
Abstract
We identified fifty-one peer-reviewed studies that geospatially analyzed the relationship between the community nutrition environment (CNE) and obesity. Eighty percent of studies found at least one significant association between the CNE and obesity. However we calculated the proportion of studies that found at least one significant association between the CNE and obesity in the expected direction for each food store type and measurement technique, and the proportion across the different store types and measurement techniques was just 32 %. Different methods for classifying, locating, and analyzing food stores produced mixed results and challenged direct study level comparison.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
An increased prevalence of obesity in the United States over the last two decades has led to hundreds of thousands of excess deaths annually [1–3]. This increase has coincided with changes in home, school, community and other environments that influence diet and health-related behavior [4, 5]. The “community nutrition environment” (CNE), which defines the number, type, location and accessibility of food outlets, is of particular interest to both researchers and policy-makers since the ubiquity of unhealthy foods and lack of access to healthy foods may contribute to the obesity epidemic [6–9].
Prior reviews of food environments and obesity have not focused on the CNE, have included only a relatively small number of studies (<20), or were conducted before 2010 [9–11]. The burgeoning interest in food deserts and interventions on access to healthy food among both researchers and practitioners demands the most up-to-date evidence. Moreover, evidence on the food environment is being applied in increasingly proactive ways, such as in Health Impact Assessments (HIAs). HIAs use existing research—often relying on systematic reviews and meta-analysis—to estimate future effects of policies, plans and projects. This demand for timely and robust data has reinforced the need for research frameworks, study designs and metrics that maximize comparability across studies. To fill these gaps, we reviewed studies of the CNE and obesity, examining the methods, metrics and results.
Methods
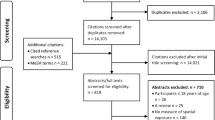
We searched the MEDLINE database using the terms “Access to Healthy Foods”, “Built Environment”, “Food Access”, “Food Environment”, “Supermarket”, and “Food Desert”, paired with “BMI”, “Diet”, “Obesity”, and “Overweight”, for a total of 24 queries. We limited the search to peer-reviewed journal articles in the English-language and conducted in human populations between July 1, 2002, and July 1, 2012. From a total of 673 articles, we excluded 552 based on the article’s title and abstract because they did not directly analyze the food store number, type, location or other aspect of the community nutrition environment. Of the remaining 121 articles, we excluded 72 that were conducted outside the United States, did not spatially analyze the food environment, or did not have an obesity-related health outcome. From the remaining 49 articles we used the “snowball” technique and checked all citations to include an additional 21 articles. Of these final 70 studies, 13 were excluded because they were review articles, two were excluded because the obesity outcomes were projections rather than direct measurements (computer simulations), two because the measures were put into an index so direct interpretation was not possible and two more because although they spatially analyzed the food environment, they did not measure food store presence, frequency or distance. A total of fifty-one remaining relevant articles were included in the review. (Figure 1, Appendix 1).

Study exclusions and inclusions
For each study we classified the technique for spatially measuring food stores as frequency, proximity, or presence. Frequency includes count, density, and ratio measures. We also identified the type of food store. Studies often applied one measurement technique (e.g. presence) but examined multiple associations, stratifying by race, gender, income, or other demographic or socioeconomic variables. Studies also applied different types and sizes of buffers around areas of interest. A buffer is a distance around a point of interest such as a home or school that is used to represent an estimate of that individual’s food environment. A Euclidean buffer encompasses points of interest within a straight-line radius while a network buffer represents the distance around one point one could travel accounting for the roads and available walkways.
For each combination of food store type and measurement technique, we characterized a study as having a positive, negative or null finding depending on the observed associations between the food store and obesity. If any association was found to be positive or negative for a certain food store type and measurement technique in a study, the study was considered to have found a positive or negative finding between that food store type with that measurement technique, and obesity. For example, if a study analyzed the association between the proximity to a fast food restaurant and obesity for males and females and found a significant association in just one gender, the study was recorded as having found a positive finding for measuring the relationship between proximity to fast food restaurants and obesity. This criteria was applied regardless of the number of associations tested, meaning if a study analyzed the association between the presence of a convenience store and obesity at three different buffer lengths and separately for males and females, if at least one association was found to be positive the study was recorded as having a positive finding regarding the association between the presence of a convenience store and obesity. We calculated the proportion of studies that found at least one significant association between the CNE and obesity in the expected direction from the total number of findings. We looked at findings across the six most common store types (fast food restaurant, convenience stores, small food stores, grocery stores, supermarkets and full service restaurants) and measurement techniques (frequency, proximity and presence). In one instance a study found both a positive and negative finding for a food store type and food store measure and was included in the review as a positive and negative finding [12].
All but two studies used BMI to determine obesity or overweight status. The formula to calculate one’s BMI is weight (kg)/[height (m)]2. All studies used BMI cutoffs consistent with the CDC’s definition for BMI Z-Scores or adult BMI where a BMI between 25.0 and 29.9 is indicative of being overweight and a BMI ≥30 indicates obesity [13]. Alternate methods included using a maternal weight >200 lbs. as a proxy for obesity [14], and using different standards that adjust for age and gender in assessing the weight status of adolescents [15].
