
Abstract
Emotion regulation corresponds to the individual’s ability to identify and modulate emotional experiences and improvements thereof over the course of psychotherapy are associated with the reduction in psychiatric symptoms across multiple diagnoses. However, the extent to which changes in the capacity for emotion regulation over the course of therapy relate to individual differences in emotion-related self-perceptions, degree of psychiatric distress, and the reasons for seeking psychotherapy remain understudied. This study explored the relations between changes in the capacity for emotion regulation over 8 months of psychotherapy, as defined by all subscales of the Difficulties for Emotion Regulation Scale, trait emotional intelligence and psychological distress. In addition, this study examined whether changes in the capacity for emotion regulation differed between patients reporting at least one regulation treatment goal and those reporting other goals. Data were collected as part of an ongoing program evaluation at an urban community-based mental health clinic. Self-report questionnaires were completed by 74 patients prior to beginning psychotherapy and after completing 8 months of psychotherapy. We found that higher trait emotional intelligence and lower psychological distress were related to improvements in emotion regulation. Moreover, the capacity for emotion regulation, particularly emotional awareness and limited access to emotion regulation strategies, worsened among individuals who reported at least one regulation treatment goal relative to those who reported other goals. As such, an initial phase of psychotherapy that focuses on integrating skills and self-awareness of emotional sensations prior to or in conjunction with embarking on an open-ended exploratory treatment is recommended.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Emotion regulation corresponds to the individual’s ability to identify and modulate emotional experiences and improvements thereof over the course of psychotherapy are associated with the reduction in psychiatric symptoms across multiple diagnoses (Sloan et al. 2017). Stated differently, many mental disorders are considered disorders of emotion regulation due to difficulties within the individual to identify and modulate emotional experiences. In this vein, studies have found that improvements in emotion regulation over the course of a psychotherapy treatment or targeted intervention are associated with a reduction in psychiatric symptoms across a range of diagnoses (Sloan et al. 2017).
While emotion regulation can be learned throughout the life course, including in adulthood, the development of emotion regulation is rooted in an individual’s earliest relationship. Through this relationship, the child’s internal experiences are contained and regulated by the caregiver who mirrors back to the child the child’s affective states. These moments set the foundation for the child to learn to contain and regulate their own experiences. In contrast, the absence of these early life experiences can result in difficulties with emotion regulation and vulnerability for psychopathology over the life course (Bateman and Fonagy 2016). Relatedly, attachment within the therapeutic relationship may provide a unique opportunity for adults to nurture self-regulatory capacities that were underdeveloped in childhood.
Emotional Intelligence as the Foundation for Emotion Regulation
One dominant framework of emotion regulation is Gratz and Roemer’s (2004) conceptualization of emotion regulation as a multidimensional construct consisting of four dimensions: (i) awareness and understanding of emotions, (ii) acceptance of emotions, (iii) ability to engage in goal directed, rather than impulsive, behavior in the context of negative emotions, and (iv) utilization of emotion regulation strategies. This model of emotion regulation includes intercorrelated attributes of emotion regulation (operationalized by the six subscales of the Difficulties in Emotion Regulation Scale; DERS) that together encapsulate the overarching construct (Hallion et al. 2018). While there is growing consensus regarding the centrality of emotion regulation to psychological well-being, how to define and operationalize emotion regulation remains an active debate (Sloan et al. 2017).
Importantly, data suggests that the Awareness subscale of the DERS included by Gratz and Roemer (2004) has a different pattern of association to the other subscales of emotion regulation, as well as to related constructs such as depression (Hallion et al. 2018). In this vein, recent studies have found that a five-factor model of emotion regulation, which excludes the Awareness subscale, fits the data best (Hallion et al. 2018). If the awareness dimension does in fact represent a different latent construct, including this dimension as part of the total score for emotion regulation may misconstrue the relationship between emotion regulation and covariates. Nevertheless, to date, Awareness remains a facet of Gratz and Roemer’s framework for emotion regulation and continues to be included in studies examining emotion regulation as a broad construct.
