
Abstract
This study analyzes associated factors to self-perceived oral health and use of oral health services in native and immigrant adults from the PELFI cohort in Spain. A cross-sectional analysis was conducted (401 adults ≥ 18 years, from Spain, Ecuador, Colombia and Morocco). Frequencies for sociodemographic, self-perceived general and oral health variables were calculated. The association between oral health/oral health services use and origin country was estimated by logistic regression (adjusted odds ratio-aOR-; 95% confidence intervals -95%CI-). Ecuadorian men were more likely to report dental caries (aPR 2.75; 95%CI 1.30–5.80) and Moroccan women were more likely to report gingival bleeding (aPR 3.61; 95%CI 1.83–7.15) and the use of oral health services ≥ 1 year/never (aPR 1.69; 95%CI 1.06–2.69). Colombian women were less likely to report missing teeth (aPR 0.73; 95%CI 0.56–0.95). Poor self-perceived oral health indicators were observed in immigrants and were modified for sociodemographic and general health variables.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
According to the proposed definition of World Dental Federation (FDI), oral health is multi-faceted and includes the ability to speak, smile, smell, taste, touch, chew, swallow and convey a range of emotions through facial expressions with confidence and without pain, discomfort and disease of the craniofacial complex [1]. Therefore, it is considered an important element in public health due to its relationship with general health and quality of life of people [2], and not only depends on individual and biological factors, but also has been related to social, political aspects and the economic context of the countries [3]. In addition, oral health impacts in social groups considering the burden of oral treatments [4].
The oral health perception for each person that belongs to a social group is determined by the parameters that the group accepts and establishes. Additionally, it is influenced by the social and cultural context of individuals [5, 6]. The use of subjective measures to assess health variables allow to recognize the oral health status of individuals and its relation to the general health status and the functional capacity that indicates the personal well-being and satisfaction [7].
In a society characterized by multiple social, economic, political, geographic, demographic and environmental inequalities, the migratory processes are evident and dynamic. These processes have an impact on both the sending and hosting migrants’ countries. Nowadays, it is estimated that there are 258 million international migrants and a lot of them in irregular situation [8]. According to research, migrants are exposed to high levels of social vulnerability, which determines a considerable number of health needs [9].
For several decades, the Spanish territory has been an attractive destination for migrant people that proceed form different countries and cultures. Most immigrants are in economically productive age, and are looking for job opportunities in order to improve the economic situation of themselves and their families [10, 11]. However, the economic crisis had an important impact because many of these immigrants had to return to their countries of origin. Nowadays, the demographic profile of immigrants has changed because people with a better economic situation, with nationality or other working permissions, have remained in Spain [12].
New Contribution of the Literature
Although research using oral health indicators have drawn attention about the healthy migrant effect, especially in some groups of immigrants [13], it is well recognized that the loss of this effect increases over time [14]. Studies have reported a positive association between the fact of being an immigrant and to find low oral health conditions [15, 16] and poor access to oral health services [17,18,19]. For that means, it is important to explore the role of the social determinants that regulate the oral health situation in different social groups. This exploration is necessary because studies focused on the working immigrant population are scarce [20, 21].
Specifically, in Spain, several studies have been carried out in immigrant groups with the objective of identifying oral health conditions in comparison with the native population; many of them conducted on children samples [22,23,24]. General findings showed lower oral health levels in immigrant children or with immigration background in comparison with their counterparts. One of the most recent oral health studies in Spain aimed to analyze oral health services use and related factors in the immigrant working population compared to Spanish counterparts. This research used a cross-sectional approach of working population (n = 8591), that responded Spanish National Health Survey (SNHS) [25]. In this study, inequalities in oral health services use were found in immigrant workers according to sociodemographic explanatory variables.
The oral health of immigrants and issues related are priorities in public health. Accordingly, this study aims to analyze associated factors to self-perceived oral health and use of oral health services in native and immigrant adults from the PELFI cohort in Spain.
