
Abstract
Family caregivers play an important role to care cancer patients since they exchange medical information with health care providers. However, relatively little is known about how family caregivers seek medical information using mobile apps and the Internet. We examined factors associated with medical information seeking by using mobile apps and the Internet among family caregivers and the general public using data from the 2014 Health Information National Trends Survey 4 Cycle 1. The study sample consisted of 2425 family caregivers and 1252 non-family caregivers (the general public). Guided by Comprehensive Model of Information Seeking (CMIS), we examined related factors’ impact on two outcome variables for medical information seeking: mobile apps use and Internet use with multivariate logistic regression analyses. We found that online medical information seeking is different between family caregivers and the general public. Overall, the use of the Internet for medical information seeking is more common among family caregivers, while the use of mobile apps is less common among family caregivers compared with the general public. Married family caregivers were less likely to use mobile apps, while family caregivers who would trust cancer information were more likely to use the Internet for medical information seeking as compared to the general public. Medical information seeking behavior among family caregivers can be an important predictor of both their health and the health of their cancer patients. Future research should explore the low usage of mobile health applications among family caregiver population.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
People use many means of seeking health information through various information technologies. The Internet has emerged as one of the most commonly used of these [1]. The Internet provides widespread access to health information and allows people to benefit from interacting with others and by sharing or exchanging information [2]. There are more than 70,000 websites that provide health information and more than 50 million people look for health information online each year [2]. In addition, mobile technology is also widely used as the means for researching health information and communication on the Internet [3]. Approximately 85% of the U.S. adults own a cell phone and among those, about 53% have smartphones and have used these to look for health information [4]. About 19% of those who own smartphones have downloaded a mobile health application (app) [4]. These software programs are downloaded and carried on mobile devices to achieve specific goals [5]. They have convenient designs so that people can learn and use easily, which can positively influence fitness and lifestyle education [6] and chronic disease management [7].
A number of prior studies examined factors for online health information seeking among individuals [8–10]. Kelly and colleagues (2010) examined factors associated with individuals seeking cancer information and found that female gender, marital status, and education positively predicted online information seeking [9]. Similarly, Oh (2015) examined predictors for online health information seeking among family caregivers and found that self-rated health and attention to the Internet were significantly predictive [10]. Lim and colleagues (2011) studied how Singaporean women adopt mobile phone technology to look for health information by applying the Technology Acceptance Model (TAM) [11]. They found that perceived usefulness and self-efficacy were significantly, positively predictive for seeking health information using mobile apps [11]. Previous research also studied health-related mobile apps in various clinical and other healthcare circumstances [7, 12, 13]. For instance, Pandey and colleagues (2013) assessed cancer-related apps available on the Apple app store and found that a large percentage of them (42.8%) were free and most of them (55.8%) had information with scientific evidence and confirmation [7].
Although previous studies investigated online health information seeking among the general population [2, 8, 9], relatively little is known about certain groups like family caregivers to cancer patients or survivors and how differently they seek the information compared with the general public. Family caregivers play an important role of seeking the information cancer patients need [14], in particular when those patients are too ill to look for the information themselves [10]. Family caregivers also play a crucial role in cancer care among cancer patients, in that they receive information from health professionals, provide physicians with patient information, and support treatment decision making [15]. Patients with medical information are more likely to control and deal with their unpredictable health, better follow their plans of care, and recover faster than those with less information [16, 17]. Although healthcare providers or physicians are perceived as a main source of health information [18], individuals also use online sources to seek health information [8, 10]. Meanwhile, Hesse and colleagues (2005) investigated individual preferences for cancer information sources and found that about 48.6% of individuals reported going online first and only 10.9% going to their physicians first [19].
