
Abstract
Electronic nicotine delivery systems (ENDS) are relatively new and ENDS use data from community engagement programs may help us understand usage patterns and facilitate targeted longitudinal studies. Community members in Florida, USA, were asked about ENDS use, tobacco use, and health history/concerns by Community Health Workers. Among 7253 members recruited during 2014 to 2021 into our HealthStreet program, 1177 had ever used ENDS; the proportion increased from 12 to 27% from 2014 to 2021 (adjusted odds ratio (aOR) 2.5; 95% CI 1.7–3.5; Ever versus never used ENDS). Ever tobacco use was strongly associated with ENDS use; 69% of ever users were current tobacco users. Demographic determinants (sex, age, race) and food insecurity were strongest predictors of ENDS use. Most who had ever used ENDS were aged 18–25 (aOR 5.9; 95% CI 4.6–7.6; vs. aged 60 + years), White (aOR 3.7; 95% CI 3.2–4.3; vs. Black/African American), male (aOR 1.5; 95% CI 1.3–1.7; vs. female), and recently food insecure (aOR 1.8; 95% CI 1.5–2.0; vs. not recently food insecure). Those with respiratory issues were more likely to have used ENDS compared to those without (aOR 2.0; 95% CI 1.6–2.6; aOR 1.3; 95% CI 1.1–1.5). Members concerned about hypertension were less likely to have used ENDS (aOR 0.7; 95% CI 0.5–0.9). In this relatively rural, micropolitan sample, tobacco use, socio-economic determinants, and certain health history/concerns were strongly associated with ENDS use. Community outreach approaches are needed to further understand these factors and implement interventions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Electronic nicotine delivery systems (ENDS), also known as e-cigarettes, were first imported to the United States (US) commercially in 2006 [1]. In 2017, 4.4% of US adults were current ENDS users, with the highest prevalence among those aged 18–24 years (10.1%) [2]. Over 14% of high-school students currently use e-cigarettes [3].
ENDS are often promoted as a healthier alternative to traditional tobacco products due to using water vapor created by heating ‘e-liquids’ instead of combusting tobacco leaves; thus, ENDS users theoretically avoid inhaling thousands of chemicals known to be present in smoked tobacco [4,5,6]. People who are concerned about tobacco associated health conditions may turn to using ENDS, instead of smoking cigarettes. [4, 7]. Tobacco-associated health conditions include asthma, COPD/emphysema, other breathing/lung problems, cancer, and heart/circulation problems [8,9,10].
E-liquids used in ENDS usually contain nicotine, flavors, solvents, and sometimes THC (tetrahydrocannabinol) and CBD (cannabidiol) [11]. Although using ENDS is sometimes purported to be a ‘harm reduction’ strategy, users may be unwittingly increasing nicotine dose per unit smoked [12]. Tobacco cigarettes typically contain 7–15 mg nicotine/cigarette, but some “5% nicotine” e-liquid brands contain 59 mg/mL nicotine [13,14,15,16]. Rao et al. found ten puffs of one ENDS brand resulted in serum nicotine levels five times higher than serum nicotine levels after ten puffs of a tobacco cigarette [14]. Leavens et al. determined a convenience sample study of 101 persons who used ENDS daily, consumed 10.5 ENDS pods per month on average [17].
The US Food and Drug Administration (FDA) states “There are no safe tobacco products, including ENDS”, citing health risks to ENDS users from lung injuries, seizures, and fires/explosions [18]. In 2019 − 2020, there was a highly publicized outbreak of EVALI (e-cigarette, or vaping, product use-associated lung injury) cases. ENDS users experienced severe short-term issues – some fatal; physical modification of the ENDS device or customized e-liquids were responsible for most problems in the outbreak [19,20,21,22,23,24,25,26]. In June 2022 the FDA instructed an ENDS manufacturer to stop distribution and sale of all products stating, “insufficient evidence to assess … toxicological risks”, however this Marketing Denial Order was overturned in court [27].
