
Abstract
This study investigated adolescents’ single and co-occurring developmental patterns of gambling participation and substance use and their association with gambling and substance use-related issues at age 17, controlling for confounders. Multiple assessments from age 12 to 17 were conducted in a population-based cohort (N=1594, 51.2% boys). Latent growth modeling was used to analyze developmental patterns and Generalized linear models to examine their association with age-17 gambling and substance use-related problems, types and variety of activities, and substance abuse. Results revealed six developmental patterns, including Low- or Non-substance Users or Gamblers (24.2% sample), two trajectory-classes of Later-Onset Increasing (to a moderate level) substance users, either with or without gambling participation (7.8% and 45.5%, respectively), two trajectory-classes of Early-Onset Increasing (to a higher level) substance users, either with or without gambling participation (6.2% and 12.7%, respectively), and a smaller trajectory-class of Slow-Increasing Substance Users and Early-Onset Gamblers, declining to non-gambling after age 13 (3.6%). Gambling participation and substance use did not appear to influence each other with regard to their onset and course throughout adolescence, and to age-17 types and variety of gambling activities or substances used, problems related to gambling participation or substance use, or substance abuse. These findings are consistent with the addictive syndrome model and with both common and individualized approaches to prevention and treatment for adolescent gamblers or substance users.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
With the publication of the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; APA, 2013), gambling disorder has been recategorized into the “Substance-related and Addictive Disorders” section. This change followed cumulating reports showing the association between gambling and substance use in clinical and community samples (Barnes et al., 2009; 2011; Grant & Chamberlain, 2020; Kessler et al., 2008; Petry, Stinson, & Grant, 2005). It was also motivated by the discovery of the considerable similarity between gambling and substance use disorders in regard to diagnostic criteria (e.g., tolerance, loss of control, withdrawal; Rash, Weinstock, & Van Patten, 2016; Wareham & Potenza, 2010), genetic underpinnings (Slutske et al., 2013; Vitaro et al., 2014; 2019; Xian et al., 2014), neurobiological vulnerabilities (Potenza, 2008; 2017), and co-occurrent problems (e.g., impaired social relations or school/work performance, psychological or economic difficulties, delinquency; Allami et al., 2018; Lorains et al., 2011; Loo, Kraus & Potenza, 2019; Petry et al., 2005, Wanner et al., 2009). Gambling participation and substance use in adolescence, both precursors of corresponding adult behaviors and their related problems (Carbonneau et al., 2015a; 2015b; Moss, Chen & Yi, 2014; Winters & Stinchfield, 2012), have also been shown to be associated (Barnes et al., 2011; Peters et al., 2015; Wanner et al., 2006).
Conceptually, these reports are consistent with the syndrome model of addiction (Shaffer et al., 2004). This model posits that shared neurobiological, psychological and social risk factors influence the development and maintenance of different manifestations of addiction. According to this model, gambling and substance use disorders are thus both the expression of the same underlying syndrome. From a developmental standpoint, understanding the association between gambling and substance use disorders requires a longitudinal perspective and knowledge of the different patterns of gambling participation and substance use, starting from their early manifestations and co-occurence (Cicchetti & Rogosh, 2018).
Studies that examined the longitudinal association between the two behaviors have shown mixed results. In adults, most studies investigating the link between previous substance use and later gambling participation or related problems reported either a positive association (Afifi & al., 2016; Dowling, Aarsman & Merkouris, 2021; Edgerton et al., 2015; Jun et al., 2021), no relation (Dowling et al., 2019), or a negative link where substance use level was associated with subsequent lowered gambling activity (Black et al., 2021). Of the two studies examining the link between earlier gambling participation and later substance use, one reported a positive association (Afifi & al., 2016) and the other no association (Dowling et al., 2019). Similarly ambiguous results have been found in studies examining the link between adolescent substance use and adult gambling participation, which have either shown a positive association (Merkouris et al., 2021; Vitaro et al., 2019; Werner et al., 2020) or no association (Wanner et al., 2009). Studies that examined how adolescent gambling related to adult substance use also reported either a positive (Werner et al., 2020) or no association (Vitaro et al., 2019). Finally, only one study, to our knowledge, examined possible transactional links between the two behaviors in boys, from age 16 to 17 (Vitaro et al., 2001). Results showed that substance use predicted an increase in gambling participation, but no association between earlier gambling and later substance use was found.
The mixed nature of the above findings precludes a definite conclusion. However, the reported studies were based on two times of assessment only, which limits the possibility of capturing developmental processes. To our knowledge, two studies used multiple assessment times to investigate the joint development of substance use and gambling participation. Mutti-Packer and colleagues (2017) used parallel-process latent growth curves to examine the temporal associations between alcohol misuse and problem gambling from adolescence to young adulthood. Their results first showed that baseline levels of both behaviors were associated, as were higher baseline levels of alcohol misuse and a steeper decline in problem gambling over time. However, these associations were no longer significant after including covariates (sex, household income, and other substances used) in the model. Therefore, the authors concluded that one behavior was not a risk factor for the other. Of note, the authors reported significant variability in baseline levels (for alcohol) and growth over time, suggesting heterogeneity within the sample. In the second study, Wanner and colleagues (2006) compared the latent trajectory-classes of gambling participation in low SES boys and trajectory-classes of alcohol and marijuana consumption based on annual measurements from age 11 to 16. Their results showed that the majority of adolescent-users and gamblers followed a similar trajectory for both behaviors. Indeed, 52.8% of early-onset gamblers also showed an early-onset of substance use, compared to 31.9% of late-onset gamblers. Similarly, 57.5% of late-onset gamblers also showed a late-onset for substance use compared to 36.4% of their early-onset gambler peers.
Thus, overall, there is some evidence of a temporal association between gambling participation and substance use. However, this relation is not always found, and the bidirectionality of this association has received less support than a unidirectional association linking earlier substance use to later gambling participation. There is also some evidence for a parallel process between the two behaviors. However, most of the extant studies are limited to two assessment times and by the use of mostly adult measures. Indeed, only Wanner and colleagues (2006) included multiple assessment points from age 11 through age 16. However, they used a single binary item for both gamling (i.e., gambled or not) and substance use (i.e., used or not), which limited the assessment of co-variation. The authors also examined jointly the two types of behaviors using the separate estimations of their respective trajectory-classes rather than estimating their joint course within the same analysis. The at-risk nature of the sample of urban low SES boys further limited the generalization of results. Thus, despite the importance of this period for the onset of both addictive behaviors, the development of gambling participation and substance use and their co-occurrence in pre- to late adolescence remains unclear.
Furthermore, it is unknown whether this co-occurrence is linked to a higher likelihood for adolescents to experience problems related to gambling or substance use. If both behaviors stem from the same underlying syndrome and develop in parallel (Mutti-Packer et al., 2017), adolescents involved in both types of behaviors should not experience more problems than youth involved in only one type. However, if the two types of behavior combine either additively, interactively or transactionnally, individuals showing both gambling participation and substance use could experience more problems related to each behavior than their peers who solely gamble or use substances at a comparable level. Similarly, there is no evidence of how the characteristics (e.g., frequency, variety, and types) of gambling participation or substance use may be linked to their co-occurrence in adolescence, despite evidence of the importance of these characteristics for the severity of each addictive behavior and their related problems in adolescents (Felton et al., 2015; Welte et al., 2009) and adults (Carbonneau et al., 2015a; Lynne-Landsman, Bradshaw & Ialongo, 2010; Moss et al., 2014; Williams et al., 2021). If gambling participation and substance use mutually influence or exacerbate each other, then the characteristics of each behavior may contribute to their co-occurrence in adolescents.
