
Abstract
Inherited bone marrow failure syndromes (IBMFS) including Fanconi anemia, dyskeratosis congenita, Diamond-Blackfan anemia, and Shwachman-Diamond syndrome are rare genetic disorders characterized by hematologic complications and increased risk of cancer. Patients and their families likely experience obstacles in obtaining sufficient health information given their disorders’ rarity. To investigate this possibility, we examined information-seeking behaviors and levels of general and disorder-specific genetic knowledge among 315 members of 174 families with an IBMFS, and how information-seeking behaviors and socio-demographic factors may be associated with their genetic knowledge. Cross-sectional survey data indicated that participants were most likely to have ever used the Internet or healthcare providers for genetic information. On average, participants correctly answered 57 % of items assessing general genetic knowledge and 49–59 % of disorder-specific knowledge items. Greater knowledge was associated with greater education and ever experiencing genetic counseling, attending a scientific meeting, and seeking information from the Internet and scientific literature. Among families with Fanconi anemia (whose family support organization has the longest history of providing information), greater disorder-specific genetic knowledge was also associated with seeking information from support groups and other affected families. Results suggest that families with IBMFS have uncertainty regarding genetic aspects of their disorder, and highlight potential channels for delivering educational resources.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Inherited bone marrow failure syndromes (IBMFS) include disorders such as Fanconi anemia (FA), dyskeratosis congenita (DC), Diamond-Blackfan anemia (DBA), and Shwachman-Diamond syndrome (SDS). These rare genetic disorders are characterized by hematologic complications that include bone marrow failure, myelodysplastic syndrome, and acute myeloid leukemia, as well as increased risk of syndrome-specific solid tumors and physical abnormalities (Alter et al. 2010). Affected individuals generally present with symptoms within the first decade of life, and despite recent therapeutic advances, survival rates for patients with an IBMFS remain lower than averages for the general population, with median ages of survival (reported from 2000 to 2009) of 29 years for FA, 49 years for DC, 45 years for DBA, and 36 years for SDS (Shimamura and Alter 2010).
The IBMFS are caused by mutations in multiple genes with various inheritance patterns. There are currently 16 known genes associated with FA (15 autosomal recessive [AR]; one X-linked recessive [XLR]). Nine genes associated with DC demonstrate all inheritance patterns (XLR, autosomal dominant [AD], and AR). Two of these genes can be inherited in either AD or AR patterns. Mutations in these genes account for approximately 60 % of all DC cases (Khincha and Savage 2013), indicating that other unidentified genetic risk factors exist. Over 10 ribosomal genes inherited in an AD manner are associated with DBA, which also account for approximately 60 % of known cases (Mirabello et al. 2014). A single AR gene accounts for the vast majority (>90 %) of cases of SDS (Shimamura and Alter 2010).
Given the complex nature of the IBMFS and the varying risks, benefits, and limitations of existing treatment options (e.g., androgen therapy, hematopoietic stem cell transplantation), individuals affected with an IBMFS must make numerous challenging decisions regarding the medical management of their disorder (e.g., Hamilton et al. 2013; Hutson et al. 2013). These decisions demand a minimum level of genetic literacy, or sufficient knowledge and appreciation of genetics principles, to allow informed decision-making for personal well-being (Bowling et al. 2008). Genetic literacy is especially important for patients with an IBMFS and their families due to the complex genetic origins of their disorders and the many knowledge-dependent challenges they face, including navigating the healthcare system, making treatment-related choices, and sharing information with at-risk relatives. Yet, given the rarity of their disorders, affected patients and their families likely face obstacles in obtaining genetic health information. Understanding where members of families with an IBMFS seek genetic health information, as well as what gaps exist in their genetic knowledge and literacy, can help researchers and clinicians develop and target communication efforts.
There is no existing evidence regarding the genetic information-seeking behaviors of patients or families affected with an IBMFS. Past research on genetic information seeking has focused on other populations, including the general public (Case, Johnson, Andrews, Allard, and Kelly 2004) and patients with chronic illnesses such as heart disease and diabetes (Morren, Rijken, Baanders, and Bensing 2007). This research has revealed that the Internet, healthcare providers, and print materials are popular sources of information. Similarly, an investigation of parents of children undergoing hematopoietic stem cell transplantation demonstrated that more than 80 % of respondents sought information about the transplant process from these resources; other resources such as caregiver support groups (14 %) and workshops/seminars (9 %) were used less frequently (Mayer et al. 2009). Further, a 2010 survey of members of patient organizations associated with the National Organization for Rare Disorders (NORD) found that 69 % of respondents received information or support about a health issue from a doctor or other healthcare professional, 58 % from friends or family, and 54 % from others with the same health condition (Fox 2011). Of those who got information or support from others with the same health condition, 46 % indicated that they went online for it. Whether these information-seeking patterns apply similarly to patients with an IBMFS, however, has never been examined.
