
Abstract
Internet-based interventions have emerged as a new treatment and intervention modality for psychological disorders. Given their features of treatment flexibility, anonymity and confidentiality, this modality may be well suited in the management of addictive behaviours. A systematic literature review of the effectiveness and treatment outcomes of Internet-based interventions for smoking cessation, problematic alcohol use, substance abuse and gambling was performed. Studies were included if they met the following criteria: clients received a structured therapeutic Internet-based intervention for a problematic and addictive behaviour; included more than five clients; effectiveness was based on at least one outcome; outcome variables were measured before and immediately following the interventions; had a follow-up period; and involved at least minimal therapist contact over the course of the program. Sixteen relevant studies were found; nine addressed the effects of Internet-based interventions on smoking cessation, four on gambling, two on alcohol and one on opioid dependence. All studies demonstrated positive treatment outcomes for their respective addictive behaviours. The current review concluded that Internet-based interventions are effective in achieving positive behavioural change through reducing problematic behaviours. This mode of therapy has been found to have the capacity to provide effective and practical services for those who might have remained untreated, subsequently reducing the barriers for help-seekers. This in turn provides imperative information to treatment providers, policy makers, and academic researchers.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The evolution of Internet communication systems has led to an increase in the availability and promotion of Internet-based interventions. Internet-based interventions involve the delivery of treatment programs in conjunction with clinician assistance via the Internet (Abbott et al. 2008). Clinician assistance occurs either through asynchronous or time-delayed means of communication (for example, email) or synchronous/simultaneous communication (for example, chat-based text exchanges).
Although support has been shown for Internet modes of therapy, professionals and the general population have raised concerns about Internet-based interventions; for example, high attrition rates, ethical concerns, and lack of regulations (Lester 2006; Skinner and Latchford 2006). Early studies assessing the efficacy of Internet-based interventions often incorporated small samples, had high attrition rates, and implemented relatively short follow-up periods (Danielsson et al. 2014). These limitations make it difficult to draw conclusions about the observed effects. In addition, concerns have been expressed about ethical issues relating to confidentiality, handling of urgent issues, and impersonations, represent elements of concern (Barak et al. 2008). Further, current codes of conduct do not cover various areas within Internet-based interventions, for example professional insurance of negligence, placing participants at risk of potentially unresolvable issues (Barak et al. 2008). As it has been suggested that Internet communications may soon become a standard adjunct with psychological services (Wells et al. 2007), it is prudent that these legal regulations and concerns are considered and outlined. For example, some organizations such as, the American Counseling Association, have begun to provide clear directives regarding the provisions of online treatment (Wells et al. 2007). Given this, the American Psychology Association has noted the three states in America that have already passed laws specifying the psychologists’ legal obligations in online therapy (DeAngelis 2012). Furthermore, the Health Insurance Portability and Accountability Act of 1996, has now been set in motion to cover and regulate the privacy and security of all technology-based healthcare transactions (Barak and Grohol 2011). Given the accessibility and rise of various forms of online therapy, it is imperative that the responsibilities of both the therapist and the client are continuously reviewed.
In an attempt to supersede ethical and practical concerns, recent studies have investigated the potential benefits and outcomes of Internet-based interventions using more rigorous methodological approaches (Barak et al. 2008; Castren et al. 2013; Hester et al. 2013). The findings from these investigations suggest that Internet-based interventions results in positive treatment outcomes for numerous disorders, such as anxiety (Carlbring et al. 2003; Kenwright and Marks 2004), depression (Andersson et al. 2005; Griffiths et al. 2004), substance-use (King et al. 2009) and addictive disorders, leading to the recognition of this type of intervention as a plausible treatment option (Gainsbury and Blaszczynski 2011a; Proudfoot et al. 2011). Furthermore, Internet-based interventions for addictive disorders, such as smoking and problem gambling, have been found to be successful in numerous studies, with the majority of clients reporting an improvement in their quality of life due to their maintained abstinence (Carlbring and Smit 2008; Eidem 2010).
Past meta-analyses reviewing the effectiveness of Internet-based interventions for a variety of psychological disorders have revealed an average medium effect size of 0.53 (Barak et al. 2008). This effect size was noted to be similar to the average effect size of traditional, face-to-face therapy (Barak et al. 2008) suggesting both online and face-to-face interventions can potentially provide patients with similar outcomes. Similarly, a past systematic review indicated positive treatment effects at the completion of Internet-based interventions for numerous addictive disorders (Gainsbury and Blaszczynski 2011b). Therefore, this mode of treatment can potentially enable behavioural change among participants. Ecological Momentary Interventions (EMI) have also found to be successful in treating a variety of disorders (Hay and Kinnier 1998). EMI’s are very similar to Internet-based interventions, but instead provide psychological interventions to clients via mobile phone applications rather than Internet-based websites. The sole purpose of EMI’s is to provide treatment and unstructured recommendations to people in real time and within their natural setting (Hay and Kinnier 1998). A recent systematic review by Heron and Smyth (2010) found that EMI’s were successfully delivered and efficacious in reducing symptoms for a range of concerns, such as, anxiety, eating disorder, smoking cessation and alcohol use. Given the success of distant and online interventions, the current review aimed to identify further advances in this arena and to determine the consistency of treatment outcomes for Internet-based interventions.
Internet-based psychological and medical services for all disorders have increased over the last few years with this modality offering advantages for both the consumer and the therapist (Gainsbury and Blaszczynski 2011a; Proudfoot et al. 2011). Firstly, the availability and convenience of Internet-based interventions assist clients in overcoming barriers that prevent face-to-face counseling, such as transport problems and geographical remoteness (Gainsbury and Blaszczynski 2011a; Proudfoot et al. 2011). For example, it is estimated that 90 % of people with gambling problems do not enter formal treatment (Productivity Commission 2010). This convenient and flexible method of delivery fosters treatment retention, especially in populations displaying high attrition rates (Cunningham 2007), for example, individuals diagnosed with addiction disorders. The treatment of this specific clinical population is also affected by low uptake rates and high attrition rates ranging between 17 and 76 % for traditional therapies (McLellan 2006; Westphal 2006). These figures suggest that the needs of this population are not being met with standard face-to-face treatment (Ladouceur et al. 2001; McLellan 2006; Westphal 2006). In contrast, lower attrition rates found in an Internet-based compared to a face-to-face group, suggest that the former mode of therapy may better meet the needs of this clinical population (King et al. 2009).