In this study, we examine various predictors derived from Comprehensive Model of Information Seeking (CMIS). CMIS explains individuals’ seeking information from communication channels with a comprehensive approach [17]. Variables contained in CMIS consist of health-related factors, information carrier factors, and information-seeking actions [17]. First, health-related factors include demographics (i.e., race, age, sex, and marital status), direct experience (i.e., the degree of individuals experiencing diseases), salience (i.e., personal attention to diseases), and beliefs (i.e., self-efficacy) [10]. Second, information carrier factors consist of characteristics (i.e., individuals’ perception about the credibility of information) and utility of information sources (i.e., individuals’ assessment of the usefulness of information) [20]. This study incorporates an additional construct guided by another theoretical framework ‘Social Cognitive Theory (SCT)’ since incorporating additional variables depending on the context of a study can provide more predictive power [21]. Several prior studies included and examined variables including technology anxiety [11] and perceived personal risk and anxiety [22] in individuals seeking information. Thus, we include ‘anxiety’ as the additional construct of SCT. Based on these theoretical frameworks, we examine how these factors are associated with individuals using mobile apps and the Internet for medical information seeking and the difference between family caregivers and the general public.
Methods
Data source and study sample
We used the data from the 2014 Health Information National Trends Survey 4 Cycle 1 (HINTS 4), a nationally representative health information survey collected by the National Cancer Institute (NCI) [23]. The HINTS data includes various kinds of information related to how the general public in the U.S. use different channels of information technologies, look for health information, deal with their health, and monitor changes in their health behavior [23]. The HINTS data may be used to improve health information usage among individuals with barriers to access, to enhance health communication strategies and theories, and to reduce the burden of cancer among the population [23]. Prior studies have used this database to answer questions related to online health information seeking, cancer information seeking, and health seeking behavior using mobile health applications [10, 24, 25]. The sampling for HINTS 4 consists of two stages where in stage 1, random households were chosen from the U.S. residential address file and in stage 2, an individual in the chosen household was selected using the next birthday method [26]. The study sample was obtained from HINTS 4 Cycle 4 due to its availability of information on use of mobile apps and included 3677 respondents [23]. The HINTS data are deidentified and available for public use.
Variables
Our main outcomes of interest were ‘Use of Mobile apps’ and ‘Use of the Internet’. These dependent variables were based on the questions “in the past 12 months, have you used app(s) on a smart phone or mobile device to exchange medical information with a health care professional?” and “in the past 12 months, have you used the Internet to look for cancer information for yourself?”, respectively. The dependent variables were dichotomous variables coded as 1 = yes, 0 = no.
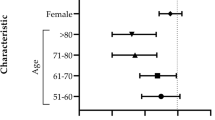
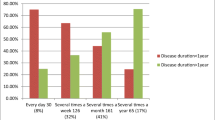
Health-related factors included demographic characteristics, direct experience, salience, and beliefs (self-efficacy). For demographic characteristics, ‘sex’, and ‘age’ were included as a binary variable (male or female) and a continuous variable, respectively. ‘Race’ consisted of ‘White, non-Hispanic’, ‘Black, non-Hispanic’ and ‘Hispanic’. ‘Marital status’ was created as a dichotomous variable coded as 1 = married or living as married, 0 = others (i.e., divorced, widowed, separated, and single). ‘Educational level (‘less than 11 years’, ‘high school graduate/some college’, and ‘college graduate/postgraduate’)’, and ‘income level (x) (‘x < $35,000′, ‘$35,000 ≤ x < $100,000′, ‘x ≥ $100,000′)’ were also included. A predictor for direct experience, ‘general health status (‘excellent/very good’, ‘good/fair’, and ‘poor’)’, was included. A predictor for salience was ‘interested in exchanging information (‘very’, ‘somewhat/a little’, and ‘not at all’)’, based on the questionnaire “how interested are you in exchanging information about diagnostic information (e.g., medical illnesses or diseases) with a health care provider electronically?” Predictors for beliefs (self-efficacy) were ‘confident in taking care of your health’ and ‘confident in getting cancer information’ with three categories: ‘completely/very’, ‘somewhat/a little’, and ‘not confident at all’, based on the questionnaire “overall, how confident are you about your ability to take good care of your health?” and “overall, how confident are you that you could get advice or information about cancer if you needed it?” respectively. As an information carrier factor, we included ‘trusting cancer information (‘a lot’, ‘some’, and ‘a little/not at all’)’, based on the questionnaire “in general, how much would you trust information about cancer from the internet (from smartphones or a tablet)?” As a predictor for anxiety, ‘concerned about the quality of the information’ was included as a dichotomous variable coded as 1 = yes, 0 = no. In addition, ‘family caregiver’ was created as a dichotomous variable based on the questionnaire “have any of your family members ever had cancer?”