There are several reasons to suspect that the Internet and online support groups are a primary genetic health information resource for families affected with an IBMFS. The IBMFS are rare; patients and family members may struggle to identify local healthcare providers with sufficient experience with their disorder and may have few opportunities to interact directly with others affected with the same disorder. Indeed, online communities and resources have been identified as valuable sources of support for parents of children with FA (Zierhut and Bartels 2012) and for those diagnosed with other rare genetic disorders (Black and Baker 2011; Gundersen 2011; Rivard and Mastel-Smith 2014; Schaffer, Kuczynski, and Skinner 2008). Each of the leading IBMFS family support organizations has a strong online presence including the Fanconi Anemia Research Fund, Inc. (founded in 1985; https://doi.org/www.fanconi.org), Diamond Blackfan Anemia Foundation, Inc. (founded in 1994; https://doi.org/www.dbafoundation.org), Shwachman-Diamond Syndrome Foundation (founded in 1994; https://doi.org/www.shwachman-diamond.org) and Dyskeratosis Congenita Outreach, Inc. (founded in 2008; https://doi.org/www.dcoutreach.org), and disseminating education and medical information are crucial elements of their missions.
Another important gap in the evidence pertains to levels of genetic knowledge among families with an IBMFS. Recent studies suggest that the general public has a modest understanding of genetic terminology and recognizes genetics as a risk factor for disease, but lacks detailed knowledge about scientific facts regarding DNA and genes, as well as patterns of inheritance (Christensen, Jayaratne, Roberts, Kardia, and Petty 2010; Condit 2010; Lanie et al. 2004; Lea, Kaphingst, Bowen, Lipkus, and Hadley 2011; but see Haga et al. 2013). Similarly, misconceptions regarding general or disorder-specific genetic knowledge are common in studies of various patient populations (e.g., testicular cancer families, Peters et al. 2008; parents with sickle cell trait, Acharya, Lang, and Ross 2009; parents of children with spinal muscular atrophy, Meldrum, Scott, and Swoboda 2007; parents and patients with cystic fibrosis, Conway et al. 1996; Hames, Beesley, and Nelson 1991). There are some data to suggest that characteristics including younger age (Ashida et al. 2011; Christensen et al. 2010; Haga et al. 2013; Peters et al. 2008), greater educational attainment (Christensen et al. 2010; Gallo, Knafl, and Angst 2009; Haga et al. 2013; Peters et al. 2008), greater income (Case et al. 2004; Gallo et al. 2009), and Internet use (Case et al. 2004) are associated with greater factual or perceived genetic knowledge. The level and determinants of genetic knowledge among patients with an IBMFS and their families remain to be described, however, and represent an important gap in the evidence needed to effectively care for this vulnerable population.
The goal of our study was to contribute descriptive information regarding genetic information-seeking behaviors and knowledge among families with an IBMFS using cross-sectional survey data collected through the National Cancer Institute (NCI) IBMFS cohort study from 2002 to 2012. We examined genetic information-seeking behaviors and levels of both general and disorder-specific genetic knowledge among a sample of members of families with an IBMFS (primarily unaffected parents of children diagnosed with an IBMFS). We also examined how information-seeking behaviors and conceptually-relevant socio-demographic factors are associated with individuals’ levels of genetic knowledge. Consistent with findings from other populations (Ashida et al. 2011; Case et al. 2004; Christensen et al. 2010; Gallo et al. 2009; Haga et al. 2013; Peters et al. 2008), we hypothesized that greater genetic knowledge would be associated with the performance of information-seeking behaviors, as well as with younger age, greater education, and greater income. Associations between genetic knowledge and additional factors including gender, relationship to an affected patient, and year of questionnaire completion were also examined in an exploratory manner.
Methods
Participants
Cross-sectional survey data were collected through the NCI IBMFS cohort study (protocol NCI 02-C-0052; clinicaltrials.gov ID NCT00027274; https://doi.org/www.marrowfailure.cancer.gov/). This study was approved by the NCI Institutional Review Board. Study procedures are reported in detail elsewhere (see Alter et al. 2010). Briefly, participants were recruited through mailings to pediatric hematologists/oncologists, medical geneticists, and IBMFS family support groups. Participants were screened for eligibility and provided written informed consent. These analyses utilized data from a mailed Individual Information Questionnaire collected from 2002 to 2012; this questionnaire collected baseline data about study participants prior to their visit to the study site and medical evaluation by the study investigators. Due to sample size limitations (e.g., insufficient number of responses from extended family members), these analyses were restricted to data collected from affected patients (i.e., probands) ages 18 and older at the time of enrollment who were diagnosed with the most common IBMFS (FA, DC, DBA, and SDS), and parents of affected patients (regardless of the patient’s age).
