
Abstract
Smoking during pregnancy is associated with poor birth outcomes. The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) is a public nutritional assistance program for low-income pregnant women and their children up to age five. This study examined differences in smoking behavior among women enrolled in the Kansas WIC program. A secondary analysis was conducted using the Pregnancy Nutrition Surveillance System dataset of enrolled women between 2005 and 2011. Geographic residency status was obtained through application of the Census tract-based rural–urban commuting area codes. Chi square tests of association were used to assess differences. Multi-variable binary logistic regression was used to assess maternal characteristics and smoking 3 months prior to pregnancy. Total sample size averaged 21,650 women for years 2005 through 2011. Low-income, rural pregnant women smoked at significantly higher rates before, during, and after pregnancy. High smoking rates have remained unchanged since 2008. The following characteristics were associated with reduced odds of smoking 3 months prior to pregnancy: being 17 years old or younger, Hispanic, a high school graduate, urban location, normal body mass index, no live births prior to current pregnancy, and using multi-vitamins. Results from this study indicate that the WIC population in rural areas may have different needs regarding smoking cessation programming than the urban WIC population. Findings help inform WIC program administrators and assist in enhancing current smoking cessation services to the Kansas WIC population.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Smoking during pregnancy is associated with major adverse health outcomes [1, 2]. Compared to nonsmoking women, women who smoke during pregnancy increase their risk of preterm membrane rupture, prematurity, placenta previa, still births, neonatal mortality, and low birth weight [3–8].
The prevalence of smoking among all U.S. women is 15.3 % [9]. This rate is higher among women of child-bearing age (15–44 years old), with 23.2 % smoking 3 months prior to pregnancy and 10.7 % of pregnant women smoking throughout their pregnancy [10, 11]. Disparities in smoking prevalence are linked to socio-economic status. The smoking rate for women who fall below the federal poverty level is reported at 25.8 % [9] and smoking rates prior to and during pregnancy among this group of women may even be higher. Fortunately, approximately 50 % of women who smoked prior to pregnancy quit before entry into prenatal care [12]. While these quit rates are encouraging, 48 % of women who stopped smoking during pregnancy relapse within 3 months of giving birth [13].
Socio-economic status and geographic location are linked to important infant health indicators. For instance, area-based measures of socio-economic disadvantage have consistently been associated with increased risk of adverse birth outcomes such as low birth weight, prematurity, and infant mortality [14–17]. More importantly, women of lower socio-economic backgrounds who also live in rural areas appear more likely to smoke prior to and during pregnancy than urban, middle-class women [18, 19]. Additionally, compared to urban-focused environments, residing in rural areas has been associated with an increased likelihood of pre-term delivery and low birth weight infants especially for women who smoke [16, 20, 21].
Particularly, increased rates of perinatal and post-neonatal mortality have been observed among rural, low-income women who smoke compared to state-level and national mortality rates [15]. The infant mortality rate (IMR) is an important indicator that measures the health and well-being of a community. Nationally, the infant mortality rate is estimated at 6.07 per 1000 live births in 2011 [22]. In Kansas, the IMR was 6.2 per 1000 live births in 2011 followed by 6.3 per 1000 live births in 2012 and 6.4 per 1000 live births in 2013 [23, 24]. Despite its annual fluctuations, infant mortality has still significantly declined over the last 20 years in Kansas [24]
In addition to adverse birth outcomes, smoking postpartum is also associated with adverse effects on infant health through increased risk of the dangers of second-hand smoke exposure [25] and its impact on certain maternal behaviors such as breastfeeding [26–28]. The short- and long-term health benefits of breastfeeding for mother and infant are well documented [29–43] and current recommendations are that infants be exclusively breastfed for the first 6 months of life [31]. Unfortunately, research evidence shows that smoking is associated with shorter duration of breastfeeding, particularly among women who continue to smoke during their pregnancy [26–28, 44, 45].
Furthermore, research findings report that low-income pregnant women who are publicly insured are at high risk for tobacco use, less likely to quit during their pregnancy, and more likely to relapse after delivery than women who have private insurance [46]. Living in rural locations appears to exacerbate smoking behaviors among this group of women already prone to adverse birth outcomes. Bailey found that Appalachian rural women with high smoking rates were more likely to smoke during pregnancy, had lower incomes, had more prior pregnancies, were less likely to have prenatal care, and smoked longer than women who quit during pregnancy [47]. Wewers and colleagues reported additional risk factors for smoking in Appalachian rural women including younger age (<30), low adult socio-economic position, and depression [48].