The Present Study
The present study aimed to fill the above gaps by examining the course of gambling participation and substance use across the ages of 12, 13, 15 and 17, in a population birth cohort. Specifically, using a method integrating variable- and person- centered approaches, the trajectories of gambling participation and substance use (i.e., their single or co-occurrence over time) were investigated. This method is especially suitable to determine longitudinal patterns of gambling participation or substance use as well as their related characteristics (Carbonneau et al., 2021; 2015b; Feldman et al., 2009). In particular, in the presence of heterogeneity within a sample, the method allows testing whether a model including latent classes of individuals provides a better fit to the longitudinal data than an initial (one-class) model based on growth curve parameters for the whole sample (Kandauda et al., 2016). This particularity is important given evidence that both adolescent and adult gamblers are heterogeneous groups with regard to the development of gambling behavior and substance use, and with regard to their related problems (Black et al., 2021; Gupta et al. 2013; Kurilla, 2021; Martínez‑Loredo et al., 2019; Nower et al. 2013).
Second, trajectories of gambling participation and substance use were examined in association with gambling and substance use variety, types of activities or substances used, and related problems (e.g., social and functional difficulties; Allami et al., 2018; Derevensky, 2015; Loo et al., 2019; Lorains et al., 2011). Given their well-established association with both gambling (Goudriaan et al., 2009) and substance use (Swendsen et al., 2009), participants’ sex, family adversity and SES were used as control variables. Based on evidence from previous studies of adolescents and young adults, we expected: (1) trajectories of low gamblers and low substance users, trajectories of increasing or frequent gamblers or substance users, and a trajectory of increasing or frequent co-occuring behaviors; (2) a similar temporal pattern as that observed in adults for distinct trajectory-classes, where earlier gambling precedes subsequent substance use, or vice-versa; (3) associations between higher trajectories of each behavior, on the one hand, and on the other hand, their respective variety, types of activities or substances used, and related problems at age 17; (4) a link between co-occurrence of both behaviors and the variety of activities or likelihood of experiencing related problems; and finally, (5) a higher prevalence of males in trajectory-classes reflecting a higher level of activity or co-occurrent gambling participation and substance use.
Methods
Participants
Participants came from a birth cohort of 2226 infants (92% White of European ancestry, 51.2% boys) representative of the children born (single births) in the province of Quebec, Canada, in 1997–1998 (see Orri et al., 2021, for additional details). All mothers giving birth after 24 weeks’ and not later than 42 weeks’ gestation who spoke English or French (Canada’s official languages) were eligible. The study design was reviewed and ethical approval of all aspects of the study was provided by the Quebec Institute of Statistics Institutional Review Board. Children were assessed with their family for the first time 5 months after birth.
Trajectories of gambling participation and substance use were based on adolescent self-reports at ages 12, 13, 15, and 17 years. The growth-mixture method used (Muthen & Muthen, 1998–2017) accommodates missing data, as participants with incomplete assessments across repeated measures can be included and all available values are used for the trajectory estimation. The sample with at least some valid gambling and substance use data (N=1594) was compared to the children for whom no data was available during the times of interest (N=632; 28.4% cohort) with respect to age 5 months socio-demographic variables: maternal age at birth of first child, paternal age at birth of target child, parental education, family income and status (i.e., intact or not), child gender and number of siblings. Small (Cohen, 1988; Sawilowsky, 2009) but significant differences were observed, with lower maternal (Cohen’s h=0.11) and paternal (h=0.13) education, lower family income (Cohen’s d=0.21), and more boys (h=0.20) in lost participants. To compensate for differential attrition, inverse probability weighting was applied in the trajectory analyses (Thompson & Arah, 2014). Specifically, using a logistic regression model, the probability was estimated that a participant would have valid data on addictive behaviors between 12 and 17 years based on the variables showing baseline differences between participants and lost subjects. The observations used in the study were then weighted by the inverse of the estimated probability. Analyses that are weighted for the inverse probability of attrition have been shown to reduce bias resulting from differential attrition in longitudinal studies (Thompson & Arah, 2014).
The characteristics examined in relation to gambling participation or substance use in the present study were measured at age 17 years and were available for 1253 (78.6%) participants. The same procedure as above was used to compare adolescents with and without age-17 data among those with valid trajectory data. Small but significant differences were observed, with younger motherhood (d=0.15), lower maternal (h=0.31) and paternal (h=0.24) education, lower family income (d=0.34), more boys (h=0.25), and a higher likelihood of parental separation (h=0.15) in lost participants. To compensate for differential attrition, inverse probability weighting was applied in the analyses involving age 17 characteristics.
Measures
Gambling participation. Participation in gambling activities was assessed at ages 12, 13 15 and 17 years with the South Oaks Gambling Screen for adolescents (SOGS-RA; Winters, Stinchfield & Fulkerson, 1993). Participants indicated how often they had engaged in 12 gambling activities over the past 12 months (e.g., purchased lottery tickets, played online sports betting games, bought scratch offs, played bingo for money, bet on games on the internet, played video lottery terminal games, played cards or games with others for money, bet on sporting events/games for money, gambled at a casino, bet on games of skill (pool, basketball), played dice games for money, and bet on other games). Participants rated the frequency of each activity on a scale ranging from 0 (never) to 6 (daily). At each time point, item scores were summed (average α: 0.80). Distribution and reliability statistics for gambling participation at each assessment time are shown in Table 1.
Substance use. Frequency of substance use over the past year of alcohol, marijuana and other illicit drugs was assessed using adolescents’ annual self-reports at ages 12, 13, 15, and 17 years. The following three items from the Personal Experience Screening Questionnaire (Henly & Winters, 1989; Winters et al., 1990) were used: “In the last 12 months: How many times did you use alcohol? How many times did you use marijuana? How many times did you use other illicit drugs like cocaine, stimulants, speed, amphetamine, tranquilizers, inhalants, heroin, opiates, hallucinogens, psychedelics, or other narcotics or hard drugs?” Each item was coded on a scale ranging from 0 (never) to 6 (daily). Substance use was computed by summing the three item scores (average α: 0.72). Distribution and reliability statistics for substance use at each assessment time are shown in Table 1.