Instrumentation
Information-Seeking Behaviors
Six items assessed whether participants had ever used various sources to obtain genetic information about the condition in their family: the Internet, media (defined as “television, radio, magazines, newspaper, etc.”), a disease-related support group, other families with the same or a similar condition, a doctor or healthcare provider, and the scientific or medical literature. One item assessed whether participants had ever attended a scientific meeting or conference relevant to the IBMFS in their family, and one item assessed whether participants had ever received genetic counseling for any IBMFS. For all items, responses were coded as 0 = “no” and 1 = “yes.” Finally, one open-ended item asked participants to list the three websites that they used most frequently to learn about the genetic condition in their family.
General Genetic Knowledge
The Genetic Knowledge Scale (GKS) consisted of 15 investigator-designed items assessing aspects of inheritance and basic genetic principles (see Online Resource 1 for items). Response options for each item included “true”, “false”, and “don’t know.” Each item was scored as “1” for the correct response or “0” for the incorrect response and “don’t know.” To compute a total score for the GKS, the items were summed and divided by the total number of answered items to produce the proportion (ranging from 0 to 1) of correct GKS items. This scale demonstrated good internal consistency (Cronbach’s α = 0.85).
Disorder-Specific Genetic Knowledge
Investigator-designed items were used to assess genetic knowledge specific to FA (FA-GKS; 6 items), DC (DC-GKS; 5 items), DBA (DBA-GKS; 6 items), and SDS (SDS-GKS; 6 items). These items assessed inheritance patterns and genetic features of each IBMFS (see Online Resource 1). Response options for each item included “true”, “false”, and “don’t know.” As with the GKS, the proportion of correct items was computed for each disorder-specific scale. These scales demonstrated good internal consistency (Cronbach’s α = 0.89 for FA-GKS; 0.89 for DC-GKS; 0.91 for DBA-GKS; and 0.91 for SDS-GKS).
Socio-Demographic Characteristics
Data were collected regarding each participant’s age, gender, race, highest level of education completed, annual household income, and year of questionnaire completion. Based on self-report, individuals were classified as being a member of a family affected by FA, DC (including those with the severe DC-variants Hoyeraal-Hreidarsson syndrome and Revesz syndrome), DBA, or SDS. Each participant was also classified into 1 of 2 categories based on his or her relationship to an affected patient. “Patients” consisted of individuals who had been diagnosed with an IBMFS (e.g., probands). “Parents” consisted of the mothers or fathers of affected patients; in only 1 case (individual with DC) was a parent already diagnosed with an IBMFS at the time of data collection.
Data Analysis
Data were examined for missing values using SPSS 19.0 Missing Values statistical analysis software. Questionnaires with ≥20 % missing items for both primary outcome variables of the general and disorder-specific GKS were excluded from analysis (n = 49). For questionnaires with ≤20 % missing items on either scale, the scale scores were computed based on the total number of answered items. For several questionnaires, data were missing on relevant study variables including education (n = 2) and income (n = 24); values for these missing responses were derived through multiple imputation.
The sampling strategy allowed for questionnaire responses from multiple members of the same family (i.e., affected patient, mother, and father); hence, the data were correlated at the family unit level and violated the assumption of independence between cases. In order to include data from each respondent, all analyses and standard error estimates were corrected to account for the correlated data with the use of SPSS Complex Samples statistical analysis software, which used Taylor linearization to compute accurate standard errors for statistical testing. This technique allowed for the inclusion of all family members, thereby maximizing the analytic sample size while protecting against inaccurate variance estimates that could arise from such a complex sampling design.
We computed descriptive statistics for all study variables. To analyze whether differences in information-seeking behaviors and genetic knowledge existed based on key variables including year of questionnaire completion, family IBMFS, and relationship to an affected patient, we used Chi-square significance tests and ANOVAs, respectively. We also examined the extent to which information-seeking behaviors and socio-demographic factors were associated with participants’ levels of genetic knowledge. First, separate univariable linear regression models were conducted to determine whether variables including all information-seeking behaviors, age, gender, education, income, year of questionnaire completion, family IBMFS, and relationship to an affected patient were associated with the outcomes of general genetic knowledge and disorder-specific knowledge. Any variables significantly (p ≤ 0.05) associated with the outcome were then included as predictors in a multivariable linear regression model. Any non-significant predictors were trimmed from the final model. All statistical tests were 2-tailed with α = 0.05.
Results
The analytic sample consisted of 315 individuals from 174 families (see Table 1). The majority of participants were from families affected with FA (n = 110), followed by DBA (n = 88), DC (n = 84), and SDS (n = 33). Within the total sample, approximately half (55.6 %) of the participants were female, and the majority (92.4 %) were Caucasian. Most participants (87 %) were unaffected parents of an affected patient.