Few studies examine socio-demographic differences in smoking prior to, during, and after pregnancy by urban versus rural residence among women enrolled in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC). WIC is a public assistance program that provides nutrition and education to eligible low-income women and children as well as breastfeeding support, immunization screening, and referrals to healthcare and drug/substance abuse services [49]. This study uniquely contributes to existing knowledge about WIC and smoking behaviors in rural versus urban locations by examining differences in smoking behavior among women enrolled in the Kansas WIC program. A predictive model that provides insight into maternal characteristics and pre-pregnancy smoking among WIC participants adds to this knowledge base. Due to the comparative nature of this study, no a priori hypotheses were constructed.
Method
Participants and Procedures
All participants were mothers who enrolled to receive benefits from the Kansas WIC program from 2005 to 2011. After providing informed consent, enrolled women completed a questionnaire related to the Pregnancy Nutrition Surveillance System [50]. Participant data were collected by the Kansas Department of Health and Environment for all Kansas counties before, during, and after pregnancy for each program year. Data were submitted to the Centers for Disease Control and Prevention on a quarterly basis per program year [51].
Geographic residency status was obtained through application of the Census tract-based rural–urban commuting area (RUCA) codes (version 2) [52]. RUCA codes were collapsed into two variables (urban vs. rural) that most accurately described urban and rural classification of residency status in Kansas [53]. Urban residency status was defined as RUCA codes one through three. RUCA codes one through three were defined as metropolitan area “core,” “high commuting,” and “low commuting” respectively [54]. Rural residency status was defined as RUCA codes four through ten. RUCA codes four through six were referred to as micropolitan area “core,” “high commuting,” and “low commuting” respectively [54]. RUCA codes seven through nine were referred to as small town “core,” “high commuting,” and “low commuting” respectively [54]. RUCA code ten was referred to as “rural area” [54]. Participants with missing zip codes and incomplete questionnaires were excluded from the analysis.
In accord with prevailing legal and ethical principles of the Institutional Review Board (IRB) at the University of Kansas School of Medicine-Wichita, this study was determined to be exempt from IRB review.
Instrument
The Pregnancy Nutrition Surveillance System (PNSS) is a program-based public health surveillance system guided by the Centers for Disease Control and Prevention. This system includes state-specific, population-based data on the nutritional status and risk factors of low-income pregnant women who participate in federally funded maternal and child health programs such as the WIC program and Title V of the Maternal and Child Health program [45, 50]. For the present study, data on maternal demographics and maternal smoking behaviors of Kansas WIC participants who were enrolled from 2005 to 2011 were used.
Study Variables
Maternal smoking behaviors for program years 2005–2011 are shown in Table 1 and included the following variables: smoking 3 months prior to pregnancy, smoking at prenatal visit, smoking during the last 3 months of pregnancy, and smoking at postpartum visit. Maternal demographic characteristics and health behaviors by smoking status for program year 2011 are shown in Table 2. For the predictive model, the primary outcome variable was smoking 3 months prior to pregnancy. This variable was defined as mothers who responded “yes” to the question whether they smoked 3 months prior to pregnancy [55, 56]. Predictor variables included maternal age, race/ethnicity, education, rural/urban residency, pre-pregnancy body mass index (BMI), parity, and multi-vitamin use prior to pregnancy. All variables in this study were categorical. Maternal age and race/ethnicity were grouped into categories to facilitate data interpretation.
Statistical Analysis
Descriptive analyses were conducted to examine maternal demographics, health behaviors, and smoking behaviors for WIC participants in urban and rural Kansas. Summary characteristics for all variables were frequencies and percentages. A trend analysis was conducted for program years 2005–2011. Chi square tests of association were used to assess differences between participants who were not smoking 3 months prior to pregnancy versus participants who were smoking 3 months prior to pregnancy. A multi-variable binary logistic regression was used to obtain adjusted odds ratios (AORs) with 95 % confidence intervals (CIs) assessing the characteristics of Kansas WIC participants and smoking 3 months prior to pregnancy. Selection of variables as the referent group was based on evidence in the literature regarding maternal demographic characteristics [9, 10, 15, 46, 48, 57] and health behaviors [47] that would increase the likelihood of a mother smoking prior to or during pregnancy. A P value of ≤.05 was considered statistically significant. Data were analyzed using the SAS System Version 9.3.1 (SAS Institute Inc., Cary, NC, USA).