Data analysis
With Pearson’s chi square tests, we first compared how significantly different family caregivers and the general public were in terms of all categorical variables. With a two-sample T-test, we also compared how significantly different family caregivers and the general public were in terms of a continuous variable, ‘age’. Based on the results from Pearson’s chi square tests and a T-test, we created interactions between a family caregiver and each variable that showed a significant difference. We then modeled the odds of mobile apps use and Internet use using four multiple logistic regression models (i.e., models 1 and 2 of mobile apps use and models 3 and 4 of Internet use). Models 1 and 3 included all predictors and control variables without interactions, while models 2 and 4 contained interaction terms of interest. Using these models, we examined how related predictors were associated with the use of mobile apps and the use of the Internet for medical information seeking among family caregivers and the general public and the difference between them.
Results
Table 1 shows the difference between ‘family caregivers’ and ‘the general public’ in terms of health-related factors, information carrier factors, and information-seeking actions. Pearson’s chi-square test results indicated that family caregivers and the general public were significantly different (p < .05) in a number of factors except for ‘income’, ‘general health status’, ‘being concerned about the quality of the information’, and ‘being interested in exchanging information’. Meanwhile, a two-sample T-test result showed that family caregivers and the general public were not significantly different in terms of age. Overall, more family caregivers than the general public (16.49% vs. 9.79%, respectively) used the Internet to look for cancer information, while fewer family caregivers than the general public (4.12% vs. 6.38%, respectively) used mobile apps to exchange medical information with a health professional.
Table 2 shows the results of our four logistic regression analyses. In models 1 and 2 of mobile apps use with and without interactions, Whites were less likely to use mobile apps for exchanging medical information with a health care professional than Blacks and Hispanics (OR 0.52, [95% CI 0.33–0.83]; OR 0.84, [95% CI 0.48–1.43]). As age increases by one year, the odds of using mobile apps for exchanging medical information decreases (OR 0.98, [95% CI 0.96–0.98]). However, no significant results were found for sex, marital status, and educational level for predicting the use of mobile apps for exchanging medical information. For income level, however, a higher level of income (≥$100,000) among individuals was associated with an increased likelihood of the use of mobile apps than the lowest income category (<$35,000) (OR 1.57, [95% CI 0.92–2.68]). Interestingly, a family caregiver was negatively predictive for the use of mobile apps for exchanging medical information (OR 0.57, [95% CI 0.39–0.81]). As compared to individuals who were ‘very’ interested in exchanging the information about diagnostic information, those who were interested ‘somewhat/a little’ and ‘not at all’ (OR 0.40, [95% CI 0.19–0.76]; OR 0.23, [95% CI 0.09–0.50]) were less likely to use mobile apps. Individuals who were concerned about the quality of the information from other sources were more likely to use mobile apps for exchanging information than those who were not (OR 2.11, [95% CI 1.30–3.45]). However, no significant results were found for trusting cancer information, general health status, and confidence in taking care of own health and getting cancer information. In model 2 including interactions, a significant interaction result between a family caregiver and marital status was found (OR 0.37, [95% CI 0.17–0.76]), implying that married or living as married caregivers were less likely to use mobile apps for exchanging medical information with a health professional than the general public who were married or living as married.