Information-Seeking Behaviors
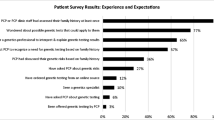
Figure 1 depicts the extent to which participants from families affected by each IBMFS ever sought genetic information from various sources. Overall, participants endorsed seeking genetic information from an average of 3.2 (SD = 1.9, range 0–8) different sources. Within the total sample, 68 % reported ever using the Internet to learn about the genetic condition in their family, 66 % used their healthcare provider, 47 % used disease-related support groups, 38 % used scientific or medical literature, 36 % had experienced genetic counseling, 31 % used other families with the condition, 24 % used media, and 17 % attended a scientific meeting. Approximately 7 % of participants did not endorse using any of the information sources. Chi-square tests of significance indicated that the use of several information sources differed based on family IBMFS, with use generally being lowest for families with DC.

Information-seeking behaviors of participants from families with an IBMFS. Asterisks indicate significant differences in information-seeking behaviors across the four IBMFS (p ≤ 0.05). Note that data were missing for Internet use (n = 1), experience with genetic counseling (n = 10), and scientific meeting attendance (n = 4)
Additional Chi-square tests of significance indicated differences in information-seeking behaviors over time. Comparing behaviors from 2002 to 2006 versus 2007 to 2012, there were significant differences in the use of support groups (53 % versus 40 %; p = 0.03), genetic counseling (43 % versus 28 %; p = 0.006), other families (37 % versus 24 %, p = 0.02), media (30 % versus 16 %; p = 0.005), and scientific meetings (27 % versus 7 %, p < 0.001). Chi-square tests indicated that only use of genetic counseling differed based on participants’ relationship to an affected patient; a higher proportion of patients (55 %) than unaffected parents (33 %) had ever used genetic counseling to learn about the genetic condition in their families (p = 0.006).
For descriptive purposes, we also summarized participants’ responses to the open-ended item assessing the three websites used most frequently to learn about their family’s genetic condition (Online Resource 2). A total of 141 participants listed at least 1 identifiable website. These websites were categorized as disease-specific (16 separate sites, n = 103), government (6 sites, n = 57), medical search (7 sites, n = 47), generic search (7 sites, n = 33), hospital and medical center (8 sites, n = 20), and other (industry/investigator/scientific literature) (4 sites, n = 4).
Levels of Genetic Knowledge
Levels of general genetic knowledge among members of families with an IBMFS are presented in Table 2. On average, participants answered 57 % of the items comprising the GKS correctly. Items that were answered correctly most frequently included those assessing whether genes are made up of DNA, whether identified genetic disorders are curable, and whether some genetic disorders occur due to two inherited mutations (see Online Resource 1). Items most frequently answered incorrectly assessed whether cells in different organs have different genes and whether XLR traits affect females more often than males. Items for which participants most frequently endorsed uncertainty included those assessing whether carriers of recessive mutations are affected by the condition and whether mutations in different genes can cause the same disorder. Within the total sample, there were no significant differences in levels of correct knowledge based on family IBMFS (F(3,166) = 0.22, p = 0.88), year of questionnaire completion (F(1,168) = 0.26, p = 0.61), or the participant’s relationship to an affected patient (F(1,168) = 0.01, p = 0.91).
Family members’ levels of disorder-specific genetic knowledge are also shown in Table 2 (see Online Resource 1 for additional details). Participants from families affected by FA and SDS answered the highest proportion of disorder-specific genetic knowledge items correctly (59 % each), whereas those from families affected by DC answered the lowest proportion of disorder-specific genetic knowledge items correctly (49 %). Among families with each IBMFS, no differences were observed in disorder-specific genetic knowledge based on year of questionnaire completion or the participant’s relationship to an affected patient (all ps > 0.05).
Correlates of Genetic Knowledge
Given that there were no significant differences in general or disorder-specific knowledge based on the family IBMFS, year of questionnaire completion, or the participant’s relationship to an affected patient, these variables were not explored in analyses of correlates of genetic knowledge. Univariable linear regression analyses revealed that greater education and income; ever seeking information from the Internet, support groups, other families, healthcare providers, and scientific literature; ever attending a scientific meeting, and ever experiencing genetic counseling were associated with greater correct general genetic knowledge among all participants (data not shown, all ps ≤ 0.03). These variables were incorporated into a multivariable model (from which any nonsignificant variables were subsequently removed); as hypothesized, this final model revealed that greater education, ever seeking information from the Internet or scientific literature, ever attending a scientific meeting, and ever experiencing genetic counseling were significantly associated with greater correct genetic knowledge (see Table 3, all ps ≤ 0.04).