There is also increasing evidence of the link between Gratz and Roemer’s (2004) approach to emotion regulation and trait emotional intelligence. Trait emotional intelligence is a construct that refers to an individual’s understanding, modulating, and use of emotions (Petrides and Furnham 2003). Trait emotional intelligence consists of four dimensions: Well-being, self-control, emotionality, and sociability (Petrides and Furnham 2003). Emotionality (defined as the perception and expression of emotions) is particularly foundational to the capacity for emotion regulation, given that an awareness of an emotion precedes one’s ability to modulate that emotion.
Trait emotional intelligence and emotion regulation are strongly associated with psychological health. As discussed above, individuals who have difficulty with emotion regulation are more vulnerable to a range of psychopathology. Having higher trait emotional intelligence is protective against psychological distress (Gugliandolo et al. 2015; Petrides et al. 2016; Rudenstine and Espinosa 2018). Given the inextricable link between these two constructs, controlling for trait emotional intelligence allows for a purer assessment of how the capacity for emotion regulation changes throughout psychotherapy (Sarrionandia et al. 2015). Further, exploration into the relation between emotion regulation and psychopathology when controlling for trait emotional intelligence has the potential to inform prevention and intervention efforts that bolster emotion regulation specifically in the context of trait emotional intelligence and subsequently improve psychological health overall.
Treatment Goals
Treatment goal analysis can provide a framework for case conceptualization and examining relevant psychotherapeutic outcomes (Silberschatz 2015). Patient-reported goals, specifically, capture what patients wish to gain from psychotherapeutic treatment. In this way treatment goal content provide one framework for understanding how to assess meaningful treatment improvements as well as to examine the relations between goal quality and goal attainment.
Importantly, clinicians across theoretical orientations conceptualize treatment goals differently (Lindhiem et al. 2016; Schöttke et al. 2014). Schöttke et al. (2014) found that therapists working from a cognitive behavioral therapy framework formulated goals relating to coping with specific problems and symptoms, while therapists using psychodynamic psychotherapy formulated more interpersonal goals and goals related to personal growth. In this vein, treatment goals may lend themselves more (or less) naturally to particular treatment approaches (Schöttke et al. 2014). Further, it may be especially important to attend to patient goals within specific presenting problems and diagnoses in order to provide targeted treatment according to the patient’s current needs.
Studies also suggest a specific relation between patient-reported treatment goals and patient psychopathology. For example, individuals who primarily endorse anxiety symptoms tend to report symptom-level treatment goals, whereas treatment goals for individuals who struggle with depression are more likely to be related to interpersonal themes (e.g., intimacy, boundaries; Holtforth et al. 2009). Although studies have explored the statistical relation between patient-reported treatment goals and psychopathology or treatment modality, to the best of our knowledge to date, no study has examined differences between regulation and non-regulation-focused treatment goals and treatment outcomes.
Present Study
Based on the above, further exploration into the significant role of emotion regulation across a psychotherapy treatment is warranted. This study was an exploratory analysis to examine associations between changes in emotion regulation, trait emotional intelligence and psychological distress over 8 months of therapy, as well as the extent to which changes in emotion regulation varied between patient-reported treatment goals coded into two categories (regulation versus non regulation-focused). We hypothesized that higher trait emotional intelligence and lower psychological distress would relate to improvements in emotion regulation over the 8 months of therapy. Moreover, we hypothesized that individuals who reported a regulation-focused treatment goal would demonstrate an improvement in emotion regulation over time due to the patient’s stated intentions to address difficulties with regulation. In contrast, we anticipated that individuals who did not report a regulation-focused treatment goal would not demonstrate a significantly consistent pattern of change in emotion regulation. In other words, we expected emotion regulation to remain the same, improve, or worsen with no predictable pattern among those who reported no regulation treatment goals. Given the exploratory nature of this work, specific hypotheses pertaining to how each dimension of emotion regulation as defined by the DERS subscales, would change over 8 months of treatment were undefined. Including an analysis of patient-reported treatment goals as a part of this exploration has the potential to identify subtypes of patients with regulatory issues at the onset and during the course of treatment. The findings from these analyses will contribute to the growing discourse on the role of treatment goals in clinical assessment and treatment planning as well as to the capacity for emotion regulation throughout a psychotherapy treatment.