Problems related to gambling at age 17 were assessed with the SOGS-RA in reference to the last 12 months, based on the following 12 items: “Try to win back money you have lost, claim to be winning money gambling but were not, feel you have a problem with gambling, gamble more than you intended to, have been criticized for your betting or told you had a problem, feel guilty about the way you gamble, feel like you would like to stop gambling but do not think that you could, hide signs of betting or gambling from people in your life, have money arguments centered on your gambling, have borrowed from someone and not paid them back as a result of your gambling, have lost time from work or school due to gambling, have borrowed money to gamble or to pay gambling debts”. Coded yes or no (1, 0), the items were summed up, resulting in a 12-point scale of gambling-related problems (Ordinal α: 0.81). Based on the SOGS-RA score sheet, a score of 1 or 2 indicates some problems with gambling, and a score of 3 or more suggests probable problem gambling (Winters et al., 1993). Using these criteria, 1.6% of participants at age 17 could be classified as having some problems related to gambling and 0.6% as probable problem gamblers. Because of the small number of participants reporting gambling-related problems, both categories were collapsed to represent problem gambling (i.e. gamblers with one or more problems).
Problems related to substance use at age 17 were based on the following items reported by participants as related to their use: psychological difficulties, harmed family relationships, harmed friendships or romantic relationships, school problems, committing an act of delinquency, feeling that the same amounts have less effect, and consulting regarding own substance use. Each item referred to the last 12 months and was coded yes-no (0,1). Summing all items resulted in a 0 to 7-point scale (Ordinal α: 0.83).
Variety of gambling activities at age 17 was calculated by summing the different types of gambling activities a participant had engaged in over the past 12 months, based on the activities listed above in regard to gambling participation, resulting in a 12-point scale (Ordinal α: 0.81). Similarly, the Variety of substances used was calculated by summing the different types of substances a participant had used over the past 12 months, resulting in an 7-point scale (Ordinal α: 0.70). Finally, to obtain an indicator of substance abuse, the participants were asked how many times they had 5 drinks or more on the same occasion over the past year. Sample descriptives with regard to the characteristics (i.e., problems and variety) of gambling participation and substance use at age 17 are shown in Table 4.
Control variables. Participant’s sex, family adversity and SES when participants were 12 years old were used as control variables. Family adversity was based on maternal age at the birth of her first child, maternal and paternal age at the birth of the target child, number of siblings, and family structure (coded as “intact: living with both biological parents” or “non-intact: not living with both biological parents”). Using these baseline socio-demographic indices (Table 2), a value at or below the sample’s 30th percentile for age variables, above the 70th percentile for number of siblings, or a positive code for non-intact family, was coded as one adversity point. The resulting indicators were averaged to obtain a parental adversity index ranging from 0 to 1. Household SES was based on parents’ occupational prestige score, education level, and income (Statistics Canada, 1995).
Data Analysis
Latent Class Growth Mixture Modeling (LCGMM) in Mplus/version-8.6 (Muthen & Muthen, 1998–2017), which integrates variable- and person-centered analyses, was first used to investigate—separately—adolescents’ course of gambling participation and substance use. This method is based on the estimation of participants’ individual growth curves (i.e., individuals’ level and growth in behavior over time). Variability across individuals is estimated as the variance of the latent intercept and slope. In the presence of significant heterogeneity within the sample, LCGMM allows to test whether a better fit would be obtained with the estimation of distinct latent classes of individuals showing similar level and growth across time (i.e., with different intercept or slopes between classes). The LCGMM procedure employs full information maximum likelihood estimation to handle missing data and was conducted in accordance with the recommended guidelines (Kandauda et al., 2016; Van de Schoot et al., 2017). Model-fit was determined by (Table 3): (1) Information criteria statistics; (2) Likelihood Ratio Test (LRT) and adjusted-LRT, given the use of weight for selective attrition, to identify the optimal number of classes; and (3) two indicators of classification: Entropy, which indexes class separation, and the Average Probabilities of Assignment (APA) of individuals in trajectory-classes (satisfactory when ≥ 0.70) (Nagin, 2005). Additionally, we considered whether enough participants were present in each trajectory-class to perform later joint-trajectory analysis and joint trajectory-class comparison with adequate statistical power.
As expected, data on gambling participation and substance use were highly skewed (Table 1), with a large proportion of individuals in the non/low-user category. Considering this distribution and the ordinal nature of the measures, we used the ordered logit-link model as recommended for modeling longitudinal trajectories with such data (Feldman et al., 2009). Growth parameter estimates of the best fitting models for gambling participation and substance use were used as basis for the joint-trajectory procedure. Joint-trajectory modeling estimates joint and conditional probabilities across the combination of each behavior’s trajectories and describes their co-occurrence throughout adolescence. A similar model testing procedure as for single-behavior analysis is used for assessing model-fit and individuals’ assignment to joint trajectory-classes. To account for uncertainty in the classification to trajectory-classes, probabilities of assignment (i.e., individual variation) were used as sampling weights in further analyses (Clark & Muthen, 2009; Nagin, 2005).
Next, adolescent joint-trajectories of gambling participation and substance use were compared on gambling and substance use-related characteristics, controlling for confounders. First, consistent with previous trajectory-studies of adolescent gambling and substance use, the lowest (i.e., non- or low- gamblers and users among the sample throughout the adolescence period) were used as reference class, which was successively compared to each of the other user-classes. Second, the gamblers’ and substance users’ classes were compared with each other. Generalized Linear Models (hereafter: GLM) were used to compare trajectory-classes on age-17 characteristics. GLM provide a unified approach for all types of response variables, including Normal, Poisson, and Binomial distributions (Hardin & Hilbe, 2018), thus allowing a consistent method of analysis across outcome variables with different distributions. Holm-Bonferroni correction was used in the analyses to compensate for multiple comparisons.
Results
Model of Joint Gambling Participation and Substance use From Age 12 to 17
For both gambling participation and substance use, significant variance in intercept, linear and quadratic slopes, as well as covariance between these parameters suggested sample heterogeneity in regard to initial level and course of each behavior. This justifies extending analyses to test whether a better fit would be obtained with the estimation of latent classes of adolescents showing similar level and growth. One through four-class models were tested before obtaining the best-fitting model. The best solution in both cases was an ordered logit-link based, LCGA 3-class quadratic model, with a fixed variance-covariance matrix structure across classes. For gambling participation, the 3-class model had a better fit than a 2-class solution, whereas a 4-class model did not provide a significant improvement, nor did alternative models based on a linear parameterization, Zip distribution, or relaxing equality constraints within (GMM) or between classes. For substance use, the 4-class solution showed better fit indices than the 3-class model and alternative models again did not provide a better fit. However, the 4-class solution implied an additional trajectory-class of only 19 individuals, which essentially split one of the classes in the 3-class model based on a difference in scores for the first two of the five assessment times. Because this low number of members was not sufficient to include this class with adequate statistical power in the subsequent analyses, the 3-class model was selected. Of note, Entropy (0.76 vs. 0.78) and APA (0.87 vs. 0.84) were similar for the 3- and 4-class solutions. The estimated growth parameters of the above models were then used for joint-trajectory analysis of gambling participation and substance use (i.e., 3 × 3 classes). Results of the Vuong-Lo-Mendell-Rubin Likelihood Ratio Test (VLMR-LRT; p = 0.0926) and Lo-Mendell-Rubin Adjusted Likelihood Ratio Test (LMR-ALRT; p = 0.0955) for 9 versus 8-class models, as well as for 8 versus 7-class models (VLMR-LRT; p = 0.0751; LMR-ALRT; p = 0.0777) and 7 versus 6-class models (VLMR-LRT; p = 0.2680; LMR-ALRT; p = 0.2758) indicated a non-significant improvement in fit between the respective models. However, the 6-class model showed a better fit than the 5-class model (VLMR-LRT; p = 0.0217; LMR-ALRT; p = 0.0238) and was selected for further analysis (Table 3). Of note, because model testing for joint-trajectory analysis was conducted from the top down, comparisons between models with a lower number of classes (i.e., 5 vs. 4; 4 vs. 3; 3 vs. 2; 2 vs. 1) were also performed and were all significant (p < 0.01 for both VLMR-LRT and LMR-ALRT) confirming the 6-class model as the best-fitting model.