ENDS-associated health issues are not fully understood. Recent meta-analyses showed strong evidence that ENDS-risks include toxic substance exposure, nicotine dependence, respiratory health problems, and initiation of smoking regular cigarettes [28]. Other risks may include cognition and brain development problems, particularly in youth, due to the nicotine content of ENDS [29]. Impaired endothelial function has been observed [14]. A positive association between the number of COVID-19 cases/deaths and proportion of ENDS users in US states has been noted [30]. Recently, a study found an association between ENDS use and fragility fractures, suggesting harm to bone health [31]. Given the gap in the literature about ENDS in the population, this analysis focused on ENDS use among a sample of HealthStreet members in Florida.
Methods and Data Analysis
University of Florida’s HealthStreet (HSt) is a Community Engagement program in Alachua County, Florida, directed and co-directed by two authors respectively (LBC and CWS), aiming to promote health equity. Since 2011, data have been collected from over 12,700 HSt members [32]. Based on Community Health Worker (CHW) outreach into the North Central Florida communities, people who are interested complete a written informed consent process, are interviewed face-to-face by a CHW with a 20 min Health Needs Assessment which includes social determinants of health (e.g., sex, age, race, ethnicity), socioeconomic status (e.g., food security status, education level), and health issues (e.g., medical history, and health concerns).
In 2014, HSt updated their survey to include questions on use of e-cigarettes and vaping ENDS devices, by asking “Have you ever used e-cigarettes or a vaping device?” Those who responded ‘yes’ were asked if they had used in the past 30 days; those who responded ‘no’ or ‘don’t know’ were coded Never Used ENDS. Similarly, participants were scored as Never Used, or Ever Used tobacco, by combining “yes” responses to questions asking about smoking cigarettes, cigars, cigarillos, hookah, bong, or water pipe (hereafter referred to as [tobacco]). Ever Used [tobacco] “yes” responses were then further divided into Current or Former tobacco use, depending on whether they answered “yes” or “no” to the follow-up question: “Have you used [tobacco] in the last 30 days?”
Our sample included 7253 HSt members ≥ 18 years old who joined HSt from 2014 to 2021. A secondary analysis was run on 5139 HSt members with 1 + tobacco associated health condition(s), as discussed in the introduction. In all analyses, members answering ‘don’t know’ to specific questions were classified as ‘no’. Similarly, members who answered, ‘don’t know’ when asked if they had heart/circulation or breathing/lung conditions, were classified as ‘no’.
Between-group differences for ENDS use groups were calculated for demographic variables, tobacco associated health conditions, and heath concerns (e.g., hypertension, heart problems, and/or cancer). Unadjusted and adjusted odds ratios for Ever Used versus Never Used ENDS in any variable group (compared to reference group) were determined using multinomial logistic regression models. The distribution by year of Ever versus Never ENDS use was analyzed. Unadjusted and adjusted odds ratios for Ever Used versus Never Used in individual years were calculated using 2014 as the baseline year. Models were adjusted for demographic variables, tobacco associated health conditions, and naming a tobacco associated health problem as one of their top-three health concerns. Statistical significance was accepted for p-values less than 0.05.
Data analyses were conducted using SAS® software version 9.4, using the functions PROC LOGISTIC, PROC FREQ, PROC GLM AND PROC TABULATE. The R programming language Version 4.0.3 [33] packages tidyverse [34], cowplot [35], RColorBrewer [36], and ggsci [37] were used to create figures.