Methods
Participants and Procedures
Participants for this study were patients at an urban community-based mental health clinic in New York City who remained in psychotherapy treatment for at minimum 8 months. The clinic is run by the clinical psychology doctoral program at The City College of New York which has a strong commitment to training psychodynamic oriented psychologists. (For additional information about the theoretical and clinical technique courses provided by this doctoral program, visit: https://www.ccny.cuny.edu/psychology/welcome). In this vein, the clinic offers open-ended (no session limit) psychotherapy. The treatment approximates what is described by Shedler (2010), p. 99–100 in terms of: “Focus on affect and expression of emotion…Exploration of attempts to avoid distressing thoughts and feelings… Identification of recurring themes and patterns…Discussion of past experience (developmental focus)…Focus on interpersonal relations…Focus on the therapy relationship; Exploration of fantasy life.” Therapists at The Psychological Center are doctoral students in the clinical psychology doctoral program at The City College of New York. All therapists receive 1 h/week per patient of in-person supervision provided by a licensed clinical psychologist in New York City who identify as psychodynamic in orientation.
All patients completed a battery of questionnaires on a computer at The Psychological Center prior to beginning psychotherapy, as well as every 4 months while they received clinical services at the clinic. This study examined change in emotion regulation after 8 months of psychotherapy, therefore the data used in this study were completed prior to starting psychotherapy and after 8 months of psychotherapy. At no risk to themselves and/or risk of losing services, patients were allowed to leave blank any question and decline to provide consent to have their deidentified data included in research publications. Of the 92 patients who completed at minimum 8 months of psychological treatment at the clinic at the time that this study was conducted, three declined to provide consent and 15 did not complete in its entirety at least one of the measures used in this study due to administrative or technological error (e.g. lost internet connection, a measure erroneously not included in questionnaire packet). The final sample size for this study was 74. Patients were on average 31.70 years old (SD = 9.22). The sample was predominantly female (72.9%) with at least a 4-year undergraduate degree (69.4%) and with either full-time or part-time employment (84.3%). The ethnic composition of the sample was 32.2% European American, 25.0% African or African American, 23.8% Latinx or Hispanic, and 19.0% Other (the other category includes those who identify as “mixed”, Asian and Native American). Approximately half of the sample (53.3%) reported household incomes below $40,000, and 21.3% reported household incomes below $20,000. The entire sample can be defined as urban as they all live within New York City. The vast majority (90.6%) reported at least one adverse childhood experience and 46.9% reported 4 or more. Importantly, a score of 4 or more adverse childhood experiences has been found to be significantly associated with more deleterious mental and physical health outcomes (Rudenstine and Espinosa 2018). The institutional review board of The City College of New York approved of the study protocol and all associated procedures.