In models 3 and 4 of the likelihood of Internet use with and without interactions, unlike models 1 and 2, race was not significantly predictive for the use of the Internet to seek cancer information (OR 0.99, [95% CI 0.73–1.33]; OR 1.26, [95% CI 0.86–1.82]). Individuals who were married or living as married and family caregivers were more likely to use the Internet to seek cancer information than unmarried or the general public (OR 1.26, [95% CI 1.01–1.57]; OR 1.67, [95% CI 1.29–2.16]), which was different from models 1 and 2. However, no significant results were found for sex, age, education, and income level. Similar to models 1 and 2, as compared to individuals who were ‘very’ interested in exchanging information about diagnostic information, those who were interested ‘somewhat/a little’ (OR 0.54, [95% CI 0.30–0.93]) were less likely to use the Internet to seek cancer information. Different from models 1 and 2, general health status was predictive in models 3 and 4. That is, individuals whose general health status was ‘good/fair’ or ‘poor’ (OR 1.30, [95% CI 1.05–1.60]; OR 1.83, [95% CI 0.97–3.27]) were more likely to use the Internet to seek cancer information than those whose general health status was ‘excellent/very good’. Unlike models 1 and 2, self-efficacy variables were significantly predictive. That is, individuals who were not confident in taking care of their own health were more likely to use the Internet to seek cancer information themselves than those where were completely or very confident (OR 2.34, [95% CI 0.85–5.97], p < .05). In addition, individuals who were not confident in getting cancer information were less likely to use the Internet to seek cancer information than those who were completely or very confident (OR 0.42, [95% CI 0.14–0.98], p < .05). Moreover, individuals who would not or would ‘a little’ trust cancer information from the Internet were less likely to use the Internet to seek cancer information than those who trusted it ‘a lot’ (OR 0.72, [95% CI 0.51–1.00], p < .05). In model 4, a significant interaction result between being a family caregiver and trusting cancer information (some) was found (OR 1.83, [95% CI 0.99–3.36], p < .05), implying that family caregivers who would trust cancer information were more likely to use the Internet for seeking cancer information than the general public who would trust cancer information.
Discussion
This study was originally motivated to fill the gap in the literature concerning online medical information seeking among family caregivers and the general public by types of health information technology and the difference between them. Our hypothesis was that family caregivers are more likely to use mobile apps and the Internet to seek medical information than the general public. However, our finding revealed that fewer family caregivers than members of the general public used mobile apps for seeking medical information, while more family caregivers than the general public used the Internet for seeking cancer information. Our results also showed that family caregivers who were married or living as married were less likely to use mobile apps; however, family caregivers who would trust cancer information in some degree were more likely to use the Internet for medical information seeking than the general public. Family caregivers may be unwilling to use mobile apps for a medical purpose due to security concerns. That is, most mobile health apps are unregulated [12, 13] and do not protect individuals’ privacy rights [12]. Or, possibly family caregivers may not have enough time to utilize mobile apps and seek medical information. Additionally, family caregivers may possibly have barriers to using mobile apps for caregiving such as not understanding how to use mobile apps, privacy regulations in a health system [27], perceived costs, and refusal by patients to allow caregivers to search for information [28].
Our findings also showed that individuals whose health status was worse were more likely to use the Internet to seek cancer information than those whose health status was excellent or very good. For the use of mobile apps, however, no association with general health status was found. However, the relationship between general health status and online medical information seeking may vary depending on individuals’ needs. For instance, previous research has found that healthy individuals are more likely to seek health information online in general [8, 29], while other research has posited that unhealthy individuals may also want to look for health information because of their specific health needs. Oh and Cho (2015) also mentioned that the relationship between online health information seeking and self-rated health relies on the likelihood of having both the resources and need to seek information [30]. Interestingly, our results revealed that Whites were less likely than Blacks to use mobile apps for exchanging medical information with a health professional. Compared with Whites, Blacks are less likely to rely on the medical system [31] so they may possibly look for other sources to confirm information they received from health professionals [9].