Results
Between 2005 and 2011, approximately one third of WIC enrolled women in urban and rural locations reported smoking 3 months prior to pregnancy (Table 1). One in five rural pregnant women reported smoking at their prenatal visit, during the last 3 months of pregnancy, and at their postpartum visit.
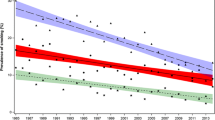
Specifically, from 2005 to 2006, there was a slight increase in smoking prevalence among rural and urban participants (Figs. 1, 2). Between 2006 and 2008, there was a downward trend in smoking prevalence for women in both rural and urban areas. Since 2008, smoking rates remained relatively stable among both rural and urban participants. Across time periods, rural women had consistently higher rates of smoking before, during, and after pregnancy than urban women.

Percentage of smoking in rural Kansas among pregnant WIC participants

Percentage of smoking in urban Kansas among pregnant WIC participants
Approximately one third (33 %) of women who smoked 3 months prior to pregnancy were 20–29 years old followed by women aged 18–19 (32.7 %) (Table 2). The majority of smokers were non-Hispanic white (42.1 %) followed by non-Hispanic black (26.7 %) and other race (25.5 %) (the “other race” category included American Indian, Asian or Hawaiian/Pacific Islander, and Multi-race). More than one third (34.5 %) of women who smoked 3 months prior to pregnancy graduated from high school followed by women who had some high school education (30.2 %).
Additionally, WIC enrolled women located in rural Kansas smoked at higher rates 3 months prior to pregnancy than urban women, 33.3 versus 27.6 % respectively. Women whose pre-pregnancy body mass index (BMI) was <18.5 (underweight) smoked at higher rates (40.2 %) followed by women whose pre-pregnancy BMI was considered normal (31.2 %) or obese (30.2 %). Furthermore, women who had three or more births before their current pregnancy smoked at higher rates than women who did not have any births before their current pregnancy, 32.2 and 29.3 % respectively. Last, women who did not use multi-vitamins before pregnancy smoked at higher rates (31.3 %) than women who used multi-vitamins (26.3 %).
After adjustment for all covariates (Table 3), the following demographic characteristics were significantly associated with decreased odds of smoking 3 months prior to pregnancy: age 17 or younger (AOR = 0.36; CI: 0.30, 0.44), being Hispanic (AOR = 0.11; CI: 0.10, 0.12), and having more than a high school education (AOR = 0.37; CI: 0.34, 0.41). WIC enrolled women located in urban areas were less likely to smoke than rural women (AOR = 0.87; CI: 0.82, 0.94). Compared to women with normal pre-pregnancy weight (BMI: 18.5–24.9), underweight women (BMI: <18.5) were 25 % more likely to smoke 3 months prior to pregnancy (AOR = 1.25; CI: 1.06, 1.46). Additionally, compared to women with normal pre-pregnancy weight, no other statistically significant differences exist for overweight (BMI: 25–29.9) or obese (BMI: >30) women. Women who had no births before their current pregnancy were less likely to smoke (AOR: 0.79; CI: 0.71, 0.87) followed by WIC enrolled women who had two births before their current pregnancy (AOR: 0.87; CI: 0.79, 0.97). Last, women who used multi-vitamins before pregnancy were less likely to smoke (AOR: 0.71; CI: 0.65, 0.77) than women who did not use multi-vitamins.
Discussion
Our findings demonstrate that there are differences in smoking rates based on geographic location among the WIC population. This study is different from others in that smoking among rural pregnant women enrolled in the WIC program was contrasted to smoking among urban pregnant women enrolled in WIC. Overall, rural pregnant women smoked at higher rates before, during, and after pregnancy compared to urban women and results indicate that high prevalence rates among the WIC population in rural and urban settings have remained unchanged since 2008.
WIC enrolled women in rural Kansas smoked at particularly higher rates 3 months prior to pregnancy compared to urban women. Also, underweight women smoked at higher rates 3 months prior to pregnancy than women who were overweight or obese. Additionally, WIC enrolled women who had three or more births before their current pregnancy smoked at higher rates 3 months prior to pregnancy than women who did not have any births prior to their current pregnancy.
Furthermore, the following characteristics were associated with reduced odds of smoking 3 months prior to pregnancy: being 17 years old or younger, Hispanic, having an education beyond high school, residing in an urban location, having a normal body mass index, not having had any live births prior to the current pregnancy, and using multi-vitamins.