Results
The data show an increasing overall trend in Ever Use of ENDS, from 12% and 13% in 2014 (main, and sub analyses respectively), to 27% in 2021 (Tables S1, S5, Figs. 1a, S7a). However, in 2020, the Ever-Used ENDS trend line dipped downward (to 18% and 16%, main, and sub-analyses). The unadjusted and adjusted odds ratios of Ever versus Never Used ENDS mirrored the proportion trend: increasing trend from 2014 to 2021, with a dip for 2020 (Figs. 1b and S7b). Adjusted odds ratios (aOR) comparing ENDS use in 2014 with 2019 and 2021 were statistically significant for the main analysis, but only for 2014 versus 2021 in the sub-analysis (Figs. 1b and S7b). By 2021 participants were more than twice as likely to have ever used ENDS compared to 2014 (main analysis: aOR 2.5, 95% CI 1.7–3.5; sub-analysis: aOR 2.2, 95% CI 1.5–3.4; Tables S1, S5, Figs. 1b, S7b). A total of 1,177 HSt members (16%) including 849 (17%) of the members with 1 + tobacco associated conditions had used ENDS (2014–2021), with significantly different distribution of Ever vs. Never ENDS use by year (p < 0.0001, Tables S1 and S5).

Distribution and odds ratios of Ever versus Never Used ENDS status for HealthStreet members by year (2014–2021). a Distribution of Ever versus Never Used ENDS by year; b Adjusted and unadjusted odds ratios for Ever versus Never Used ENDS by year, with 95% confidence intervals (CI). Odds ratios (OR) are adjusted for sex, age (categorical), race, ethnicity, ≥ 12 yrs. of education (yes/no), and food insecure (yes/no). Closed symbols indicate statistically significant OR where the 95% CI excludes 1. Wald Chi-square p-value symbols: *<0.05, and ***<0.0001.
Statistically significant differences were observed between Ever Used and Never Used populations (Tables 1, S3, Figs. S1, S2, S4, & S5). Males were 50% more likely to have ever used ENDS compared to females, with an adjusted odds ratio (aOR) of 1.5 (95% CI 1.3–1.7 main analysis; 95% CI 1.2–1.7 sub-analysis) after adjusting for race, ethnicity, age, education status, food insecurity status, tobacco associated health conditions and concerns (Table 2, S4, Fig. S3, S6).
Members in the 18–25 age group were 5.9 times (aOR 95% CI 4.6–7.6) more likely to have ever used ENDS compared to those in the 60 + age group for the main analysis (Table 2, Fig. S3). However, this likelihood increased to 6.2 times (aOR 95% CI 4.6–8.5) for members in the 18–25 age group who had tobacco-related conditions, compared to those in the 60 + age group (Table S4, Fig. S6). The average age for females and males who had ever used ENDS was similar in the main analysis (41.3 and 41.0 years respectively, Table 1, Fig. S1d), but on average, females who had tobacco-related conditions, who had ever used ENDS, were older than males (44.1 vs. 43.5 years, Table S3, Fig. S4d). Between-group differences for Ever versus Never Used ENDS were significant for 18–25, 26–40, 41–59, and 60 + age groups in both the main and the sub-analyses. Among those with tobacco associated health conditions, 27% of those aged 18–40 years had ever used ENDS (Table S3, Fig. S4b), slightly more compared to the general HSt population, where 24% and 23% of 18–25 and 26–40 years respectively had used ENDS (Table 1, Fig. S1b).
Compared to Black/African American (AA) HSt members, White HSt members were 3.7 times more likely (aOR 95% CI 3.2–4.3) overall to have Ever Used ENDS (Table 2, Fig. S3). Among those with tobacco-related health conditions, this likelihood decreased to 3.3 times more likely (aOR 95% CI 2.7–3.9, Table S4, Fig. S6). HSt members with Latino/Hispanic ethnicity were less likely to be Ever versus Never Used ENDS compared to those who did not identify as Latino/Hispanic (main analysis: aOR 0.7, 95% CI 0.6–0.9; sub-analysis: aOR 0.6, 95% CI 0.4–0.8, Tables 2, S4, Figs. S3, S6).
Almost half the HSt members had been food insecure in the past 12 months (i.e., did not have enough money to buy food, Tables 1, S3, Figs. S1e, S4e). Adjusted odds ratios show HSt members who had been food insecure in the past 12 months, were almost twice as likely to have used ENDS compared to those who were not food insecure (main analysis: aOR 1.8, 95% CI 1.5–2.0; sub-analysis: aOR 1.9, 95% CI 1.6–2.2; Tables 2, S4, Figs. S3, S6).