Developmental Patterns of Gambling Participation and Substance Use
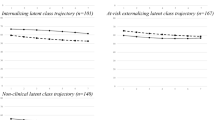
The six trajectory-classes of the final model (Fig. 1) were as follows. The first class (1) included Low- or Non-substance users or gamblers across adolescence (N=386, 24.2% sample). Adolescents of the second class (2) showed a pattern of Later-onset increasing substance users & Low- or Non-gamblers (N=725, 45.5%), starting essentially after age 13. A third class (3) included Slow-increasing substance users & Early-onset declining gamblers (N=58, 3.6%). Members of this class already reported gambling activities at age 12, which increased to age 13, but had practically quit gambling by age 15 while maintaining a low increasing level of substance use. The fourth class (4) followed a trajectory of Later-onset increasing substance users & gamblers (N=125, 7.8%) with a similar increase of both activities from age 13 onwards. The fifth class (5) showed a pattern of Early-onset increasing substance users & Low- or Non-gamblers (N=202, 12.7%). Finally, the sixth class (6) included Early-onset increasing substance users & Stable gamblers (N=98, 6.2%) who maintained a moderate level of gambling from age 12 to 17 (n.b., across-time differences on gambling: Cohen’s d=0.12, p = 0.25 for age 12-13; d=0.08, p = 0.54 for 13-15; and d=0.27 p = 0.09 for 15-17). Thus, overall, 18.8% of adolescents were part of joint trajectory-classes (i.e., 5 and 6) that involved an earlier onset of substance use and an increasing, more frequent use than their peers across adolescence. Two trajectory-classes (i.e., 4 and 6), representing 13.9% of the sample, showed a significant level of gambling participation at ages 15 and 17. Finally, boys were overrepresented in the Early-onset increasing substance users & Stable gamblers, and in the Later-onset increasing substance users trajectory-classes with or without gambling participation.

Joint trajectory-classes of gambling participation and substance use from age 12 to 17 years (N=1594). Substance users (SU). 1: Percentage sample, Girls, Boys. *: Sex difference in comparison to the reference class at p < 0.05
Characteristics of Gambling Participation and Substance Use at Age 17
Results on the association between trajectory-classes of gambling participation and substance use and their respective variety and problems, and substance abuse at age 17 (controlling for confounders) are shown in Table 4. Adolescents in the two trajectory-classes showing higher gambling participation at age 17 were more likely to report at least one gambling-related problem over the last year than youth in the reference class of Low- or Non-substance users or gamblers and any of the other trajectory-classes. However, members of these two classes did not differ from each other in post-hoc analysis (p = 0.83). Of note, based on the SOGS-RA score sheet, 9.9% of gamblers at age 17 had some gambling-related problems and 3.3% were probable problem gamblers. Later-onset increasing gamblers (class 4) and Stable gamblers (class 6) reported a higher variety of gambling activities in comparison to their peers in any of the other classes. Later-onset increasing gamblers also showed a higher gambling variety than Stable gamblers (p <0.001, Cohen’s d = 0.38). The top 3 favorite types of game played by Later-onset increasing gamblers were, respectively, playing cards (M: 0.74; SD:1.40), scratch cards (0.73; 1.25), and betting on sports events (0.55; 1.38), whereas Stable gamblers’ favorites were scratch cards (0.50; 1.09), playing cards (0.47; 0.92), and playing dices (0.33; 0.79). Finally, Later-onset increasing and Stable gamblers differed significantly in regard to the frequency of playing on internet (M = 0.43 (1.35) & 0.05 (0.28), p<0.001; d = 0.47), betting on sports (M = 0.55 (1.38) & 0.15 (0.57), p=0.007; d = 0.41) and buying lottery tickets (M = 0.33 (1.04) & 0.06 (0.34), p=0.016; d = 0.39).
Regarding age-17 indicators related to substance use, members of all trajectory-classes of users but the Slow-increasing substance users & Early-onset declining gamblers (possibly for lack of statistical power) were more likely to report at least one substance use-related problem compared to their peers from the reference class. All trajectory-classes of users also showed, on average, a higher variety of substances used, and a higher frequency of abuse (i.e., having 5 drinks or more on the same occasion) in comparison to the reference class. Results of post-hoc analyses showed that the Early-onset increasing substance users with (class 6) or without (class 5) gambling participation did not differ on the above three indicators (p > 0.13). However, Early-onset increasing substance users & Stable gamblers were more likely to report substance use-related problems (p < 0.001, Cohen’s h = 0.73), and on average, used a greater variety of substances (p < 0.001, d = 1.02) and had a higher frequency of abuse episodes (p = 0.016, d = 0.35) than the Later-onset increasing substance users & gamblers (class 4). Later-onset increasing substance users with (class 4) or without (class 2) gambling participation showed similar results for the three substance use indicators at age 17 (Table 3). However, regarding the types of substances used, the former reported a higher use of other illicit drugs than the latter (p = 0.001, d = 0.24). As for Early-onset increasing substance users, low or non-gamblers (class 5) reported a higher marijuana use (p = 0.025, d = 0.27) than their Stable gamblers peers (class 6).
Discussion
The present study aimed to (a) identify developmental patterns of single and co-occurring gambling participation and substance use in a population-based cohort from age 12 to 17, and (b) examine their association with gambling and substance use-related issues by age 17, controlling for confounders. As expected, latent growth curve models revealed significant individual differences in initial level and growth throughout adolescence for both types of behaviors (Martínez‑Loredo et al., 2019; Mutti-Packer et al., 2017). The latent class models that followed resulted in six trajectory-classes describing the single or co-occurrent courses of gambling participation and substance use in the adolescent sample. Alongside a class of Low- or Non-substance users or gamblers, the four main trajectory-classes of adolescents consisted of either Later-onset increasing (to a moderate level) or Early-onset increasing (to a higher level) substance users, with or without gambling participation. While Later-onset gamblers showed an increasing course similar to their use of substances, their Early-onset peers were already gambling at age 12 (suggesting an even earlier onset) and maintained a similar level of gambling participation up to age 17. However, by age 17, Later-onset increasing users reached a level of gambling participation more than twice that of their early-onset peers. The smallest trajectory-class—including 58 participants with slow-increasing substance use—had also started gambling by age 12 and showed a similar level to early onset-users and gamblers at age 13 before declining to essentially non-gambling thereafter. Consistent with prior reports (Buja et al., 2017), there was no trajectory-class of adolescents who gambled but did not use substances across the age 12 to 17 period. Also in line with previous research (Barnes et al., 2009), a substantial level of activity was observed earlier for gambling than for substance use. Finally, as expected, boys were overrepresented in the Early-onset and Later-onset increasing substance users trajectory-classes that also included a higher level of gambling participation (e.g., Martínez‑Loredo et al., 2019).