This study’s findings are consistent with previous research that reports a higher prevalence of smoking in rural versus urban areas especially among reproductive-aged women [47, 48, 58, 59]. Our findings indicate that this is true among rural, low-income pregnant WIC populations. Compared to urban women, rural pregnant women smoked at much higher rates 3 months prior to pregnancy and continued to smoke at high rates during and after pregnancy as well. This finding illustrates the need for smoking cessation programming specifically targeting women of reproductive age during the pre-conception period.
This study also confirms earlier findings that young rural adults between the ages of 18 to 34 smoke at especially high rates [59]. In this study, compared to 20–29 year olds, 18–19 year old women were more likely to smoke 3 months prior to pregnancy than women = or <17 years old or women >30. Research findings indicate that residents of rural communities generally start smoking at a younger age and continue smoking for longer periods of time [60]. Given this finding, women who smoke at the age of 18 or 19, as reported in this study, may experience adverse health outcomes with potentially subsequent pregnancies as they are more likely to continue smoking. Again, smoking cessation programming specifically targeting reproductive-aged young women becomes critical.
Additionally, research findings report that lower rural socio-economic status, as measured by education level and annual household income, are associated with higher rates of smoking [47, 48, 58]. Consistent with this research, the current study reports that women with a high school diploma or less smoked at significantly higher rates 3 months prior to pregnancy compared to women who had more than a high school education. Also, being a high school graduate increases one’s odds of smoking 3 months prior to pregnancy. As all women in this study are considered low-income, these findings are particularly troublesome considering the addictive properties of nicotine and increasing prices of cigarettes for women who can least afford it, but who smoke at high rates!
Overall, this study’s findings are important because they have major health consequences for women and their children. Geographic location, race, age, education level, body mass index, parity, and vitamin use should all be taken into account when designing smoking cessation interventions. It may be tempting to treat public assistance programs such as the WIC program alike and develop a smoking cessation program that fits all participants. However, our findings indicate that one size does not fit all and that intervention programs need to be culturally, geographically, and demographically appropriate.
Implications for Public Health Practice and Research
The Kansas Department of Health and Environment reports that in about one quarter of all infant deaths that took place between 2007 and 2011 in Kansas, the mother reported smoking at some time during her pregnancy [61]. While we do not imply the association between WIC mothers who smoke and reported infant deaths, we do know that high smoking rates for this same time period remained unchanged among women who received WIC benefits. To better understand the risk of smoking on poor birth outcomes among women enrolled in a WIC program, further research is needed.
In addition, infant deaths in urban versus rural locations should be examined for linkages to maternal smoking behavior and the timeline of this behavior. Rural women in particular were smoking at much higher rates 3 months prior to pregnancy than urban women, 33.3 versus 27.6 % respectively. When one compares these rates to a national smoking rate of 23.2 % 3 months prior to pregnancy, smoking prevalence for rural women is especially high. Furthermore, this study’s results indicate that WIC enrolled women who had two or more births before their current pregnancy were more likely to smoke 3 months prior to pregnancy compared to women who had no live births prior to pregnancy. This makes one wonder about young children in the home exposed to secondary smoke and its association with infant mortality though it must be noted that this is a complex area of study involving a multitude of risk factors and that smoking is merely one of these risk factors.
It is imperative that women who are in their reproductive years be informed about the risks of smoking related to their infant’s and their own health. Smoking cessation interventions should target women at all stages of the reproductive years (before, during, and after pregnancy) but should especially target rural WIC enrolled women with young children before a recurring pregnancy. Results from additional research in these areas will inform the development of smoking cessation interventions and help craft preventive messages around smoking, maternal health, and infant health.
Smoking also reduces the likelihood of breastfeeding [26–28, 44, 45]. Though women enrolled in the Kansas WIC program started breastfeeding at high rates [62], they did not continue breastfeeding for 6 months as recommended by the American Academy of Pediatrics [31]. While early breastfeeding cessation can be attributed to a number of factors, smoking is a modifiable behavior that should be addressed so that women can continue breastfeeding. Therefore, it may be useful to incorporate an educational component on the risks of smoking to mother and infant in breastfeeding support interventions especially those that target the WIC population. Moreover, an effective smoking cessation component may be particularly important in efforts to encourage women to breastfeed for longer periods of time.
Limitations and Future Direction
One of the limitations of this study is self-report bias of the PNSS surveillance system. Smoking behaviors during pregnancy may carry a certain stigma and cause individuals to report less of the behavior than is actually taking place though research reports that women are truthful when reporting their smoking habits during pregnancy [63]. The findings from this study are also somewhat limited in that they may not be generalizable to all states. States that did not participate in the PNSS may still provide WIC benefits. Therefore, national PNSS reports are not representative of all WIC programs and are also not representative of all low-income pregnant women. The national report is representative of the population that is served by the public health programs submitting the data and this includes Kansas. Last, in order to draw stronger conclusions about smoking behaviors, infant mortality, and breastfeeding behaviors among rural and urban pregnant WIC women, additional research should be conducted.