Not surprisingly, our results revealed that being interested in online information exchange with a healthcare provider strongly, positively predicted individuals using both mobile apps and the Internet for medical information seeking. Moreover, individuals who were concerned about the quality of cancer information from other sources were more likely to use mobile apps in exchanging medical information with a health professional than those who were not concerned, suggesting that they trust the cancer information source more than being concerned about the mechanism by which they receive the information. Additionally, individuals who would trust ‘a lot’ about cancer information from the Internet were more likely to use the Internet for cancer information seeking than those who would trust the Internet for cancer information ‘a little’ or ‘not at all’. As a matter of fact, the Internet is not the main source that people use to seek cancer information [9]; people look for cancer information from various sources such as mass media, health magazines, and health professionals [9, 32]. However, people are less likely to give validity to the information from media sources than from information from a computer [2]. Dutta-Bergman (2004) investigated how consumers seek health information using various communication channels and mentioned that mass media such as TV or radio function as a main source among individuals who are not health-oriented, whereas the Internet better supports health-active individuals [33].
Our measures of self-efficacy showed mixed results. Confidence in getting cancer information was positively associated with the likelihood of using the Internet for cancer information seeking, whereas confidence in taking care of one’s own health was not associated with Internet information seeking. Lim et al. (2011) examined predictors associated with Singaporean women using mobile phones for health information seeking and found that self-efficacy was significantly, positively predictive [11]. Similarly, Pálsdóttir (2008) tested how self-efficacy influenced information seeking behaviors among four groups with different levels of self-efficacy and found that the higher level self-efficacy group looked for information more often as compared to lower level self-efficacy groups [34]. However, Oh (2015) did not find any association between self-efficacy and online health information seeking [10]. This gap may be explained by previous research. Rimal (2001) found that individuals with higher self-efficacy and perception of risk were more likely to be involved in information seeking than those with lower self-efficacy and perception of risk. In other words, individuals seeking information behavior may vary depending on the level of risk perception along with self-efficacy [35].
We believe our study has several implications for policy. Health policymakers and insurance providers may consider policies that promote use of effective mobile healthcare applications that have been shown to contribute to improving health outcomes via subsidies or other incentives. Nevertheless, mobile health applications should be developed based on standard guidelines and confirm more authentication procedures to protect individuals’ health information [36]. Moreover, the Internet has various kinds of unregulated and unassessed sources of information [37] and in particular, there is common criticism about incorrect and misleading information in the Internet [38]. Thus, there should be better assessment of the quality of online information using peer reviews and rating systems [2].
Our study has several limitations. First, this study used cross-sectional data; although we found relationships between the predictors and outcome variables, we may not infer causation between them. Second, although the Comprehensive Model of Information Seeking (CMIS) captured various predictors for online information seeking, our results were bounded by the limitations of the CMIS. That is, the contribution of health-related factors like demographics (i.e., age, race, income, and education) was fundamentally small to this framework [17]. Nevertheless, a number of studies used CMIS and confirmed that it explained online information seeking well. Third, there could be moderating factors associated with the use of mobile apps and the Internet for medical information seeking. One example of moderating factors would be the extent of health risk perception among individuals. Thus, future research needs to examine how individuals seek medical information differently depending on the level of risk perception.
Conclusion
To our best knowledge, this study using a nationally representative sample is the first to examine the difference in medical information seeking behavior between family caregivers and the general public by types of health information technology. We found that online medical information seeking is different between family caregivers and the general public. Overall, the use of the Internet is more common, while the use of mobile apps is less common for medical information seeking among family caregivers as compared to the general public. Particularly, married family caregivers were less likely to use mobile apps than the general public. Since benefits from using mobile apps in healthcare have already been documented in terms of effectiveness and better supporting or assisting services for patients with serious conditions or illness [12, 13], there may be more potentiality to enhance healthcare delivery and improve health outcomes among patients and caregivers as well as the general public. In this sense, healthcare professionals may provide patients, their caregivers, and those with specific health needs educational materials or sessions to teach how to utilize mobile apps. Family caregivers play an important role in caring for cancer patients and may seek the information that cancer patients need. In this regard, medical information seeking behavior among family caregivers can be an important predictor of both their health and the health of their cancer patients. Future research should explore the low usage of mobile health applications among family caregiver population.
References
Kim, H., and Xie, B., Health literacy and internet-and mobile app-based health services: a systematic review of the literature. Proceedings of the Association for Information Science and Technology. 52(1):1–4, 2015.
