
Abstract
Prenatal genetic counselors are health care professionals who counsel women making reproductive decisions which include decisions such as terminating pregnancies due to fetal anomalies. Little is known about the experiences and practices of prenatal genetic counselors working with women who have the option of termination after 24 weeks gestation. In this national survey of 168 genetic counselors who have practiced prenatal genetic counseling, we asked about their general practice patterns, including indications for which termination is offered and types of abortion care services that are coordinated by genetic counselors. We report respondents’ self-assessments of level of understanding of federal abortion law and abortion procedures. Seventy-six percent of respondents have offered and counseled on termination after 24 weeks and 93% of respondents believe it is the responsibility of the counselor to discuss this option with patients. However, one-third report that they have some or no understanding of the procedures and three-quarters report that they have some or no understanding of federal abortion law. The results of this study provide insight into knowledge and experiences of genetic counselors working with these patients, allowing for improved genetic counselor training and continuing education to provide better guidance and develop more effective means of assisting patients.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Genetic counselors are masters-prepared professionals trained in medical genetics and counseling; prenatal genetic counselors work with women who have an increased chance of having a child with a birth defect or genetic condition, some of whom may decide to terminate due to genetic and medical anomalies. The American College of Obstetricians and Gynecologists (ACOG) recommends that all pregnant women be offered screening or diagnostic testing for aneuploidy and neural tube defects, noting that prenatal genetic testing allows the opportunity to decide to terminate a pregnancy (Cheschier & Bulletins-Obstetrics 2003; Committee on Practice Bulletins-Obstetrics 2016). The National Society of Genetic Counselors (NSGC) supports the right of all individuals and couples to make reproductive choices, which includes using information from genetic counseling or testing to decide whether to end a pregnancy (NSGC Position Statement 2013).
In the United States, abortion is allowable in the third trimester based on the medical judgment of a patient’s attending physician (Roe v. Wade 1973). The third trimester of a pregnancy can be approximated to start at week 25 and is a stage at which a fetus may be viable with or without medical intervention (Chervenak and McCullough 1997; Hack and Fanaroff 1989). Studies have found that the types of fetal abnormalities that lead to abortion after 24 weeks predominantly include conditions in which the fetus is either unlikely to survive or is expected to have a severely compromised quality of life (Barel et al. 2009; Bosma et al. 1997; Drummond et al. 2003;). However, a study has shown that maternal fetal medicine specialists do not always concur on what constitutes a lethal anomaly (Jacobs et al. 2015). Other studies have identified the situational reasons that the termination was performed after 24 weeks rather than earlier in the pregnancy. One reason is that the fetal prognosis is unclear, therefore necessitating a more thorough evaluation to avoid unnecessary termination in the first or second trimester (Dommergues et al. 1999). Other reasons are a lack of early prenatal screening, parents taking time to make decisions about testing, and anomalies that developed later on in the pregnancy (Barel et al. 2009; Dommergues et al. 1999). Considering their professional responsibilities, one would expect prenatal genetic counselors to be primary health care providers for counseling on late-term termination.
Advances in genetic testing have increased the number and complexity of prenatal screening and testing options, challenging genetic counselors to provide adequate teaching and counseling of options, expectations, and follow-up (Norton 2008). Information about fetal abnormalities can be difficult for a patient to understand (Asplin et al. 2011; Koponen et al. 2012), but there is relief at having the opportunity to make the decision to continue a pregnancy or not (Bryar 1997; Ferreira da Costa et al. 2005; Gammeltoft et al. 2008). The decision to terminate is viewed as choosing between two unwanted options, with grief and isolation further exacerbated by stigma of abortion and disability (McCoyd 2007). Adding to the complexity of the situation, increasing costs with gestational age, distance, and harassment, are documented barriers to termination (Henshaw 1995). Such barriers greatly impact patient care and stratify patients based on resources (Dehlendorf et al. 2010). Lafarge et al. (2014) found that the role of health professionals is an important theme in women’s experiences with termination for fetal abnormality, and that timely, unbiased, and clear information about the fetal findings and termination procedures is valued by the patient (Asplin et al. 2011; Gammeltoft et al. 2008; Kerns et al. 2012). The review concluded that many women found their care pathway fragmented, suggesting that patient care could be improved by the development and implementation of structured, coordinated paths to care.