Conclusion
The main goal of this study was to shed light on smoking behaviors among the pregnant WIC population in Kansas. It appears that WIC participants in Kansas smoked at higher rates before, during, and after pregnancy than WIC participants nationally and that smoking prevalence was higher for rural compared to urban women. A trend analysis discovered that smoking rates among WIC women have remained high for the last few years. This finding underscores the need for effective smoking cessation programming targeting rural women of reproductive age particularly during pre-conception. Results from this study add to the current literature in that the rural WIC population may have different needs regarding smoking cessation programming than the urban WIC population and that interventions should be culturally, geographically, and demographically appropriate. Furthermore, this study’s results will help inform WIC program administrators of smoking behaviors and assist in enhancing current services and their delivery to the Kansas WIC population.
References
Centers for Disease Control and Prevention. Tobacco use and pregnancy. Retrieved January 24, 2015, from http://www.cdc.gov/reproductivehealth/tobaccousepregnancy/
Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health. (2010). How tobacco smoke causes disease: The biology and behavioral basis for smoking-attributable disease: A report of the Surgeon General. Retrieved from http://www.ncbi.nlm.nih.gov/books/NBK53017/
Centers for Disease Control and Prevention, Office on Smoking and Health. (2001). Women and smoking: A report of the Surgeon General. Retrieved from http://www.ncbi.nlm.nih.gov/books/NBK44303/
Ventura, S. J., Hamilton, B. E., Mathews, T., & Chandra, A. (2003). Trends and variations in smoking during pregnancy and low birth weight: Evidence from the birth certificate, 1990–2000. Pediatrics, 111, 1176–1180.
Chelchowska, M., Ambroszkiewicz, J., Jablonka-Salach, K., Gajewska, J., Maciejewski, T. M., Bulska, E., & Leibschang, J. (2013). Tobacco smoke exposure during pregnancy increases maternal blood lead levels affecting neonate birth weight. Biological Trace Element Research, 155, 169–175. doi:10.1007/s12011-013-9775-8.
Ko, T. J., Tsai, L. Y., Chu, L. C., Yeh, S. J., Leung, C., Chen, C. Y., & Hsieh, W. S. (2013). Parental smoking during pregnancy and its association with low birth weight, small for gestational age, and preterm birth offspring: A birth cohort study. Pediatrics and Neonatology,. doi:10.1016/j.pedneo.2013.05.005.
Raisanen, S., Sankilampi, U., Gissler, M., Kramer, M. R., Hakulinen-Viitanen, T., Saari, J., & Heinonen, S. (2013). Smoking cessation in the first trimester reduces most obstetric risks, but not the risks of major congenital anomalies and admission to neonatal care: A population-based cohort study of 1,164,953 singleton pregnancies in Finland. Journal of Epidemiology and Community Health,. doi:10.1136/jech-2013-202991.
Zhang, K., & Wang, X. (2013). Maternal smoking and increased risk of sudden infant death syndrome: A meta-analysis. Legal Medicine, 15, 115–121. doi:10.1016/j.legalmed.2012.10.007.
Jamal, A., Agaku, I. T., O’Connor, E., King, B. A., Kenemer, J. B., & Neff, L. (2014). Current cigarette smoking among adults—United States, 2005–2013. Morbidity and Mortality Weekly Report, 63, 1108–1112.
Tong, V., Dietz, P., Morrow, B., D’Angelo, D., Farr, S., Rockhill, K., & England, L. (2013). Trends in smoking before, during, and after pregnancy—Pregnancy Risk Assessment Monitoring System, United States, 40 Sites, 2000–2010. Morbidity and Mortality Weekly Report, 62, 1–19.
Dalenius, K., Brindley, P., Smith, B., Reinold, C., & Grummer-Strawn, L. M. (2012). Pregnancy Nutrition Surveillance 2010 Report. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention.
Tong, V., England, L., Dietz, P., & Asare, L. (2008). Smoking patterns and use of cessation interventions during pregnancy. American Journal of Preventive Medicine, 35, 327–333. doi:10.1016/j.amepre.2008.06.033.