Only 1181 (16%) of HSt members overall—including 866 (17%) of members with tobacco-related conditions—had less than 12 years education; 223 (19%) and 169 (20%) of these groups had used ENDS (Tables 1, S3). The majority of HSt members (main analysis: 6072, 84%; sub-analysis: 4273, 83%) had 12 or more years of education; 16% of these members had used ENDS (main & sub-analysis: 954 & 680 members respectively). Adjusted odds of being an Ever/Never ENDS user as regards education level were not statistically significant (Tables 2, S4, Figs. S3, S6).
Of the 7253 HSt members, 5139 members (71%) had one or more tobacco associated health conditions: 1484 members (29%) had asthma, 562 (11%) had COPD/emphysema, 2206 (43%) had other breathing/lung problems, 815 (16%) had cancer, and 4130 (80%) had heart/circulation problems (Table S3, Fig. S5a). Significant Ever versus Never Used ENDS distributions were found for all health conditions except cancer (Table S3, Fig. S5a).
Compared to HSt members in general, those who had COPD/emphysema were significantly more likely to have Ever Used than Never Used ENDS (aOR 2.0, 95% CI 1.6–2.6); this was also the case for those reporting types of breathing conditions other than asthma (aOR 1.3, 95% CI 1.1–1.5), but none of the other adjusted odds for tobacco associated health histories were significant (Table 2, Fig. S3). Members who listed hypertension as one of their top three health concerns were significantly less likely have ever used ENDS (aOR 0.7; 95% CI 0.5–0.9, Table 2, Fig. S3). There were no significant ENDS use between-group differences, nor were there any significant adjusted odds ratios, among those who were concerned about heart problems or cancer (Tables 1, 2).
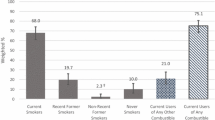
The majority of those who had ever used ENDS were current tobacco users: 809 (69%) of members in the main analysis, and 601 (71%) among members with tobacco associated health history (Tables S2, S6, Fig. 2). In contrast just 2% of those who had never used tobacco (65 and 40 members, main & sub-analyses) had ever used ENDS (Tables S2, S6, Fig. 2). Around 5% of ENDS users had never used tobacco (main analysis: 65, 6%; sub-analysis: 40, 5%; Tables S2, S6, Fig. 2).

Percentage of HealthStreet members by tobacco and ENDS use status, comparing main sample with subset of those with tobacco associated health conditionsa (2014–2021). aAsthma, COPD/emphysema, chronic bronchitis, chronic sinus infections, pneumonia, all cancers, arrhythmias, chest pain/angina, clots, coronary artery disease, heart attack, heart murmur, heart palpitations, high cholesterol, high blood pressure, mitral valve prolapse, deep vein thrombosis, other heart/circulation conditions.
Discussion
Demographic and socioeconomic trends we observed for ENDS use within the HealthStreet Community mirrored national findings. Ever-use use of ENDS was more frequent in members who were White, young, male, recently food-insecure, and/or had respiratory health issues compared to other groups [2, 38]. However, decreased ENDS use in HealthStreet data during 2020 (relative to 2019 and 2021, Fig. 1a, Table S1), contrasted with studies suggesting no change or increased use of ENDS during 2020 [39, 40]. We attributed this anomaly to the COVID-19 lockdown restrictions which limited how many HSt members CHW could survey in 2020.