Results
Study Parameters
Of the 51 articles examined (Table 1), 32 analyzed adults and 19 investigated children and/or adolescents. Forty studies used a cross sectional design, four used repeated cross sections, and seven used a longitudinal design. We abstracted details on the methods and results focusing on the geographic scope of each study, referring to the bounded area that the author wished to make inferences about, and the level at which the food environment was measured. The scope of the studies ranged from cities to the entire United States, with the most common being cities (n = 9), counties (n = 7), states (n = 12) and the nation (n = 13). Within these scopes the food environment was analyzed at different levels, most commonly homes with surrounding buffers (n = 13), census tracts (n = 11), and counties (n = 8).
Measuring the Community Nutrition Environment
There was substantial variation in how food stores were spatially measured, located, and classified (Table 2). The CNE was defined by presence (n = 13), proximity (n = 13) and three frequency measures, density (n = 23), count (n = 16), and ratios of stores (n = 3). Sixteen studies used a combination of these spatial methods. Density refers to the number of stores within a specified area measure such as a census tract, or one square mile. Density was separated into three categories: the number of stores per capita (n = 12), the number of stores per area (n = 11), and all other measures of density (n = 2). Count refers to the number of stores within a specified distance, for example the number of stores within a 1 mile buffer of a home or school. Ratios were typically used as the number of healthy stores divided by the number of unhealthy stores. Presence is a binary measure that indicates the presence of at least one store in a specified area. Proximity is a measure of the distance between a store and a point of interest such as a school or home.
To locate food stores, studies used commercial databases (n = 25), government sources (n = 25), field measurements (n = 4), or the Yellow Pages (n = 7). Nine studies used a combination of these methods. Only two Dun and Bradstreet (n = 10) and Info USA (n = 9) of the seven databases were used in multiple studies. Studies determined food stores type using government coding systems including North American Industry Classification System (n = 21) and Standard Industrial Classification codes (n = 13). However, actual codes were provided in just 56 % of studies.
Buffer Zones
Among 20 studies using buffers there were fourteen different buffer sizes ranging from 1/10 of a mile to 10 miles. One mile (n = 9), 1/2 mile (n = 10), and 1/4 mile (n = 7) were the most commonly used buffer sizes. Network buffers, which measure distance using streets and sidewalks, were applied in nine studies and Euclidean buffers, which measure straight line distance, were used in eight studies. In one study both buffer types were applied and in two other studies the buffer type was unknown. Seven of the nine studies that used Network buffers found at least one significant association while five of the eight studies that used Euclidean buffers found at least one significant association. Five studies found varying results depending on the buffer size used.
Measured Effects
The relationship between the CNE and obesity varied widely across the different types of food stores and measurement techniques (Table 3). Fast food restaurants (n = 48), convenience stores (n = 30) and supermarkets (n = 29) were the most frequently tested store types, where these numbers represent the number of findings found across the studies. Fast food restaurants and convenience stores are hypothesized to contribute to the consumption of unhealthy food and obesity, while supermarkets are hypothesized to increase the consumption of fruits and vegetables and therefore promote a healthy weight. Studies analyzing the presence of convenience stores (n = 7), fast food restaurants (n = 7), and supermarkets (n = 9) corroborated these hypotheses 71, 71, and 38 % of the time respectively. Among the six most commonly analyzed food stores—fast food restaurants, convenience stores, supermarkets, grocery stores, small grocery stores, and full service restaurants −32 % of findings found at least one significant association with obesity in the expected direction, 10 % of findings found at least one significant association in the unexpected direction, and 58 % of findings found no association. A finding refers to each time a study analyzed a specific food store type using frequency, proximity, or presence. If they found at least one positive or negative association, they were recorded as finding a positive or negative finding, respectively. Among studies that found a statistically significant association between the CNE and obesity, the effect sizes were typically small and the p-values were usually borderline significant. For example, three studies (ID#’s 30, 33, 38) found fast food restaurant frequency to be significantly associated with odds of obesity and provided odds ratios. These odds ratios ranged from 1.05 to 1.79 and the lower 95 % confidence limit were consistently close to 1.0. Reference groups for these calculations varied, with some studies using quartiles of fast food restaurant frequency and others using different population subsets.
Discussion
Overview of Study Results
The initial purpose of this review was to examine the effects of the CNE on obesity. However the heterogeneity of the metrics applied precluded a conclusive summary of effect size and therefore we focused on describing the application of metrics across studies. Although the methods and results of individual studies were inconsistent, as a whole this body of research suggests that food environments are associated with obesity. Most studies (80 %) found at least one statistically significant association between the food environment and obesity. However, many studies looked at multiple associations with obesity, using different food store types and measurement techniques including frequency, proximity, and presence. When considering the balance of positive, negative and null findings among the studies and the varying store types and measurement techniques, the percent of statistically significant findings in the expected direction drop to 32 %.
Results varied widely by food store type and measurement technique. Thirty-seven percent of findings from studies analyzing the association between the frequency of fast food restaurant stores and obesity found a positive correlation. This was the largest percent of findings found in the expected direction for any specific food store type and measurement technique where there were ten or more findings. This may be because fast food outlets act as both a direct determinant of obesity and as a proxy for other obesity-related neighborhood conditions [16]. Among all studies, including those where there were <10 findings, studies using the presence measure to assess the CNE were the most likely to have significant findings in the expected direction. This may be because the presence of a store best captures an individual’s ability to access certain foods. We found that compared with adult studies, those of children and adolescents were less likely to observe a significant finding relating obesity to the food environment. This may be due to several things, including children’s’ participation in school breakfast and lunch programs which crowd out opportunities for fast food consumption. However, the variation in metrics along with the different food stores examined across these studies made it difficult to interpret these comparisons.