Tran, T., Reeder, A., Funke, L., & Richmond, N. (2013). Association between smoking cessation interventions during prenatal care and postpartum relapse: Results from 2004 to 2008 multi-state PRAMS data. Maternal and Child Health Journal, 17, 1269–1276. doi:10.1007/s10995-012-1122-8.
Blumenshine, P., Egerter, S., Barclay, C. J., Cubbin, C., & Braveman, P. A. (2010). Socioeconomic disparities in adverse birth outcomes: A systematic review. American Journal of Preventive Medicine, 39, 263–272. doi:10.1016/j.amepre.2010.05.012.
McElroy, J. A., Bloom, T., Moore, K., Geden, B., Everett, K., & Bullock, L. F. (2012). Perinatal mortality and adverse pregnancy outcomes in a low-income rural population of women who smoke. Birth Defects Research. Part A: Clinical and Molecular Teratology, 94, 223–229. doi:10.1002/bdra.22891.
Strutz, K. L., Dozier, A. M., van Wijngaarden, E., & Glantz, J. C. (2012). Birth outcomes across three rural-urban typologies in the Finger Lakes region of New York. Journal of Rural Health, 28, 162–173.
American College of Obstetricians and Gynecologists. (2014). Committee Opinion No. 586: Health disparities in rural women. (2014). Obstetrics and Gynecology, 123, 384–388. doi:10.1097/01.AOG.0000443278.06393.d6.
Shoff, C., & Yang, T. C. (2013). Understanding maternal smoking during pregnancy: Does residential context matter? Social Science and Medicine, 78, 50–60. doi:10.1016/j.socscimed.2012.11.027.
Song, H., & Fish, M. (2006). Demographic and psychosocial characteristics of smokers and nonsmokers in low-socioeconomic status rural Appalachian 2-parent families in Southern West Virginia. Journal of Rural Health, 22, 83–87. doi:10.1111/j.1748-0361.2006.00011.x.
Hillemeier, M. M., Weisman, C. S., Chase, G. A., & Dyer, A.-M. (2007). Individual and community predictors of preterm birth and low birthweight along the rural–urban continuum in Central Pennsylvania. Journal of Rural Health, 23, 42–48. doi:10.1111/j.1748-0361.2006.00066.x.
Bailey, B. A., & Cole, L. K. (2009). Rurality and birth outcomes: Findings from Southern Appalachia and the potential role of pregnancy smoking. Journal of Rural Health, 25, 141–149. doi:10.1111/j.1748-0361.2009.00210.x.
National Center for Health Statistics. National Vital Statistics Reports. Deaths: Final data for 2011. Retrieved from http://www.cdc.gov/nchs/data_access/Vitalstatsonline.htm
Kansas Department of Health and Environment, Bureau of Epidemiology and Public Health Informatics, Division of Public Health. Infant mortality Kansas, 2012 research brief. Retrieved December 9, 2013, from http://kdheks.gov/bephi/
Kansas Department of Health and Environment, Bureau of Epidemiology and Public Health Informatics, Division of Public Health. Infant mortality Kansas, 2013 research brief. Retrieved January 28, 2015, from http://kdheks.gov/bephi/
Hawkins, S. S., & Berkman, L. (2013). Identifying infants at high-risk for second-hand smoke exposure. Child Care, Health and Development,. doi:10.1111/cch.12058.
Liu, J., Rosenberg, K. D., & Sandoval, A. P. (2006). Breastfeeding duration and perinatal cigarette smoking in a population-based cohort. American Journal of Public Health, 96, 309–314. doi:10.2105/ajph.2004.060798.
Scott, J. A., Binns, C. W., Oddy, W. H., & Graham, K. I. (2006). Predictors of breastfeeding duration: Evidence from a cohort study. Pediatrics, 117, e646–e655. doi:10.1542/peds.2005-1991.
Gerd, A. T., Bergman, S., Dahlgren, J., Roswall, J., & Alm, B. (2012). Factors associated with discontinuation of breastfeeding before 1 month of age. Acta Paediatrica, 101, 55–60. doi:10.1111/j.1651-2227.2011.02405.x.
Horta, B. L., Bahl, R., Martines, J. C., & Victora, C. G. (2007). Evidence on the long-term effects of breastfeeding—systematic reviews and meta-analyses. Geneva: World Health Organization.
Ip, S., Chung, M., Raman, G., Chew, P., Magula, N., DeVine, D.,… Lau, J. (2007). Breastfeeding and maternal and infant health outcomes in developed countries. Evidence Report/Technology Assessment, 153, 1–186.
American Academy of Pediatrics. (2012). Breastfeeding and the use of human milk. Pediatrics, 129, e827–e841. doi:10.1542/peds.2011-3552.
