
Abstract
Direct-to-consumer personal genomic testing (DTC-PGT) results lead some individuals to seek genetic counseling (GC), but little is known about these consumers and why they seek GC services. We analyzed survey data pre- and post-PGT from 1026 23andMe and Pathway Genomics customers. Participants were mostly white (91%), female (60%), and of high socioeconomic status (80% college educated, 43% household income of ≥$100,000). After receiving PGT results, 43 participants (4%) made or planned to schedule an appointment with a genetic counselor; 390 (38%) would have used in-person GC had it been available. Compared to non-seekers, GC seekers were younger (mean age of 38 vs 46 years), more frequently had children <18 (26% vs 16%), and were more likely to report previous GC (37% vs 7%) and genetic testing (30% vs 15%). In logistic regression analysis, seeking GC was associated with previous GC use (OR = 6.5, CI = 3.1–13.8), feeling motivated to pursue DTC-PGT for health reasons (OR = 4.3, CI = 1.8–10.1), fair or poor self-reported health (OR = 3.1, CI = 1.1–8.3), and self-reported uncertainty about the results (OR = 1.8, CI = 1.1–2.7). These findings can help GC providers anticipate who might seek GC services and plan for clinical discussions of DTC-PGT results.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Direct-to-consumer personal genomic testing (DTC-PGT) gives people commercial access to personalized genomic information that ranges from ancestry and physical traits to carrier status, medication response, and disease risk. With the DTC approach, testing is initiated by the individual and generally does not require involvement of a healthcare provider. Many tests offered DTC are not considered standard of care and most are not offered in genetics clinics (Caulfield and McGuire 2012; Hock et al. 2011; Uhlmann and Sharp 2012). Its limited clinical validity and utility and the lack of involvement of medical intermediaries have made DTC-PGT the subject of controversy since its inception (Gutierrez 2013; Mathews et al. 2012; Wade and Wilfond 2006).
Proponents of DTC-PGT argue that individuals have a right to direct access to their personal genomic information. However, others are concerned that obtaining such information without a qualified medical intermediary to assist with pre-test counseling, informed consent, and report interpretation could be harmful, with the potential for misinterpretation of test results and distress from unexpected findings (Gutierrez 2013; Roberts and Ostergren 2013). The clinical validity and utility of SNP-based risk profiling for common diseases offered through DTC services is not well established at this time. Most of the SNPs analyzed have a very small effect size and DTC-GT companies are sometimes not consistent in the SNPs they report, resulting in differing risk estimates (Bunnik et al. 2015; Kalf et al. 2014). Of note, evidence of harm caused by DTC-PGT is limited (Dohany et al. 2012) and several studies have found no difference between baseline and follow-up anxiety symptoms among DTC-PGT customers (Bloss et al. 2011; Bloss et al. 2013; Darst et al. 2013; Francke et al. 2013; James et al. 2011).
Some of these concerns led the Food and Drug Administration (FDA) in 2013 to send a warning letter to the DTC-PGT company 23andMe, ordering them to immediately stop marketing until they obtained official authorization (Gutierrez 2013). At that time, 23andMe removed the health-related testing from products sold to US customers, but continued to offer ancestry and trait testing. Then in 2015, the FDA approved 23andMe’s marketing of a carrier test for Bloom syndrome after the company had provided study data indicating that the test had sufficient accuracy in detecting carrier status and that consumers could understand test instructions and results when provided in a DTC format (Gutierrez 2013). Further, the FDA indicated that related carrier screening tests for autosomal recessive disorders would be exempt from their premarket review process, opening the door for 23andMe and other companies to market this particular type of genetic test in a DTC format. In April 2017, the FDA allowed 23andMe to market tests for 10 additional diseases or conditions, including Parkinson’s disease, late onset Alzheimer’s disease, and Celiac disease (FDA 2017).
The above concerns about DTC-PGT prompted genetics professional societies, including the American College of Medical Genetics and Genomics (ACMG), the American Society of Human Genetics (ASHG), and the National Society of Genetic Counselors to issue position statements. These statements all advocate for the involvement of genetics professionals in the testing process (ACMG Board of Directors 2015; Hudson et al. 2007; NSGC Executive Office 2015). NSGC supports the right of individuals to pursue DTC-PGT provided the choice is autonomous and informed, but maintains that companies offering DTC-PGT have a duty to make genetics professionals easily accessible to customers (NSGC Executive Office 2015). ACMG advocates that a genetics expert should be available to all DTC-PGT consumers and should be actively involved in the interpretation and disclosure of results (ACMG Board of Directors 2015). ASHG recommends that companies offering DTC-PGT be transparent about the risks and limitations of testing; that professional organizations educate providers about this form of testing; and that federal government agencies regulate DTC-PGT (Hudson et al. 2007).