Study Designs
The vast majority of studies were cross-sectional, which provide a limited view of the relationship between the food environment and obesity, since they cannot draw causal inferences or directionality. Longitudinal studies can further elucidate the relationship between CNE and obesity. We found that four of the seven studies using a longitudinal study design were conducted between during or after 2011, suggesting increased investment in this more rigorous design.
Defining the Consumer Nutrition Environment
Expanding the CNE to include more food store types and considering the accessibility of food stores would lead to more accurate depictions of one’s food environment. Determining a population or individual’s car ownership status also has implications for determining an appropriate buffer size.
More recent studies are measuring a broader community nutrition environment including farmer’s markets [15, 17] emergency food stores [18], flea markets [19], direct farm sales [20], and other unaddressed food sources. Other potential food sources such as community gardens are less well-studied. Including more food store and food source types will yield a more accurate measurement of the community nutrition environment.
Variables that influence people’s ability to get to food stores are an important but often unmeasured component of food access [21, 22]. We found that studies did not consistently report whether people had access to an automobile. Additionally, the majority of studies did not address public transit and other components of the built environment that may support food procurement. Although some of this data is available from the census (car ownership) or direct observation (bus stops and transit stops), the resources required to obtain and use this data for defining the CNE are unclear. The lack of such data will continue to limit the ability of researchers to draw inference regarding the relationship between the CNE and obesity.
Researchers applied different buffer types and varying buffer sizes often without justification. Research suggests a network buffer is typically preferable to a Euclidean buffer as it accounts for the city streets and actual path a person would take to get to a food store [15, 23]. However, recent studies continue to implement Euclidean buffers without discussion [17, 24]. The size of a buffer should reflect a population’s age, their transportation abilities, and existing research. Of 2,384 adult participants of The Multi-Ethnic Study of Atherosclerosis, 47 % indicated they did most of their food shopping within one mile of their home [25]. Based on this example, researchers need to apply appropriate buffer sizes to adequately describe individual’s food environments. Although the different buffer sizes and types did not appear to influence effect size and significance, the issue of determining an appropriate buffer size and type highlights the challenges of measuring the CNE for diverse populations with different abilities to procure food. However, the justification of buffer types and sizes for certain food store types and populations would likely provide more realistic measures of access. Moreover, standardization within the tools used to calculate and measure buffers could support comparable studies. A new buffering method called the “sausage” network buffer may be more easily replicable across different software and yield results similar to network buffers [26]. A “sausage” network buffer is created by buffering all roads out a certain “street distance” from the starting point, and for a radius of some number of meters on each side of the road center line. Although this method still needs to be evaluated, it can be used across different mapping software which could lead to more consistent data analysis.
Classifying Food Store Types
Identifying food store types is also a crucial aspect of interpreting a community nutrition environment. Unfortunately, there is not a consistent definition for fast food restaurants [27]. Often, definitions are derived from the North American Industry Classification System (NAICS) code for limited service restaurants. However, we could not confirm definitions since <2–3 of studies we reviewed that used NAICS codes, identified the codes they used. Moreover, many researchers chose to modify the “fast food” category, often forming their own unique definition of a fast food restaurant [15, 28]. Researchers have also created new categories of food stores by combining NAICS codes, such as supercenters and supermarkets [29], and by further categorizing stores initially defined by NAICS into independent and chain stores [30]. Beyond the codes, researchers could create further heterogeneity by classifying based on store name. For example, one researcher may include a pizzeria or doughnut shop into their “fast food” category, while another may not. We found thirty-two different food store types/definitions (Appendix 2) in the fifty-one studies we reviewed, a large number that can be partially attributed to these varied classification practices. Consensus on standardized definitions will produce comparative research to advance the field. Ohri-Vachaspati et al. [31] proposed a method for systematically reclassifying commercial database information to make it easier to use for research, however continued research is needed to explore the utility and validity of such methods.
Locating Food Stores
Commercial and public databases used to identify food stores have been reported to be inaccurate and dissimilar [25, 32–36]. For example, when checked by site visit, Dun and Bradstreet measures of CNE had a positive predictive value of 78 %, but a sensitivity of 55 % [37]. Larger discrepancies are often observed when testing the accuracy of public datasets, and internet sources such as the Yellow Pages may be accurate only 50 % of the time [38]. These statistics are alarming considering this review has shown that the majority of studies (41 of 51) used only one measurement tool for locating food stores. As other researchers have noted, future studies should use multiple measurement tools for locating food stores to improve study validity [37, 39].
Analyzing the Community Nutrition Environment
The studies we reviewed used various combinations of counts, densities, ratios, presence and proximity (distance) to measure the CNE. It is unclear which of these methods is preferable and likely depends on the particular research question and the type of store being examined. For example, given the surrounding transportation and land use characteristics, distance might be a more relevant measure for grocery stores while density might be better for fast food. It is also unclear whether density or proximity might be more beneficial for certain populations or geographic areas. Many authors did not justify the method they were using to measure the CNE. Further research should distinguish the differences in effect sizes of density versus distance. Densities measured the number of stores within a certain area, and sometimes included the number of people in that area (density per capita). Other options such as kernel density measure the number of stores in a buffer zone surrounding a central point but then weights these stores differently depending on their spatial relationship to the center point [40]. A better understanding of the constraints and applications of these and other measures will aid the development of new techniques.