Thus, overall, the trajectories of substance use were similar for gamblers and non-gamblers, which could suggest that the development of each addictive behavior does not depend on the development of the other during this age-period. These findings differ from those of prior studies that investigated the link between gambling and substance use across two assessment times (e.g., Afifi et al., 2016; Merkouris et al., 2021; Vitaro et al., 2001; 2019). However, the results are consistent with those of other reports using adults (Dowling et al., 2019), or investigating youths in their transition from adolescence to young adulthood (Mutti-Packer et al., 2017; Wanner et al., 2009), suggesting that one behavior is not a risk factor for the other. Notably, the present findings are also consistent with the two studies that used multiple assessment times and focussed partly or entirely on the adolescence period (Mutti-Packer et al., 2017; Wanner et al., 2006). While Wanner and colleagues reported similar trajectory patterns for gambling and substance use, Mutti-Packer and collaborators found no associations between the initial levels or slopes of the two behaviors after including covariates.
The apparent similarities and discrepancies across studies (including the present one) may in fact be coherent with the syndrome model of addiction (Shaffer et al., 2004). Indeed, the two behaviors may be linked through a common genetic basis (Slutske et al., 2013; Vitaro et al., 2019) and risk factors (Lorains et al., 2011; Mutti-Packer et al., 2017; Vitaro et al., 2001), but without affecting each other, thus developing in parallel (Mutti-Packer et al., 2017). The emergence of gambling or substance use—or of both behaviors—as well as their respective onset may be due to the timing and level of individuals’ exposure to each of these objects of addiction. This exposure may provide different opportunities for the expression of the underlying syndrome (Shaffer et al., 2004). This may include the availability, accessibility, as well as a positive or tolerant attitude toward one activity or the other in a youth’s environment (Grant & Chamberlain, 2020). Hence, exposure can vary over time, which may lead to the substitution of one addictive behavior for another. For instance, a higher prevalence of gambling than substance use has been reported in early teens, possibly because some parents consider their children’s gambling as a harmless activity (Barnes et al., 2009). Moreover, playing cards or dice with peers may be more accessible or less worrying than using substances for these young adolescents. However, this activity may shift—at least partly—to substance use later in adolescence. This seems to be the case in the smallest trajectory-class of this study around mid-adolescence. It is also possible that the change in landscape in regard to the variety and appeal of gambling opportunities for older adolescents (or young adults) triggers new behaviors in individuals already prone to addictive behaviors like substance use. Further research including valid measures of exposure over time are needed to clarify the role of exposure in the evolving expression of gambling participation and substance use in adolescence (Shaffer et al., 2004).
The two trajectory-classes with higher gambling participation showed some similarities and differences in regard to their association with gambling characteristics at age 17. As expected, adolescents of these two trajectory-classes reported a higher variety of gambling activities compared to those in the reference class or in other classes of users or gamblers. Similarly, adolescents in both trajectory-classes with higher gambling participation reported more gambling-related problems at age 17 than all the other trajectory-classes, but they did not differ from each other in this regard. Of note, controlling for trajectory-classes and other confounders, boys were 10 times more likely to experience gambling-related problems, a finding consistently reported for adolescents (Derevensky, 2015; Vitaro et al., 2004). Since problem gambling in adolescence has been shown to increase the likelihood of experiencing similar problems in adulthood (Carbonneau et al., 2015a, b), this further supports the idea that higher adolescent gamblers in this sample are at risk of problem gambling later on. However, the different level of substance use between the two classes of higher gamblers was not related to the likelihood of experiencing gambling-related problems, underlining the lack of interplay between the two behaviors.
Early- and later-onset gamblers did not differ for their preferred type of gambling activity, as both reported playing cards and scratch cards as top-2 favorites, consistent with previous reports (Martínez‑Loredo et al., 2019; Verdura-Vizcaíno et al., 2014). However, Later-onset increasing gamblers showed a higher variety of gambling activities than their stable gambler peers. This characteristic is important, as it was shown that maintaining a higher variety of gambling activities from adolescence to adulthood increases the risk of adult problem gambling, above and beyond the experience of gambling problems in adolescence (Carbonneau et al., 2015a). Moreover, Later-onset increasing gamblers reported more gambling activity on the internet than Stable gamblers, a characteristic that has been shown to increase the likelihood of at-risk and problem gambling (Potenza et al., 2011). Thus, by age 17, Later-onset increasing gamblers may be the most at risk among higher gamblers with regard to later problem gambling.
As expected, members of all trajectory-classes of users reported overall a higher variety of substances used as well as a higher likelihood of substance abuse and of experiencing problems related to their use. Moreover, despite small differences in the level of use of one substance or another, early-onset higher users with or without gambling participation reported a higher variety of substances used and were more likely to report substance abuse and problems related to using substances than their respective later-onset user peers with or without gambling participation, which is consistent with previous reports (Carbonneau et al., 2021; Felton et al., 2015; Moss et al., 2014). Thus, adolescents in trajectory-classes with a similar longitudinal pattern of substance use did not differ with regard to substance use characteristics, irrespective of whether they were also gambling or not. Together, these results further support the hypothesis that these behaviors do not mutually influence or exacerbate each other, consistent with a general addictive syndrome (Shaffer et al., 2004; Vitaro et al., 2001; 2019; Werner et al., 2020).
In sum, the associations between joint-trajectories of gambling participation and substance use and their characteristics (i.e., variety, sub-types of activity, and related problems at age 17) remained essentially behavior-specific, as the course of each behavior did not seem to influence the other’s particularities. With regard to gambling participation, the results also suggest that a later onset followed by an increasing course warrants serious attention. Follow-up of the two trajectory-classes of higher gamblers should help determine to what extent the observations at 17 years of age foreshadow gambling problems or their severity in adulthood. The present findings support the relevance of considering the patterns of gambling participation and substance use to assess adolescents’ risk with regard to addictive behaviors, as well as to implement preventive and therapeutic interventions (Derevensky, 2015; Vitaro et al., 2014; Volkow & Boyle, 2018). Indeed, while the results are consistent with an addictive syndrome model and thus with a common approach to intervention, the additional problems experienced in relation to either gambling participation or substance use also support the idea of a differential or individualized approach to prevention and treatment (Derevensky, 2015; Grant & Chamberlain, 2020; Vitaro et al., 2014; Werner et al., 2020).