While these professional organizations advocate for genetics experts to meet with DTC-PGT customers, a survey of 312 genetic counselors found that the field lacks consensus regarding the role that genetic counselors should play (Hock et al. 2011). In this 2008 study, 55% thought genetic counselors have a professional obligation to be knowledgeable about DTC-PGT, and 48% felt that genetic counselors should be able to interpret results. The study also revealed that most genetic counselors had limited experience working with DTC-PGT consumers, with only 14% reporting ever having received requests for test interpretation or discussion (Hock et al. 2011). Despite the limited involvement of genetic counselors in DTC-PGT to date, Harris et al. (2013) highlighted several emerging roles for genetic counselors within this field, including: genetic educator for both consumers and physicians; mediator between consumers and physicians; lifestyle/health advisor to explain what behavior changes are indicated by results; risk interpreter; and even entrepreneur (Harris et al. 2013). NSGC does not currently have practice guidelines to help guide genetic counselors in their interactions with clients seeking genetic counseling for PGT.
While DTC-PGT does not require genetic counseling at any point in the testing process, some consumers seek follow-up with a healthcare provider after receiving their DTC-PGT results. Previous surveys of consumers of personal genomic testing (PGT) companies found that 20–40% of participants discussed their results with their primary care provider (PCP) and 1–14% discussed them with a genetic counselor (Bloss et al. 2013; Kaufman et al. 2012; van der Wouden et al. 2016). Although previous studies have examined what leads DTC-PGT consumers to follow-up with their primary care provider (PCP) after receiving their results (van der Wouden et al. 2016; Wasson et al. 2014), we are unaware of any studies assessing predictors of seeking genetic counseling services following DTC-PGT. This study aimed to identify such predictors, thereby enhancing understanding of this patient population and informing counselors’ preparation for clinical encounters.
Methods
Participants and Procedures
The Impact of Personal Genomics (PGen) Study was a longitudinal survey-based study of new customers from DTC-PGT service providers 23andMe and Pathway Genomics. During the time period the study was conducted, 23andMe provided disease risk information in their results and Pathway Genomics operated under a DTC model. The study was conducted by a multidisciplinary research team based at Harvard Medical School / Brigham and Women’s Hospital and the University of Michigan School of Public Health and aided by a team of consultants representing academic and industry perspectives (Lehmann et al. 2012). Participants were recruited after placing an order for DTC-PGT through one of the above companies between March and July 2012. Participants who purchased DTC-PGT through 23andMe (the standard cost of which was USD $99) during this time frame were sent an email from the company describing the study and inviting them to participate. Members of PatientsLikeMe, a health-based social networking site, received emails offering DTC-PGT through Pathway Genomics at a subsidized cost of $25 if they participated in the study. Participants were also recruited through a banner advertisement on the Pathway Genomics website.
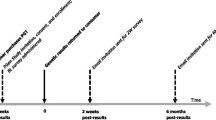
Three web-based surveys were sent by email to participants through a third-party survey research firm at the following time-points: 1) baseline after testing was ordered, but before results were received; 2) approximately 2 weeks after the DTC-PGT results were viewed; and 3) approximately 6 months after the results were viewed. Participants were compensated with electronic gift cards ($10 for completion of the baseline survey, $20 for the 2 week survey, and $20 for the 6 month survey). Complete details of the study design have been reported previously (Carere et al. 2014).
The baseline survey was completed by 1464 participants, 1046 of whom went on to submit the 6 month survey. Of these participants, 1026 indicated at 6 months whether or not they had sought GC after receiving their results, and were therefore eligible to be included in the present analysis.
Measures
Demographics
Demographic information including age, sex, race/ethnicity, education level, employment status, marital status, and household income were collected through self-report at baseline.
Personal and Family Health Information
Personal and family medical history was ascertained at baseline by providing a list of 14 disease categories (e.g., cancer, diabetes, heart conditions) and asking participants to indicate if a doctor had ever told them they had the medical condition (Yes/No). Self-reported health was assessed at baseline using one item from the SF-36 Short-Form Health Survey (Ware and Sherbourne 1992).
Previous Genetics Experience
Previous genetics experience was assessed at baseline by asking participants whether they had ever met with a genetic counselor, had genetic testing (and if yes, what type), or purchased PGT through a different company. Diagnostic, carrier, predictive/presymptomatic, prenatal, and medication response genetic testing responses were categorized as “health-related,” while ancestry, trait, and nutrigenomic testing responses were categorized as “recreational/lifestyle.”