Internet-based interventions are more cost-effective compared to face-to-face interventions. This is mainly attributed to having reduced demand for costly therapist resources and lower ongoing costs (Gainsbury and Blaszczynski 2011a; McCrone et al. 2004). Therefore, online programs can provide services to a large number of people without associated increases in cost. Thirdly, the anonymity of Internet-based interventions provides a platform for people who are unwilling to access face-to-face treatment, often due to stigma and embarrassment (Cunningham 2007; Gainsbury et al. 2014). In addition, due to the anonymity of Internet-based interventions, clients usually provide more open and honest responses to sensitive topics (Gainsbury and Blaszczynski 2011a). Fourthly, the Internet provides a platform for effective empirical evaluation, as the use of online resources, completion of exercises, and tracking data can be readily extracted (Proudfoot et al. 2011). Finally, Internet interventions can be conducted concurrently with various forms of therapist contact, such as, telephone calls and emails, which may suit clients more than face-to-face therapies.
Increasingly funding bodies and policy makers are limiting funding to treatment demonstrated empirically to be effective. Given the rapidly changing Internet environment and dynamic changes in online interventions, the current paper aimed to evaluate the effectiveness of Internet-based intervention programs for the treatment of addictive behaviours. This is an important area of research as Internet-based interventions are likely to be a viable treatment option to aid those with various psychological disorders, including addictive disorders. As a growing proportion of the population have easy and affordable access to the Internet and are comfortable seeking help via this means, Internet interventions are likely to be of increasing value to consumers and treatment providers.
Method
Initial Search
The initial literature review was conducted in May, 2015. The search strategy followed guidelines outlines in the Cochrane Reviewers’ Handbook (Alderson et al. 2004). Electronic databases including PsycINFO, MEDLINE, Embase, and Google Scholar were searched using combinations of the following terms: internet, online, treatment, therapy, intervention, gambling, addiction, alcohol, and tobacco. In addition to these electronic searches, reference lists of relevant review papers identified in the literature search were examined for relevant references.
Inclusion Criteria
Studies were included if they met the following criteria: (1) clients received a structured therapeutic Internet-based intervention for addiction recognized addictive disorder; (2) the study included more than five clients; (3) effectiveness was based on at least one assessed outcome; (4) outcome variables were measured before and immediately following the interventions (additional follow-up outcomes also included); and (5) the intervention involved at least minimal therapist contact over the course of the treatment program (including telephone and face-to-face support).
Classification of Studies
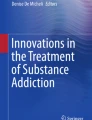
The search strategy included screening the title and abstract of 3868 journal articles and identifying ineligible studies, within PsycINFO, MEDLINE, Embase and Google Scholar. Due to the large number of results generated by Google Scholar, only the first 500 articles were reviewed. This limit was enforced, as the relevant articles found within Google Scholar had been uncovered by the former databases. Most papers were excluded based on the title or information contained in the abstract. Where necessary, the complete paper was obtained and assessed for classification. A second independent reviewer (JO) screened a random selection of 30 % of these articles to ensure inter-rater reliability, which was 95 %. A detailed overview of the search strategy is displayed in Fig. 1.

Overview of search strategy
Papers were excluded if: (1) they were not in a relevant field; (2) they were a duplicate of a previously collected paper; (3) the intervention was not a therapy program (i.e. self-help, personalized feedback, peer support, prevention, education, newsletters, or information or non-expert advice); (4) treatment was not for addiction disorders; (5) programs were not completed via the Internet; or (6) they were not in English.
Information Extraction and Summary
The following data were extracted from each publication: author, publication year, country, study design, sample size, age, sex, type of intervention, outcome measure, and main effects. Articles were ranked on the basis of the study design, according to The Australian National Health and Medical Research Council (NHMRC), shown in Table 1.
Evaluation of Selected Papers
All papers were classified according to the Downs and Black (1998) checklist. The checklist demonstrates high test–retest reliability (r = 0.88), good inter-rater reliability (r = 0.75), and high internal consistency (KR-20 = 0.89). The checklist contains 27 items; each item was scored out of one point (0 = no/unable to determine; 1 = yes). Total score could therefore range from 0 to 27 points. The quality of each paper was categorized as poor (0–9 points), moderate (10–18 points), or good (19–20 points). Double coding was performed on a subset of articles (30 %) and occasional disagreements were discussed in further detail until a consensus on the final score was reached. High inter-rater reliability (r = 0.90) was demonstrated, which reflects a substantial agreement between raters.
Results
After excluding all studies that did not fill the inclusion criteria, a final number of 16 articles were included in the review and summarized in Table 2.
Sample Characteristics
Of the 16 included articles, the majority of studies evaluated the effect of Internet-based intervention on smoking cessation (Abroms et al. 2008; Brendryen et al. 2008; Graham et al. 2011; Hotta et al. 2007; Japuntich et al. 2006; Linke et al. 2012; Mermelstein and Turner 2006; Woodruff et al. 2007; Zbikowski et al. 2008), four studies evaluated the effect of Internet-based intervention on gambling (Carlbring et al. 2012; Carlbring and Smit 2008; Castren et al. 2013; Myrseth et al. 2013), with two studies examining Internet-based programs for excessive alcohol consumption (Blankers et al. 2011; Hester et al. 2013) and one for opioid dependence (King et al. 2009).
Target populations primarily consisted of treatment-seeking adults however two papers evaluated Internet-based programs developed for adolescents (Mermelstein and Turner 2006; Woodruff et al. 2007), one for college students (Abroms et al. 2008) and one for university employees (Hotta et al. 2007). Among the 16 studies, nine were conducted in the United States, two in Norway, two in Sweden, one in Finland, one in the Netherlands and one in Japan. The majority were randomized controlled trials, with between 37 and 11,143 participants.
Evaluation of Quality of the Studies
The overall mean quality score on the Downs and Black (1998) checklist was in the moderate range (M = 17.5, SD = 2.88). As seen in Table 3, scores ranged from 13 (moderate; n = 9) to 22 (good; n = 7). Inspection of the quality assessment criteria conveyed that all studies met seven out of 27 criteria, with Brendryen et al.’s (2008) study achieving the highest criteria of 22. However, only one of the sixteen articles reported distribution of principal confounders, ensured researchers were blind, and examined whether compliance with the intervention was reliable. Furthermore, none of the selected studies met three of the 27 criteria, which included; reporting adverse effects of the intervention, making an attempt to blind participants to their condition, and ensuring that the randomization assignment was concealed from both patients and health care staff until the recruitment was complete.