Terminating a pregnancy after 24 weeks gestation is a complex choice for the patient; it is imperative that genetic counselors provide appropriate medical information, expectations, and options for patients to assist the decision making process. We surveyed prenatal genetic counselors to investigate if they offer abortion after 24 weeks, the medical indications for termination, and their self-reported understanding of federal abortion law and termination procedures. This research aims to examine practices and knowledge of genetic counselors to potentially identify areas for improved counseling around this difficult decision.
Methods
Participants
We recruited subjects through the Student Research Survey Program of the National Society of Genetic Counselors (NSGC) in February 2013. We sent an email to NSGC members, an organization that includes students and practicing professionals. We excluded genetic counselors who had not practiced prenatal counseling and students.
Procedures
This study was approved by California State University, Stanislaus Institutional Review Board. The email described the purpose of the study and included a link to the survey. Participants gave informed consent by opening the link. We administered the survey through Research Electronic Data Capture (REDCap), a secure online survey platform. To ensure privacy, the surveys were anonymous and collected no identifying information. The survey remained open for thirty days following the initial invitation, and a second invitation was sent a week before closing.
Instrumentation
The survey was written by two authors with input and suggestions from the third author. All authors have experience with counseling women about termination for anomalies. We piloted the study among seven genetic counselors, two genetics department assistants, and one medical geneticist. The 18-question survey focused on prenatal genetic counselors’ practice patterns around and understanding of abortion after 24 weeks. We asked demographics (gender, age, years in prenatal practice, state location, and religious affiliation); if respondents had ever offered the option of abortion after 24 weeks and, if so, the indication for the abortion. Respondents could select from seven indications or “other” and asked to describe the indication. Respondents could choose more than one indication. We asked respondents to self-assess their knowledge regarding abortion law in the US and abortion procedures, each with four answer options from which to choose: understand very well, understand well, some understanding, no understanding.
Data Analysis
We analyzed the data using SPSS Statistics Version 20. Descriptive statistics, including frequencies, means, medians, standard deviations, and standard errors were calculated for demographic variables. We used demographics as predictors for understanding of abortion law and procedures. We report descriptive statistics and use independent t tests and chi square tests to analyze predictors for offering the option of abortion after 24 weeks gestation. Bivariate analyses were used to test the relationships between the demographic variables and understanding of abortion law and procedures.
Results
Of 2815 practicing members of the NSGC (NSGC PSS 2012), 168 (6.0%) counselors responded. Respondents ranged in age from 24 to 63 years old, with a mean age of 37.1 years (SD = 9.8) (Table 1). All respondents were from the United States and represented 32 states, which were further divided into regions for analysis. We categorized each state into a region (West, South, Northeast, or Midwest) based on the regions listed in the United States Census Bureau ( Statistical Abstract of the United States 2012. N.p.: United States Govt Printing Office 2011. Web.). Over one-third of the respondents were from the West; the rest were equally distributed between the Northeast, Midwest, and South. Years in prenatal genetic counseling practice ranged from less than one year to more than 30 years, with a median of 6.25 years. The response rate and demographic characteristics are similar to other publications on surveys of genetic counselors (Balcom et al. 2013; Enns et al. 2010) and the mean age of respondents in this study is similar to the respondents to the NSGC professional status survey, which found the majority of respondents to be in the age group of 29 to 39 years (NSGC PSS 2012).
All genetic counselors reported being aware that third-trimester abortion services existed. A number of respondents specifically referenced Boulder Abortion Clinic in Boulder, Colorado. Services in New Mexico, Kansas (as a past site), and “out of state” or a “neighboring state” were also mentioned.
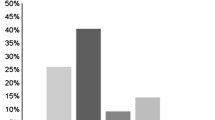
One hundred and forty-two (84.4%) of the respondents reported they have offered abortion after 24 weeks. Of these respondents, some provided specific descriptions of medical indications (Table 2). Some medical indications can be included in more than one category (for example, trisomy 13 may be considered both lethal and a chromosomal abnormality) and respondents were able to select more than one answer. The most common medical reason for offering this option to patients was for lethal anomalies (n = 121) (Fig. 1). Among the 26 (15.6%) who reported never having offered a third-trimester abortion, 21 (80.0%) reported not encountering the situation in their practice, 5 (19.2%) reported that it is not a feasible option for their patients, 1 (3.8%) did not know it was an option, and 1 (3.8%) reported not being comfortable with the option.