Motivations and Interests
Motivations for testing were assessed at baseline by asking participants to rate the importance of 12 listed reasons for seeking DTC-PGT on a 3-point Likert scale (1 = not at all important; 2 = somewhat important; 3 = very important). We created a composite “health-related motivation score” (possible range: 5–15) by summing scores from the five scale items pertinent to the individual’s health or health care planning: 1) interest in finding out about personal risk for specific diseases, 2) desire to improve health, 3) interest in finding out about drug response, 4) desire to create a better plan for the future, and 5) interest in obtaining information about risk of health conditions for current and future children (Cronbach’s alpha = 0.77).
Using a 3-point Likert scale (1 = not at all interested; 2 = somewhat interested; 3 = very interested), participants were asked at baseline to indicate their level of interest in learning five types of genetic information: risk of disease or health condition; drug response; carrier status; ancestry; and traits.
Disease Risk Perceptions
Disease risk perceptions were assessed in the baseline survey. Participants were given a list of 24 conditions and asked to compare their chances of developing the disease to the average man or woman of their age, using a 5-point Likert scale (1 = much lower than average to 5 = much higher than average).
Genetic Knowledge
Genetic knowledge was assessed at baseline with nine true/false statements about genetics and health. These questions were selected from several validated measures of assessing genetic knowledge in the lay public (Bowling et al. 2008; Furr and Kelly 1999; Molster et al. 2009; Smerecnik et al. 2011). Participants were given a score of 0–9 based on the sum of their correct responses (Ostergren et al. 2015).
Numeracy
Numeracy was assessed at baseline with an abbreviated (5 question) version of a validated objective numeracy scale (Lipkus et al. 2001). Each participant was given a score from 0 to 100 based on their percentage of correct responses.
Genetic Self-Efficacy
Genetic self-efficacy, or confidence in one’s ability to interpret genetic information, was assessed at baseline with an adapted version of a published self-efficacy measure (Ashida et al. 2012; Carere et al. 2016). Participants used a 7-point Likert scale (1 = strongly disagree to 7 = strongly agree) to rate their level of agreement or disagreement with five statements about their confidence in their ability to understand and use genetic information. Each participant was given a score of 5–35 based on the sum of their responses, with higher scores indicating higher genetic self-efficacy (Cronbach’s alpha = 0.93).
Reactions to Results
Reactions to results were assessed at 2 weeks post-viewing of results. Participants responded to 13 statements about potential reactions to test results and indicated how often they experienced these reactions by using a 4-point Likert scale (0 = Never to 3 = Often). This measure was adapted from a validated measure of psychological impact of genetic susceptibility testing (Chung et al. 2009). We created a composite “results uncertainty score” (0–3) by averaging responses to the five scale items addressing the potential uncertainty of test results (Cronbach’s alpha = 0.76).
Perceived Utility of Results
Perceived utility of results was assessed on the 6-month survey using 8 items. Participants were asked to what extent they agreed or disagreed with statements about the utility of PGT (i.e. “What I learned about my personal genomic testing can help reduce my chances of getting sick”) on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). Responses were summed and participants were given a score ranging from 8 to 40 (Cronbach’s alpha = 0.77).
Use of Medical Services
Use of medical services was assessed on the 6-month survey by asking which medical professionals (e.g., genetics specialist, primary care provider) the participants had subsequently scheduled an appointment with to discuss their DTC-PGT results. Those who indicated they had met with a PCP and/or with a genetic counselor were asked to rate their satisfaction with each of these discussions on a 3-point Likert scale (1 = not at all satisfied to 3 = very satisfied). Participants were also asked if they would have utilized in-person genetic counseling services had they been available (1 = strongly disagree to 5 = strongly agree).
Data Analysis
Descriptive statistics were used to characterize participants based on demographics, genetic literacy, genetics self-efficacy, numeracy, personal and family medical history, previous genetics experience, motivations for testing, disease risk perceptions, reactions to results, use of medical services, and perceived utility of testing.
Participants were divided into 2 groups: GC seekers and GC non-seekers. GC seekers were those who indicated on the 6-month survey that they had either met or scheduled an appointment with a genetic counselor to discuss their results. Those who had neither met with nor made an appointment with a GC were included in the GC non-seekers group. Chi-square analyses and t-tests were used to compare the two groups based on the variables noted above.