Correlates of correct disorder-specific genetic knowledge were also examined (Table 3); however, these analyses were not conducted for those from families with SDS because few participants completed the disorder-specific GKS (n = 32). Among families with DBA, univariable linear regression analyses revealed that only ever attending a scientific meeting was significantly associated with greater correct DBA-specific genetic knowledge (p = 0.01).
Among families with DC, univariable linear regression analyses revealed that female gender, completing a college degree (as compared to completing high school or less), ever seeking information from the Internet, support groups, and a healthcare provider, and ever experiencing genetic counseling were associated with greater correct DC-specific genetic knowledge (all ps ≤ 0.04). The final multivariable linear regression model indicated that ever seeking information from the Internet and ever experiencing genetic counseling were the only significant correlates of greater correct DC-specific genetic knowledge (ps ≤ 0.01).
Among families with FA, univariable linear regression analyses indicated that ever seeking information from support groups, other families, and the scientific literature, as well as ever attending a scientific meeting were associated with greater correct FA-specific genetic knowledge (all ps ≤ 0.03). The final multivariable model indicated that ever seeking information from support groups or other families, and ever attending a scientific meeting were significantly associated with greater correct knowledge regarding the genetics of FA (all ps ≤ 0.02).
Discussion
This is the first study to examine information-seeking behaviors and genetic knowledge of members of families with an IBMFS, for whom complex genetic information and the ability to understand and utilize it are critical. Results underscore that these families turn to multiple sources in their search for information about their disorder, with participants endorsing use of an average of three different resources. Congruent with studies in other populations (e.g., Mayer et al. 2009; Morgan et al. 2014; Rivard and Mastel-Smith 2014), most participants sought genetic information from the Internet (particularly disease-specific websites maintained by family support organizations) and healthcare providers. In addition, nearly half of participants sought information from a support group. Approximately a third of participants sought information from genetic counseling, with use of this service being more common among affected patients than their parents.
Some trends emerged in the extent to which participants endorsed different information-seeking behaviors over time. A greater proportion of participants used the media as an information source in the earlier years of the study (i.e., 2002 to 2006), which may be due in part to widespread news coverage of a child with FA whose parents used pre-implantation genetic diagnosis to create a sibling donor for her stem cell transplantation in 2000 (BBC News 2000; Belkin 2001; Faison 2005). However, we believe that the other observed time-related differences in information-seeking behaviors should be interpreted cautiously because they may be an artifact of the study methodology. Specifically, participants were initially recruited from family support organizations and healthcare providers, whereas participants in later years were more commonly self-referred. Thus, the more frequent endorsement of support groups, other families, genetic counseling, and scientific meetings by participants recruited in the earlier years of this study may simply reflect the study recruitment strategy, rather than secular trends in information-seeking behaviors.
Participants demonstrated some limitations in their genetic knowledge, as they correctly answered an average of 57 % of the items assessing general genetic knowledge, and 49 %–59 % of the disorder-specific genetic knowledge items. Participants were particularly uncertain about the disease risks faced by carriers of recessive mutations; relationships between gender, gender-specific disorders (e.g., breast or testicular cancer), and disorders with an XLR inheritance pattern; and the possibility that mutations in different genes result in the same disorder. These specific issues are highly relevant to the inheritance and etiology of the IBMFS, and likely represent topics about which patients and their families need greater clarity in order to understand and make decisions about their individual and shared risks. One may have expected to observe a substantial improvement in participants’ genetic knowledge over the 10-year duration of this study, commensurate with increasing scientific knowledge about the role of genetics in health and the explosion of knowledge about the IBMFS genes. However, levels of genetic knowledge did not differ among those participants enrolled in the earlier years of this study as compared to those participants enrolled in the later years of the study, suggesting that an information gap exists, and that families with an IBMFS may have challenges accessing genetic information that is timely, accurate, and comprehensible.
It was hypothesized that several different socio-demographic factors would be associated with genetic knowledge. However, results indicate that education was the only significant correlate; more educated participants had greater general genetic knowledge, perhaps finding it easier to locate and interpret complex genetic and medical information. Several information-seeking behaviors were also associated with genetic knowledge, as predicted. Use of scientific literature was associated with greater general genetic knowledge, and use of the Internet and genetic counseling were both associated with greater general and DC-specific genetic knowledge. Although only a small proportion of participants had previously attended a scientific meeting, use of this resource was associated with greater general, DBA-, and FA-specific genetic knowledge. Finally, use of a support group and other affected families was associated with greater FA-specific genetic knowledge. Contrary to predictions, use of media or a healthcare provider was not significantly associated with knowledge. These results demonstrate the value of diverse information channels for patients and families affected with an IBMFS, and highlight promising avenues for targeting future educational messages and interventions. For example, it may be possible to improve families’ understanding of the genetic nature of their disorder by increasing their awareness and access to relevant scientific meetings (e.g., Camp Sunshine 2014). However, attending such meetings may not be feasible for all families, and Internet-based interventions that capitalize on developments in social media and healthcare could also be effective, providing widely distributed information and opportunities to establish meaningful relationships with other patients and affected families.