Smoking Cessation
Among the nine studies that addressed smoking cessation, seven were conducted in the United States (Abroms et al. 2008; Graham et al. 2011; Japuntich et al. 2006; Linke et al. 2012; Mermelstein and Turner 2006; Woodruff et al. 2007; Zbikowski et al. 2008), one in Norway (Brendryen et al. 2008) and one in Japan (Hotta et al. 2007). The majority were randomised controlled trials (RCT) (Abroms et al. 2008; Brendryen et al. 2008; Graham et al. 2011; Japuntich et al. 2006; Linke et al. 2012; Mermelstein and Turner 2006; Woodruff et al. 2007), with two being non-comparative studies evaluating the success of an Internet-based intervention (Hotta et al. 2007; Zbikowski et al. 2008). The number of clients in each study ranged from n = 38 to n = 11,143, and all studies included both male and female participants.
These studies showed that Internet-based interventions may have a positive effect on smoking cessation. Specifically, several studies found that online use and number of log-ins was positively associated with quit outcomes (Graham et al. 2011; Japuntich et al. 2006; Zbikowski et al. 2008). Graham et al. (2011) found that less than 1 % of participants who chose to use the Web program never returned to the website after registering. This suggests that participants who are interested in using Internet interventions are likely to engage and complete the program. Additionally, the Internet was found to be a generally successful method in guiding smoking cessation because of its visual appeal, accessibility, anonymity, interactivity and so on. However, Woodruff et al. (2007) found that the positive results of the Internet-based intervention was not generally maintained at 1 year follow-up assessments, and suggested that the implementation of booster sessions or additional communication methods may have been benficial in helping clients maintain their abstinence.
Studies that included additional methods of communication with a therapist, such as, e-mails and telephone calls, reported an advantage in treatment outcomes, such as, e-mails and telephone calls. For example, participants who utilized the Internet intervention more frequently were also more engaged in telephone counseling (Zbikowski et al. 2008). Similarly, Hotta et al. (2007) reported that participants who engaged with e-mail messaging in the first week of the program sustained abstinence at the 1-year follow-up, while those who did not engage with this additional component were less likley to sustain cessation for 1 year. However, a separate study found that the addition of the proactive telephone did not provide significant improvement in abstinence above and beyond the online program (Mermelstein and Turner 2006). A main limitation mentioned in several studies was the lack of generalizability to the sample frame, as the study sample was comprised of either college students, those who enrolled to participate or those who already utilize the service and not based on randomization to the service (Abroms et al. 2008; Graham et al. 2011; Japuntich et al. 2006; Woodruff et al. 2007; Zbikowski et al. 2008).
Gambling
Four studies addressed the effect of Internet-based interventions on pathological gambling; two studies were conducted in Sweden (Carlbring et al. 2012; Carlbring and Smit 2008), one in Norway (Myrseth et al. 2013) and one in Finland (Castren et al. 2013). Three were non-comparative studies evaluating the success of a cessation program, and one was a RCT. The number of participants varied between n = 66 to n = 471, and all studies included both male and female participants. The four Internet-based interventions resulted in favourable changes in pathological gambling and treatment effects were sustained at follow-ups, up to 3 years following treatment completion (Carlbring et al. 2012; Carlbring and Smit 2008; Castren et al. 2013; Myrseth et al. 2013). The implementation of Internet-based interventions and the addition of various treatment components, such as telephone consultations, were found to be both time-efficient and cost-effective, compared to face-to-face treatment methods (Myrseth et al. 2013). Although these programs had dropouts, these rates were consistent with other studies and appeared to be similar or somewhat lower than face-to-face therapy, with drop out rates ranging between between 17 and 31 % (Carlbring et al. 2012; Carlbring and Smit 2008; Castren et al. 2013; Myrseth et al. 2013).
Half of participants completed all eight modules, and from the original sample over 50 % of participants maintained their abstinence at 36 months (Carlbring and Smit 2008). This finding suggests that participants who maintained abstinence were also more likely to have completed the entire program. Internet-based interventions for problem gamblers decreased participants’ engagement with gambling-related activities and it has also had a positive effect on their general psychological distress and psychopathology (Carlbring and Smit 2008; Carlbring et al. 2012; Castren et al. 2013; Myrseth et al. 2013). This positive effect was also consistent for participants who had more severe ratings of depression and anxiety (Carlbring et al. 2012). However, the majority of these findings must be interpreted with cautions, as there was a lack of control groups and comparison groups, such as face-to-face treatment, that would have been valuable in order to examine the effectiveness of Internet-based interventions.
Problematic Alcohol
Two RCT-studies addressed the effectiveness of Internet-based interventions on problem drinking; one was conducted in the United States (Hester et al. 2013), and one in the Netherlands (Blankers et al. 2011). The number of participants varied between n = 189 and n = 205, and all studies included both male and female participants. Both the cessation interventions resulted in positive changes in problematic alcohol consumption habits and related negative consequences. This positive result was evident within Blankers et al.’s (2011) study for both the Internet-based self-help and the Internet-based intervention It was expected that the Internet-based intervention would have higher abstinence rates at 3- and 6-month follow-up compared to the self-help group, however, this hypothesis was not supported, as there was no difference between treatment groups at follow-up, as they both produced positive effects. Within one study the face-to-face condition compared to Internet-based condition was significantly predictive of all outcomes, including, abstinence, reduction in mean drinks per day and alcohol related consequences (Hester et al. 2013). Although the effect of the face-to-face treatment was greater than the Internet-based intervention group, this was only true for one outcome treatment outcome, reduction in mean drinks per day. Hester et al. (2013) found that a frequently mentioned benefit of Internet-based treatment was that individuals who might not otherwise seek treatment would consider an online intervention. Both studies reported several advantages for Internet-based interventions, such as, anonymity which helped facilitate self-disclosure, openness and disinhibition of participants within therapy (Blankers et al. 2011; Hester et al. 2013), and written communication allowed participants the possibility of rereading the material and their interactions with the therapist (Blankers et al. 2011). Limitations mentioned include the high attrition rate (Blankers et al. 2011), the lack of a control group in order to ascertain the effectiveness of the intervention and the lack of generalizability, as the majority of participants had high levels of education and required a significant other to corroborate alcohol intake, potentially limiting the sample (Hester et al. 2013).