Temporal Acquisition of Data
Five studies, although cross-sectional, used exposure (CNE) and outcome (obesity) measures from different time periods [18, 34, 41–43]. For example they may have used current information regarding the obesity status of an area, but used data on store type and location from a different time period. Three of these studies found significant results in the unexpected direction. Future studies should account for changes of the food environment over time as it can change rapidly [44].
Other Considerations
Studies did not always describe every association tested or define the food stores they were examining. Therefore our conclusions regarding the number of positive and negative findings should be interpretably carefully. For each food store type and measurement technique, a study was considered to have a positive or negative finding if just one association was found to be positive or negative; this biased our results to report more positive and negative findings than null results. Although a limitation for conducting a meta-analysis, this did not limit our ability to analyze the varying metrics studies implemented.
Conclusion
Our findings provide additional, updated evidence supporting the association between the CNE and obesity and our review has identified methodological issues for improving research. Although none of the studies used an experimental design, most of the studies we reviewed controlled for myriad factors influencing the relationship between the CNE and obesity. Still, unmeasured components of the CNE and other parts of the food environment such as the “consumer nutrition environment”—which looks at price, promotions, and nutritional quality—are important considerations in determining access to food. These have been studied elsewhere [45–48]. Most studies we examined found an association between the community nutrition environment and obesity despite the heterogeneous metrics, designs, and scopes of the studies. While the volume of research on the effects of the CNE on obesity has expanded, a concerted effort to standardize metrics and methods would increase comparability and certainty in describing this relationship. This would also serve the needs of practitioners in communities, who are increasingly using tools such as the Food Environment Atlas to create local estimates of food access and understand how it may change with certain policies.
References
Flegal, K. M., Carroll, M. D., Ogden, C. L., & Curtin, L. R. (2010). Prevalence and trends in obesity among US adults, 1999–2008. JAMA, the Journal of the American Medical Association, 303(3), 235–241. doi:10.1001/jama.2009.2014.
Ogden, C. L., Carroll, M. D., Kit, B. K., & Flegal, K. M. (2012). Prevalence of obesity and trends in body mass index among US children and adolescents, 1999–2010. JAMA, the Journal of the American Medical Association, 307(5), 483–490. doi:10.1001/jama.2012.40.
Flegal, K. M., Graubard, B. I., Williamson, D. F., & Gail, M. H. (2007). Cause-specific excess deaths associated with underweight, overweight, and obesity. JAMA, the Journal of the American Medical Association, 298(17), 2028–2037. doi:10.1001/jama.298.17.2028.
Nader, P. R., Huang, T. T., Gahagan, S., Kumanyika, S., Hammond, R. A., & Christoffel, K. K. (2012). Next steps in obesity prevention: Altering early life systems to support healthy parents, infants, and toddlers. Childhood Obesity (Print), 8(3), 195–204. doi:10.1089/chi.2012.0004.
Woodman, J., Lorenc, T., Harden, A., & Oakley, A. (2008). Social and environmental interventions to reduce childhood obesity: A systematic map of reviews. London: EPPI-Centre, Social Science Research Unit, Institute of Education, University of London.
Glanz, K., Sallis, J. F., Saelens, B. E., & Frank, L. D. (2005). Healthy nutrition environments: Concepts and measures. American Journal of Health Promotion: AJHP, 19(5), 330–333., ii.
Story, M., Kaphingst, K. M., Robinson-O’Brien, R., & Glanz, K. (2008). Creating healthy food and eating environments: Policy and environmental approaches. Annual Review of Public Health, 29, 253–272. doi:10.1146/annurev.publhealth.29.020907.090926.
Giskes, K., van Lenthe, F., Avendano-Pabon, M., & Brug, J. (2011). A systematic review of environmental factors and obesogenic dietary intakes among adults: Are we getting closer to understanding obesogenic environments? Obesity Reviews: An Official Journal of the International Association for the Study of Obesity, 12(5), e95–e106. doi:10.1111/j.1467-789X.2010.00769.x.
Papas, M. A., Alberg, A. J., Ewing, R., Helzlsouer, K. J., Gary, T. L., & Klassen, A. C. (2007). The built environment and obesity. Epidemiologic Reviews, 29, 129–143. doi:10.1093/epirev/mxm009.
Booth, K. M., Pinkston, M. M., & Poston, W. S. (2005). Obesity and the built environment. Journal of the American Dietetic Association, 105(5 Suppl 1), S110–S117. doi:10.1016/j.jada.2005.02.045.
Feng, J., Glass, T. A., Curriero, F. C., Stewart, W. F., & Schwartz, B. S. (2010). The built environment and obesity: A systematic review of the epidemiologic evidence. Health & Place, 16(2), 175–190. doi:10.1016/j.healthplace.2009.09.008.
Chen, S., Florax, R. J., Snyder, S., & Miller, C. C. (2010). Obesity and access to chain grocers. Economic Geography, 86(4), 431–452.