Study Limitations
This study provides important insight into the experiences of families with four of the most common IBMFS. This study identifies various genetic information-seeking behaviors used by members of these families; however, the study measures were limited in scope. Additional aspects of information-seeking, such as frequency of these behaviors or individuals’ satisfaction, comprehension, perceived utility, or perceived credibility of different information resources, were not examined and should be investigated with future research. This study also examined how various factors may be associated with individuals’ levels of genetic knowledge. Although the findings were consistent with our predictions, it is important to acknowledge that the cross-sectional nature of the data precludes any conclusions regarding causality and changes in information needs or knowledge over time. Furthermore, we were unable to examine how the timing of a patient’s diagnosis may be related to her/his information seeking and knowledge, although it is likely that patients’ and families’ information needs change as they progress through the different stages of managing and treating their disorder. In addition, we were only able to examine a small number of socio-demographic factors in this sample. Although the study sample was diverse in terms of education and income, participants were predominantly Caucasian; thus it is not known whether similar patterns may be observed among families of other racial and ethnic backgrounds. Additional socio-demographic and medical factors, such as geographic location (e.g., rural versus urban residence), extent of previous experience with other chronic diseases, access to a regular healthcare provider, and quality of the relationship with a healthcare provider, may also be associated with individuals’ levels of genetic knowledge. As previously noted, participants were recruited from family support organizations and through healthcare providers, and over time, participants were also self-referred to the study. Thus, there is the possibility of a volunteerism bias, and the generalizability of these findings to the broader population of patients and families affected with an IBMFS is unknown.
Practice Implications
These findings have several implications for those who provide care to individuals from families affected by an IBMFS, and other rare genetic disorders. It is noteworthy that only about one-third of study participants had ever experienced genetic counseling. The reason for this low level of uptake is not clear, as individuals may lack access (including appropriate referrals and adequate insurance coverage) to trained genetic counselors, may lack awareness of their services, may be unable to overcome practical barriers (such as time away from work, transportation, or child care) to obtaining genetic counseling, or may lack interest in pursuing genetic counseling. Although we cannot determine whether the positive association observed in this study between use of genetic counseling and genetic knowledge is due to genetic counseling improving individuals’ knowledge, or to those with greater knowledge being more likely to seek out counseling, efforts should be made to better understand and ultimately minimize these obstacles so that those in greatest need can access these educational and supportive resources. Given that genetic counseling was found to be used more commonly among affected patients than their parents, it may be particularly helpful for counselors to provide patients with specific encouragement and advice for how to effectively share genetic information and resources with their parents and other family members.
These findings also highlight that patients’ and family members’ genetic education and disease management are dynamic processes that benefit from the efforts of many. Healthcare providers are critical resources, as doctors were commonly-noted information sources and the use of genetic counseling was associated with greater levels of genetic knowledge. However, an important role also exists for peer-to-peer education and patient advocacy. For families with an IBMFS, attendance at scientific meetings and the use of support groups and other affected families were also related to greater knowledge. Yet, it is important to recognize that the benefits of these patient advocacy efforts may take some time to accrue; the use of support groups and other affected families were only significantly associated with greater disorder-specific genetic knowledge for those from families with FA. FA is the IBMFS with the oldest family support organization, as it was founded nearly a decade before those of DBA and SDS, and more than two decades before that of DC. Conversely, families with DC, which lacked a family support organization for most of this study, reported the lowest levels of many information-seeking behaviors and disorder-specific genetic knowledge. These findings underscore the vital role of these organizations in connecting families with health information.
Research Recommendations
Future studies must focus on ways to improve genetic knowledge of patients with IBMFS and their family members, as knowledge is a key component of both genetic literacy (Bowling et al. 2008) and the emerging domain of genomic literacy (Hurle et al. 2013), and is critical for making informed health-related decisions. Investigations are needed to determine what specific types of information (e.g., information about patterns of inheritance, about mechanisms of disease etiology, etc.) are needed to allow patients and their families to feel most prepared to make the complex array of health decisions necessitated by their disorders. In addition, research should explore which educational approaches and information resources are most effective for teaching these concepts. It also remains possible that the individuals who are currently seeking genetic information are those with the greatest basic understanding of genetic concepts; thus it will be critical to determine how the efficacy of different educational strategies may vary based on an individual’s initial familiarity with genetics, general educational attainment, information preferences, and past information-seeking experiences. Finally, future studies should examine how members of these families are interacting with, and communicating about, their different genetic information resources. For example, investigations could examine to what extent patients or parents are sharing their findings with other family members, and how these individuals in turn respond to develop a shared understanding of their hereditary disease risk.