Opioid Dependence
One RCT-study from the United States assessed the effectiveness of an Internet-based intervention (in the form of online group therapy) on opioid-dependent outpatients, with 37 participants, both female and male (King et al. 2009). No significant differences were found between the online therapy group and the face-to-face counseling group, after treatment. However, participants expressed a preference for the Internet-based services. With only one RCT, there is limited but positive evidence on the effects of Internet-based interventions on substance abuse. King et al. (2009) noted two main limitations, small sample size and the short study duration. As subsequent evaluations should have larger samples in order to further the development of this Internet-based program, and the treatment duration for this particular clinical population routinely occurs in long-term care, rather than a 6-week period.
Type of Intervention
No single model of therapy was used within the articles identified, however, it was evident that Cognitive Behavioural Therapy (CBT) was the most commonly reported intervention (Blankers et al. 2011; Carlbring et al. 2012; Carlbring and Smit 2008; Castren et al. 2013; Hester et al. 2013; Japuntich et al. 2006; Myrseth et al. 2013). Direct contact with therapists for support and encouragement was provided either over the telephone (Blankers et al. 2011; Carlbring et al. 2012; Carlbring and Smit 2008; Castren et al. 2013; Graham et al. 2011; Linke et al. 2012; Mermelstein and Turner 2006; Myrseth et al. 2013; Zbikowski et al. 2008), through SMS messages (Brendryen et al. 2008; Hester et al. 2013; Linke et al. 2012), via email (Abroms et al. 2008; Hester et al. 2013; Linke et al. 2012) or via interactive voice response messages to the mobile phone (Brendryen et al. 2008). Several approaches also provided peer-based social support between participants through online discussion forums (Blankers et al. 2011; Japuntich et al. 2006; Zbikowski et al. 2008), emails (Hotta et al. 2007), or face-to-face group therapy sessions (King et al. 2009; Woodruff et al. 2007). Internet-based interventions also incorporated motivation interviewing strategies (Blankers et al. 2011; Carlbring and Smit 2008; Castren et al. 2013; Hester et al. 2013; Hotta et al. 2007; Mermelstein and Turner 2006; Myrseth et al. 2013; Woodruff et al. 2007) and behavioural approaches (Linke et al. 2012; Woodruff et al. 2007). However, no study reported the effectiveness of these different online components.
Therapist Contact
Studies rarely isolated and reported the effectiveness of therapist contact. All sixteen studies had some form of therapist contact, however, only seven investigated the usefulness of this contact (Abroms et al. 2008; Graham et al. 2011; Hester et al. 2013; Japuntich et al. 2006; Mermelstein and Turner 2006; Woodruff et al. 2007; Zbikowski et al. 2008). Three studies highlighted the usefulness of telephone calls and found that telephone calls significantly increased cessation at post-assessment and follow-up (Graham et al. 2011; Mermelstein and Turner 2006; Zbikowski et al. 2008). In addition, the greater number of telephone calls completed was associated with increased utilization of the Internet-based intervention (Zbikowski et al. 2008). Two studies employed the use of e-mails as a means of therapist contact and found that sending and receiving emails within the first week of therapy was associated with long-term smoking cessation (Japuntich et al. 2006). It was suggested that emails may be a more promising platform than standard print material, as participants noted reading their emails and adopting the suggested techniques at a much higher rate compared to their self-help books (Abroms et al. 2008). One study investigated the effectiveness of a clinician-led virtual world group, and found that this group led to greater abstinence rates and a reduction in cigarette consumption, when compared to a control group (Woodruff et al. 2007).
The use of face-to-face meetings in conjunction with an Internet-based intervention was the final mode of therapist contact found within this review (Hester et al. 2013). Mixed findings were found for this study, as participants allocated to the face-to-face group demonstrated stronger outcomes compared to participants allocated to both the Internet-based intervention and face-to-face meeting groups (Hester et al. 2013). Although the latter group resulted in weaker outcomes compared to the face-to-face meeting group, their outcomes were only slightly weaker for one dependent variable, a reduction in mean drinks per drinking day (Hester et al. 2013). Among these interventions, it’s evident that the implementation of at least minimal therapist contact is found to be useful and result in positive treatment outcomes when combined with Internet-based interventions.
Effectiveness of the Intervention
The failure to measure and include the effect sizes of Internet-based interventions, limits the conclusions that could potentially be drawn with regards to treatment effectiveness. Past research rarely investigated the effect sizes of interventions and as a result this was listed as a common limitation of Internet-based interventions (Gainsbury and Blaszczynski 2011b). However, it is evident within this review that current research has begun to address this limitation, as five studies reported and identified the effect sizes of their interventions (Blankers et al. 2011; Carlbring and Smit 2008; Hester et al. 2013; Japuntich et al. 2006; Myrseth et al. 2013). Large effect sizes were noted within four studies (Carlbring and Smit 2008; Hester et al. 2013; Japuntich et al. 2006; Myrseth et al. 2013). The Carlbring and Smit (2008) study displayed large and sustained treatment effects, with large effect sizes at post-treatment, 6-, 18-, 36-month follow-ups (ds = 0.83; 2.58; 1.96; 1.98). Within a separate study, the mean effect sizes of the primary outcome variables, reduction in alcohol consumption and alcohol-related problems, were slightly larger for the Internet-based application combined with face-to-face group meetings (d = 0.97) compared to face-to-face group meetings only (d = 0.96) (Hester et al. 2013). These large effect sizes were further demonstrated within Myrseth et al. (2013) study, as their findings suggested that the Internet-based intervention was associated with substantial improvement at post-treatment and follow-up (ds = 1.72; 1.68).
In contrast to these significant and large effect sizes, Japuntich et al.’s (2006) study yielded a large but insignificant treatment effect (OR = 1.59). However, it was concluded that the comparisons were similar or larger in magnitude to odds ratios in related research, as Strecher et al. (2005), found an OR of 1.34. One study investigated the effect sizes for the primary and secondary outcome measures at 3-month follow-up and indicated small effects for Internet-based self-help and small-to-medium effects for Internet-based interventions (Blankers et al. 2011). The difference in effect sizes was said to be due to the inclusion of chat-based therapy sessions, as this component substantially improved the treatment effects within the Internet-based intervention group. Given that conclusions about the treatment effectiveness are more easily drawn from effect sizes, it would be expected that future studies further facilitate this comparison and report the effect sizes of their interventions.