Centers for Disease Control and Prevention. (2014). Body mass index. http://www.cdc.gov/healthyweight/assessing/bmi/index.html. Accessed 12 Aug 2014.
Janevic, T., Borrell, L. N., Savitz, D. A., Herring, A. H., & Rundle, A. (2010). Neighbourhood food environment and gestational diabetes in New York City. Paediatric and Perinatal Epidemiology, 24(3), 249–254. doi:10.1111/j.1365-3016.2010.01107.x.
Howard, P. H., Fitzpatrick, M., & Fulfrost, B. (2011). Proximity of food retailers to schools and rates of overweight ninth grade students: An ecological study in California. BMC Public Health, 11, 68. doi:10.1186/1471-2458-11-68.
Smoyer-Tomic, K. E., Spence, J. C., Raine, K. D., et al. (2008). The association between neighborhood socioeconomic status and exposure to supermarkets and fast food outlets. Health & Place, 14(4), 740–754. doi:10.1016/j.healthplace.2007.12.001.
Jilcott, S. B., Keyserling, T., Crawford, T., McGuirt, J. T., & Ammerman, A. S. (2011). Examining associations among obesity and per capita farmers’ markets, grocery stores/supermarkets, and supercenters in US counties. Journal of the American Dietetic Association, 111(4), 567–572. doi:10.1016/j.jada.2011.01.010.
Zick, C. D., Smith, K. R., Fan, J. X., Brown, B. B., Yamada, I., & Kowaleski-Jones, L. (2009). Running to the Store? The relationship between neighborhood environments and the risk of obesity. Social Science and Medicine, 69(10), 1493–1500. doi:10.1016/j.socscimed.2009.08.032.
Dean, W. R., Sharkey, J. R., & St John, J. (2011). Pulga (flea market) contributions to the retail food environment of colonias in the South Texas border region. Journal of the American Dietetic Association, 111(5), 705–710. doi:10.1016/j.jada.2011.02.009.
Truong, K., Fernandes, M., An, R., Shier, V., & Sturm, R. (2010). Measuring the physical food environment and its relationship with obesity: Evidence from California. Public Health, 124(2), 115–118. doi:10.1016/j.puhe.2009.12.004.
Bader, M. D., Purciel, M., Yousefzadeh, P., & Neckerman, K. M. (2010). Disparities in neighborhood food environments: Implications of measurement strategies. Economic Geography, 86(4), 409–430.
Laraia, B., Epel, E., & Siega-Riz, A. M. (2013). Food insecurity with past experience of restrained eating is a recipe for increased gestational weight gain. Appetite, 65, 178–184. doi:10.1016/j.appet.2013.01.018.
Oliver, L. N., Schuurman, N., & Hall, A. W. (2007). Comparing circular and network buffers to examine the influence of land use on walking for leisure and errands. International Journal of Health Geographics, 6, 41. doi:10.1186/1476-072x-6-41.
An, R., & Sturm, R. (2012). School and residential neighborhood food environment and diet among California youth. American Journal of Preventive Medicine, 42(2), 129–135. doi:10.1016/j.amepre.2011.10.012.
Moore, L. V., Diez Roux, A. V., Nettleton, J. A., & Jacobs, D. R, Jr. (2008). Associations of the local food environment with diet quality—a comparison of assessments based on surveys and geographic information systems: the multi-ethnic study of atherosclerosis. American Journal of Epidemiology, 167(8), 917–924. doi:10.1093/aje/kwm394.
Forsyth, A., Van Riper, D., Larson, N., Wall, M., & Neumark-Sztainer, D. (2012). Creating a replicable, valid cross-platform buffering technique: The sausage network buffer for measuring food and physical activity built environments. International Journal of Health Geographics, 11, 14. doi:10.1186/1476-072x-11-14.
Mellor, J. M., Dolan, C. B., & Rapoport, R. B. (2010). Child body mass index, obesity, and proximity to fast food restaurants. International Journal of Pediatric Obesity: IJPO: An Official Journal of the International Association for the Study of Obesity,. doi:10.3109/17477161003777433.
Sturm, R. (2008). Disparities in the food environment surrounding US middle and high schools. Public Health, 122(7), 681–690. doi:10.1016/j.puhe.2007.09.004.
Michimi, A., & Wimberly, M. C. (2010). Associations of supermarket accessibility with obesity and fruit and vegetable consumption in the conterminous United States. International Journal of Health Geographics, 9, 49. doi:10.1186/1476-072x-9-49.
Brown, A. F., Vargas, R. B., Ang, A., & Pebley, A. R. (2008). The neighborhood food resource environment and the health of residents with chronic conditions: The food resource environment and the health of residents. Journal of General Internal Medicine, 23(8), 1137–1144. doi:10.1007/s11606-008-0601-5.
Ohri-Vachaspati, P., Martinez, D., Yedidia, M. J., & Petlick, N. (2011). Improving data accuracy of commercial food outlet databases. American Journal of Health Promotion: AJHP, 26(2), 116–122. doi:10.4278/ajhp.100120-QUAN-21.
Oreskovic, N. M., Winickoff, J. P., Kuhlthau, K. A., Romm, D., & Perrin, J. M. (2009). Obesity and the built environment among Massachusetts children. Clin Pediatr (Phila), 48(9), 904–912. doi:10.1177/0009922809336073.