Duijts, L., Jaddoe, V. W., Hofman, A., & Moll, H. A. (2010). Prolonged and exclusive breastfeeding reduces the risk of infectious diseases in infancy. Pediatrics, 126, e18–e25. doi:10.1542/peds.2008-3256.
Heinig, M. J. (2001). Host defense benefits of breastfeeding for the infant. Effect of breastfeeding duration and exclusivity. Pediatric Clinics of North America, 48, 105–123. ix.
Ladomenou, F., Moschandreas, J., Kafatos, A., Tselentis, Y., & Galanakis, E. (2010). Protective effect of exclusive breastfeeding against infections during infancy: A prospective study. Archives of Disease in Childhood, 95, 1004–1008. doi:10.1136/adc.2009.169912.
Huffman, S. L., Zehner, E. R., & Victora, C. (2001). Can improvements in breast-feeding practices reduce neonatal mortality in developing countries? Midwifery, 17, 80–92. doi:10.1054/midw.2001.0253.
McVea, K. L., Turner, P. D., & Peppler, D. K. (2000). The role of breastfeeding in sudden infant death syndrome. Journal of Human Lactation, 16, 13–20.
Vennemann, M. M., Bajanowski, T., Brinkmann, B., Jorch, G., Yucesan, K., Sauerland, C., & Mitchell, E. A. (2009). Does breastfeeding reduce the risk of sudden infant death syndrome? Pediatrics, 123, e406–e410. doi:10.1542/peds.2008-2145.
Gerstein, H. C. (1994). Cow’s milk exposure and type I diabetes mellitus. A critical overview of the clinical literature. Diabetes Care, 17, 13–19.
Bernier, M. O., Plu-Bureau, G., Bossard, N., Ayzac, L., & Thalabard, J. C. (2000). Breastfeeding and risk of breast cancer: A meta-analysis of published studies. Human Reproduction Update, 6, 374–386.
Danforth, K. N., Tworoger, S. S., Hecht, J. L., Rosner, B. A., Colditz, G. A., & Hankinson, S. E. (2007). Breastfeeding and risk of ovarian cancer in two prospective cohorts. Cancer Causes and Control, 18, 517–523. doi:10.1007/s10552-007-0130-2.
Jordan, S. J., Cushing-Haugen, K. L., Wicklund, K. G., Doherty, J. A., & Rossing, M. A. (2012). Breast-feeding and risk of epithelial ovarian cancer. Cancer Causes and Control, 23, 919–927. doi:10.1007/s10552-012-9963-4.
Schwarz, E. B., Brown, J. S., Creasman, J. M., Stuebe, A., McClure, C. K., Van Den Eeden, S. K., & Thom, D. (2010). Lactation and maternal risk of type 2 diabetes: A population-based study. American Journal of Medicine, 123, e861–e866. doi:10.1016/j.amjmed.2010.03.016.
Stuebe, A. M., Rich-Edwards, J. W., Willett, W. C., Manson, J. E., & Michels, K. B. (2005). Duration of lactation and incidence of type 2 diabetes. Journal of the American Medical Association, 294, 2601–2610. doi:10.1001/jama.294.20.2601.
Amir, L. H., & Donath, S. M. (2003). Does maternal smoking have a negative physiological effect on breastfeeding? The epidemiological evidence. Breastfeeding Review, 11, 19–29.
Jacobson, L. T., Twumasi-Ankrah, P., Redmond, M. L., Ablah, E., Hines, R. B., Johnston, J., & Collins, T. C. (2015). Characteristics associated with breastfeeding behaviors among urban versus rural women enrolled in the Kansas WIC program. Maternal and Child Health Journal, 19, 828–839. doi:10.1007/s10995-014-1580-2.
Tong, V., Jones, J., Dietz, P., D’Angelo, D., & Bombard, J. (2009). Trends in smoking before, during, and after pregnancy: Pregnancy Risk Assessment Monitoring System (PRAMS), United States, 31 sites, 2000–2005. Morbidity and Mortality Weekly Report, 58, 1–29.
Bailey, B. A. (2006). Factors predicting pregnancy smoking in Southern Appalachia. American Journal of Health Behavior, 30, 413–421. doi:10.5555/ajhb.2006.30.4.413.
Wewers, M. E., Salsberry, P. J., Ferketich, A. K., Ahijevych, K. L., Hood, N. E., & Paskett, E. D. (2012). Risk factors for smoking in rural women. Journal of Women’s Health, 21, 548–556. doi:10.1089/jwh.2011.3183.