Measures
Difficulties in Emotion Regulation Scale (DERS)
The DERS is a reliable and valid 36-question self-report measure aimed at assessing various maladaptive emotion regulation strategies (Gratz and Roemer 2004). Items are presented on a five-point Likert scale ranging from one (almost never) to five (almost always), Sample items include “I am clear about my feelings,” “When I’m upset I acknowledge my emotions”, and “When I’m upset, I feel like I can remain in control of my behaviors.” The questionnaire yields an overall score, as well as six subscale scores that relate to cognitive and behavioral dimensions of emotion regulation: (i) nonacceptance of emotional responses (tendency to have a negative reaction to one’s own distress); (ii) difficulties engaging in goal-directed behavior (difficulty focusing on tasks in the context of negative emotions); (iii) impulse control difficulties (lack of control over one’s behavior in the context of one’s own negative emotions); (iv) lack of emotional awareness (inattention to negative emotions); (v) limited access to emotion regulation strategies (belief that there is little one can do to regulate oneself when upset); and (vi) lack of emotional clarity (the degree to which an individual understands his emotions). Higher scores suggest greater problems with overall and subscale specific emotion regulation. The Cronbach’s alpha internal consistency estimates for this sample at baseline and 8-month follow-up, respectively, were high (DERS total α = 0.89 and 0.90; DERS nonacceptance α = 0.93 and 0.91, DERS goals α = 0.87 and 0.89, DERS impulse α = 0.85 and 0.87, DERS awareness α = 0.83 and 0.84, DERS strategies α = 0.90 and 0.92, DERS clarity α = 0.83 and 0.81).
Trait Emotional Intelligence Questionnaire-Short Form (TEIQue-SF)
The TEIQue is a widely used, psychometrically sound, measure of dispositional emotional intelligence (Cooper and Petrides 2010; Petrides et al. 2009). Items are presented in a seven-point Likert scale ranging from one (strongly disagree) to seven (strongly agree). Sample items include: “Expressing my emotions with words is not a problem for me” and “I often find it difficult to see things from another person’s viewpoint.” This 30-item self-report measure yields an overall trait EI score, with higher scores reflecting higher levels of trait emotional intelligence. The Cronbach’s alpha internal consistency estimate for the TEIQue-SF was high, α = 0.91 and 0.89 (baseline and 8-month follow-up, respectively).
The Brief Symptom Inventory (BSI)
The BSI is a 53-item, self-report measure of the degree to which individuals have experienced distress over the last week. Responses range from zero (not at all) to four (extremely) (Derogatis 1993). Symptoms assessed include “nervousness or shakiness inside”, “poor appetite”, “feeling inferior to others”, and “never feeling close to another person.” The scale yields multiple global distress indices and nine symptom subscales. The psychometric properties of the scale and all subscales have been documented in studies using clinical samples, which indicate Cronbach’s alpha internal consistencies over 0.70 for all subscales and test–retest reliabilities between 0.68 and 0.91 (Derogatis 1993). In this sample, Cronbach’s alpha internal consistency estimates for the BSI were high (α = 97 for both baseline and 8-month follow-up). The mean BSI scores were within the clinical significant range (Derogatis 1993).
Treatment Goals
Prior to beginning psychotherapy treatment, patients were asked to state in their own words their goals for treatment with the following prompt: “Please list three things you hope to work on while in therapy at The Psychological Center”. Qualitative analysis of reported treatment goals was conducted by using a generative and exploratory data analytic approach (Grounded Theory) in order to best understand the treatment goals reported (Charmaz 2014). Grounded Theory analysis requires three phases of data evaluation: (1) Open Coding to first group the raw treatment goal data; (2) Axial Coding to reflect the prominent themes of the cumulative data; and (3) Selective Coding which is the overall thematic organization related to theoretical underpinnings.
Participants (N = 74) reported a total of 216 raw treatment goal units. Initial coding of treatment goals using Open Coding by three independent raters led to the development of a total of nine Axial Code treatment goal categories across raters. Raters for the Open Coding included one clinical psychologist with a background in qualitative and quantitative data analysis (Rudenstine) and two advanced clinical psychology doctoral students with training in qualitative and quantitative data analysis. Axial Coding was completed by the aforementioned clinical psychologist and one of the two doctoral students. All raters were trained in the grounded theory research methodology. As a result of subsequent discussion between the raters, the nine Axial Codes were condensed into six Selective Coding categories connecting a thematic organization to theoretical underpinnings.