Logistic regression was performed to identify predictors of GC seeking. Regression analysis was performed in a step-wise fashion. First, a series of univariate regressions was performed using variables that were found to be most strongly correlated (those with the lowest p-values) with GC seeking based on chi-square and t-tests. Then, the variables that were most strongly associated with GC seeking individually (e.g., those that were significant at a p-value of <0.05 and had the largest OR) were fitted into a multivariate regression model in a stepwise fashion. All data were analyzed using SPSS statistical software. Statistical significance for analyses was set at p < 0.05.
Results
Out of the total analytic sample of 1026, there were 43 GC seekers (4%) and 983 GC non-seekers (96%). GC seekers included both those who had already discussed their results with a genetics specialist (genetic counselors and geneticists) (n = 31), and those who had an appointment with a genetics specialist pending (n = 12). Demographic information, stratified by GC seeking behavior, is presented in Table 1. The sample was predominantly white (91%), female (60%), married (52%), college educated (80%), and wealthy, with 43% earning a household income of $100,000 or more. The GC seekers were significantly younger than the non-seekers, with an average age of 38.1 years (vs 46.2, p < 0.01). GC seekers were also more likely to have children under the age of 18 years (26 vs 16%, p < 0.01), to be students (16 vs 8%, p < 0.05), and to be unemployed (19 vs 6%, p < 0.01). GC seekers and non-seekers were otherwise similar in terms of sex, race, marital status, income, and education.
Overall, participants had high numeracy, genetics knowledge, and genetics self-efficacy. GC seekers scored lower on the objective numeracy test than the non-seekers, with an average of 4.49 items correct out of 5 (vs 4.71in non-seekers, p < 0.05). GC seekers and non-seekers did not significantly differ in their baseline objective genetic knowledge score (overall sample mean = 8.15, range 0–9) or genetic self-efficacy score (overall sample mean = 29.02, range 5–35).
Personal and family health history of the participants is summarized in Table 2. GC seekers did not report a greater number of conditions in their personal medical history, but they were significantly more likely to report their general health as poor or fair (32.6 vs 14.4%, p < 0.001). GC seekers also reported a higher number of medical conditions in their family history (7.6 vs 6.6, p < 0.05) and feeling at risk for a higher number of conditions (4.3 vs 3.0, p < 0.05). GC seekers were more likely to have had previous genetic counseling (37.2 vs 7.4%, p < 0.001), and previous genetic testing (30.0 vs 14.9%, p < 0.01). The type of previous genetic testing also differed between the groups, with GC seekers more frequently having had testing typically offered through medical professionals (25.6 vs 11.2%, p < 0.05) and less frequently having previously had recreational testing (2.3 vs 7.2%, p < 0.05).
The motivations for testing are summarized in Table 3. GC seekers scored higher than non-seekers on our composite health-related motivations scale (14.3 vs 11.6, p < 0.001). Compared to non-seekers, GC seekers tended to be more motivated to pursue PGT due to the following specific factors: interest in learning about risks to current or future children; desire to create a better plan for the future; desire to improve health; and interest in finding out about drug response. When asked how interested they were in learning about different types of results, GC seekers were significantly more likely to report being very interested in carrier status (58.1 vs 31.5%, p < 0.01) and drug response (74.4 vs 52.8%, p < 0.05) compared to non-seekers.
Reactions to results from the 2-week survey are summarized in Table 4. GC seekers scored higher on our results reaction uncertainty scale than non-seekers (1.2 vs 0.8, p < 0.001) and were more likely to endorse the following specific items: feeling concerned about how their results will affect insurance status; feeling uncertain about what results mean about personal risk; feeling unsure of what to do to prevent disease; having had difficulty talking about results with others; and feeling motivated to change lifestyle based on results. At 6 months, GC seekers also rated the perceived utility of test results as higher than non-seekers (4.2 vs. 3.8, p < .05). Changes in risk perceptions across time points were not found to differ significantly between GC seekers and non-seekers.
While only 3% reported sharing their results with a genetic counselor (as compared to the 8% who said they intended to do so in the baseline survey), 29% had shared them with their PCP and 17% had shared with another medical professional (e.g., physician assistant, nurse, obstetrician/gynecologist, oncologist). Over half (55%) of GC seekers had also shared their results with their PCP, vs 27% of GC non-seekers. Satisfaction with discussion of DTC-PGT did not differ significantly by type of provider, with 13% (vs 18%) feeling not at all satisfied and 39% (vs 35%) feeling very satisfied with their discussion with their genetic counselor (vs PCP). 39% of participants either somewhat (23%) or strongly agreed (16%) that they would have utilized in-person genetic counseling services had they been available.