Methods
Participants and Data Collection
This is a cross-sectional analysis from a prospective cohort study. Data were drawn from the Platform of Longitudinal Studies on Immigrant Families (Acronym in Spanish for Proyecto de Estudios Longitudinales en Familias Immigrantes). PELFI project comprises a prospective multi-site cohort study drawn from a convenience sample in order to access the hard-to-reach population of immigrant families. The recruitment began in 2015, and additional details of the methodology are described elsewhere [26]. Briefly, 250 families were recruited through the use of key informants, with an enrollment rate of 82%; within each family, every adult (i.e. ≥ 18 years) and adolescent (i.e. 12–17 years) was interviewed. Specifically, for this analysis we used data from the first and second wave and we selected 401 adults (females: n = 146; 61.3%), from the sub-cohorts of Alicante (n = 192) and Barcelona (n = 209). Data were collected through a structured questionnaire which can be consulted at the following webpage: https://web.ua.es/es/gi-saludpublica/trabajo-inmigracion-y-salud-en-una-cohorte-de-poblacion-inmigrante-en-espana.html
Measures
The exposure variable was country of origin. Surveyed people were born in Spain (n = 101), Ecuador (n = 126), Colombia (n = 122) and Morocco (n = 52). According to national reports, the last three groups have the most important statistically representation in the Spanish territory [26]. As sociodemographic variables were considered the following: sex, age, educative level (≤ primary, secondary, ≥ university), marital status (single, married/cohabited, other), type of family (single-parent, two-parent), social class; it was coded considering the Spanish National Classification of Occupations-2011 with the following categories: non manual; management workers, technicians and professionals, support technicians and professionals, office workers, services and sales workers, qualified agriculture and fishing workers, industrial qualified workers; manual: operators and assemblers and unqualified workers), employment situation (yes, no).
To evaluate health status, certain general and oral health indicators were used separately: (1) Self-rated general health: categorized as good (good/very good) or poor (fair/poor/very poor). (2) Body Mass Index (BMI): defined as a person's weight in kilograms divided by the square of his/her height in meters (kg/m2), and with this information and according to the parameters of the WHO [27], the following characteristics were determined: (a) underweight: BMI ≤ 18.50; (b) normal weight: BMI between 18.50 and 24.99; (c) overweight-obesity: BMI ≥ 25.00. It is important to highlight that this measure was based on the self-perception of individuals when reporting their weight and height; (3) Mental Health (as assessed by the 12-item General Health Questionnaire; responses scoring ≥ 3 were classified as poor mental health [28]. With respect to state of oral health, variables used were: self-perceived dental caries, self-perceived gingival bleeding, missing teeth, presence of dental prosthesis (yes/no). The variables were re-categorized into “yes” (presence of the problem) and “no” (absence of the problem), considering the knowledge and the perception of the individual about this own health/disease process. The use of oral health services was obtained from responses to the question regarding one’s last visit to a dentist, stomatologist or dental hygienist for an exam, consultation or treatment for dental problems. The response options were re-categorized to construct a dichotomous variable (< 1 year/ ≥ 1 year-never).
Statistical Analysis
SPSS software version 22.0-IBM® was used to carry out all of the analyses. Analyses were conducted separately for men and women. First, absolute and relative frequencies were calculated for each of the sociodemographic and health variables according to the country of origin. Tests of statistical significance were carried out to observe differences among variables (Kruskal–Wallis test for polychotomous variables -age- and the Chi-square test for the distribution of frequencies for categorical variables). Three logistical regression models were developed to estimate the association between country of origin (exposure variable) and the oral health variables. (95%CI): Model 1 used only the variable country of origin (Spain used as reference category), Model 2 were built upon Model 1 and adjusted for all sociodemographic variables and finally Model 3 used health variables. We estimated Odds Ratios (OR) with confidence intervals of 95% and later they were converted in prevalence ratios (PR) by using the mathematical formula proposed by Miettinen [29].