As a comparison cannot be made between the effect sizes of all the included studies, it is beneficial to highlight the abstinence rates as one way to compare intervention outcomes. Four studies reported no statistically significant results between interventions (Hester et al. 2013; Japuntich et al. 2006; King et al. 2009; Linke et al. 2012). Nonetheless, two studies comparing face-to-face therapy to online group therapy demonstrated that the Internet-based intervention and face-to-face therapy displayed both similar and high abstinence rates (Hester et al. 2013; King et al. 2009). Eight studies found significantly greater self-reported abstinence rates at the end of the treatment trial for participants in the Internet-based intervention when compared to controls (Blankers et al. 2011; Carlbring and Smit 2008; Myrseth et al. 2013; Woodruff et al. 2007) and different intervention groups (Abroms et al. 2008; Brendryen et al. 2008; Graham et al. 2011; Mermelstein and Turner 2006), with improvements being sustained at 3 to 18-month follow-ups. Positive treatment outcomes and high abstinence rates were also evident within four non-comparative online intervention studies (Carlbring et al. 2012; Castren et al. 2013; Hotta et al. 2007; Zbikowski et al. 2008).
Discussion
We identified 16 studies that examined the effect of Internet-based interventions to reduce addictive behaviours, including smoking cessation, opioid dependence, alcohol abuse and gambling. The review found consistent evidence across all trials that Internet-based interventions display positive treatment outcomes and benefits for participants. More specifically, twelve studies reported positive treatment outcomes for their Internet-based interventions (Abroms et al. 2008; Blankers et al. 2011; Brendryen et al. 2008; Carlbring et al. 2012; Carlbring and Smit 2008; Castren et al. 2013; Graham et al. 2011; Hotta et al. 2007; Mermelstein and Turner 2006; Myrseth et al. 2013; Woodruff et al. 2007; Zbikowski et al. 2008), four studies reported positive results for both treatment groups, however, there was no significant difference between these groups (Hester et al. 2013; Japuntich et al. 2006; King et al. 2009; Linke et al. 2012). Although the studies consistently displayed positive treatment effects, several methodological flaws were evident, in particular, the lack of a control or group in twelve of the studies, the reliance on self-report measures and the lack of consistency across the type of Internet-based interventions provided to participants. The studies found within this review provide support for the utilization of Internet-based interventions.
Positive treatment outcomes were noted for several addictive behaviours. Firstly, all the Internet-based studies targeting problem gamblers illustrated positive treatment outcomes on gambling behaviour (Carlbring et al. 2012; Carlbring and Smit 2008; Castren et al. 2013; Myrseth et al. 2013). Specifically, the majority of participants were regarded as recovered or improved at post-treatment, as there was a significant reduction in gambling behaviour (Carlbring et al. 2012; Carlbring and Smit 2008; Myrseth et al. 2013). In addition, significant reductions were evident in gambling related behaviour, gambling urges, negative social consequences and gambling related problems (Castren et al. 2013). All positive outcomes were noted to be present at follow-up, ranging from 3- to 36-months (Carlbring et al. 2012; Carlbring and Smit 2008; Castren et al. 2013; Myrseth et al. 2013). Of note, Myrseth et al. (2013) and Carlbring et al. (2012) did not employ a comparison treatment group and thus the positive effects found may be attributed to other factors, for example history, maturation, or to nonspecific treatment influences that could confound the results.
Several studies achieved positive Internet-based treatment outcomes on smoking behaviours, such as smoking fewer cigarettes and abstaining from smoking (Abroms et al. 2008; Brendryen et al. 2008; Graham et al. 2011; Hotta et al. 2007; Mermelstein and Turner 2006; Woodruff et al. 2007; Zbikowski et al. 2008). However, two studies concluded that there was no significant difference in abstinence rates between treatment groups (Japuntich et al. 2006; Linke et al. 2012). Japuntich et al. (2006) noted that a possible explanation for these findings might be due to the participant’s infrequent use of the online modules, as those reporting greater Internet usage were more likely to abstain from smoking.
Studies investigating the effectiveness of Internet-based programs on problem drinkers and opioid dependent patients, found face-to-face groups to be slightly more effective compared to Internet-based interventions (Hester et al. 2013; King et al. 2009). However, patients expressed a preference for Internet-based services, reporting convenience and increased confidentiality as major reasons (King et al. 2009). Blankers et al. (2011) concluded that the combination of an Internet-based intervention and proactive telephone calls is more effective at reducing alcohol consumption, compared to Internet-based intervention in conjunction with Internet-based forums. The positive effects for addictive behaviours found in the majority of studies and the preference reported for Internet-based therapy reflects the need for such services to exist. However, it is imperative to gain a better understanding of the types of programs that affect positive outcomes. In order to guide development of future treatment programs, studies should attempt to report on the individual effectiveness of treatment components and therapist contact.
The most commonly utilized Internet-based interventions were CBT and Motivational Interviewing (MI), both of which can be easily adapted into Internet-based interventions and have been used successfully in the treatment of addictions (Proudfoot et al. 2011). This is supported within the current review, as the majority of studies utilized CBT strategies within their programs (Abroms et al. 2008; Blankers et al. 2011; Brendryen et al. 2008; Carlbring et al. 2012; Carlbring and Smit 2008; Castren et al. 2013; Hester et al. 2013; Japuntich et al. 2006; Myrseth et al. 2013). Several programs also reported the inclusion of MI strategies, in order to complement CBT modules (Blankers et al. 2011; Carlbring and Smit 2008; Castren et al. 2013; Hester et al. 2013; Myrseth et al. 2013), while other studies implemented various MI strategies to complement studies utilizing behavioural approaches and peer-based social support (Graham et al. 2011; Hotta et al. 2007; Mermelstein and Turner 2006; Woodruff et al. 2007). The inclusion of MI within CBT centered therapy has been found to increase positive treatment outcomes for people with addiction (Freidenberg et al. 2002). MI attempts to enhance intrinsic motivation to change by exploring and resolving ambivalence (Carlbring et al. 2010), This is particularly important for those who have not reached the action phase of change and may not be ready to cease or reduce their problem behaviour (Monaghan and Blaszczynski 2009; Prochaska et al. 1992). This type of treatment enhancement has been supported by numerous studies, as both treatment outcomes and abstinent rates are higher in groups with MI (e.g. Hodgins et al. 2001). However, no study within the current review evaluated the difference between CBT and MI treatment outcomes.