Conclusion
Families affected by an IBMFS use a variety of strategies to obtain genetic information, with the majority turning to the Internet and their healthcare provider. Several behaviors including use of genetic counseling, attending a scientific meeting, and seeking information from the Internet and scientific literature were associated with greater genetic knowledge. Notably, among families with FA, the group with the oldest family support organization, greater knowledge was also associated with seeking information from support groups and other affected families. Some uncertainty exists among families affected by an IBMFS regarding genetic aspects of their diagnosis and disease risks; yet, these results highlight potential information channels for delivering future genetic educational resources to these individuals.
References
Acharya, K., Lang, C. W., & Ross, L. F. (2009). A pilot study to explore knowledge, attitudes, and beliefs about sickle cell trait and disease. Journal of the National Medical Association, 101(11), 1163–1172.
Alter, B. P., Giri, N., Savage, S. A., Peters, J. A., Loud, J. T., Leathwood, L., et al. (2010). Malignancies and survival patterns in the National Cancer Institute inherited bone marrow failure syndromes cohort study. British Journal of Haematology, 150(2), 179–188.
Ashida, S., Goodman, M., Pandya, C., Koehly, L. M., Lachance, C., Stafford, J., et al. (2011). Age differences in genetic knowledge, health literacy and causal beliefs for health conditions. Public Health Genomics, 14(4–5), 307–316.
BBC News. (2000). Baby created to save older sister. Retrieved May 23, 2014, from https://doi.org/news.bbc.co.uk/2/hi/health/954408.stm.
Belkin, L. (2001). The made-to-order savior. The New York Times. Retrieved May 23, 2014, from https://doi.org/www.nytimes.com/2001/07/01/magazine/the-made-to-order-savior.html.
Black, A. P., & Baker, M. (2011). The impact of parent advocacy groups, the Internet, and social networking on rare diseases: The IDEA League and IDEA League United Kingdom example. Epilepsia, 52(Suppl 2), 102–104.
Bowling, B. V., Acra, E. E., Wang, L., Myers, M. F., Dean, G. E., Markle, G. C., et al. (2008). Development and evaluation of a genetics literacy assessment instrument for undergraduates. Genetics, 178(1), 15–22.
Camp Sunshine. (2014). About camp. Retrieved June 09, 2014, from https://doi.org/www.campsunshine.org/about_camp/.
Case, D. O., Johnson, J. D., Andrews, J. E., Allard, S. L., & Kelly, K. M. (2004). From two-step flow to the internet: the changing array of sources for genetics information seeking. Journal of the American Society for Information Science and Technology, 55(8), 660–669.
Christensen, K. D., Jayaratne, T. E., Roberts, J. S., Kardia, S. L. R., & Petty, E. M. (2010). Understandings of basic genetics in the United States: results from a national survey of black and white men and women. Public Health Genomics, 13(7–8), 467–476.
Condit, C. M. (2010). Public understandings of genetics and health. Clinical Genetics, 77(1), 1–9.
Conway, S., Pond, M., Watson, A., & Hamnett, T. (1996). Knowledge of adult patients with cystic fibrosis about their illness. Thorax, 51, 34–38.
Faison, A. M. (2005). The miracle of Molly. 5280. Retrieved May 23, 2014, from https://doi.org/www.5280.com/magazine/2005/08/miracle-molly.
Fox, S. (2011). Peer-to-peer Health Care. Pew Research Center. Retrieved March 31, 2014, from https://doi.org/www.pewinternet.org/2011/02/28/peer-to-peer-health-care-2/.
Gallo, A., Knafl, K., & Angst, D. (2009). Information management in families who have a child with a genetic condition. Journal of Pediatric Nursing, 24(3), 194–204.
Gundersen, T. (2011). “One wants to know what a chromosome is”: the internet as a coping resource when adjusting to life parenting a child with a rare genetic disorder. Sociology of Health & Illness, 33(1), 81–95.
Haga, S. B., Barry, W. T., Mills, R., Ginsburg, G. S., Svetkey, L., Sullivan, J., et al. (2013). Public knowledge and attitudes toward genetics and genetic testing. Genetic Testing and Molecular Biomarkers, 17(4), 327–335.
Hames, A., Beesley, J., & Nelson, R. (1991). Cystic fibrosis: what do patients know, and what else would they like to know? Respiratory Medicine, 85(5), 389–392.
Hamilton, J. G., Hutson, S. P., Moser, R. P., Kobrin, S. C., Frohnmayer, A. E., Alter, B. P., et al. (2013). Sources of uncertainty and their association with medical decision making: exploring mechanisms in Fanconi anemia. Annals of Behavioral Medicine, 46(2), 204–216.