This conversion was carried out on the basis that OR tend to overestimate the strength of association with prevalences higher than 10%. In both cases (OR-PR), the statistical significance and the magnitude of the associations was checked.
Ethics Approval and Consent to Participate
Ethical approval of the PELFI project was obtained from the ethical committees of the University of Alicante (Act UA- 2014-06-26) and the Vall d’Hebron Research Institute. Confidentiality was guaranteed throughout the research process, and all respondents gave informed consent to participate in accordance with Spanish regulations.
Results
Table 1 presents the sociodemographic characteristics of the sample according to sex and country of origin. The median of age ranged from 41.0 years in case of Ecuadorian females to 48.0 years for Moroccan males. People from Spain in both sexes had the highest proportion of people with university studies and those from Morocco have the highest frequency of people with primary studies (both sexes). The Moroccan groups had the highest percentage of married people. Ecuadorian and Colombian women had more frequently single-parent families. Manual social class were observed more frequently in Colombian an Ecuadorian for both sexes. Finally, Colombian and Moroccan men and Moroccan women had the highest frequency of unemployed people.
Table 2 shows the frequency of selected health and oral health indicators for the sample. Moroccan men and Spanish women reported the highest frequency of poor self-rated general health (57.1% and 60.7% respectively). The highest prevalence of overweight/obesity was found in Moroccan women (71.0%). Spanish men and Moroccan women had the highest frequency of poor mental health (65.9% and 67.7% respectively). In comparison with their counterparts, Moroccan women reported highest frequencies of self-perceived dental caries (48.4%) and Moroccan men reported highest frequencies of self-perceived gingival bleeding (61.9%) and missing teeth (76.2%). Colombian men and Ecuadorian women reported more presence of dental prosthesis (43.5% and 39.0% respectively). Moroccan men and women referred the use of oral health services ≥ 1 year/never (71.4% and 61.3 respectively). We found statistically differences in the distribution of the frequencies in case of self-rated health and mental health for males (p < 0.05), self-perceived dental caries for women (p < 0.01), and self-perceived gingival bleeding for both sexes (p < 0.01).
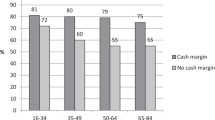
Considering the logistic multivariate analysis for the probability of the selected oral health indicators (Tables 3 and 4), men from Ecuador were more likely to report self-perceived dental caries (PR 2.75; 95%CI 1.30–5.80), women from Morocco were more likely to report self-perceived gingival bleeding (PR 3.61; 95%CI 1.83–7.15). Women from Colombia were less likely to report missing teeth (PR 0.73; 95%CI 0.56–0.95). Men and Women from Morocco had a tendency to report no presence of dental prosthesis (p < 0.10). Lastly, Fig. 1 shows the logistic analysis for the probability of use of oral health services (1 year or more prior), Moroccan women were more likely to report the use of oral health services ≥ 1 year/never (PR 1.69; 95%CI 1.06–2.69).

Multivariate logistic analysis for the probability of use of oral health services / ≥ 1 year-never according to the country of origin. PELFI Cohort. Spain (n = 401)
Discussion
Main findings of this study show that there exist differences in self-perceived oral health indicators according to the country of origin and sex. In general terms, people from Morocco reported the greater prevalence of oral health variables in the sample (dental caries, gingival bleeding and a low use of oral health services). However, after adjusting for sociodemographic and health variables by means of logistic regression models, men from Ecuador were more likely to report self-perceived dental caries, women from Morocco were more likely to self-perceived gingival bleeding and Moroccan women were more likely to report the use of oral health services ≥ 1 year/never.