When this analysis was conceptualized, we anticipated patterns of ENDS use would be different for HSt members who had a history of tobacco associated health conditions, compared to the overall sample. We expected that HSt members who had tobacco associated health history would be more likely to be former or current ENDS users (‘Ever Used ENDS’), and less likely to be classified as ‘Never Used ENDS’. As ENDS are frequently used as smoking cessation aids, it is likely that those who had tobacco associated health conditions would have been more likely to have tried ENDS as a lesser-harm alternative. This was based on the premise that after experiencing a health problem attributed to or made worse by tobacco, HSt members may have turned to using ENDS as smoking cessation devices [21]. Instead, the patterns of tobacco/ENDS usage from the HSt population overall and for those who had tobacco associated health conditions were almost identical (Fig. 2, Tables S2, S6). For example, about one third of HSt members (main analysis: 36%, sub-analysis: 37%) had never used tobacco or ENDS devices. Allowing for the fact that there is limited evidence on health issues attributable to ENDS, and looking at tobacco data alone, the percentage of those who currently use, formerly used, or have never used tobacco is virtually the same for those who did (38%, 29%, 33%) and did not (40%, 27%, 33%) report tobacco associated health conditions. Health messaging may encourage tobacco users to switch to ENDS to try to minimize risks. However, ENDS use patterns in HSt suggest perhaps tobacco users who turn to ENDS use for tobacco smoking cessation purposes may need additional support to successfully quit.
A limitation of our study is that ENDS are new, and most users are young, so exploring associations between ENDS use and older-age related health conditions may give rise to low estimates. Despite this limitation, HSt members reporting COPD/emphysema were twice as likely to be ever-users than never-users of ENDS (aOR 2.0, 95% CI 1.6–2.6, Table 2). We anticipate an even stronger association in the future. COPD is typically diagnosed over the age of 40, and more usually over age 65 [41], and of our 4,694 HSt members aged > 40 years, only 572 (12%) had used ENDS (Table 1). Another limitation is potential misclassification bias as regards ‘Ever Use’ because if a HSt member had used an ENDS device one time, they were categorized as ‘Ever Used ENDS’. Also, misclassification of tobacco associated heart condition status could have occurred, if a member had early coronary artery disease without symptoms [42].
An important strength of our study is the huge number of members in the HealthStreet community, and the consistency in ENDS-related data collection from 2014 to date. This ensures that we can compare data over the years to examine trends. CHW are actively recruiting new members, widening their scope of questions, and forming a Cancer Survivor Cohort which will link medical records with HSt data [43]. Thus, moving forward we will be able to see how ENDS use changes associations in future years, and link ENDS use with medical records on health conditions.
HealthStreet’s longitudinal data collection on ENDS use and a multitude of demographic, economic, and other health variables, will help us understand associations between ENDS use, and long-term health – including data from medical records will potentially enable identification of sub-populations to target public health and medical resources more effectively.
Data Availability
Participants of this study did not agree for their data to be shared publicly, so supporting data is not available.
Code Availability
R code is available on request.
References
U.S. Customs and Border Protection. (2006). NY m85579: The tariff classification of a nicotine inhaler and parts from China. U.S. Department of Homeland Security. Retrieved from https://rulings.cbp.gov/search?term=m85579&collection=ALL&sortBy=RELEVANCE&pageSize=30&page=1
State Health Access Data Assistance Center (SHADAC). (n.d.). SHADAC analysis of behavioral risk factor surveillance system (BRFSS) public use files, percent of adults who currently use e-cigarettes some days or every day. State Health Compare, University of Minnesota. Retrieved October 28, 2022, from http://statehealthcompare.shadac.org/table/218/percent-of-adults-who-currently-use-ecigarettes-some-days-or-every-day-by-race-ethnicity#1/39,40,41,43/24/250
Cooper, M., Park-Lee, E., Ren, C., Cornelius, M., Jamal, A., & Cullen, K. A. (2022). Notes from the field: E-cigarette use among middle and high school students — United States, 2022. Morbidity and Mortality Weekly Reports, 71, 1283–1285. https://doi.org/10.15585/mmwr.mm7140a3
Committee on Toxicity of Chemicals in Food, Consumer Products and the Environment. (2020). Statement on the potential toxicological risks from electronic nicotine (and non-nicotine) delivery systems (E(N)NDS – e-cigarettes). Statement Number 2020/04. Retrieved from https://cot.food.gov.uk/sites/default/files/2020-09/COT%20E%28N%29NDS%20statement%202020-04.pdf
American Cancer Society. (2022). American Cancer Society position statement on electronic cigarettes. Retrieved from https://www.cancer.org/healthy/stay-away-from-tobacco/e-cigarettes-vaping/e-cigarette-position-statement.html
Feeney, S., Rossetti, V., & Terrien, J. (2022). E-Cigarettes—a review of the evidence—harm versus harm reduction. Tobacco Use Insights, 15, 1–8. https://doi.org/10.1177/1179173X221087524
Robertson, L., Hoek, J., Blank, M. L., Richards, R., Ling, P., & Popova, L. (2019). Dual use of electronic nicotine delivery systems (ENDS) and smoked tobacco: a qualitative analysis. Tobacco Control, 28(1), 13–19. https://doi.org/10.1136/tobaccocontrol-2017-054070.