Table 5 summarizes the logistic regression model of variables associated with GC seeking. Previous GC, being motivated to pursue DTC-PGT for health reasons, reporting poor general health, and feeling uncertainty about results were most strongly associated with seeking GC following DTC-PGT. These variables predict 20.4% of the variance seen in GC seeking in this study population.
Discussion
This is the first study to look beyond the proportion of DTC-PGT customers who seek genetic counseling to identify how consumers’ demographics, attitudes, and test results might influence seeking a consultation. We found that 4% of consumers in our study population sought genetic counseling for their results. This is slightly higher than the 1% rate observed by Kaufman et al. (2012), but lower than the 14% rate reported by Bloss et al. (2013), likely due to the fact that participants in the latter study were provided with free access to GC services through the DTC-PGT company. Given the moderate interest in utilizing genetic counseling services reported by our participants, the proportion of GC seekers may have been higher had genetic counseling been more accessible. Lack of awareness of, or experience with, accessing genetic counseling may explain the low utilization rate observed here, given that the strongest predictor of seeking GC for results was having had genetic counseling prior to pursuing DTC-PGT. Over one-third of GC seekers had prior experiences with genetic counseling, compared to less than 10% of non-seekers. The low rate of GC seeking could also be attributed to the fact that many users were not pursuing testing for health reasons, but rather for recreational reasons, such as general curiosity or for ancestry information. Health-related motivators associated with GC seeking in our study included learning about risks to family members and carrier status.
Poorer self-reported health was an important predictor of seeking genetic counseling, which is consistent with related PGen study data indicating that some people seek DTC-PGT to help explain a currently active medical condition, as opposed to identifying risks for potential future disease (Meisel et al. 2015). GC seekers also tended to report a greater number of conditions in their family medical history, which could explain why they perceived being at increased risk for more conditions than non-seekers. Participants frequently reported personal and family histories of common, complex conditions (such as arthritis, heart disease, and GI conditions) that are seen in primary care or specialty settings and not typically seen in genetics clinics. Given that generally there are no specific genetic tests for these common, complex conditions currently, some patients may have been seeking genetics specialty care for a non-genetic condition, which could potentially explain why there was no significant difference in visit satisfaction levels for genetic counselors and primary care physicians. Consumers may have been hoping for further testing or medical recommendations from genetic counseling, creating a potential mismatch between client expectations and what medical providers can provide.
Predictors of seeking genetic counseling extend beyond participants’ characteristics to their reactions to learning their results. After receiving results, GC seekers felt more motivated to use them to improve their health than non-seekers but also perceived a higher degree of uncertainty about their results. Given the group’s high levels of numeracy, genetic knowledge, and genetic self-efficacy, one might assume they would have high comprehension of results. However, many DTC test reports are complex and the personal health implications of test results are often ambiguous, which may contribute to users’ uncertainty (Ostergren et al. 2015). Because the GC seekers reported high motivation to improve their health but greater uncertainty about results, they may have sought genetic counseling to help clarify how their personal genetic information can inform future health behaviors and medical care.
Consistent with previous studies, we found that consumers were significantly more likely to share their results with their PCP than a genetic counselor (Kaufman et al. 2012; Bloss et al. 2013). Given that the conditions included in DTC-PGT results are those typically seen in a primary care setting and that PCPs are much more accessible than genetic counselors, this result is not surprising and may, in fact, be entirely appropriate. Over half of GC seekers had also shared their results with their PCP. Potential explanations for this finding include needing a referral from a PCP to schedule a genetic counseling appointment, lack of satisfaction with the initial PCP encounter, or lack of awareness of genetic counseling prior to discussing the results with a PCP.
Consumers’ pre-test expectations may also be related to perceptions of utility of DTC-PGT. GC seekers believed that testing had significantly higher utility than non-seekers, yet genetic counselors typically view DTC-PGT as of lower utility than customers do (Leighton et al. 2012). Consumers may have incorrect perceptions about the utility of testing and put more weight on the usefulness of results than the medical professionals they are consulting. While consumers are more likely to go to a PCP than a genetic counselor to discuss their results, a survey of family and internal medicine providers found that only 39% of PCPs were aware of DTC-PGT and 85% felt unprepared to answer patient questions about their results (Powell et al. 2012).
Limitations and Future Directions
There are several limitations to this study. Participants are early adopters of DTC-PGT and may not be representative of the current population of DTC-PGT consumers. Participants are also not representative of the general population in terms of race, education level, and income. The small sample size of GC seekers also limits the power of the study to detect group differences in key study outcomes. Some survey items may be prone to recall or other self-reporting biases and some survey measures were developed by the research team and/or not formally validated. The relatively short follow-up time period may have meant missing some participants who decided to seek GC services beyond the final 6-month survey. We also lack detailed information on what specifically prompted participants to seek GC, such as whether it was the test results alone or a combination of the results and family medical history. To address such study limitations, we need to know more about the subjective experiences of DTC-PGT consumers whose results prompt them to seek genetic counseling. Qualitative research might be particularly useful to explore this population’s motivations and counseling experiences.