The differences observed according to health and oral health variables considering the migration status in the sample show several situations that deserve to be commented. First, as discussed in the scientific literature, there exists a correspondence between general and oral health and disparities in oral epidemiologic profiles may be increased in populations considered potentially vulnerable [5]. Secondly, migration constitutes a social determinant of health since most immigrants experience a disadvantaged socio-economic and cultural position in host societies and they are, therefore, converted into groups which are especially vulnerable to health risk factors [30].
Findings of studies conducted in different geographical contexts show that the immigrant population reports poor oral health indicators when is compared with the native population. Nevertheless, factors related to the host country and specific characteristics of the immigrants’ social and demographic profile should be considered. For example, a study conducted with a small sample size of immigrant and refugees from 15 different countries, found that of all the participants, 63% reported having caries, 13% need for tooth extraction and 68% bleeding on brushing [31]. Other study carried out in USA reported that noncitizen immigrants reported having substantially poorer oral health than natives, although significant statistically differences did not remain in the adjusted models [15]. A similar study with data provided by The National Health and Nutrition Examination Survey conducted in 2011–2012 (USA), reported disparities according to migration status, incorporating predictor variables such as ethnicity background, citizenship, demographics and socioeconomic status (60% of American immigrants reported their oral health as fair/bad) [16]. Other studies carried out in European countries using clinical [18] and self-reported oral health outcomes [25] observed worse oral health and higher treatment needs in immigrants when compared with age-matched native people. The Oral Health Spanish Survey 2015, a clinical and representative clinical study, found a prevalence of dental caries of 56.7% in foreign-born adults of 35–44 years in comparison to 36.7% found in Spanish-born counterparts (statistically significant differences p < 0.05) [32]. This situation is similar when comparing periodontal indexes.
Research has emphasized the relatively good state of health in recent immigrants, -that means the healthy migrant effect-, but results in PELFI sample evidenced how this situation is often eroded by the migratory process itself and by the living conditions experienced by immigrant populations in the Spanish territory. One study carried out in Canada, showed an increase in the proportion of self-reported oral health problems over time [14]. Possible explanations lie in the psychological stress associated with the process of resettlement and experiences of discrimination in the host countries. In addition, a systematic review explored the impact of the acculturation phenomenon in oral health outcomes [33]. Another aspect that must be taken into account is the fact that the demographic profile of immigrants has suffered several changes in the Spanish territory and especially during economic crisis after 2009 [12]. Further research should consider longitudinal approaches in order to observe changes in oral health indicators in different foreign-born groups over time in several age groups and introducing other variables such as nationality/citizenship, country of origin, time of migration, specific sociodemographic characteristics and clinical/self-reported outcomes.
Health services are an important social determinant of health and inequalities in health. Findings showed a trend of low use or oral health services for immigrants in comparison with their Spanish counterparts in the sample (although significant statistically differences were found for Moroccan women in case of multivariate logistic models). This situation is comparable to other studies conducted in similar populations [17, 18, 34]. Previous research conducted in Spanish working population by means of representative data, found inequalities in immigrant women that can be explained by socioeconomic situation and education level [25]. Scientific literature generally suggests that immigrants (as other deprived and vulnerable groups) have higher and more complex oral health needs, but receive less health care provision or face barriers to health care [17,18,19, 34]. This situation is well-known as the inverse care law and has been applied to oral health care [35]. Possible explanatory structural factors involved in oral health accessibility include insurance, service costs and administrative difficulties inherent in the host country’s health care system [17,18,19, 34]. In addition, immigration background, cultural and sociodemographic characteristics, should be taking into account [19, 25].
Differences in health outcomes were found in the PELFI sample. Oral research discusses the sex/gender variations in the social impact of oral health outcomes [36]. Similarly, studies carried out in other populations found sex differences in dental visits, daily tooth brushing frequency, choice of toothbrush and toothpaste for oral self‐care [37]. Further studies should analyse the possible factors that explain the existing sex/gender differences in the use profile of the health services, in the self-care practices about oral hygiene and those related to the self-perception and self-recognition of their oral health condition in specific immigrant groups.