Medical indications for offering termination after 24 weeks gestation
Table 3 displays the proportions of respondents who have or have not offered termination after 24 weeks, by demographic characteristics. Age, years in practice, religious affiliation, and understanding of law or procedures were not found to be significant predictors of offering the option. Geographic location approached significance (p = 0.08), with the West having the most respondents who have offered termination after 24 weeks (94.6%).
Understanding of Abortion Law
We asked respondents about their level of understanding of Federal abortion law after 24 weeks gestation in the United States. Over half of respondents reported having some understanding of abortion law (58.3%), while very few reported understanding the law very well (7.7%). For further analysis, we collapsed understanding of abortion law after 24 weeks into two categories: understand well or very well (25.6%) and some or no understanding (74.4%) and used demographics variable as predictors. Geographic location was the only significant predictor of understanding of abortion law (p = 0.03) (Table 4).
Understanding of Abortion Procedures
One hundred sixty-six (98.8%) genetic counselors reported their level of understanding of the induction termination procedure and 165 (98.2%) reported their level of understanding of the D&E procedure (Fig. 2).

Respondents’ understanding of abortion procedures
We collapsed understanding of induction termination and D&E into two groups: understand well or very well versus some or no understanding. We used demographic variables as predictors of respondents’ understanding of either procedure. The number of years in practice was the only significant predictor associated with understanding of induction termination, with the average number of years in practice of respondents who understand the procedure well or very well at 11.4 years versus 6.4 years among those who reported some or no understanding of the procedure (p = 0.02). For understanding of D&E, years in practice approached significance (p = 0.06) as those reporting they understand the procedure well or very well were in practice for a mean of 10.9 years versus 6.9 years among those reporting some or no understanding of the procedure (Table 5).
Direct Involvement with Patient Care
The majority of respondents identified genetic counselors (93.5%) as the providers who discuss termination options after 24 weeks with patients, followed by other prenatal care providers such as a perinatologist, obstetrician, or nurse practitioner (62.5%) (respondents were allowed to choose multiple options). Six (3.6%) of the respondents reported that the option is not discussed at their workplace. Of those six, one specified that terminations after 24 weeks are not covered by insurance. Another respondent commented, “We don't do much prenatal and I don't think it's ever come up. I know our organization does not provide or cover abortion in any circumstance, so patients would have to go elsewhere and probably pay out of pocket.”
Ninety-five of the 167 (56.9%) respondents reported that they had been involved in coordinating third-trimester abortion services. Many respondents described referrals to out-of-state providers such as the Boulder Abortion Clinic. Other types of coordination care included compiling patient packets, sending medical records, coordinating airfare and hotel arrangements, and coordinating funding assistance. Respondents also provided reasons for not coordinating care, including not being financially feasible for the patient, the facility did not provide these services, or the patient did not pursue this option.
Respondents were asked their perceptions of barriers that patients face when considering third-trimester abortion services (Fig. 3). Barriers described by respondents include the patient’s own personal beliefs, family beliefs, dangers to the mother (lack of experienced providers, future conception), and societal beliefs. One respondent’s comment within the “other” category is as follows: “Patients may have to travel long distances at their own expense. Not all doctors support this procedure and will not necessarily even present the option to patients. Family members may be opposed to the procedure and may pressure the patient not to have the procedure.” (Respondent 113). Some genetic counselors expressed frustration in their comments; for example, one respondent said, “Out-of-state options are incredibly expensive. I often feel angry when our 'medicaid' patients would opt for late termination of pregnancy but they cannot afford it. This is an inequality that infuriates me profoundly.” (Respondent 38).

Reported patient-related barriers to accessing third-trimester abortion services
Discussion
The results from this survey show that offering the option of abortion after 24 weeks gestation is not uncommon in the prenatal genetic counseling practice and is offered for medical anomalies and genetic disorders. This information is valuable because it helps identify practical experiences and possible gaps in knowledge of abortion law and procedures, which can be used to improve counseling strategies.