Conclusions
Genetic counselors may increasingly be asked to see patients who are seeking counseling for their DTC-PGT results and therefore an understanding of who seeks these services and why is needed. Our results suggest this population may be motivated to pursue testing to address current health problems and to seek GC services to help resolve uncertainty surrounding their personal test results. These users may also be seeking counseling for common complex conditions for which no clinical genetic testing is currently available. The DTC-PGT landscape has changed since this study was conducted, and many SNPs with low associations with common disease risk are no longer reported to the consumer. Nevertheless, genetic counselors may be advised to address mismatches between client expectations and what services can actually be offered, to explore what clients had hoped testing would provide or how they believed it could improve their health, and to address potential misconceptions about the validity and utility of testing.
References
ACMG Board of Directors. (2015). Direct-to-consumer genetic testing: A revised position statement of the American College of Medical Genetics and Genomics. Genetics in Medicine, 18(2), 207–208. doi:10.1038/gim.2015.190.
Ashida, S., Goodman, M. S., Stafford, J., Lachance, C., & Kaphingst, K. A. (2012). Perceived familiarity with and importance of family health history among a medically underserved population. Journal of Community Genetics, 3(4), 285–295. doi:10.1007/s12687-012-0097-x.
Bloss, C. S., Darst, B. F., Topol, E. J., & Schork, N. J. (2011). Direct-to-consumer personalized genomic testing. Human Molecular Genetics, 20(R2), R132–R141. doi:10.1093/hmg/ddr349.
Bloss, C. S., Wineinger, N. E., Darst, B. F., Schork, N. J., & Topol, E. J. (2013). Impact of direct-to-consumer genomic testing at long term follow-up. Journal of Medical Genetics, 50(6), 393–400. doi:10.1136/jmedgenet-2012-101207.
Bowling, B. V., Acra, E. E., Wang, L., Myers, M. F., Dean, G. E., Markle, G. C., et al. (2008). Development and evaluation of a genetics literacy assessment instrument for undergraduates. Genetics, 178(1), 15–22. doi:10.1534/genetics.107.079533.
Bunnik, E. M., Janssens, A. C. J. W., & Schermer, M. H. N. (2015). Personal utility in genomic testing: Is there such a thing? Journal of Medical Ethics, 41(4), 322–326. doi:10.1136/medethics-2013-101887.
Carere, D. A., Couper, M. P., Crawford, S. D., Kalia, S. S., Duggan, J. R., Moreno, T. A., et al. (2014). Design, methods, and participant characteristics of the impact of personal genomics (PGen) study, a prospective cohort study of direct-to-consumer personal genomic testing customers. Genome Medicine, 6(12), 96. doi:10.1186/s13073-014-0096-0.
Carere, D. A., Kraft, P., Kaphingst, K. A., Roberts, J. S., & Green, R. C. (2016). Consumers report lower confidence in their genetics knowledge following direct-to-consumer personal genomic testing. Genetics in Medicine, 18(1), 65–72. doi:10.1038/gim.2015.34.
Caulfield, T., & McGuire, A. L. (2012). Direct-to-consumer genetic testing: Perceptions, problems, and policy responses. Annual Review of Medicine, 63, 23–33. doi:10.1146/annurev-med-062110-123753.
Chung, S., Mehta, K., Shumway, M., Alvidrez, J., & Perez-Stable, E. J. (2009). Risk perception and preference for prevention of Alzheimer’s disease. Value in Health, 12(4), 450–458. doi:10.14440/jbm.2015.54.A.
Darst, B. F., Madlensky, L., Schork, N. J., Topol, E. J., & Bloss, C. S. (2013). Perceptions of genetic counseling services in direct-to-consumer personal genomic testing. Clinical Genetics, 84(4), 335–339. doi:10.1111/cge.12166.
Dohany, D., Gustafson, S., Ducaine, W., & Zakalik, D. (2012). Psychological distress with direct-toconsumer genetic testing: a case report of an unexpected BRCA positibe test result. Journal of Genetic Counseling, 21(3), 399–401.
Food & Drug Administration. (2017). FDA allows marketing of first direct-to-consumer tests that provide genetic risk information for certain conditions. Retrieved from https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm551185.htm.