Whilst this analysis helps provide an in-depth understanding of the oral health conditions and the use of oral health services in a sample of immigrant and native working people, in interpreting the results, it is important to take the study’s limitations into account. The process of recruitment of families in the PELFI cohort was carried out using a convenience sample, which could result in selection bias, since many people were invited to participate through associations and through snowball sampling. An underestimation of the study results should not be discarded since people who had less social support or worse economic conditions did not participate. Difficulties for obtaining a probabilistic sample is considered a common problem in research focused on immigrant population [38].
All health indicators studied were based on the interviewees’ own perception, and this self-report is likely to vary depending on social and cultural factors. A complete estimation of oral and general health and nutritional status (BMI) should be confirmed by clinical examinations. However, self-perceived indicators constitute broad measures of health-related well-being transcending restrictive biomedical point of views of health and disease and permit its social construction. In addition, self-evaluation of oral health could be an advantageous approach for examining oral health status of communities [39, 40].
Despite the above-mentioned limitations, this study permitted an approach to the study of oral health situation and oral health service utilization in native and immigrant population through primary data proceeding of the PELFI cohort, the first longitudinal study focused in migrant families in Spain. Further research could be focused on understanding other social and contextual factors involved in accessibility to oral health services and oral health inequalities in immigrants through life course approaches and multilevel analysis strategies.
Conclusions
Oral health problems are public health concern due to this magnitude, severity and because they affect the quality of life of people. These problems are multi-factorial and depend on biological, social and contextual characteristics. In this context, findings of this study show how immigrants are in a disadvantaged position in society, which refers to the numerous risk factors that produces more frequently oral health outcomes in comparison to the native population. Similarly, the use of oral health services is lower, and this situation can be explained for individual and structural factors related to the health systems of the host countries. The identification of oral health needs of the immigrant population should be the basis for strategies based on social reality, focused on the social determinants. To assume the guarantee of the right to health as a fundamental issue should assure equity in access to oral health care for all citizens.
References
Glick M, Williams DM, Kleinman DV, Vujicic M, Watt RG, Weyant RJ. A new definition for oral health developed by the FDI World Dental Federation opens the door to a universal definition of oral health. Int Dent J. 2016;66(6):322–4.
Bagde R, Rao RD, Jain AK, Verma MR. Impact of oral health on quality of life. Int J Oral Care Res. 2017;5(4):342–4.
Costa SM, Martins CC, Pinto MQC, Vasconcelos M, Abreu M. Socioeconomic factors and caries in people between 19 and 60 years of age: an update of a systematic review and meta-analysis of observational studies. Int J Environ Res Public Health. 2018;15(8):1775.
Yee R, Sheiham A. The burden of restorative dental treatment for children in Third World countries. Int Dent J. 2002;52(1):1–9.
Hakeberg M, Wide BU. Self-reported oral and general health in relation to socioeconomic position. BMC Public Health. 2017;18(1):63.
de los Ángeles Ramírez M, Suárez Paniagua S, de la Fuente Hernández J, Shimada Beltrán H, Reyes Durán JF, Acosta-Torres LS. Componentes culturales que influyen en la salud bucal [cultural components that influence oral health]. Salud(i)Ciencia. 2015;21(3):294–300.
Luchi CA, Peres KG, Bastos JL, Peres MA. Inequalities in self-rated oral health in adults. Rev Saude Publica. 2013;47(4):740–51.
United Nations. Department of Economic and Social Affairs. Population Division. Trends in International Migrant Stock: The 2017 Revision. (United Nations database, POP/DB/MIG/Stock/Rev.2017). New York: United Nations; 2017.
Rechel B, Mladovsky P, Ingleby D, Mackenbach JP, McKee M. Migration and health in an increasingly diverse Europe. Lancet. 2013;381(9873):1235–45.