“Lethal anomalies” was the most common reason given for discussing abortion after 24 weeks. This is not surprising, given that restrictions to termination vary by state and many states limit abortion after 24 weeks to lethal anomalies only (Guttmacher Institute 2013b, 3). Some indications have unclear severity or prognosis (for example, “severe” hydrocephaly). There were also indications that are not lethal or severe, like trisomy 21. Indications coincide with previous studies. Only 15.6% of respondents reported that they had not offered the option of abortion after 24 weeks, with the most common reason being that the respondent had not encountered the situation in their practice. This finding is not explained by these respondents having had fewer years in practice. It is unclear if a lack of concordance among medical professionals on what constitutes a “lethal” anomaly (Jacobs et al. 2015) contributes to variation in practice among respondents. It is possible that these respondents have encountered similar serious medical indications but were unaware that other genetic counselors offered abortion for those indications or disagreed on what constitutes “lethal,” “severe,” or “appropriate.”
All of the respondents claimed to be aware of third-trimester abortion services and the majority had offered this option in practice, yet most respondents report limited understanding of federal abortion law after 24 weeks gestation. Respondents from the South were the most likely to report a better understanding of abortion law. Approximately one-third of respondents reported only having “some understanding” of abortion procedures. The number of years in practice was associated with better understanding of procedures, with respondents reporting a better understanding the longer they had been in practice. This is to be expected considering that, over time, the situation may have occurred more often in one’s practice, increasing counseling opportunities. Interestingly, while a lack of understanding of abortion law and procedures is evident, 93.5% of respondents claimed that genetic counselors are the health care providers responsible for discussing this option with patients, and 56.9% of respondents had been directly involved with coordinating care for patients. Genetic counselors’ experiences provide valuable perspectives on the barriers that patients face. Abortion after 24 weeks gestation is an expensive procedure, typically costing thousands of dollars in addition to possible out-of-state travel (Guttmacher Institute 2013a, 1; Jones et al. 2008); therefore it is not surprising that most respondents reported financial difficulty and travel to be barriers to accessing these services. Considering expressed needs of patients (Asplin et al. 2011; Gammeltoft et al. 2008; Kerns et al. 2012), this high level of involvement necessitates that genetic counselors be knowledgeable in all aspects of abortion after 24 weeks in order to offer timely, unbiased information. It has been shown that patients report difficulty in both understanding ultrasound findings and in deciding to continue or end a pregnancy for fetal abnormality (Asplin et al. 2011; Koponen et al. 2012; Lafarge et al. 2014); these differences in practice and level of genetic counselors’ understanding may add to an already-reported fragmented care pathway.
Research Recommendations
Further research into counselors’ personal opinions and beliefs about abortion after 24 weeks may help clarify variations in practice. When asking counselors why they had not offered abortion after 24 weeks, we provided an option of not being comfortable. However, we did not ask specific reasons why they felt uncomfortable, or how strongly they felt about it. Relatedly, how counselors feel about offering the option for lethal versus non-lethal indications could be explored. Interviews of patients’ personal experiences would aid in understanding the psychosocial and practical support needs of patients.
Educational Recommendations
Genetic counselors vary in their self-perceived understanding of federal abortion law and abortion procedures, indicating the need for increased education in these areas. Less-experienced counselors expressed less familiarity with procedures, highlighting an area in which students could benefit from more training. Federal law on abortion after 24 weeks, places where abortion services exist, barriers to optimum patient care, and abortion procedures should be specifically addressed as part of graduate curriculum and continuing education.
Clinical Recommendations
Abortion after 24 weeks needs to be considered when discussing the implications of prenatal screening and diagnosis with earlier access and results desirable to avoid some of these described barriers. Genetic counselors and other healthcare providers should work together to maintain open dialogue about abortion counseling practices and expectations to provide improved training and continuing education and address the barriers to options. Prenatal diagnostic centers could implement standard operating procedures and identify resource gaps relevant to the particular patient population and geography to improve the care pathway for patients as individuals and for patient care overall.
Study Limitations
A limitation to this study is that respondents were self-selected which may have led to a response bias towards genetic counselors that have an increased interest in this topic or have worked with patients who have made the decision to have an abortion after 24 weeks gestation. The results may not fully reflect the views and experiences of all prenatal genetic counselors. Another limitation is that, because respondents provided a self-assessment of level of understanding of third trimester abortion law and procedures, their true understanding may differ from their self-perceived understanding, as self-report is not a validated measure. Respondents may have been reluctant to share ignorance or overstate knowledge. We asked genetic counselors to participate if they had practiced prenatal counseling at any point in their career but did not ask if they were currently practicing; therefore it was not possible to assess if there was variation in responses between currently- or formerly-practicing counselors. We did not ask participants about their patient volume or whether their primary specialty was prenatal practice; the contribution of those variables to counselor’s knowledge and understanding of law and procedures is unclear.