The final six treatment goal categories were: (1) psychiatric symptoms (i.e., “my anxiety”, “social anxiety”,); (2) interpersonal (i.e., “discuss my problems in my family”, “relationship skills, ability to maintain friendships, possibility of being able to form romantic relationships”); (3) intrapersonal (i.e., “trusting myself, feeling capable”, “learn more about what I go through/myself”); (4) life responsibilities (i.e., “juggling work/school while learning to support myself without parental assistance”, “work balance”); (5) regulation (i.e., “regulating my emotions”, “controlling a stressed response which results in anger and/or depression”), and (6) narrative building (i.e., “my past; I was in a physically abusive relationship and although I feel safe and health I still live with that trauma in some ways”, “Making connections from my past and present to help me understand why I feel the way I feel, so I can help heal from it and experience less daily distress”). Treatment goal coding within the categories was conducted by two of the three raters, which yielded moderate agreement, Cohen’s Kappa (k) value of 0.788 (p < 0.001). Disagreement was found on 44 individual goals. Following a recoding of these goals based on discussion of specific questions and discrepancies, k = 0.98, (p < 0.001), indicating high agreement. Remaining discrepancies (2) were reconciled and recoded. For this study, we created a binary variable where 1 equals the patient reported at least one regulation treatment goal (n = 36 patients) and 0 equals the patient did not report any regulation treatment goal (n = 38 patients).
Data Analysis
Regression analyses for repeated measures, specifically generalized estimating equations (GEE; Muth et al. 2016), were used to examine the associations between changes in trait emotional intelligence, psychological distress and emotion regulation over the course of therapy, as well as compare changes in emotion regulation from baseline to follow-up between treatment goal groups. All GEE regressions defined an identity link function, with a normal distribution, and correlations between observations were assumed to adhere to the compound symmetry assumption of general linear models (i.e., exchangeable correlation structure). Inference was based on robust standard errors, which address any misidentification of the correlation structure (Muth et al. 2016). The normality assumption to ensure GEE efficiency was confirmed via Shapiro Francia tests, which produced test statistics with p values > 0.05 for all residuals. Item-level missing cases were lower than 6%. According to little’s MCAR test (χ2(179) = 161.89, p = 0.82) missing cases were missing completely at random, which is an important assumption of GEE models. Therefore, we imputed missing values using the expectation maximization (EM; Fernández-García et al. 2018) algorithm. All analyses were conducted using STATA version 15 (StataCorp 2015).
Analytical power computations assuming moderate effects, a significance level of 0.05 and two-tailed tests indicated that a sample size of 74 yielded statistical power of 0.80 or above in t-tests and GEE models, including the comparison of changes in DERS over time between treatment goals groups. All power computations were conducted using the software R (R Core Team 2013). Calculations of power for t-tests were conducted using the pwr package (Champely 2006), which is based the framework proposed by Cohen. Similarly, power analysis calculations for the effects obtained in GEE models, including the interaction of treatment goals and the time effect in GEE regressions were conducted using the long power package (Donohue et al. 2016).
Results
Sample Characteristics and Bivariate Relations
Table 1 presents means and standard deviations (SD) for all psychometric measures for the entire sample at baseline and at 8-month follow-up. As shown, on average, patients exhibited a decrease in symptoms of psychological distress from baseline to follow-up. Importantly, on average, patients’ level of psychological distress went from clinically significant to not clinically significant (Derogatis 1993). No other changes from baseline to follow-up were statistically significant for the entire sample. In addition, mean differences in trait emotional intelligence, BSI or DERS between the two treatment goal groups were not statistically significant at the 95% confidence level.