American Cancer Society. (2020). Health risks of smoking tobacco. Retrieved from https://www.cancer.org/healthy/stay-away-from-tobacco/health-risks-of-tobacco/healthrisks-of-smoking-tobacco.html
Centers for Disease Control and Prevention. (2020). Smoking and tobacco use: Health effects. CDC. Retrieved from https://www.cdc.gov/tobacco/basic_information/health_effects/index.htm
Centers for Disease Control and Prevention. (2021). Smoking and tobacco use: Health effects of cigarette smoking. CDC. Retrieved from https://www.cdc.gov/tobacco/data_statistics/fact_sheets/health_effects/effects_cig_smoking/index.htm
Centers for Disease Control and Prevention. (n.d.). E-cigarette, or vaping, products visual dictionary. Retrieved October 28, 2022, from https://www.cdc.gov/tobacco/basic_information/e-cigarettes/pdfs/ecigarette-or-vaping-products-visual-dictionary-508.pdf
Marynak, K. L., Gammon, D. G., Rogers, T., Coats, E. M., Singh, T., & King, B. A. (2015). Sales of nicotine-containing electronic cigarette products: United States. American Journal of Public Health, 107(5), 702–705. https://doi.org/10.2105/AJPH.2017.303660.
JUUL. (n.d.). What JUULpod flavors and nicotine strengths does JUUL offer? Retrieved October, 28, 2022, from https://support.juul.com/s/article/What-JUULpod-flavors-and-nicotine-strengths-does-JUUL-offer-UnitedStates
Rao, P., Liu, J., & Springer, M. L. (2020). JUUL and combusted cigarettes comparably impair endothelial function. Tobacco Regulatory Science, 6(1), 30–37. https://doi.org/10.18001/TRS.6.1.4.
Taghavi, S., Khashyarmanesh, Z., Moalemzadeh-Haghighi, H., et al. (2012). Nicotine content of domestic cigarettes, imported cigarettes and pipe tobacco in Iran. Addiction & Health, 4(1–2), 28–35. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3905555/.
Talih, S., Salman, R., El-Hage, R., et al. (2020). A comparison of the electrical characteristics, liquid composition, and toxicant emissions of JUUL USA and JUUL UK e-cigarettes. Scientific Reports, 10(1), 7322. https://doi.org/10.1038/s41598-020-64414-5.
Leavens, E., Stevens, E. M., Brett, E. I., et al. (2019). JUUL electronic cigarette use patterns, other tobacco product use, and reasons for use among ever users: Results from a convenience sample. Addictive Behaviors, 95, 178–183. https://doi.org/10.1016/j.addbeh.2019.02.011.
U.S. Food and Drug Administration. (2022). E-Cigarettes, vapes, and other electronic nicotine delivery systems (ENDS). Retrieved from https://www.fda.gov/tobacco-products/products-ingredients-components/e-cigarettes-vapes-and-other-electronic-nicotine-delivery-systems-ends
O’Callaghan, M., Boyle, N., Fabre, A., Keane, M. P., & McCarthy, C. (2022). Vaping-associated lung injury: A review. Medicina (Kaunas), 58(3), 412–430. https://doi.org/10.3390/medicina58030412.