U.S. Department of Agriculture, Food and Nutrition Service. Women, Infants and Children (WIC), WIC Benefits and Services. Retrieved December 18, 2013, from http://www.fns.usda.gov/wic/wic-benefits-and-services
Centers for Disease Control and Prevention. What is PedNSS/PNSS? What is PNSS? Retrieved February 6, 2015, from http://www.cdc.gov/pednss/what_is/pnss/index.htm
Centers for Disease Control and Prevention. What is PedNSS/PNSS? What is PNSS? What data are collected and analyzed? Retrieved May 27, 2014, from http://www.cdc.gov/pednss/what_is/pnss/what_data.htm
U.S. Department of Agriculture. 2000 rural–urban commuting area codes. Retrieved June 5, 2013, from http://www.ers.usda.gov/data-products/rural-urban-commuting-area-codes.aspx
U.S. Department of Agriculture, Economic Research Service. Kansas-rural definitions: State-level maps. Retrieved February 12, 2015, from http://www.ers.usda.gov/datafiles/Rural_Definitions/StateLevel_Maps/KS.pdf
WWAMI RUCA Rural Health Research Center. RUCA data code definitions: Version 2. Retrieved February 14, 2015, from http://depts.washington.edu/uwruca/ruca-codes.php
Centers for Disease Control and Prevention. (2004). Pregnancy Nutrition Surveillance System user’s guide. Field definitions, codes, and edits. Retrieved from http://www.cdc.gov/pednss/additional_tools/pnss_users_guide/PNSS_Users_Guide_Fields.pdf
Centers for Disease Control and Prevention. (2004). Pregnancy Nutrition Surveillance System User’s Guide. Record Specifications. Retrieved from http://www.cdc.gov/pednss/additional_tools/pnss_users_guide/PNSS_Users_Guide_Record_Specs.pdf
Baron, R., Mannien, J., de Jonge, A., Heymans, M. W., Klomp, T., Hutton, E. K., & Brug, J. (2013). Socio-demographic and lifestyle-related characteristics associated with self-reported any, daily and occasional smoking during pregnancy. PLoS ONE, 8, e74197. doi:10.1371/journal.pone.0074197.
Doescher, M. P., Jackson, J. E., Jerant, A., & Gary Hart, L. (2006). Prevalence and trends in smoking: A national rural study. Journal of Rural Health, 22, 112–118. doi:10.1111/j.1748-0361.2006.00018.x.
Horn, K. (2012). Cutting tobacco’s rural roots: Tobacco use in rural communities. Retrieved December 11, 2013, from http://www.lung.org/about-us/publications/
Lutfiyya, M. N., Shah, K. K., Johnson, M., Bales, R. W., Cha, I., McGrath, C., … Lipsky, M. S. (2008). Adolescent daily cigarette smoking: Is rural residency a risk factor? Rural Remote Health, 8, 875
Kansas Department of Health and Environment, Bureau of Epidemiology and Public Health Informatics, Division of Public Health. Selected Special Statistics, Stillbirths, and Infant Deaths Kansas, 2011. Retrieved December 9, 2013, from http://www.kdheks.gov/phi/index.htm
U.S. Department of Agriculture, Food and Nutrition Service, Office of Research and Analysis. (2011). WIC Participant and Program Characteristics 2010. Retrieved June 15, 2013, from http://www.fns.usda.gov/ora/MENU/Published/WIC/FILES/WICPC2010.pdf
Ross, J. A., Swensen, A. R., & Murphy, S. E. (2002). Prevalence of cigarette smoking in pregnant women participating in the special supplemental nutrition programme for Women, Infants and Children (WIC) in Minneapolis and Saint Paul, Minnesota, USA. Paediatrica and Perinatal Epidemiology, 16, 246–248.
Acknowledgments
The authors would like to thank Martha Hagen, MS, RD, LD, IBCLC, State of Kansas WIC Breastfeeding Coordinator, and Sandy Perkins, MS, RD, LD, former Acting State of Kansas WIC Nutrition Services Director with the Kansas Department of Health and Environment for supplying the University of Kansas School of Medicine-Wichita with the dataset.
Conflict of interest
The authors have no conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Jacobson, L.T., Dong, F., Scheuermann, T.S. et al. Smoking Behaviors Among Urban and Rural Pregnant Women Enrolled in the Kansas WIC Program. J Community Health 40, 1037–1046 (2015). https://doi.org/10.1007/s10900-015-0029-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10900-015-0029-x