Ronda-Perez E, Agudelo-Suarez AA, Lopez-Jacob MJ, Garcia AM, Benavides FG. Scoping review about working conditions and health of immigrant workers in Spain. Rev Esp Salud Publica. 2014;88(6):703–14.
Gea-Sanchez M, Alconada-Romero A, Briones-Vozmediano E, Pastells R, Gastaldo D, Molina F. Undocumented immigrant women in Spain: a scoping review on access to and utilization of health and social services. J Immigr Minor Health. 2017;19(1):194–204.
Bastia T. Should I stay or should I go? Return migration in times of crises. J Int Dev. 2011;23(4):583–95.
Spolsky VW, Marcus M, Der-Martirosian C, Coulter ID, Maida CA. Oral health status and the epidemiologic paradox within Latino immigrant groups. BMC Oral Health. 2012;12:39.
Calvasina P, Muntaner C, Quinonez C. The deterioration of Canadian immigrants' oral health: analysis of the Longitudinal Survey of Immigrants to Canada. Community Dent Oral Epidemiol. 2015;43(5):424–32.
Wilson FA, Wang Y, Borrell LN, Bae S, Stimpson JP. Disparities in oral health by immigration status in the United States. J Am Dent Assoc. 2018;149(6):414–21e3.
Liu Y. Differentiation of self-rated oral health between American non-citizens and citizens. Int Dent J. 2016;66(6):350–5.
Wilson FA, Wang Y, Stimpson JP, McFarland KK, Singh KP. Use of dental services by immigration status in the United States. J Am Dent Assoc. 2016;147(3):162–9e4.
Aarabi G, Reissmann DR, Seedorf U, Becher H, Heydecke G, Kofahl C. Oral health and access to dental care—a comparison of elderly migrants and non-migrants in Germany. Ethn Health. 2018;23(7):703–17.
Calvasina P, Muntaner C, Quinonez C. Factors associated with unmet dental care needs in Canadian immigrants: an analysis of the longitudinal survey of immigrants to Canada. BMC Oral Health. 2014;14:145.
Gao X, Chan CW, Mak SL, Ng Z, Kwong WH, Kot CC. Oral health of foreign domestic workers: exploring the social determinants. J Immigr Minor Health. 2014;16(5):926–33.
Quandt SA, Hiott AE, Grzywacz JG, Davis SW, Arcury TA. Oral health and quality of life of migrant and seasonal farmworkers in North Carolina. J Agric Saf Health. 2007;13(1):45–55.
Paredes Gallardo V, Paredes Cencillo C, Mir PB. Prevalencia de la caries dental en el niño inmigrante: estudio comparativo con el niño autóctono [prevalence of dental caries: comparison between immigrant and autochthonous children]. An Pediatr (Barc). 2006;65(4):337–41.
Almerich Silla JM, Montiel Company JM. Oral health survey of the child population in the Valencia Region of Spain (2004). Med Oral Patol Oral Cir Bucal. 2006;11(4):E369–81.
Riatto SG, Montero J, Perez DR, Castano-Seiquer A, Dib A. Oral health status of Syrian children in the Refugee Center of Melilla, Spain. Int J Dent. 2018;2018:2637508.
Munoz-Pino N, Vives-Cases C, Agudelo-Suarez AA, Ronda-Perez E. Comparing oral health services use in the Spanish and immigrant working population. J Immigr Minor Health. 2018;20(4):809–15.
Cayuela-Mateo A, Martinez-Martinez JM, Ferrer Serret L, Felt E, Casabona IBJ, Collazos Sanchez F, et al. PELFI project: recruitment and sociodemographic characteristics of immigrant and autochthonous families from alicante and Barcelona City Subcohorts. Rev Esp Salud Publica. 2017;91:e1–e9.
World Health Organization. Obesity and overweight. Fact sheet. Updated June 2016. https://www.who.int/mediacentre/factsheets/fs311/en/. Accessed 3 Apr 2017.