Strengths and Limitations
A large population cohort and multiple assessments to estimate jointly adolescents’ longitudinal patterns of gambling participation and substance use are important strengths of the present study. Using an integrated variable- and person-centered method provided a valid account of adolescents’ developmental course in comparison to their peers. Examining the associations between trajectory-classes and gambling or substance use characteristics at age 17—within a multivariate framework controlling for confounders—strengthens the conclusions of this study. However, several limitations should be noted. First, adolescents’ gambling participation and substance use were based on self-reports, which may implicate participants’ self-presentation concerns or recall bias. Unfortunately, there is no easily available alternative to assess large population-based samples, and self-reports remain the most widely used method for surveys in the general population (Barnes et al., 2009; 2011; Johnston et al., 2018). Second, it is important to underline the associative, rather than causal, nature of the results. This limitation is especially important considering that the characteristics examined at age 17 were assessed concurrently to the last assessment of gambling participation and substance use. Third, using one problem as threshold for problem gambling implies that most participants with a positive code reported subclinical levels of problem gambling. However, prior studies have highlighted the importance of considering lower, subclinical levels of problem gambling with regard to addictive behaviors and psychosocial adjustment (Buja et al., 2017; Carbonneau et al., 2015b). Fourth, the results of LCGMM have been criticized for not being easily replicated across studies (Petersen et al., 2019). Hence, we followed the recommendations for conducting analyses and reporting in latent trajectory studies, such as reporting on preliminary steps of analysis and on alternative models tested and using a range of indices and criteria when enumerating classes (Kandauda et al., 2016; Van de Schoot et al., 2017). Finally, the study was based on a population of mostly French-speaking adolescents and replications are needed to examine the generalizability of the results.
These limitations notwithstanding, the present study contributes to filling a gap in the extant literature, first by investigating developmental patterns of single and co-occurrent gambling participation and substance use based on multiple assessments from pre- to late adolescence, in a population-based cohort. Second, this study showed that these two behaviors do not appear to influence or exacerbate each other during adolescence, which is consistent with an addictive syndrome perspective. In terms of clinical implications, the present results confirm the importance of considering both the frequency and the variety of activities for both gambling participation and substance use to assess adolescents’ level of risk (Carbonneau et al., 2015a; 2021). The findings also underline the importance of screening for both addictive behaviors and their related problems in individuals seeking help regarding their gambling or substance use. Finally, the study supports both a common and specific approach to prevention and treatment with adolescent gamblers and substance users (Grant & Chamberlain, 2020; Vitaro et al., 2014).
References
Afifi, T. O., Nicholson, R., Martins, S. S., & Sareen, J. A. (2016). Longitudinal Study of the Temporal Relation Between Problem Gambling and Mental and Substance Use Disorders Among Young Adults. Canadian Journal of Psychiatry, 61(2), 102–111. doi:https://doi.org/10.1177/0706743715625950
Allami, Y., Vitaro, F., Brendgen, M., Carbonneau, R., & Tremblay, R. E. (2018). Identifying at-risk profiles and protective factors for problem gambling: A longitudinal study across adolescence and early adulthood. Psychology of Addictive Behaviors, 32(3), 373–382. https://doi.org/10.1037/adb0000356
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington: American Psychiatric Association
Barnes, G. M., Welte, J. W., Hoffman, J. H., & Tidwell, M. C. (2009). Gambling, alcohol, and other substance use among youth in the United States. Journal of Studies on Alcohol and Drugs, 70(1), 134–142. https://doi.org/10.15288/jsad.2009.70.134
Barnes, G. M., Welte, J. W., Hoffman, J. H., & Tidwell, M. C. O. (2011). The co-occurrence of gambling with substance use and conduct disorder among youth in the United States. The American Journal on Addictions, 20, 166–173. https://doi.org/10.1111/j.1521-0391.2010.00116.x
Black, D. W., Allen, J., & Bormann, N. L. (2021). Are Comorbid Disorders Associated with Changes in Gambling Activity? A Longitudinal Study of Younger and Older Subjects with DSM-IV Pathological Gambling. Journal of Gambling Studies. Advance online publication. https://doi.org/10.1007/s10899-021-10000-x
Buja, A., Lion, C., Scioni, M., Vian, P., Genetti, B., Vittadello, F. … Baldo, V. (2017). SOGS-RA gambling scores and substance use in adolescents. Journal of Behavioral Addictions, 6(3), 425–433. https://doi.org/10.1556/2006.6.2017.043
Carbonneau, R., Vitaro, F., Brendgen, M., & Tremblay, R. E. (2015a). Variety of gambling activities from adolescence to age 30 and association with gambling problems: a 15-year longitudinal study of a general population sample. Addiction, 110(12), 1985–1993. https://doi.org/10.1111/add.13083
Carbonneau, R., Vitaro, F., Brendgen, M., & Tremblay, R. E. (2015b). Trajectories of gambling problems from mid-adolescence to age 30 in a general population cohort. Psychology of Addictive Behaviors, 29(4), 1012–1021. https://doi.org/10.1037/adb0000102
Carbonneau, R., Vitaro, F., Brendgen, M., & Tremblay, R. E. (2021). Alcohol, Marijuana and Other Illicit Drugs Use Throughout Adolescence: Co-occurring Courses and Preadolescent Risk-Factors. Child Psychiatry and Human Development. https://doi.org/10.1007/s10578-021-01202-w. https://doi.org/10.1007/s10578-021-01202-wAdvance online publication
Cicchetti, D., & Rogosh, F. A. (2018). A Developmental Psychopathology Perspective on Substance Use. Alcohol Use Disorders: A Developmental Science Approach to Etiology. New-York: Oxford University Press
Clark, S. L., & Muthen, B. (2009). Relating latent class analysis results to variables not included in the analysis. Available at http://www.statmodel.com/download/Relatinglca.pdf
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.).). Hillsdale, NJ: Erlbaum
Derevensky, J. L. (2015). Youth Gambling: Some Current Misconceptions. Austin Journal of Psychiatry and Behavior Science, 2(2), 1039
Dowling, N. A., Aarsman, S. R., & Merkouris, S. S. (2021). Risk, compensatory, and protective factors in problem gambling: The role of positive mental health characteristics. Addictive Behaviors, 112, 106604. https://doi.org/10.1016/j.addbeh.2020.106604