Hart, J. L., Payne, T. J., Groom, A., et al. (2021). Association between electronic nicotine delivery systems (ENDS) device and E-liquid alterations and flavor use with clinical and EVALI-like symptoms. Preventative Medicine Reports, 24, 101619. https://doi.org/10.1016/j.pmedr.2021.101619.
Hartmann-Boyce, J., McRobbie, H., Butler, A. R., et al. (2021). Electronic cigarettes for smoking cessation. Cochrane Database of Systematic Reviews, 9(9), CD010216. https://doi.org/10.1002/14651858.CD010216.pub6
Centers for Disease Control and Prevention. (2021). Outbreak of lung injury associated with the use of e-cigarette, or vaping, products. CDC. Retrieved from https://www.cdc.gov/tobacco/basic_information/e-cigarettes/severe-lung-disease.html
Hajat, C., Stein, E., Shantikumar, S., Niaura, R., Ferrara, P., & Polosa, R. (2022). A scoping review of studies on the health impact of electronic nicotine delivery systems. Internal and Emergency Medicine, 17(1), 241–268. https://doi.org/10.1007/s11739-021-02835-4.
Deliwala, S., Sundus, S., Haykal, T., Theophilus, N., & Bachuwa, G. (2020). E-cigarette, or vaping, product use-associated lung injury (EVALI): Acute lung illness within hours of switching from traditional to e-cigarettes. Cureus, 12(4), e7513. https://doi.org/10.7759/cureus.7513.
Li, Y., Fairman, R. T., Churchill, V., Ashley, D. L., & Popova, L. (2020). Users’ modifications to electronic nicotine delivery systems (ENDS): Interviews with ENDS enthusiasts. International Journal of Environmental Research and Public Health, 17(3), 918–926. https://doi.org/10.3390/ijerph17030918.
Massey, Z. B., Li, Y., Holli, J., et al. (2020). Modifications to electronic nicotine delivery systems: Content analysis of YouTube videos. Journal of Medical Internet Research, 22(6), e17104. https://doi.org/10.2196/17104.
U.S. Food and Drug Administration. (2022). FDA denies authorization to market JUUL products: Currently marketed products must be removed from the US market. Retrieved from https://www.fda.gov/news-events/press-announcements/fda-denies-authorization-market-juul-products
Asfar, T., Jebai, R., Li, W., et al. (2022). Risk and safety profile of electronic nicotine delivery systems (ENDS): an umbrella review to inform ENDS health communication strategies. Tobacco Control. https://doi.org/10.1136/tc-2022-057495
Lyzwinski, L. N., Naslund, J. A., Miller, C. J., & Eisenberg, M. J. (2022). Global youth vaping and respiratory health: epidemiology, interventions, and policies. Nature Partner Journals Primary Care Respiratory Medicine, 32(1), 14. https://doi.org/10.1038/s41533-022-00277-9.
Li, D., Croft, D. P., Ossip, D. J., & Xie, Z. (2020). The association between statewide vaping prevalence and COVID-19. Preventive Medicine Reports, 20, 101254. https://doi.org/10.1016/j.pmedr.2020.101254.
Agoons, D. D., Agoons, B. B., Emmanuel, K. E., Matawalle, F. A., & Cunningham, J. M. (2021). Association between electronic cigarette use and fragility fractures among US adults. American Journal of Medicine Open, 1–6, 100002. https://doi.org/10.1016/j.ajmo.2021.100002.
Cottler, L. B. (2022). Community health needs assessment. University of Florida. Retrieved from https://healthstreet.program.ufl.edu/wordpress/files/2022/01/CHNA.pdf
R Core Team. (2020). R: A language for statistical computing. Vienna: R Foundation for Statistical Computing. Retrieved from https://www.r-project.org
Wickham, H., Averick, M., Bryan, J., et al. (2019). Welcome to the tidyverse. The Journal of Open Source Software, 4(43), 1686. https://doi.org/10.21105/joss.01686.