Cline, R.J., and Haynes, K.M., Consumer health information seeking on the internet: the state of the art. Health Education Research. 16(6):671–692, 2001.
Hawkes, C.P., Walsh, B.H., Ryan, C.A., and Dempsey, E.M., Smartphone technology enhances newborn intubation knowledge and performance amongst pediatric trainees. Resuscitation. 84(2):223–226, 2012.
Fox, S., and Duggan, M., Mobile health 2012. Pew Internet & American Life Project, Washington, DC, 2012.
Wallace, S., Clark, M., and White, J., ‘It’s on my iPhone’: attitudes to the use of mobile computing devices in medical education, a mixed-methods study. BMJ Open. 2(4):e001099, 2012.
Boulos, M.N., Wheeler, S., Tavares, C., and Jones, R., How smartphones are changing the face of mobile and participatory healthcare: an overview, with example from eCAALYX. Biomedical Engineering Online. 10(24), 2011. doi:10.1186/1475-925X-10-24.
Pandey, A., Hasan, S., Dubey, D., and Sarangi, S., Smartphone apps as a source of cancer information: changing trends in health information-seeking behavior. Journal of Cancer Education. 28(1):138–142, 2013.
Cotton, S.R., and Gupta, S.S., Characteristics of online and offline health information seekers and factors that discriminate between them. Social Science & Medicine. 59(9):1795–1806, 2004.
Kelly, B., Hornik, R., Romantan, A., Schwartz, J.S., et al., Cancer information scanning and seeking in the general population. Journal of Health Communication. 15(7):734–753, 2010.
Oh, Y.S., Predictors of self and surrogate online health information seeking in family caregivers to cancer survivors. Social Work in Health Care. 54(10):939–953, 2015.
Lim, S., Xue, L., Yen, C.C., Chang, L., et al., A study on Singaporean women’s acceptance of using mobile phones to seek health information. International Journal of Medical Informatics. 80(12):e189–e202, 2011. doi:10.1016/j.ijmedinf.2011.08.007.
Knorr, K., Aspinall, D., and Wolters, M. (2015). On the privacy, security and safety of blood pressure and diabetes apps. In: ICT Systems Security and Privacy Protection (pp. 571–584). Springer International Publishing.
Ranchordas, S., and Kaplan, B. (2016). MHealth for Alzheimer’s disease: Regulation, Consent, and Privacy Concerns. In: Beyond IP: The Future of Privacy (Fordham University Press, 2017), Forthcoming.
Arrington, M.I., “She’s right behind me all the way”: an analysis of prostate cancer narratives and changes in family relationships. Journal of Family Communication. 5(2):141–162, 2005. doi:10.1207/s15327698jfc0502_5.
Bevan, J.L., and Pecchioni, L.L., Understanding the impact of family caregiver cancer literacy on patient health outcomes. Patient Education and Counseling. 71(3):356–364, 2008.
Matthews, A.K., Sellergren, S.A., Manfredi, C., and Williams, M., Factors influencing medical information seeking among African American cancer patients. Journal of Health Communication. 7(3):205–219, 2002.
Johnson, J.D., and Meischke, H., A comprehensive model of cancer-related information seeking applied to magazines. Human Communication Research. 19(3):343–367, 1993.
Pennbridge, J., Moya, R., and Rodrigues, L., Questionnaire survey of California consumers’ use and rating of sources of health care information including the internet. Western Journal of Medicine. 171(5–6):302, 1999.
Hesse, B.W., Nelson, D.E., Kreps, G.L., Croyle, R.T., et al., Trust and sources of health information: the impact of the internet and its implications for health care providers: findings from the first health information National Trends Survey. Archives of Internal Medicine. 165(22):2618–2624, 2005.
Johnson, J. D., Cancer-related information seeking: Hampton Press, 1997.
Holden, R.J., and Karsh, B.T., The technology acceptance model: its past and its future in health care. Journal of Biomedical Informatics. 43(1):159–172, 2010.
