia records. J. Clin. Anesth. 5:275–283, 1993.
Reich, D. L., Wood, R. K., Mattar, R., Krol, M., Adams, D. C., Hossain, S. et al., Arterial Blood Pressure and Heart Rate Discrepancies Between Handwritten and Computerized Anesthesia Records. Anesth. Analg. 91:612–616, 2000. https://doi.org/10.1213/00000539-200009000-00022.
Lerou, J. G., Dirksen, R., van Daele, M., Nijhuis, G. M., and Crul, J. F., Automated charting of physiological variables in anesthesia: A quantitative comparison of automated versus handwritten anesthesia records. J. Clin. Monit. 4(1):37–47, 1988.
Allard, J., Dzwonczyk, R., Yablok, D., Block, F. E., and Mcdonald, J. S., Effect of automatic record keeping on vigilance and record keeping time. Br. J. Anaesth. 74(5):619–626, 1995. https://doi.org/10.1093/bja/74.5.619.
Feldman, J. M., Do anesthesia information systems increase malpractice exposure? Results of a Survey. Anesth. Analg. 99(3):840–843, 2004. https://doi.org/10.1213/01.ANE.0000130259.52838.3B.
Simpao, A. F., Ehrenfeld, J. M., Special Case: Perioperative Information Management Systems. In: Ehrenfeld JM, Cannesson M, editors. Monit. Technol. Acute Care Environ., New York: Springer New York, 2014, p. 391–7. https://doi.org/10.1007/978-1-4614-8557-546.
Wax, D. B., Beilin, Y., Levin, M., Chadha, N., Krol, M., and Reich, D. L., The effect of an interactive visual reminder in an anesthesia information management system on timeliness of prophylactic antibiotic administration. Anesth. Analg. 104:1462–1466, table of contents, 2007. https://doi.org/10.1213/01.ane.0000263043.56372.5f.
Simpao, A. F., Tan, J. M., Lingappan, A. M., Gálvez, J. A., Morgan, S. E., and Krall, M. A., A systematic review of near real-time and point-of-care clinical decision support in anesthesia information management systems. J. Clin. Monit. Comput. 31(5):885–894, 2017. https://doi.org/10.1007/s10877-016-9921-x.
Stonemetz, J., Anesthesia information management systems marketplace and current vendors. Anesthesiol. Clin. 29:367–375, 2011. https://doi.org/10.1016/j.anclin.2011.05.009.
Egger Halbeis, C. B., Epstein, R. H., Macario, A., Pearl, R. G., and Grunwald, Z., Adoption of Anesthesia Information Management Systems by Academic Departments in the United States. Anesth. Analg. 107(4):1323–1329, 2008. https://doi.org/10.1213/ane.0b013e31818322d2.
Stol, I. S., Ehrenfeld, J. M., and Epstein, R. H., Technology Diffusion of Anesthesia Information Management Systems into Academic Anesthesia Departments in the United States. Anesth. Analg. 118(3):644–650, 2014. https://doi.org/10.1213/ANE.0000000000000055.
Balust, J., Egger Halbeis, C. B., and Macario, A., Prevalence of anaesthesia information management systems in university-affiliated hospitals in Europe. Eur. J. Anaesthesiol. 27:202–208, 2010. https://doi.org/10.1097/EJA.0b013e3283313fc2.
Sinclair, D. R., Methodologies of anesthesia information management system development. J. Clin. Anesth. 25:425–427, 2013. https://doi.org/10.1016/j.jclinane.2013.02.009.
Nair, B. G., Gabel, E., Hofer, I., Schwid, H. A., and Cannesson, M., Intraoperative clinical decision support for anesthesia: A narrative review of available systems. Anesth. Analg. 124(2):603–617, 2017. https://doi.org/10.1213/ANE.0000000000001636.
Vigoda, M. M., and Feinstein, D. M., Anesthesia information management systems. Adv. Anesth. 26:121–136, 2008. https://doi.org/10.1016/j.aan.2008.07.011.
Kooij, F. O., Klok, T., Hollmann, M. W., and Kal, J. E., Decision Support Increases Guideline Adherence for Prescribing Postoperative Nausea and Vomiting Prophylaxis. Anesth. Analg. 106(3):893–898, 2008. https://doi.org/10.1213/ane.0b013e31816194fb.
Nair, B. G., Newman, S.-F., Peterson, G. N., Wu, W.-Y., and Schwid, H. A., Feedback Mechanisms Including Real-Time Electronic Alerts to Achieve Near 100% Timely Prophylactic Antibiotic Administration in Surgical Cases. Anesth. Analg. 111:1293–1300, 2010. https://doi.org/10.1213/ANE.0b013e3181f46d89.
Lubarsky, D. A., Sanderson, I. C., Gilbert, W. C., King, K. P., Ginsberg, B., Dear, G. L., Coleman, R. L., Pafford, T. D., and Reves, J. G., Using an anesthesia information management system as a cost containment tool. Description and validation. Anesthesiology 86(5):1161–1169, 1997.
Egger Halbeis, C. B., and Epstein, R. H., The value proposition of anesthesia information management systems. Anesthesiol. Clin. 26(4):665–679, 2008. https://doi.org/10.1016/j.anclin.2008.07.007.
Shah, N. J., Tremper, K. K., and Kheterpal, S., Anatomy of an anesthesia information management system. Anesthesiol. Clin. 29(3):355–365, 2011. https://doi.org/10.1016/j.anclin.2011.05.013.
Pysyk, C. L., Jee, R., and Zunder, I., Change in staff anesthesiologists’ opinions of an anesthesia information management system (AIMS). J. Clin. Monit. Comput. 33(3):541–542, 2019. https://doi.org/10.1007/s10877-018-0178-4.
Gálvez, J. A., Rothman, B. S., Doyle, C. A., Morgan, S., Simpao, A. F., and Rehman, M. A., A Narrative Review of Meaningful Use and Anesthesia Information Management Systems. Anesth. Analg. 121(3):693–706, 2015. https://doi.org/10.1213/ANE.0000000000000881.
Acknowledgments
The author would like to acknowledge the help of Pavel Waldauf, M.D., Pavel Kellovský M.D., Robert Wagner, M.D., Michal Nejedlý, M.D., and Jiří Mokrejs, M.D., in providing information about each of the AIMS and that of Skans Victoria Airey for her invaluable language help during preparation of this article.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
None.
Ethical Approval
This article does not contain any studies with human participants or animals performed by the author.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Image & Signal Processing
Rights and permissions
About this article

Cite this article
Bruthans, J. Anesthesia Information Management Systems in the Czech Republic from the Perspective of Early Adopters. J Med Syst 44, 70 (2020). https://doi.org/10.1007/s10916-020-1545-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10916-020-1545-5