Conclusions
To our knowledge this study represents the only survey of genetic counselors’ practices with patients that face the decision of termination of pregnancy after 24 weeks gestation and suggests that genetic counselors view themselves as primary healthcare providers in this situation. Genetic counselors have significant knowledge of the indications for termination and the barriers to appropriate healthcare options. A notable self-perceived lack of understanding of abortion laws and procedures indicated in this study demonstrates the need for education in these areas, as understanding the utility and limitations of the option is an important part of a genetic counselor’s skill set. This need will continue to increase with the growing interest in and demand for prenatal screening and diagnosis.
References
Asplin, N., Wessel, H., Marions, L., & Georgsson Ohman, S. (2011). Pregnant Women’s Experiences, Needs, and Preferences Regarding Information about Malformations Detected by Ultrasound Scan. Sexual and Reproductive Healthcare, 3(2), 73–78.
Balcom, J. R., Veach, P. M., Bemmels, H., Redlinger-Grosse, K., & Leroy, B. S. (2013). When the Topic is you: Genetic Counselor Responses to Prenatal Patients’ Requests for Self Disclosure. Journal of Genetic Counseling, 22(3), 358–373.
Barel, O., Vaknin, Z., Smorgick, N., Reish, O., Mendlovi, S., Herman, A., & Maymon, R. (2009). Fetal abnormalities leading to third trimester abortion: nine year experience from a single medical center. Prenatal Diagnosis, 29, 223–228.
Bosma, J., van der Wal, G., & Hosman-Benjaminse, S. L. (1997). Late termination of pregnancy in North Holland. British Journal of Obstetrics and Gynaecology, 104, 478–487.
Bryar, S. (1997). One Day You’re Pregnant and One Day You’re Not: Pregnancy Interruption for Fetal Anomalies. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 26(5), 559–566.
Chervenak, F. A., & McCullough, L. B. (1997). The limits of viability. Journal of Perinatal Medicine, 25, 418–420.
Cheschier, N., & Bulletins-Obstetrics, A. C. o. P. (2003). ACOG practice bulletin. Neural tube defects. Number 44, July 2003. (Replaces committee opinion number 252, March 2001). Int J Gynaecol Obstet, 83(1), 123–133. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/14626221. Accessed 14 Aug 2017
Committee on Practice Bulletins-Obstetrics, C. o. G., & the Society for Maternal-Fetal, M. (2016). Practice Bulletin No. 163: Screening for Fetal Aneuploidy. Obstet Gynecol, 127(5), e123–137. https://doi.org/10.1097/AOG.0000000000001406.
Dehlendorf, C., Rodriguez, M. I., Levy, K., Borrero, S., & Steinauer, J. (2010). Disparities in Family Planning. American Journal of Obstetrics and Gynecology, 202(6), 214–220.
Dommergues, M., Benachi, A., Benifla, J., des Noettes, R., & Dumez, Y. (1999). The reasons for termination of pregnancy in the third trimester. British Journal of Obstetrics and Gynaecology, 106, 297–303.
Drummond, C. L., Molina Gomes, D., Senat, M. V., Audibert, F., Dorion, A., & Villie, Y. (2003). Fetal karyotyping after 28 weeks of gestation for late ultrasound findings in a low risk population. Prenatal Diagnosis, 23, 1068–1072.
Enns, E. E., Boudreault, P., & Palmer, C. G. S. (2010). Examining the Relationship Between Genetic Counselors’ Attitudes Towards Deaf People and the Genetic Counseling Session. Journal of Genetic Counseling, 19(20), 161–173.
Ferreira da Costa, L., Hardy, E., Duarte Osis, M. J., & Faundes, A. (2005). Termination of Pregnancy for Fetal Abnormality Incompatible with Life: Women’s Experiences in Brazil. Reproductive Health Matters, 13(26), 139–146.