Wilke, C. O. (2020). Cowplot: Streamlined plot theme and plot annotations for ‘ggplot2’. R package version 1.1.1. Retrieved from https://CRAN.R-project.org/package=cowplot
Neuwirth, E. (2014). RColorBrewer: ColorBrewer palettes. R package version 1.1-2. Retrieved from https://CRAN.R-project.org/package=RColorBrewer
Xiao, N. (2018). Ggsci: Scientific journal and sci-fi themed color palettes for ‘ggplot2’. R package version 2.9. Retrieved from https://CRAN.R-project.org/package=ggsci
Assari, S., Mistry, R., & Bazargan, M. (2020). Race, educational attainment, and e-cigarette use. Journal of Medical Research and Innovation, 4(1), e000185. https://doi.org/10.32892/jmri.185.
Boakye, E., Osuji, N., Erhabor, J., et al. (2022). Assessment of patterns in e-cigarette use among adults in the US, 2017–2020. JAMA Network Open, 5(7), e2223266. https://doi.org/10.1001/jamanetworkopen.2022.23266.
Kalkhoran, S. M., Levy, D. E., & Rigotti, N. A. (2022). Smoking and e-cigarette use among U.S. adults during the COVID-19 pandemic. American Journal of Preventive Medicine, 62(3), 341–349. https://doi.org/10.1016/j.amepre.2021.08.018.
Raherison, C., & Girodet, P. O. (2009). Epidemiology of COPD. European Respiratory Review, 18(114), 213–221. https://doi.org/10.1183/09059180.00003609.
Centers for Disease Control and Prevention. (2021). Coronary heart disease. CDC. Retrieved from https://www.cdc.gov/heartdisease/coronary_ad.htm
Cheng, T. Y. D., Chaudhari, P. V., Bitsie, K. R., Striley, C. W., Varma, D. S., & Cottler, L. B. (2022). The HealthStreet cancer survivor cohort: A community registry for cancer research. Journal of Cancer Survivorship. https://doi.org/10.1007/s11764-022-01173-4.
Funding
Funding was provided by the National Institutes of Health and National Clinical and Translational Science Award with Grant No. UL1 TR001427 (P.I.: Mitchell, D). Ting-Yuan David Cheng is supported by the National Cancer Institute with Grant No. R37 CA248371. HealthStreet Funding was provided by University of Florida Clinical and Translational Science Institute. Rebecca Jane Austin-Datta is supported by a Graduate Student Stipend from the Department of Epidemiology, University of Florida. We would like to thank the members of the HealthStreet Community.
Author information
Authors and Affiliations
Contributions
RJAD participated in contributions to conception and design, methodology, data interpretation, project administration, article drafting, article revision, and final manuscript approval. PVC participated in data curation, data analysis, data interpretation, article revision, and final manuscript approval. T-YDC participated in contributions to conception and design, conception and design, methodology, supervision, and final manuscript approval. GK participated in visualization, data interpretation, article revision, and final manuscript approval. CWS participated in contributions to funding acquisition, acquisition of data, methodology, project administration, supervision, article revision, and final manuscript approval. LBC participated in contributions to conception and design, funding acquisition, acquisition of data, methodology, project administration, supervision, article revision, and final manuscript approval.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethical Approval
HealthStreet protocol was approved by the University of Florida Institutional Review Board.
Informed Consent
All participants provide their written consent.
Consent for Publication
All authors consent to publish this manuscript and supplemental materials.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Austin-Datta, R.J., Chaudhari, P.V., Cheng, TY.D. et al. Electronic Nicotine Delivery Systems (ENDS) use Among Members of a Community Engagement Program. J Community Health 48, 338–346 (2023). https://doi.org/10.1007/s10900-022-01169-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10900-022-01169-2