Dowling, N. A., Butera, C. A., Merkouris, S. S., Youssef, G. J., Rodda, S. N., & Jackson, A. C. (2019). The Reciprocal Association between Problem Gambling and Mental Health Symptoms/Substance Use: Cross-Lagged Path Modelling of Longitudinal Cohort Data. Journal of Clinical Medicine, 8(11), 1888. https://doi.org/10.3390/jcm8111888
Edgerton, J. D., Melnyk, T. S., & Roberts, L. W. (2015). Problem Gambling and the Youth-to-Adulthood Transition: Assessing Problem Gambling Severity Trajectories in a Sample of Young Adults. Journal of Gambling Studies, 31(4), 1463–1485. https://doi.org/10.1007/s10899-014-9501-2
Feldman, B., Masyn, K. E., & Conger, R. (2009). New approaches to studying problem behaviors: A comparison of methods for modeling longitudinal, categorical adolescent drinking data. Developmental Psychology, 45, 652–676
Felton, J. W., Kofler, M. J., Lopez, C. M., Saunders, B. E., & Kilpatrick, D. G. (2015). The emergence of co-occurring adolescent polysubstance use and depressive symptoms: A latent growth modeling approach. Development & Psychopathology, 27, 1367–1383
Goudriaan, A. E., Slutske, W. S., Krull, J. L., & Sher, K. J. (2009). Longitudinal patterns of gambling activities and associated risk factors in college students. Addiction, 104, 1219–1232. https://doi.org/10.1111/j.1360-0443.2009.02573.x
Grant, J. E., & Chamberlain, S. R. (2020). Gambling and substance use: Comorbidity and treatment implications. Progress in Neuro-psychopharmacology & Biological Psychiatry, 99, 109852. https://doi.org/10.1016/j.pnpbp.2019.109852
Gupta, R., Nower, L., Derevensky, J. L., Blaszczynski, A., Faregh, N., & Temcheff, C. (2013). Problem gambling in adolescents: an examination of the pathways model. Journal of Gambling Studies, 29(3), 575–588. https://doi.org/10.1007/s10899-012-9322-0
Hardin, J. W., & Hilbe, J. M. (2018). Generalized Linear Models and extensions Fourth Edition. College Station Texas, Stata Press
Henly, G. A., & Winters, K. C. (1989). Development of psychosocial scales for the assessment of adolescents involved with alcohol and drugs. International Journal of the Addictions, 24, 973–1001. https://doi.org/10.3109/10826088909047324
Johnston, L. D., Miech, R. A., O’Malley, P. M., Bachman, J. G., Schulenberg, J. E., & Patrick, M. E. (2018). Monitoring the future national survey results on drug use: 1975-2017: Overview, key findings on adolescent drug use. Ann Arbor: Institute for Social Research, University of Michigan
Jun, H. J., Sacco, P., & Cunningham-Williams, R. M. (2021). Gambling in Emerging Adulthood: the Role of Adolescent Depressive Symptoms, Antisocial Behaviors, and Alcohol Use. International Journal of Mental Health and Addiction, 19, 494–507. https://doi.org/10.1007/s11469-019-00087-0
Kandauda, A. S., Wickrama, T. K. L., Walker-O’Neal, C., & Lorenz, F. O. (2016). Higher-order growth curves and mixture modeling with Mplus. New-York: Routledge
Kessler, R. C., Hwang, I., LaBrie, R., et al. (2008). DSM-IV pathological gambling in the National Comorbidity Survey Replication. Psychological Medecine, 38(9), 1351–1360. doi:https://doi.org/10.1017/S0033291708002900
Kurilla, A. (2021). Is Subtyping of Gamblers Based on the Pathways Model of Problem and Disordered Gambling Valid? A Systematic Review. Journal of Gambling Studies. https://doi.org/10.1007/s10899-020-09995-6. https://doi.org/10.1007/s10899-020-09995-6Advance online publication
Loo, J., Kraus, S. W., & Potenza, M. N. (2019). A systematic review of gambling-related findings from the National Epidemiologic Survey on Alcohol and Related Conditions. Journal of Behavioral Addictions, 8(4), 625–648. https://doi.org/10.1556/2006.8.2019.64
Lorains, F. K., Cowlishaw, S., & Thomas, S. A. (2011). Prevalence of comorbid disorders in problem and pathological gambling: systematic review and meta-analysis of population surveys. Addiction, 106(3), 490–498. https://doi.org/10.1111/j.1360-0443.2010.03300.x
Lynne-Landsman, S. D., Bradshaw, C. P., & Ialongo, N. S. (2010). Testing a developmental cascade model of adolescent substance use trajectories and young adult adjustment. Development & Psychopathology, 22, 933–948
Martínez-Loredo, V., Grande-Gosende, A., Fernández-Artamendi, S., Secades-Villa, R., & Fernández-Hermida, J. R. (2019). Substance Use and Gambling Patterns Among Adolescents: Differences According to Gender and Impulsivity. Journal of Gambling Studies, 35(1), 63–78. https://doi.org/10.1007/s10899-018-09824-x
Merkouris, S. S., Greenwood, C. J., Youssef, G. J., Letcher, P., Vassallo, S., Dowling, N. A., & Olsson, C. A. (2021). Adult Gambling Problems and Histories of Mental Health and Substance Use: Findings from a Prospective Multi-Wave Australian Cohort Study. Journal of Clinical Medicine, 10(7), 1406. https://doi.org/10.3390/jcm10071406
Moss, H. B., Chen, C. M., & Yi, H. (2014). Early adolescent patterns of alcohol, cigarettes, and marijuana polysubstance use and young adult substance use outcomes in a nationally representative sample. Drug and Alcohol Dependence, 136, 51–62
Muthén, L. K., & Muthén, B. O. (1998-2017). Mplus User’s Guide. Eighth Edition. Los Angeles, CA: Muthén & Muthén
Mutti-Packer, S., Hodgins, D. C., El-Guebaly, N., Casey, D. M., Currie, S. R., Williams, R. J. … Schopflocher, D. P. (2017). Problem gambling symptomatology and alcohol misuse among adolescents: A parallel-process latent growth curve model. Psychology of Addictive Behaviors, 31(4), 447–456. https://doi.org/10.1037/adb0000261
Nagin, D. S. (2005). Class-based modeling of development. Cambridge: Harvard University Press
Nower, L., Martins, S. S., Lin, K. H., & Blanco, C. (2013). Subtypes of disordered gamblers: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Addiction, 108(4), 789–798. https://doi.org/10.1111/add.12012
Orri, M., Boivin, M., Chen, C., Ahun, M. N., Geoffroy, M. C., Ouellet-Morin, I. … Côté, S. M. (2021). Cohort Profile: Quebec Longitudinal Study of Child Development (QLSCD). Social Psychiatry and Psychiatric Epidemiology, 56(5), 883–894. https://doi.org/10.1007/s00127-020-01972-z
Peters, E. N., Nordeck, C., Zanetti, G., O’Grady, K. E., Serpelloni, G., Rimondo, C., & Schwartz, R. P. (2015). Relationship of gambling with tobacco, alcohol, and illicit drug use among adolescents in the USA: Review of the literature 2000–2014. The American Journal on Addictions, 24, 206–216. https://doi.org/10.1111/ajad.12214
Petersen, K. J., Qualter, P., & Humphrey, N. (2019). The application of latent class analysis for investigating population child mental health: A systematic review. Frontiers in Psychology, 10, 1214
Petry, N. M., Stinson, F. S., & Grant, B. F. (2005). Comorbidity of DSM-IV pathological gambling and other psychiatric disorders: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Journal of Clinical Psychiatry, 66(5), 564–574. doi:https://doi.org/10.4088/jcp.v66n0504
Potenza, M. N. (2017). Clinical neuropsychiatric considerations regarding nonsubstance or behavioral addictions. Dialogues in Clinical Neuroscience, 19(3), 281–291. https://doi.org/10.31887/DCNS.2017.19.3/mpotenza