Populations who are dealing with addictive disorders are noted to display high treatment attrition rates along with low uptake rates (McLellan 2006; Westphal 2006). This indicates the need for a change in therapy, as their needs are not currently being met. Internet-based interventions have resulted in lower attrition rates as compared to face-to-face treatment (King et al. 2009). Attrition rates varied across the identified studies, with dropout rates ranging from 7 to 42 %. This attrition rate is lower compared to face-to-face treatment, which was noted to be between 17 and 76 % (Ladouceur et al. 2001). Several factors have been suggested to contribute to higher response rates, such as therapist support, tailored email reminders, and a combination of email and telephone follow-ups (Danielsson et al. 2014).
The population and the particular characteristics of participants that would most benefit from Internet-based interventions was an issue evaluated within several studies. Women may be more likely to benefit from Internet-based interventions as they were more adherent to the overall intervention and utilized the Internet services significantly more than men (Mermelstein and Turner 2006; Zbikowski et al. 2008). Furthermore, middle-aged participants were more likely to use the Internet-based intervention services compared to younger participants (Japuntich et al. 2006; Zbikowski et al. 2008). However, the majority of studies in our review did not report demographic characteristics, making it difficult to evaluate which characteristics may have influenced treatment effectiveness, or which population these interventions are likely to be of most benefit. Future research should focus on evaluating which populations are more or less likely to benefit from technology-based interventions.
Although the evaluation of the literature was conducted in a systematic fashion, limitations remain, the first being the failure to complete a meta-analysis. This limited the review from being able to meaningfully interpret the pool of data obtained and ascertain the clinically relevant effects of this intervention. The current review is also limited by the lack of research conducted within this field. Despite the increasing number of studies being conducted within the digital arena few met the definition of being qualified as an Internet-based intervention. For example, the majority of excluded studies commonly employed self-help programs with no therapist input; subsequently the study was unable to fit the definition of an Internet-based intervention as outlined within this review.
Given the scarcity of research obtained within the review, there are a number of limitations, such as methodological flaws, within the studies collected. Firstly, the most common limitation noted was the inability of studies to make inferences about the success of the study, due to the lack of pure control groups, subsequently affecting the evaluation of the interventions effectiveness (Carlbring et al. 2012; Castren et al. 2013; Hotta et al. 2007; Zbikowski et al. 2008). Despite the increased utilization of Internet-based interventions, RCTs on their effectiveness are lacking. This is mainly attributed to the lack of pure control groups included within the selected studies. Although this can be seen as a methodological limitation, there are ethical concerns surrounding the allocation of participants to an intervention, denying those who want an intervention or asking participants to wait. At the outset of treatment, researchers commonly weigh up the importance of an ideal research design against the well-being of the participants (Jamison et al. 2006). Instead, different interventions are typically compared, commonly with a stepwise-design offering a different levels of support, for example web support, emails and telephone calls (Abroms et al. 2008; Brendryen et al. 2008; Graham et al. 2011; Hester et al. 2013; Japuntich et al. 2006; King et al. 2009; Mermelstein and Turner 2006) or no control/group (Carlbring et al. 2012; Castren et al. 2013; Hotta et al. 2007; Zbikowski et al. 2008). The difficulty of this undertaking was evident within Carlbring and Smit’s (2008) study, as comparisons between conditions were unable to be made at follow-up given that the wait-list group was eventually provided with therapy. However, subsequently, researchers are unable to ascertain whether the results may be accounted for by other factors, such as life changes.
Other limitations were the relatively small sample sizes of several studies (Carlbring and Smit 2008; King et al. 2009; Linke et al. 2012) and the recruitment of participants from restricted populations, such as university employees (Hotta et al. 2007), thus limiting the possible generalizability of the findings. Finally, the reliability and accuracy of the self-report measures used were addressed in several studies (Abroms et al. 2008; Blankers et al. 2011; Brendryen et al. 2008; Graham et al. 2011; Hester et al. 2013; Linke et al. 2012; Mermelstein and Turner 2006; Myrseth et al. 2013; Zbikowski et al. 2008), however this was an inherent limitation affecting the majority of studies. Some studies used objective methods such biochemical, for example saliva and urine, verification in addition to self-report measures, which limited the reliance on self-report data (Abroms et al. 2008; Japuntich et al. 2006; King et al. 2009; Linke et al. 2012; Mermelstein and Turner 2006). Future research should aim to address methodological concerns, such as measurement issues and the inclusion of pure control groups. For example, future studies should aim to include objective measures of abstinence, in order to confirm subjectively reported abstinent rates. The combination of these factors will assist in evaluating treatment component effectiveness. The criticisms outlined here are included to enable future research to extent the current research findings. However, it is important to note that clinical trials are difficult to execute and must balance providing appropriate treatment within the restraints of a treatment setting and limited funding with methodological rigour. It must be recognized that if it were not for the continuous efforts of these researchers, the development of Internet-based interventions and other online tools may not be so advanced.
Based on the studies reviewed, Internet-based interventions can have a positive effect on a range of clinical populations with addictive disorders. However, as this is a growing area of research, further research is required to examine the effect various forms of Internet-based interventions have on this clinical population. The current review aimed to lend credence to a new form of treatment that is currently available for problem gamblers, and has also been found to be quite successful in addressing other problems or concerns, such as low mood or anxiety (McCrone et al. 2004). Furthermore, this mode of therapy has been found to meet the needs of problem gamblers and reduce the barriers for help-seekers, subsequently providing imperative information to treatment providers, policy makers, and academic researchers. Support was found for Internet-based interventions, as it has the potential to enhance treatment uptake and outcomes in a sample of problem gamblers, with outcomes being sustained at follow-ups.
References
Abbott, J. M., Klein, B., & Ciechomski, L. (2008). Best practices in online therapy. Journal of Technology in Human Services, 26(2–4), 360–375. doi:10.1080/15228830802097257.
Abroms, L. C., Windsor, R., & Simons-Morton, B. (2008). Getting young adults to quit smoking: A formative evaluation of the x-pack program. Nicotine and Tobacco Research, 10(1), 27–33. doi:10.1080/14622200701767852.