Francke, U., Dijamco, C., Kiefer, A. K., Eriksson, N., Moiseff, B., Tung, J. Y., & Mountain, J. L. (2013). Dealing with the unexpected: consumer responses to direct-access BRCA mutation testing. PeerJ, 1, e8. doi:10.7717/peerj.8.
Furr, L. A., & Kelly, S. E. (1999). The genetic knowledge index: Developing a standard measure of genetic knowledge. Genetic Testing, 3(2), 193–199. doi:10.1089/gte.1999.3.193.
Gutierrez, A. (2013). Warning Letter. Retrieved from http://www.fda.gov/ICECI/EnforcementActions/WarningLetters/2013/ucm376296.htm.
Harris, A., Kelly, S. E., & Wyatt, S. (2013). Counseling customers: Emerging roles for genetic counselors in the direct-to-consumer genetic testing market. Journal of Genetic Counseling, 22(2), 277–288. doi:10.1007/s10897-012-9548-0.
Hock, K. T., Christensen, K. D., Yashar, B. M., Roberts, J. S., Gollust, S. E., & Uhlmann, W. R. (2011). Direct-to-consumer genetic testing: An assessment of genetic counselors’ knowledge and beliefs. Genetics in Medicine, 13(4), 325–332. doi:10.1097/GIM.0b013e3182011636.
Hudson, K., Javitt, G., Burke, W., Byers, P., & ASHG Social Issues Committee. (2007). ASHG Statement on Direct-to-Consumer Genetic Testing in the United States. American Journal of Human Genetics, 81(3), 635–637.
James, K. M., Cowl, C. T., Tilburt, J. C., Sinicrope, P. S., Robinson, M. E., Frimannsdottir, K. R., et al. (2011). Impact of direct-to-consumer predictive genomic testing on risk perception and worry among patients receiving routine care in a preventive health clinic. Mayo Clinic Proceedings, 86(10), 933–940. doi:10.4065/mcp.2011.0190.
Kalf, R. R. J., Mihaescu, R., Kundu, S., Knijff, P. D., Green, R. C., & Janssens, A. C. J. (2014). Variations in predicted risks in personal genome testing for common complex diseases. Genetics in Medicine, 16(1), 1–13. doi:10.1038/gim.2013.80.Variations.
Kaufman, D. J., Bollinger, J. M., Dvoskin, R. L., & Scott, J. A. (2012). Risky business: Risk perception and the use of medical services among customers of DTC personal genetic testing. Journal of Genetic Counseling, 21(3), 413–422. doi:10.1007/s10897-012-9483-0.
Lehmann, L. S., Kaufman, D. J., Sharp, R. R., Moreno, T. A., Mountain, J. L., Roberts, J. S., & Green, R. C. (2012). Navigating a research partnership between academia and industry to assess the impact of personalized genetic testing. Genetics in Medicine : Official Journal of the American College of Medical Genetics, 14(2), 268–273. doi:10.1038/gim.2011.59.
Leighton, J. W., Valverde, K., & Bernhardt, B. A. (2012). The general public’s understanding and perception of direct-to-consumer genetic test results. Public Health Genomics, 15(1), 11–21. doi:10.1159/000327159.
Lipkus, I. M., Samsa, G., & Rimer, B. K. (2001). General performance on a numeracy scale among highly educated samples. Medical Decision Making, 21, 37–44.
Mathews, R., Hall, W., & Carter, A. (2012). Direct-to-consumer genetic testing for addiction susceptibility: A premature commercialisation of doubtful validity and value. Addiction, 107(12), 2069–2074. doi:10.1111/j.1360-0443.2012.03836.x.
Meisel, S. F., Carere, D. A., Wardle, J., Kalia, S. S., Moreno, T. A., Mountain, J. L., et al. (2015). Explaining, not just predicting, drives interest in personal genomics. Genome Medicine, 7(1), 74. doi:10.1186/s13073-015-0188-5.
Molster, C., Charles, T., Samanek, A., & O’Leary, P. (2009). Australian study on public knowledge of human genetics and health. Public Health Genomics, 12(2), 84–91. doi:10.1159/000164684.
NSGC Executive Office. (2015). Direct Access to Genetic Testing. Retrieved from http://nsgc.org/p/bl/et/blogid=47&blogaid=22.
Ostergren, J. E., Gornick, M. C., Carere, D. A., Kalia, S. S., Uhlmann, W. R., Ruffin, M. T., et al. (2015). How well do customers of direct-to-consumer personal genomic testing services comprehend genetic test results? Findings from the impact of personal genomics study for the PGen study group. Public Health Genomics, 18(4), 216–224. doi:10.1159/000431250.