Hurle, B., Citrin, T., Jenkins, J. F., Kaphingst, K. A., Lamb, N., Roseman, J. E., et al. (2013). What does it mean to be genomically literate?: national human genome research institute meeting report. Genetics in Medicine, 15(8), 658–663.
Hutson, S. P., Han, P. K. J., Hamilton, J. G., Rife, S. C., Al-Rahawan, M. M., Moser, R. P., et al. (2013). The use of haematopoietic stem cell transplantation in Fanconi anaemia patients: a survey of decision making among families in the US and Canada. Health Expectations. doi:https://doi.org/10.1111/hex.12066.
Khincha, P. P., & Savage, S. A. (2013). Genomic characterization of the inherited bone marrow failure syndromes. Seminars in Hematology, 50(4), 333–347.
Lanie, A. D., Jayaratne, T. E., Sheldon, J. P., Kardia, S. L. R., Anderson, E. S., Feldbaum, M., et al. (2004). Exploring the public understanding of basic genetic concepts. Journal of Genetic Counseling, 13(4), 305–320.
Lea, D. H., Kaphingst, K. A., Bowen, D., Lipkus, I., & Hadley, D. W. (2011). Communicating genetic and genomic information: health literacy and numeracy considerations. Public Health Genomics, 14(4–5), 279–289.
Mayer, D. K., Tighiouart, H., Terrin, N., Stewart, S., Peterson, E., Jeruss, S., et al. (2009). A brief report of caregiver needs and resource utilization during pediatric hematopoietic stem cell transplantation. Journal of Pediatric Oncology Nursing, 26(4), 223–229.
Meldrum, C., Scott, C., & Swoboda, K. J. (2007). Spinal muscular atrophy genetic counseling access and genetic knowledge: parents’ perspectives. Journal of Child Neurology, 22(8), 1019–1026.
Mirabello, L., Macari, E. R., Jessop, L., Ellis, S. R., Myers, T., Giri, N., et al. (2014). Whole-exome sequencing and functional studies identify RPS29 as a novel gene mutated in multi-case Diamond-Blackfan anemia families. Blood. doi:https://doi.org/10.1182/blood-2013-11-540278.
Morgan, T., Schmidt, J., Haakonsen, C., Lewis, J., Della Rocca, M., Morrison, S., Biesecker, B., & Kaphingst, K. A. (2014). Using the internet to seek information about genetic and rare diseases: a case study comparing data from 2006 and 2011. Journal of Medical Internet Research Protocols, 3(1), e10. doi:https://doi.org/10.2196/resprot.2916.
Morren, M., Rijken, M., Baanders, A. N., & Bensing, J. (2007). Perceived genetic knowledge, attitudes towards genetic testing, and the relationship between these among patients with a chronic disease. Patient Education and Counseling, 65(2), 197–204.
Peters, J. A., Beckjord, E. B., Banda Ryan, D. R., Carr, A. G., Vadaparampil, S. T., Loud, J. T., et al. (2008). Testicular cancer and genetics knowledge among familial testicular cancer family members. Journal of Genetic Counseling, 17(4), 351–364.
Rivard, M. T., & Mastel-Smith, B. (2014). The lived experience of fathers whose children are diagnosed with a genetic disorder. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 43(1), 38–49.
Schaffer, R., Kuczynski, K., & Skinner, D. (2008). Producing genetic knowledge and citizenship through the internet: mothers, pediatric genetics, and cybermedicine. Sociology of Health & Illness, 30(1), 145–159.
Shimamura, A., & Alter, B. P. (2010). Pathophysiology and management of inherited bone marrow failure syndromes. Blood Reviews, 24(3), 101–122.
Zierhut, H. A., & Bartels, D. M. (2012). Waiting for the next shoe to drop: the experience of parents of children with Fanconi anemia. Journal of Genetic Counseling, 21(1), 45–58.
Funding
This research was supported in part by the Intramural Research Program of the Division of Cancer Epidemiology and Genetics (DCEG) of the National Cancer Institute (JAP, BPA), and by contract HHSN261200655001C with Westat (AGC). JGH was supported in part by the National Cancer Institute Cancer Prevention Fellowship Program. PKJH was supported by the National Human Genome Research Institute through the Intergovernmental Personnel Act. We are extremely grateful to all participating patients and families affected with an IBMFS.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Compliance with Ethical Standards
Conflict of Interest The authors declare that they have no conflict of interest.
Human Studies and Informed consent All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Animal Studies No animal studies were carried out by the authors for this article.
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOCX 16 kb)
Rights and permissions
About this article

Cite this article
Hamilton, J.G., Hutson, S.P., Frohnmayer, A.E. et al. Genetic Information-Seeking Behaviors and Knowledge among Family Members and Patients with Inherited Bone Marrow Failure Syndromes. J Genet Counsel 24, 760–770 (2015). https://doi.org/10.1007/s10897-014-9807-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10897-014-9807-3