Moore, L. V., & Diez Roux, A. V. (2006). Associations of neighborhood characteristics with the location and type of food stores. American Journal of Public Health, 96(2), 325–331. doi:10.2105/ajph.2004.058040.
Rundle, A., Neckerman, K. M., Freeman, L., et al. (2009). Neighborhood food environment and walkability predict obesity in New York City. Environmental Health Perspectives, 117(3), 442–447. doi:10.1289/ehp.11590.
Sharkey, J. R., & Horel, S. (2008). Neighborhood socioeconomic deprivation and minority composition are associated with better potential spatial access to the ground-truthed food environment in a large rural area. The Journal of Nutrition, 138(3), 620–627.
Paquet, C., Daniel, M., Kestens, Y., Leger, K., & Gauvin, L. (2008). Field validation of listings of food stores and commercial physical activity establishments from secondary data. The International Journal of Behavioral Nutrition and Physical Activity, 5, 58. doi:10.1186/1479-5868-5-58.
Liese, A. D., Colabianchi, N., Lamichhane, A. P., et al. (2010). Validation of 3 food outlet databases: Completeness and geospatial accuracy in rural and urban food environments. American Journal of Epidemiology, 172(11), 1324–1333. doi:10.1093/aje/kwq292.
Lake, A. A., Burgoine, T., Greenhalgh, F., Stamp, E., & Tyrrell, R. (2010). The foodscape: classification and field validation of secondary data sources. Health & Place, 16(4), 666–673. doi:10.1016/j.healthplace.2010.02.004.
Kersten, E., Laraia, B., Kelly, M., Adler, N., & Yen, I. H. (2012). Small food stores and availability of nutritious foods: A comparison of database and in-store measures, Northern California, 2009. Preventing Chronic Disease, 9, E127.
Charreire, H., Casey, R., Salze, P., et al. (2010). Measuring the food environment using geographical information systems: A methodological review. Public Health Nutrients, 13(11), 1773–1785. doi:10.1017/s1368980010000753.
Sanchez, B. N., Sanchez-Vaznaugh, E. V., Uscilka, A., Baek, J., & Zhang, L. (2012). Differential associations between the food environment near schools and childhood overweight across race/ethnicity, gender, and grade. American Journal of Epidemiology, 175(12), 1284–1293. doi:10.1093/aje/kwr454.
Ahern, M., Brown, C., & Dukas, S. (2011). A national study of the association between food environments and county-level health outcomes. The Journal of Rural Health: Official Journal of the American Rural Health Association and the National Rural Health Care Association., 27(4), 367–379. doi:10.1111/j.1748-0361.2011.00378.x.
Morland, K. B., & Evenson, K. R. (2009). Obesity prevalence and the local food environment. Health Place, 15(2), 491–495. doi:10.1016/j.healthplace.2008.09.004.
Cohen, D. A. (2005). Obesity and the built environment: Changes in environmental cues cause energy imbalances. International Journal of Obesity, 2008(32 Suppl 7), S137–S142. doi:10.1038/ijo.2008.250.
Walker, R. E., Keane, C. R., & Burke, J. G. (2010). Disparities and access to healthy food in the United States: A review of food deserts literature. Health & Place, 16(5), 876–884. doi:10.1016/j.healthplace.2010.04.013.
Larson, N. I., Story, M. T., & Nelson, M. C. (2009). Neighborhood environments: Disparities in access to healthy foods in the U.S. American Journal of Preventive Medicine, 36(1), 74–81. doi:10.1016/j.amepre.2008.09.025.
Lovasi, G. S., Hutson, M. A., Guerra, M., & Neckerman, K. M. (2009). Built environments and obesity in disadvantaged populations. Epidemiologic Reviews, 31, 7–20. doi:10.1093/epirev/mxp005.
Gustafson, A., Hankins, S., & Jilcott, S. (2012). Measures of the consumer food store environment: A systematic review of the evidence 2000–2011. Journal of Community Health, 37(4), 897–911. doi:10.1007/s10900-011-9524-x.
Acknowledgments
This research was supported by Cooperative Agreement Number 1-U48-DP001908 from the Centers for Disease Control and Prevention, Prevention Research Centers Program.
Author information
Authors and Affiliations
Corresponding author
Additional information
The findings and conclusions in this review are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Appendices
Appendix 1: Studies Included in the Review, Identification #s
-
1.
Sanchez BN, Sanchez-Vaznaugh EV, Uscilka A, Baek J, Zhang L. Differential associations between the food environment near schools and childhood overweight across race/ethnicity, gender, and grade. American journal of epidemiology. 2012; 175:1284–93.
-
2.
Salois MJ. Obesity and diabetes, the built environment, and the ‘local’ food economy in the United States, 2007. Economics and human biology. 2012; 10:35–42.
-
3.
Lee H. The role of local food availability in explaining obesity risk among young school-aged children. Social science & medicine (1982). 2012; 74:1193–203.
-
4.
Hutchinson PL, Nicholas Bodor J, Swalm CM, Rice JC, Rose D. Neighbourhood food environments and obesity in southeast Louisiana. Health & place. 2012; 18:854–60.
-
5.
Dunn RA, Sharkey JR, Horel S. The effect of fast-food availability on fast-food consumption and obesity among rural residents: an analysis by race/ethnicity. Economics and human biology. 2012; 10:1–13.