Potenza, M. N. (2008). Review. The neurobiology of pathological gambling and drug addiction: An overview and new findings. Philosophical Transactions of the Royal Society of London Series B, Biological Sciences, 363, 3181–3189. https://doi.org/10.1098/rstb.2008.0100
Potenza, M. N., Wareham, J. D., Steinberg, M. A., Rugle, L., Cavallo, D. A., Krishnan-Sarin, S., & Desai, R. A. (2011). Correlates of at-risk/problem internet gambling in adolescents. Journal of the American Academy of Child and Adolescent Psychiatry, 50(2), 150–159e3. https://doi.org/10.1016/j.jaac.2010.11.006
Rash, C. J., Weinstock, J., & Van Patten, R. (2016). A review of gambling disorder and substance use disorders. Substance Abuse & Rehabilitation, 7, 3–13. doi:https://doi.org/10.2147/SAR.S83460
Sawilowsky, S. (2009). New effect size rules of thumb. Journal of Modern Applied Statistical Methods, 8(2), 467–474. Doi:https://doi.org/10.22237/jmasm/1257035100
Shaffer, H. J., LaPlante, D. A., LaBrie, R. A., Kidman, R. C., Donato, A. N., & Stanton, M. V. (2004). Toward a syndrome model of addiction: multiple expressions, common etiology. Harvard Review of Psychiatry, 12(6), 367–374. https://doi.org/10.1080/10673220490905705
Slutske, W. S., Ellingson, J. M., Richmond-Rakerd, L. S., Zhu, G., & Martin, N. G. (2013). Shared genetic vulnerability for disordered gambling and alcohol use disorder in men and women: evidence from a national community-based Australian twin study. Twin Research and Human Genetics, 16(2), 525–534
Statistics Canada. (1995). Overview of survey instruments for 1994-1995 data collection, cycle 1. Ottawa, ON: Statistics Canada
Swendsen, J., Conway, K. P., Degenhardt, L., Dierker, L., Glantz, M., Jin, R., et al. (2009). Socio-demographic risk factors for alcohol and drug dependence: the 10-year follow-up of the national comorbidity survey. Addiction, 104, 1346–1355
Thompson, C. A., & Arah, O. A. (2014). Selection bias modeling using observed data augmented with imputed record-level probabilities. Annals of Epidemiology, 24(10), 747–753
Van de Schoot, R., Sijbrandij, M., Winter, S. D., Depaoli, S., & Vermunt, J. K. (2017). The GRoLTS-Checklist: Guidelines for reporting on latent trajectory studies. Structural Equation Modeling, 24, 451–467. DOI: https://doi.org/10.1080/10705511.2016.1247646
Verdura-Vizcaíno, E. J., Fernández-Navarro, P., Petry, N., Rubio, G., & Blanco, C. (2014). Differences between early-onset pathological gambling and later-onset pathological gambling: data from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). Addiction, 109(5), 807–813. https://doi.org/10.1111/add.12461
Vitaro, F., Brendgen, M., Ladouceur, R., & Tremblay, R. E. (2001). Gambling, delinquency, and drug use during adolescence: Mutual influences and common risk factors. Journal of Gambling Studies, 17, 171–190. https://doi.org/10.1023/A:1012201221601
Vitaro, F., Dickson, D. J., Brendgen, M., Lacourse, E., Dionne, G., & Boivin, M. (2019). Longitudinal interplay between gambling participation and substance use during late adolescence: A genetically-informed study. Psychology of Addictive Behaviors, 33(5), 457–466. https://doi.org/10.1037/adb0000482
Vitaro, F., Hartl, A. C., Brendgen, M., Laursen, B., Dionne, G., & Boivin, M. (2014). Genetic and environmental influences on gambling and substance use in early adolescence. Behavior Genetics, 44(4), 347–355. https://doi.org/10.1007/s10519-014-9658-6
Vitaro, F., Wanner, B., Ladouceur, R., Brendgen, M., & Tremblay, R. E. (2004). Trajectories of gambling during adolescence. Journal of Gambling Studies, 20, 47–69
Volkow, N. D., & Boyle, M. (2018). Neuroscience of Addiction: Relevance to Prevention and Treatment. The American Journal of Psychiatry, 175(8), 729–740. https://doi.org/10.1176/appi.ajp.2018.17101174
Wanner, B., Vitaro, F., Ladouceur, R., Brendgen, M., & Tremblay, R. E. (2006). Joint trajectories of gambling, alcohol and marijuana use during adolescence: a person- and variable-centered developmental approach. Addictive Behaviors, 31(4), 566–580. https://doi.org/10.1016/j.addbeh.2005.05.037
Wanner, B., Vitaro, F., Carbonneau, R., & Tremblay, R. E. (2009). Crosslagged links among gambling, substance use, and delinquency from midadolescence to young adulthood: Additive and moderating effects of common risk factors. Psychology of Addictive Behaviors, 23, 91–104. https://doi.org/10.1037/a0013182
Wareham, J. D., & Potenza, M. N. (2010). Pathological gambling and substance use disorders. The American Journal of Drug and Alcohol Abuse, 36(5), 242–247. https://doi.org/10.3109/00952991003721118
Welte, J. W., Barnes, G. M., Tidwell, M. C. O., & Hoffman, J. H. (2009). The association of form of gambling with problem gambling among American youth. Psychology of Addictive Behaviors, 23, 105–112
Werner, K. B., Cunningham-Williams, R. M., Ahuja, M., & Bucholz, K. K. (2020). Patterns of gambling and substance use initiation in African American and White adolescents and young adults. Psychology of Addictive Behaviors, 34(2), 382–391. https://doi.org/10.1037/adb0000531
Williams, R. J., Leonard, C. A., Belanger, Y. D., Christensen, D. R., El-Guebaly, N., Hodgins, D. C. … Stevens, R. (2021). Predictors of gambling and problem gambling in Canada. Canadian Journal of Public Health, 112(3), 521–529. https://doi.org/10.17269/s41997-020-00443-x
Winters, K. C., & Stinchfield, R. D. (2012). Youth Gambling: Prevalence, Risk and Protective Factors and Clinical Issues. In: Increasing the odds, vol. 7, What Clinicians Need to Know About
Gambling Disorders. National Center for Responsible Gaming (NCRG)
Winters, K. C., Stinchfield, R. D., & Fulkerson, J. (1993). Toward the development of an adolescent gambling problem severity scale. Journal of Gambling Studies, 9, 63–84. https://doi.org/10.1007/BF01019925
Winters, K. C., Stinchfield, R. D., Henly, G. A., & Schwartz, R. H. (1990). Validity of adolescent self-report of alcohol and other drug involvement. International Journal of the Addictions, 25, 1379–1395. https://doi.org/10.3109/10826089009068469
Xian, H., Giddens, J. L., Scherrer, J. F., Eisen, S. A., & Potenza, M. N. (2014). Environmental factors selectively impact co-occurrence of problem/pathological gambling with specific drug-use disorders in male twins. Addiction, 109(4), 635–644. https://doi.org/10.1111/add.12407
Acknowledgments
We thank the families and the participants of the Montreal Longitudinal and Experimental Study for their collaboration to this project, and the staff of the Research Unit on Children?s Psychosocial Maladjustment for data collection and management.
Funding
We thank the Quebec Government Ministry of Health, the Fond Quebecois de la Recherche sur la Societe et la Culture, Canada’s Social Science and Humanities Research Council.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Carbonneau, R., Vitaro, F., Brendgen, M. et al. Developmental Patterns of Gambling Participation and Substance use Throughout Adolescence in a Population Birth Cohort. J Gambl Stud 39, 137–157 (2023). https://doi.org/10.1007/s10899-022-10107-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10899-022-10107-9