Alderson, P. Green, S. & Higgins, J. P. T. (2004, June 2014). Cochrane reviewers’ handbook 4.2.2. Retrieved July 10th, 2014. http://www.cochrane.org/handbook
Andersson, G., Bergstrom, J., Hollandare, F., Carlbring, P., Kaldo, V., & Ekselius, L. (2005). Internet-based self-help for depression: Randomised controlled trial. British Journal of Psychiatry, 187, 456–461. doi:10.1080/15228830802094627.
Barak, A., & Grohol, J. M. (2011). Current and future trends in internet-supported mental health interventions. Journal of Technology in Human Services, 29, 155–196. doi:10.1080/15228835.2011.616939.
Barak, A., Hen, L., Boniel-Nissim, M., & Shapira, N. (2008). A comprehensive review and a meta-analysis of the effectiveness of internet based psychotherapeutic interventions. Journal of Technology in Human Services, 26, 109–160. doi:10.1080/15228830802094429.
Blankers, M., Koeter, M. W. J., & Schippers, G. M. (2011). Internet therapy versus internet self-help versus no treatment for problematic alcohol use: A randomized controlled trial. Journal of Consulting and Clinical Psychology, 79(3), 330–341. doi:10.1037/a0023498.
Brendryen, H., Drozd, F., & Kraft, P. (2008). A digital smoking cessation program delivered through internet and cell phone without nicotine replacement (happy ending): Randomized controlled trial. Journal of Medical Internet Research, 10(5), e51. doi:10.1111/j.1360-0443.2007.02119.x.
Carlbring, P., Degerman, N., Jonsson, J., & Andersson, G. (2012). Internet-based treatment of pathological gambling with a three-year follow-up. Cognitive Behaviour Therapy, 41(4), 321–334. doi:10.1080/16506073.2012.689323.
Carlbring, P., Ekselious, L., & Andersson, G. (2003). Treatment of panic disorder via the Internet: A randomized trial of CBT vs. applied relaxation. Journal of Behavior Therapy and Experiemental Psychiatry, 34(2), 129–140. doi:10.1016/S0005-7916(03)00026-0.
Carlbring, P., Jonsson, J., Josephson, H., & Forsberg, L. (2010). Motivational interviewing versus cognitive behavioral group therapy in the treatment of problem and pathological gambling: A randomized controlled trial. Cognitive Behaviour Therapy, 39(2), 92–103. doi:10.1080/16506070903190245.
Carlbring, P., & Smit, F. (2008). Randomized trial of internet-delivered self-help with telephone support for pathological gamblers. Journal of Consulting and Clinical Psychology, 76(6), 1090–1094. doi:10.1037/a0013603.
Castren, S., Pankakoski, M., Tamminen, M., Lipsanen, J., Ladouceur, R., & Lahti, T. (2013). Internet-based CBT intervention for gamblers in Finland: Experiences from the field. Scandinavian Journal of Psychology, 54(3), 230–235. doi:10.1111/sjop.12034.
Commission, Productivity. (2010). Gambling: Final report. Canberra: Government of Australia.
Cunningham, J. (2007). Translation of addictions science into practice. In P. Miller & D. Kavanagh (Eds.), Internet-based interventions for alcohol, tobacco and other substances of abuse (pp. 399–438). New York: Elsevier-Pergamon.
Danielsson, A.-K., Eriksson, A.-K., & Allebeck, P. (2014). Technology-based support via telephone or web: A systematic review of the effects on smoking, alcohol use and gambling. Addictive Behaviors, 39(12), 1846–1868. doi:10.1016/j.addbeh.2014.06.007.
DeAngelis, T. (2012). Practising distance therapy, legally and ethically. American Psychology Association. Monitor on Psychology, 43(3), 52.
Downs, S. H., & Black, N. (1998). The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. Journal of Epidemiology & Community Health, 52, 377–384.
Eidem, M. (2010). Addressing problem gambling: Some snapshots from Norway. Paper presented at the Discovery 2010 Conference, Toronto, ON.
Freidenberg, B. M., Blanchard, E. B., Wulfert, E., & Malta, L. S. (2002). Changes in physiological arousal to gambling cues among participants in motivationally enhanced cognitive–behavior therapy for pathological gambling: A preliminary study. Applied Psychophysiology and Biofeedback, 27(4), 251–260. doi:10.1023/A:1021057217447.
Gainsbury, S., & Blaszczynski, A. (2011a). Online self-guided interventions for the treatment of problem gambling. International Gambling Studies, 11(3), 289–308. doi:10.1080/14459795.2011.617764.
Gainsbury, S., & Blaszczynski, A. (2011b). A systematic review of internet-based therapy for the treatment of addictions. Clinical Psychology Review, 31, 490–498. doi:10.1016/j.cpr.2010.11.007.
Gainsbury, S., Hing, N., & Suhonen, N. (2014). Professional help-seeking for gambling problems: Awareness, barriers and motivators for treatment. Journal of Gambling Studies, 30(2), 503–519. doi:10.1007/s10899-013-9373-x.
Graham, A. L., Cobb, N. K., Papandonatos, G. D., Moreno, J. L., Kang, H., Tinkelman, D. G., & Abrams, D. B. (2011). A randomized trial of internet and telephone treatment for smoking cessation. Archives of Internal Medicine, 171(1), 46–53. doi:10.1001/archinternmed.2010.414.
Griffiths, K. M., Christensen, H., Jorm, A. F., Evans, K., & Groves, C. (2004). Effect of web-based depression literacy and cognitive-behavioural therapy interventions on stigmatising attitudes to depression: Randomised controlled trial. British Journal of Psychiatry, 185, 342–349. doi:10.1192/bjp.185.4.342.
Hay, C., & Kinnier, R. (1998). Homework in counseling. Journal of Mental Health Counseling, 20, 122–132.
Heron, K. E., & Smyth, J. M. (2010). Ecological momentary interventions: incorporating mobile technology into psychosocial and health behaviour treatments. British Journal of Health Psychology, 15(Pt 1), 1–39. doi:10.1348/135910709X466063.
Hester, R. K., Lenberg, K. L., Campbell, W., & Delaney, H. D. (2013). Overcoming addictions, a web-based application, and SMART recovery, an online and in-person mutual help group for problem drinkers, part 1: Three-month outcomes of a randomized controlled trial. Journal of Medical Internet Research, 15(7), e134. doi:10.2196/jmir.2565.