-
6.
An R, Sturm R. School and residential neighborhood food environment and diet among California youth. Am J Prev Med. 2012; 42:129–35.
-
7.
Leung CW, Laraia BA, Kelly M, Nickleach D, Adler NE, Kushi LH, et al. The influence of neighborhood food stores on change in young girls’ body mass index. Am J Prev Med. 2011; 41:43–51.
-
8.
Jilcott SB, Wade S, McGuirt JT, Wu Q, Lazorick S, Moore JB. The association between the food environment and weight status among eastern North Carolina youth. Public health nutrition. 2011; 14:1610–7.
-
9.
Jilcott SB, Keyserling T, Crawford T, McGuirt JT, Ammerman AS. Examining associations among obesity and per capita farmers’ markets, grocery stores/supermarkets, and supercenters in US counties. Journal of the American Dietetic Association. 2011; 111:567–72.
-
10.
Howard PH, Fitzpatrick M, Fulfrost B. Proximity of food retailers to schools and rates of overweight ninth grade students: an ecological study in California. BMC public health. 2011; 11:68.
-
11.
Gregson J. Poverty, sprawl, and restaurant types influence body mass index of residents in California counties. Public health reports (Washington, DC: 1974). 2011; 126 Suppl 1:141–9.
-
12.
Gibson DM. The neighborhood food environment and adult weight status: estimates from longitudinal data. American journal of public health. 2011; 101:71–8.
-
13.
Ford PB, Dzewaltowski DA. Neighborhood deprivation, supermarket availability, and BMI in low-income women: a multilevel analysis. Journal of community health. 2011; 36:785–96.
-
14.
Cerin E, Frank LD, Sallis JF, Saelens BE, Conway TL, Chapman JE, et al. From neighborhood design and food options to residents’ weight status. Appetite. 2011; 56:693–703.
-
15.
Block JP, Christakis NA, O’Malley AJ, Subramanian SV. Proximity to food establishments and body mass index in the Framingham Heart Study offspring cohort over 30 years. American journal of epidemiology. 2011; 174:1108–14.
-
16.
Ahern M, Brown C, Dukas S. A national study of the association between food environments and county-level health outcomes. The Journal of rural health: official journal of the American Rural Health Association and the National Rural Health Care Association. 2011; 27:367–79.
-
17.
Truong K, Fernandes M, An R, Shier V, Sturm R. Measuring the physical food environment and its relationship with obesity: evidence from California. Public health. 2010; 124:115–8.
-
18.
Michimi A, Wimberly MC. Associations of supermarket accessibility with obesity and fruit and vegetable consumption in the conterminous United States. International journal of health geographics. 2010; 9:49.
-
19.
Mellor JM, Dolan CB, Rapoport RB. Child body mass index, obesity, and proximity to fast food restaurants. International journal of pediatric obesity: IJPO: an official journal of the International Association for the Study of Obesity. 2010.
-
20.
Laska MN, Hearst MO, Forsyth A, Pasch KE, Lytle L. Neighbourhood food environments: are they associated with adolescent dietary intake, food purchases and weight status? Public health nutrition. 2010; 13:1757–63.
-
21.
Janevic T, Borrell LN, Savitz DA, Herring AH, Rundle A. Neighbourhood food environment and gestational diabetes in New York City. Paediatric and perinatal epidemiology. 2010; 24:249–54.
-
22.
Ford PB, Dzewaltowski DA. Limited supermarket availability is not associated with obesity risk among participants in the Kansas WIC Program. Obesity (Silver Spring, Md). 2010; 18:1944–51.
-
23.
Chen S, Florax RJ, Snyder S, Miller CC. Obesity and access to chain grocers. Economic geography. 2010; 86:431–52.
-
24.
Bodor JN, Rice JC, Farley TA, Swalm CM, Rose D. The association between obesity and urban food environments. Journal of urban health: bulletin of the New York Academy of Medicine. 2010; 87:771–81.
-
25.
Black JL, Macinko J, Dixon LB, Fryer GE, Jr. Neighborhoods and obesity in New York City. Health & place. 2010; 16:489–99.
-
26.
Zick CD, Smith KR, Fan JX, Brown BB, Yamada I, Kowaleski-Jones L. Running to the store? The relationship between neighborhood environments and the risk of obesity. Social science & medicine (1982). 2009; 69:1493–500.
-
27.
Rundle A, Neckerman KM, Freeman L, Lovasi GS, Purciel M, Quinn J, et al. Neighborhood food environment and walkability predict obesity in New York City. Environmental health perspectives. 2009; 117:442–7.
-
28.
Powell LM, Bao Y. Food prices, access to food outlets and child weight. Economics and human biology. 2009; 7:64–72.
-
29.
Oreskovic NM, Winickoff JP, Kuhlthau KA, Romm D, Perrin JM. Obesity and the built environment among Massachusetts children. Clinical pediatrics. 2009; 48:904–12.
-
30.
Oreskovic NM, Kuhlthau KA, Romm D, Perrin JM. Built environment and weight disparities among children in high- and low-income towns. Academic pediatrics. 2009; 9:315–21.
-
31.
Morland KB, Evenson KR. Obesity prevalence and the local food environment. Health & place. 2009; 15:491–5.