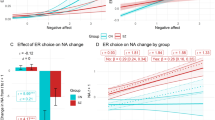
Generalized Estimating Equations Results
Table 2 presents the results from seven individual GEE regressions assessing the associations between trait emotional intelligence, psychological distress and changes in DERS (total and for each subscale) over time, while comparing changes in DERS between individuals with and without regulation as a treatment goal. As hypothesized, higher trait emotional intelligence was related to lower DERS, and higher BSI was related to higher DERS, with the exception of awareness, which did not relate to BSI. In accordance with Table 1, the time effect, which assesses changes in DERS on average, was not significant in any of the models. However, the interaction between treatment goals and time, assessing average differences in the trajectory of change in DERS between treatment goal groups was significant for DERS total, awareness and strategies. In combination, the lack of time effect and significant interaction between time and treatment goals indicate that the two treatment goal groups exhibited different patterns of change in DERS total, awareness and strategies. Upon close inspection, and in contrast to our hypothesis, individuals without regulation as a treatment goal experienced a decrease in DERS, whereas those with regulation as a treatment goal had increased DERS scores (see Table 2). According to Wald tests these slopes were significantly different from each other for all three DERS subscales (see note on Table 2).
Discussion
Using a help-seeking, urban and low socioeconomic status clinical sample, this study gauged the extent to which trait emotional intelligence and psychological distress relate to changes in the capacity for emotion regulation (operationalized by DERS total score and each subscale) over 8 months of psychotherapy, and whether the trajectory of changes in DERS varied between individuals with different treatment goals. We chose to examine each of the DERS subscales in addition to the total score because the capacity for emotion regulation relies on multiple processes (i.e., awareness and understanding of emotions, acceptance of emotions, impulse control and goal-directedness, and access to regulation strategies). Accordingly, such focus provides insight into different facets of emotion regulation that may be a weakness or a strength within the individual and can inform the choice of intervention (Hallion et al. 2018). Nonetheless, the subscales were not completely redundant as identified by variance inflation factors (VIFs) no larger than 2.9.
As hypothesized, higher emotional intelligence and lower psychological distress were significant correlates of the capacity for emotion regulation. These findings are in accordance with the literature (Gugliandolo et al. 2015; Petrides et al. 2016; Rudenstine and Espinosa 2018; Sarrionandia et al. 2015) and highlight the importance of targeting trait emotional intelligence and emotional intelligence in an effort to improve psychological health.
On average, the capacity for overall emotion regulation as well as the awareness and strategies subscales improved over the course of 8 months of psychotherapy amongst patients without regulation as a self-identified treatment goal. That overall emotion regulation, awareness, and strategies improved echoes previous studies that found that psychotherapy fosters emotion regulation among patients (Rabinovich 2016). While further exploration into the mechanisms underlying this change is needed, there are several possible explanations for these findings. The attachment-like relationship between patients and their therapists may nurture the capacity for self-regulation in the patient through the patient’s experience of being mentalized by the therapist as well as being engaged in a synchronous interaction (Koole and Tschacher 2016). Similarly, moments in which the therapist seeks clarification about a patient’s emotional experience may help the patient develop greater awareness of their feelings (awareness). Additionally, the process of identifying alternative coping strategies or direct suggestions made by the therapist to the patient may offer the patient a newfound confidence in his ability to regulate himself when distressed (strategies; Linehan 2015; Neacsiu et al. 2014).
Notwithstanding, patients who reported at least one regulation treatment goal had the opposite trajectory. As stated in “Measures” section, the awareness subscale reflects an individual’s level of awareness (very aware or inattentive) to emotional responses. Strategies refers to the belief that there is something one can do to regulate themselves when distressed. The notion that some patients’ psychiatric symptoms worsen over the course of therapy, and in particular over the first year, has been well-documented (Owen et al. 2015). In addition, having greater difficulty with emotion regulation at the onset of psychotherapy may leave the individual prone to feeling flooded by the emotions stirred up in therapy and yet unable to cope with the emotions or process the content (Rabinovich 2016). Therefore, those individuals who feel ill-equipped to contain their emotional experiences may benefit from specific interventions in order to affect a measurable change as measured by the DERS (Neacsiu et al. 2014).