Sanchez-Lopez Mdel P, Dresch V. The 12-Item General Health Questionnaire (GHQ-12): reliability, external validity and factor structure in the Spanish population. Psicothema. 2008;20(4):839–43.
Schiaffino A, Rodriguez M, Pasarin MI, Regidor E, Borrell C, Fernandez E. Odds ratio or prevalence ratio? Their use in cross-sectional studies. Gac Sanit. 2003;17(1):70–4.
Castañeda H, Holmes SM, Madrigal DS, Young M-ED, Beyeler N, Quesada J. Immigration as a social determinant of health. Annu Rev Public Health. 2015;36:375–92.
Mattila A, Ghaderi P, Tervonen L, Niskanen L, Pesonen P, Anttonen V, et al. Self-reported oral health and use of dental services among asylum seekers and immigrants in Finland—a pilot study. Eur J Public Health. 2016;26(6):1006–100.
Bravo Pérez M, Almerich Silla J, Ausina Márquez V, Avilés Gutiérrez P, Blanco González J, Canorea Díaz E, et al. Encuesta de salud oral en España 2015 [Oral Health Spanish Survey 2015]. RCOE. 2016;21(Supl1):8–48.
Gao XL, McGrath C. A review on the oral health impacts of acculturation. J Immigr Minor Health. 2011;13(2):202–13.
Cruz GD, Chen Y, Salazar CR, Karloopia R, LeGeros RZ. Determinants of oral health care utilization among diverse groups of immigrants in New York City. J Am Dent Assoc. 2010;141(7):871–8.
Dehmoobadsharifabadi A, Singhal S, Quinonez C. Investigating the "inverse care law" in dental care: a comparative analysis of Canadian jurisdictions. Can J Public Health. 2017;107(6):e538–e544544.
Mc Grath C, Bedi R. Gender variations in the social impact of oral health. J Ir Dent Assoc. 2000;46(3):87–91.
Azodo CC, Barnabas U. Gender difference in oral health perception and practices among Medical House Officers. Rus Open Med J. 2012;1(2):0208.
Monge S, Ronda E, Pons-Vigues M, Vives Cases C, Malmusi D, Gil-Gonzalez D. Methodological limitations and recommendations in publications on migrant population health in Spain. Gac Sanit. 2015;29(6):461–3.
Marino R, Schofield M, Wright C, Calache H, Minichiello V. Self-reported and clinically determined oral health status predictors for quality of life in dentate older migrant adults. Community Dent Oral Epidemiol. 2008;36(1):85–94.
Blizniuk A, Ueno M, Zaitsu T, Kawaguchi Y. Association between self-reported and clinical oral health status in Belarusian adults. J Investig Clin Dent. 2017;8(2):e12206.
Acknowledgements
The authors would like to thank all the individuals and families from the PELFI cohort of the cities of Barcelona and Alicante that agreed to take part in this study.
Funding
Healthcare Research Fund of the Spanish Ministry of Health (Ref. PI14/01146-PI14/02005), Institute for Health Carlos III-FEDER. Immigration and Health Subprogram in the Center for Biomedical Network Research on Epidemiology and Public Health (CIBERESP-SIS), Spain.
Author information
Authors and Affiliations
Contributions
AAAS coordinated the design of the manuscript confection and drafted the manuscript. The rest of the authors made substantial contributions to the interpretation of data. All the authors contributed to the revision of the different versions of the manuscript and the approval of the final version to be submitted to the journal.
Corresponding author
Ethics declarations
Conflict of interest
All the authors declare that they have no conflict of interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Agudelo-Suárez, A.A., Muñoz-Pino, N., Vivares-Builes, A.M. et al. Oral Health and Oral Health Service Utilization in Native and Immigrant Population: A Cross-Sectional Analysis from the PELFI Cohort in Spain. J Immigrant Minority Health 22, 484–493 (2020). https://doi.org/10.1007/s10903-020-00972-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10903-020-00972-0