-
32.
Li F, Harmer P, Cardinal BJ, Bosworth M, Johnson-Shelton D, Moore JM, et al. Built environment and 1-year change in weight and waist circumference in middle-aged and older adults: Portland Neighborhood Environment and Health Study. American journal of epidemiology. 2009; 169:401–8.
-
33.
Li F, Harmer P, Cardinal BJ, Bosworth M, Johnson-Shelton D. Obesity and the built environment: does the density of neighborhood fast-food outlets matter? American journal of health promotion: AJHP. 2009; 23:203–9.
-
34.
Inagami S, Cohen DA, Brown AF, Asch SM. Body mass index, neighborhood fast food and restaurant concentration, and car ownership. Journal of urban health: bulletin of the New York Academy of Medicine. 2009; 86:683–95.
-
35.
Galvez MP, Hong L, Choi E, Liao L, Godbold J, Brenner B. Childhood obesity and neighborhood food-store availability in an inner-city community. Academic pediatrics. 2009; 9:339–43.
-
36.
Davis B, Carpenter C. Proximity of fast-food restaurants to schools and adolescent obesity. American journal of public health. 2009; 99:505–10.
-
37.
Currie J DS, Moretti E, et al. Do fast food restaurants contribute to obesity? National Bureau of Economic Research bulletin on aging and health. 2009:2–3.
-
38.
Mehta NK, Chang VW. Weight status and restaurant availability a multilevel analysis. Am J Prev Med. 2008; 34:127–33.
-
39.
Li F, Harmer PA, Cardinal BJ, Bosworth M, Acock A, Johnson-Shelton D, et al. Built environment, adiposity, and physical activity in adults aged 50–75. Am J Prev Med. 2008; 35:38–46.
-
40.
Grafova IB. Overweight children: assessing the contribution of the built environment. Preventive medicine. 2008; 47:304–8.
-
41.
Brown AF, Vargas RB, Ang A, Pebley AR. The neighborhood food resource environment and the health of residents with chronic conditions: the food resource environment and the health of residents. Journal of general internal medicine. 2008; 23:1137–44.
-
42.
Wang MC, Kim S, Gonzalez AA, MacLeod KE, Winkleby MA. Socioeconomic and food-related physical characteristics of the neighbourhood environment are associated with body mass index. Journal of epidemiology and community health. 2007; 61:491–8.
-
43.
Powell LM, Auld MC, Chaloupka FJ, O’Malley PM, Johnston LD. Associations between access to food stores and adolescent body mass index. Am J Prev Med. 2007; 33:S301–7.
-
44.
Lopez RP. Neighborhood risk factors for obesity. Obesity (Silver Spring, Md). 2007; 15:2111–9.
-
45.
Liu GC, Wilson JS, Qi R, Ying J. Green neighborhoods, food retail and childhood overweight: differences by population density. American journal of health promotion: AJHP. 2007; 21:317–25.
-
46.
Morland K, Diez Roux AV, Wing S. Supermarkets, other food stores, and obesity: the atherosclerosis risk in communities study. Am J Prev Med. 2006; 30:333–9.
-
47.
Jeffery RW, Baxter J, McGuire M, Linde J. Are fast food restaurants an environmental risk factor for obesity? The international journal of behavioral nutrition and physical activity. 2006; 3:2.
-
48.
Sturm R, Datar A. Body mass index in elementary school children, metropolitan area food prices and food outlet density. Public health. 2005; 119:1059–68.
-
49.
Maddock J. The relationship between obesity and the prevalence of fast food restaurants: state-level analysis. American journal of health promotion: AJHP. 2004; 19:137–43.
-
50.
Chou SY, Grossman M, Saffer H. An economic analysis of adult obesity: results from the Behavioral Risk Factor Surveillance System. Journal of health economics. 2004; 23:565–87.
-
51.
Burdette HL, Whitaker RC. Neighborhood playgrounds, fast food restaurants, and crime: relationships to overweight in low-income preschool children. Preventive medicine. 2004; 38:57–63.
Appendix 2: Food Store Descriptions
1. Beverage and snack foods |
2. Chain grocer |
3. Chain restaurant |
4. Convenience store |
5. Direct farm sales |
6. Drug store |
7. Emergency food providers |
8. Ethnic food store |
9. Ethnic supermarket |
10. Farmer’s market |
11. Fast food restaurant |
12. Food retail of any type |
13. Full-service restaurant |
14. Grocery store |
15. Healthy BMI store |
16. Healthy food places |
17. Healthy grocery store |
18. Independent restaurant |
19. Independently owned grocery store |
20. Independent supermarket |
21. Intermediate BMI store |
22. Limited service restaurant |
23. Non fast food restaurant |
24. Restaurant total |
25. Sit down restaurant |
26. Small food store/grocery store |
27. Specialty store |
28. Supercenter |
29. Supermarket |
30. Supermarkets and produce vendors |
31. Unhealthy BMI store |
32. Unhealthy food places |
Rights and permissions
About this article

Cite this article
Gamba, R.J., Schuchter, J., Rutt, C. et al. Measuring the Food Environment and its Effects on Obesity in the United States: A Systematic Review of Methods and Results. J Community Health 40, 464–475 (2015). https://doi.org/10.1007/s10900-014-9958-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10900-014-9958-z