Powell, K. P., Christianson, C. A., Cogswell, W. A., Dave, G., Verma, A., Eubanks, S., & Henrich, V. C. (2012). Educational needs of primary care physicians regarding direct-to-consumer genetic testing. Journal of Genetic Counseling, 21(3), 469–478. doi:10.1007/s10897-011-9471-9.
Roberts, J. S., & Ostergren, J. (2013). Direct-to-consumer genetic testing and personal genomics services: A review of recent empirical studies. Current Genetic Medicine Reports, 1(3), 182–200. doi:10.1007/s40142-013-0018-2.
Smerecnik, C. M. R., Mesters, I., De Vries, N. K., & De Vries, H. (2011). Applying a theory-based framework to understand public knowledge of genetic risk factors: A case for the distinction between how-to knowledge and principles knowledge. Public Health Genomics, 14(4–5), 259–270. doi:10.1159/000294149.
Uhlmann, W. R., & Sharp, R. R. (2012). Genetic testing integration panels (GTIPs): A novel approach for considering integration of direct-to-consumer and other new genetic tests into patient care. Journal of Genetic Counseling, 21(3), 374–381. doi:10.1007/s10897-011-9468-4.
van der Wouden, C. H., Carere, D. A., Maitland-van der Zee, A. H., Ruffin, M. T., Roberts, J. S., & Green, R. C. (2016). Consumer perceptions of interactions with primary care providers after direct-to-consumer personal genomic testing. Annals of Internal Medicine. doi:10.7326/M15-0995.
Wade, C. H., & Wilfond, B. S. (2006). Ethical and clinical practice considerations for genetic counselors related to direct-to-Consuemr Marketing of Genetic Tests. American Journal of Medical Genetics Part C, 142C, 284–292. doi:10.1002/ajmg.c.
Ware, J., & Sherbourne, C. (1992). The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Medical Care, 30(6), 473–483.
Wasson, K., Cherny, S., Sanders, T. N., Hogan, N. S., & Helzlsouer, K. J. (2014). Who are you going to call? Primary care patients’ disclosure decisions regarding direct-to-consumer genetic testing. Narrative Inquiry in Bioethics, 4(1), 53–68. doi:10.1353/nib.2014.0026.
Acknowledgements
The Impact of Personal Genomics (PGen) Study was funded by a grant from the National Institutes of Health (NIH), National Human Genomic Research Institute (NHGRI) (R01-HG005092). DRK was supported by the Jane Engelberg Memorial Fellowship from the National Society of Genetic Counselors. DAC is supported by a Michael G. DeGroote Postdoctoral Fellowship from McMaster University and a Canadian Institutes of Health Research Postdoctoral Fellowship. Nonauthor members of the PGen Study team include the following: Sarah Kalia, Kurt Christensen, Harvard Medical School and Brigham and Women’s Hospital; Mick Couper, Brent Doil, Michele Gornick, Lan Le, Jenny Ostergren, University of Michigan School of Public Health; Joanna Mountain, 23andMe; Glenn Braunstein, Pathway Genomics; Scott Crawford, Sound Rocket; Adrienne Cupples, Clara Chen, Catharine Wang, Boston University; Sarah Gollust, University of Minnesota; Stacy Gray, City of Hope Comprehensive Cancer Center; Kimberly Kaphingst, University of Utah; Barbara Koenig, University of California-San Francisco; Lisa Lehmann, US Department of Veterans Affairs; and Richard Sharp, Mayo Clinic. The authors also wish to acknowledge Margaret Helm, Caroline Weipert, and Erica Schonman for their assistance.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of Interest
Diane R Koeller, Wendy R Uhlmann, Deanna Alexis Carere, J Scott Roberts and the PGen Study Group declare that they have no conflict of interest. Robert C Green receives compensation for speaking or consultation from AIA, GenePeeks, Helix, Illumina, Prudential and Veritas, and is co-founder and advisor to Genome Medical, Inc.
Human Studies and Informed Consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000 (5). Informed consent was obtained from all patients for being included in the study.
Animal Studies
No animal studies were carried out by the authors for this article.
Rights and permissions
About this article

Cite this article
Koeller, D.R., Uhlmann, W.R., Carere, D.A. et al. Utilization of Genetic Counseling after Direct-to-Consumer Genetic Testing: Findings from the Impact of Personal Genomics (PGen) Study. J Genet Counsel 26, 1270–1279 (2017). https://doi.org/10.1007/s10897-017-0106-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10897-017-0106-7