Hodgins, D. C., Currie, S. R., & el-Guebaly, N. (2001). Motivational enhancement and self-help treatments for problem gambling. Journal of Consulting and Clinical Psychology, 69(1), 50–57. doi:10.1037/0022-006X.69.1.50.
Hotta, K., Kinumi, K., Naito, K., Kuroki, K., Sakane, H., Imai, A., & Tobe, K. (2007). An intensive group therapy programme for smoking cessation using nicotine patch and internet mailing supports in a university setting. International Journal of Clinical Practice, 61(12), 1997–2001. doi:10.1111/j.1742-1241.2007.01466.x.
Jamison, D. T., Breman, J. G., Measham, A. R., Alleyne, G., Claeson, M., Evans, D. B., & Musgrove, P. (2006). Diseease control priorities in developing countries (2nd ed.). Washington (DC): World Bank.
Japuntich, S. J., Zehner, M. E., Smith, S. S., Jorenby, D. E., Valdez, J. A., Fiore, M. C., & Gustafson, D. H. (2006). Smoking cessation via the internet: A randomized clinical trial of an internet intervention as adjuvant treatment in a smoking cessation intervention. Nicotine and Tobacco Research, 8(Suppl 1), S59–S67. doi:10.1080/14622200601047900.
Kenwright, M., & Marks, I. M. (2004). Computer-aided self-help for phobia/panic via Internet at home: A pilot study. The British Journal of Psychiatry, 164(5), 448–449. doi:10.1192/bjp.184.5.448.
King, V. L., Stoller, K. B., Kidorf, M., Kindbom, K., Hursh, S., Brady, T., & Brooner, R. K. (2009). Assessing the effectiveness of an Internet-based videoconferencing platform for delivering intensified substance abuse counseling. Journal of Substance Abuse Treatment, 36(3), 331–338. doi:10.1016/j.jsat.2008.06.011.
Ladouceur, R., Gosselin, P., Laberge, M., & Blaszczynski, A. (2001). Dropouts in clinical research: Do results reported reflect clinical reality? Behavior Therapist, 24, 44–46.
Lester, D. (2006). E-therapy: Caveats from experiences with telephone therapy. Psychological Reports, 99, 894–896. doi:10.2466/PR0.99.3.894-896.
Linke, S. E., Rutledge, T., & Myers, M. G. (2012). Intermittent exercise in response to cigarette cravings in the context of an internet-based smoking cessation program. Mental Health and Physical Activity, 5(1), 85–92. doi:10.1016/j.mhpa.2012.02.001.
McCrone, P., Knapp, M., Proudfoot, J., Ryden, C., Cavanagh, K., Shapiro, D. A., & Tylee, A. (2004). Cost-effectiveness of computerised cognitive-behavioural therapy for anxiety and depression in primary care: Randomised controlled trial. The British Journal of Psychiatry, 185, 55–62. doi:10.1192/bjp.185.1.55.
McLellan, A. (2006). What we need is a system: Creating a responsive and effective substance abuse treatment system. In W. R. Miller & K. M. Carroll (Eds.), Rethinking substance abuse: What the science shows, and what we should do about it. New York: Guildford Press.
Mermelstein, R., & Turner, L. (2006). Web-based support as an adjunct to group-based smoking cessation for adolescents. Nicotine and Tobacco Research, 8(Suppl1), S69–S76. doi:10.1080/14622200601039949.
Monaghan, S., & Blaszczynski, A. (2009). Internet-based intervnetions for the treatment of problem gambling. Toronto: Centre for Addiction and Mental Health.
Myrseth, H., Brunborg, G. S., Eidem, M., & Pallesen, S. (2013). Description and pre-post evaluation of a telephone and internet based treatment programme for pathological gambling in Norway: A pilot study. International Gambling Studies, 13(2), 205–220. doi:10.1080/14459795.2012.759610.
Prochaska, J. O., DiClemente, C. C., & Norcross, J. C. (1992). In search of how people change: Applications to addictive behaviors. American Psychologist, 47(9), 1102–1114. doi:10.1037/0003-066X.47.9.1102.
Proudfoot, J., Klein, B., Barak, A., Carlbring, P., Cuijpers, P., Lange, A., & Andersson, G. (2011). Establishing guidelines for executing and reporting internet intervention research. Cognitive Behaviour Therapy, 40(2), 82–97. doi:10.1080/16506073.2011.573807.
Skinner, A. E. G., & Latchford, G. (2006). Attitudes to counselling via the Internet: A comparison between in-person counselling clients and Internet support group users. Counselling and Psychotherapy Research, 6, 158–163. doi:10.1080/14733140600853641.
Strecher, V. J., Shiffman, S., & West, R. (2005). Randomised controlled trial of a web-based computer-tailored smoking cessation program as a supplement to nicotine patch therapy. Addiction, 100, 682–688. doi:10.1111/j.1360-0443.2005.01093.x.
Wells, M., Mitchell, K. J., Finkelhor, D., & Becker-Blease, K. A. (2007). Online mental health treatment: Concerns and considerations. CyberPsychology and Behavior, 10, 453–459. doi:10.1089/cpb.2006.9933.
Westphal, J. (2006). Attrition among gambling treatment patients: Clinical and research implications. Paper presented at the Internation Gambling Conference, Auckland, New Zealand.
Woodruff, S. I., Conway, T. L., Edwards, C. C., Elliott, S. P., & Crittenden, J. (2007). Evaluation of an internet virtual world chat room for adolescent smoking cessation. Addictive Behaviors, 32(9), 1769–1786. doi:10.1016/j.addbeh.2006.12.008.
Zbikowski, S. M., Hapgood, J. Smucker, Barnwell, S., & McAfee, T. (2008). Phone and web-based tobacco cessation treatment: Real-world utilization patterns and outcomes for 11,000 tobacco users. Journal of Medical Internet Research, 10(5), e41. doi:10.2196/jmir.999.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Chebli, JL., Blaszczynski, A. & Gainsbury, S.M. Internet-Based Interventions for Addictive Behaviours: A Systematic Review. J Gambl Stud 32, 1279–1304 (2016). https://doi.org/10.1007/s10899-016-9599-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10899-016-9599-5