Gammeltoft, T., Tran, M. H., Nguyen, T. H., & Nguyen, T. T. H. (2008). Late-Term Abortion for Fetal Anomaly: Vietnamese Women’s Experiences. Reproductive Health Matters, 16(31 Suppl), 46–56.
Guttmacher Institute (2013a). (1) "State Policies in Brief. An Overview of Abortion Laws." www.guttmacher.org . N.p., 21 Mar. 2013. Web. <http://www.guttmacher.org.ezproxy.lib.csustan.edu:2048/statecenter/spibs/spib_OAL.pdf>.
Guttmacher Institute (2013b). (3) "State Policies in Brief. State Policies on Later Abortion." www.guttmacher.org . N.p., 21 Mar. 2013. Web. <http://www.guttmacher.org.ezproxy.lib.csustan.edu:2048/statecenter/spibs/spib_PLTA.pdf>.
Hack, M., & Fanaroff, A. A. (1989). Outcomes of extremely low-birthweight infants between 1982 and 1988. New England Journal of Medicine, 312, 1642–1647.
Henshaw, S. K. (1995). Factors Hindering Access to Abortion Services. Family Planning Perspectives, 27(2), 54–59.
Jacobs, A. R., Dean, G., Wasenda, E. J., Porsch, L. M., Moshier, E. L., Luthy, D. A., & Paul, M. E. (2015). Late Termination of Pregnancy for Lethal Fetal Anomalies: A National Survey of Maternal-Fetal Medicine Specialists. Contraception, 91(1), 12–18.
Jones, R. K., Zolna, M. R., Henshaw, S. K., & Finer, L. N. (2008). Abortion in the United States: Incidence and Access to Services, 2005. Perspectives in Sexual and Reproductive Health, 40, 6–16.
Kerns, J., Vanjani, R., Freedman, L., Mechstroch, K., Drey, E. A., & Steinauer, J. (2012). Women’s Decision Making Regarding Choice of Second Trimester Termination Method for Pregnancy Complications. International Journal of Gynecology and Obstetrics, 116(3), 244–248.
Koponen, K., Laaksonen, K., & Vehkakoski, T. (2012). Parental and Professional Agency in Terminations for Fetal Anomalies: Analysis of Finnish Women’s Accounts. Scandinavian Journal of Disability Research, 15(1), 33–44.
Lafarge, C., Mitchell, K., & Fox, P. (2014). Termination of Pregnancy for Fetal Abnormality: A Meta-ethnography of Women’s Experienced. Reproductive Health Matters, 22(44), 191–201.
McCoyd, J. L. M. (2007). Pregnancy Interrupted: Loss of a Desired Pregnancy After Diagnosis of Fetal Anomaly. Journal of Psychosomatic Obstetrics and Gynecology, 28(1), 37–48.
National Society of Genetic Counselors Position Statements. (2013) Retrieved from http://www.nsgc.org/p/bl/et/blogaid=35.
National Society of Genetic Counselors. (2012). 2012 Professional status survey: executive summary. Retrieved 2013 from http://www.nsgc.org.
Norton, M. E. (2008). Genetic Screening and Counseling. Current Opinion in Obstetrics and Gynecology, 20(2), 157–163.
Roe v Wade, 410 U.S. 113, 164–165 (1973).
United States Census Bureau. “Census Regions and Divisions of the United States.” Census.goc. N.p. (2011). Web. Retrieved from https://www2.census.gov/geo/pdfs/maps-data/maps/reference/us_regdiv.pdf.
Acknowledgements
This study was conducted in partial fulfillment of the requirements for the first author’s degree of Master of Science in Genetic Counseling.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Rachel Graziani, Laurie Nemzer, and Jennifer Kerns declare that they have no conflict of interest.
Human Studies and Informed Consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all patients for being included in the study.
Animal Studies
No animal studies were carried out by the authors for this article.
Electronic supplementary material
ESM 1
(DOCX 16 kb)
Rights and permissions
About this article

Cite this article
Graziani, R.N.A., Nemzer, L. & Kerns, J. The Experience of Genetic Counselors Working with Patients Facing the Decision of Pregnancy Termination after 24 Weeks Gestation. J Genet Counsel 27, 626–634 (2018). https://doi.org/10.1007/s10897-017-0151-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10897-017-0151-2