Zhao, X., and Cai, X., The role of risk, efficacy, and anxiety in smokers’ cancer information seeking. Health Communication. 24(3):259–269, 2009.
National Cancer Institute (2016). What is HINTS. Retrieved May 17, 2016 from http://url.hints.cancer.gov/
Nguyen, G.T., and Bellamy, S.L., Cancer information seeking preferences and experiences: disparities between Asian Americans and whites in the health information National Trends Survey (HINTS). Journal of Health Communication. 11(S1):173–180, 2006.
Bhuyan, S.S., Lu, N., Chandak, A., Kim, H., Wyant, D., Bhatt, J., Kedia, S., and Chang, C.F., Use of mobile health applications for health-seeking behavior among US adults. Journal of Medical Systems. 40(6):1–8, 2016.
National Cancer Institute (2016). Frequently asked questions about HINTS. Retrieved May 17, 2016 from http://url.hints.cancer.gov/faq.aspx.
Zulman, D.M., Piette, J.D., Jenchura, E.C., Asch, S.M., et al., Facilitating out-of-home caregiving through health information technology: survey of informal caregivers’ current practices, interests, and perceived barriers. Journal of Medical Internet Research. 15(7):e123, 2013.
National Alliance for Caregiving and United Healthcare. (2011). e-Connected family caregiver: Bringing caregiving into the twenty-first century. Retrieved June 25, 2016 from http://url.caregiving.org/data/FINAL_eConnected_Family_Caregiver_Study_Jan%202011.pdf
Chou, W.Y.S., Liu, B., Post, S., and Hesse, B., Health-related internet use among cancer survivors: data from the health information National Trends Survey, 2003–2008. Journal of Cancer Survivorship. 5(3):263–270, 2011.
Oh, Y.S., and Cho, Y., Examining the relationships between resources and online health information seeking among patients with chronic diseases and healthy people. Social Work in Health Care. 54(2):83–100, 2015.
Armstrong, K., Ravenell, K.L., McMurphy, S., and Putt, M., Racial/ethnic differences in physician distrust in the United States. American Journal of Public Health. 97(7):1283–1289, 2007.
Basch, E.M., Thaler, H.T., Shi, W., Yakren, S., and Schrag, D., Use of information resources by patients with cancer and their companions. Cancer. 100(11):2476–2483, 2004.
Dutta-Bergman, M.J., Primary sources of health information: comparisons in the domain of health attitudes, health cognitions, and health behaviors. Health Communication. 16(3):273–288, 2004.
Pálsdóttir, Á., Information behavior, health self-efficacy beliefs and health behavior in Icelanders’ everyday life. Information Research. 13(1):4, 2008.
Rimal, R.N., Perceived risk and self-efficacy as motivators: understanding individuals’ long-term use of health information. Journal of Communication. 51(4):633–654, 2001.
Adhikari, R., Richards, D., and Scott, K., Security and privacy issues related to the use of mobile health apps. In: Australasian Conference on Information Systems (ACIS), 2014.
Gregory-Head, B., Patients and the internet: guidance for evidence-based choices. The Journal of the American College of Dentists. 66(2):46–50, 1998.
Silberg, W.M., Lundberg, G.D., and Musacchio, R.A., Assessing, controlling, and assuring the quality of medical information on the internet: Caveant lector et viewor—let the reader and viewer beware. JAMA. 277(15):1244–1245, 1997.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Mobile & Wireless Health
The original version of this article was revised: Soumitra Sudip Bhuyan should be removed since the name of the author was listed twice as Soumitra S. Bhuyan. Additionally, the word “Management” in the author's affiliation was misspelled.
An erratum to this article is available at http://dx.doi.org/10.1007/s10916-017-0707-6.
Rights and permissions
About this article

Cite this article
Kim, H., Paige Powell, M. & Bhuyan, S.S. Seeking Medical Information Using Mobile Apps and the Internet: Are Family Caregivers Different from the General Public?. J Med Syst 41, 38 (2017). https://doi.org/10.1007/s10916-017-0684-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10916-017-0684-9