Given the exploratory nature of this study, there is limited empirical data to draw upon in explaining the results that emerged counter to our expectations. We had anticipated finding an improvement in emotion regulation among those patients who reported a desire to work on regulation-related issues, if for no other reason than their treatment goal would inform the focus of the treatment. It is plausible that a behavior or symptom-oriented treatment where specific skills were taught in each session that targeted the presenting problem (dysregulation) might have resulted in improvements in emotion regulation over the 8-month period. However, the psychotherapy provided to the study’s patients emphasized, among other things, intrapsychic and unconscious conflicts and their role in development, the identification of defenses, and internal representations of experiences and relations. Therefore, it makes sense that emotion regulation worsened among those who reported a regulation-focused treatment goal. For example, difficulty in emotion regulation may result in these patients becoming dysregulated by the therapy content and yet being unable to identify and control the subsequent emotions. Others argue that it is through this process of being exposed to anxiety-provoking content coupled with the experience of being contained by the therapist that the patient develops the capacity for regulation over time (Rabinovich 2016).
Additional psychotherapy research is needed to examine the mechanisms underlying change in emotion regulation throughout psychotherapy. To the best of our knowledge this is the first study to examine if patient reported treatment goals may provide insight into how the capacity for emotion regulation will change over 8 months of psychotherapy. Therefore, complementing the empirical work above, we call upon foundational and highly respected psychological theory to help us explain why a subgroup of patients who reported a regulation treatment goal demonstrated worse emotion regulation overall as well as DERS Awareness and Strategies over 8 months of treatment.
Identifying a regulation treatment goal may suggest, among other things, a desire to gain control over one’s emotions, behaviors, and/or thoughts. As evidenced by dialectical behavior therapy (DBT), the desire to control emotional experiences often is due to finding these experiences to be overwhelming (Linehan 2015). For individuals who do not experience the world to be a benign place, the therapeutic environment may feel at best uncomfortable, and at worst, threatening. A safe and predictable holding environment helps us tolerate our inner life (Elliot and Prager 2016). Nevertheless, if the therapeutic environment and relationship are perceived to be uncomfortably unknown, they will fail at first to offer the necessary containment to the patient (Rabinovich 2016). The lack of such an environment may result in the patient decompensating further or in the avoidance of one’s inner life by employing a false self (Elliot and Prager 2016). Importantly, because the patients’ overall functioning did not significantly worsen over the first 8 months of treatment, it is plausible that defenses (i.e., avoidance) were unconsciously employed to cope with the anxiety stirred up by the treatment itself and in turn prevent further decompensation. The result is being less in touch with oneself, operationalized by reporting greater inattention to one’s emotion responses (awareness). Lastly, the fear that one cannot regulate themselves when distressed may in turn preclude them from being open to trying, let alone considering, new approaches that could increase their internal sense of control (strategies). We suggest that these individuals may cope with intense affect elicited by the therapeutic process, including the transference to the therapist, by avoidance. This affective avoidance is represented by the Awareness subscale in the DERS. Neither of these explanations propose this subgroup of individuals will fail to thrive throughout a psychological treatment. Rather, as these individuals internalize a benevolent experience with their therapist, they will likely become less fearful of their internal experiences and in turn present as psychologically healthier. Future empirical research is needed to verify these claims and theoretical expositions.
Several limitations are worth mentioning. First, the current study examined a help-seeking, low SES, urban clinical population; caution should be used when generalizing these findings. Second, bias or perceived ability for emotion regulation or emotional intelligence may be present due to the use of self-report measures. Third, while the training provided to therapists at the clinic is grounded in psychodynamic principles, the clinic does not systemically document the techniques and interventions used in each treatment. Fourth, individual characteristics of the therapists are not included in these analyses, which may reduce generalizability of this study, and future studies that account for therapist characteristics are warranted. Fifth, whereas analytical power was adequate to identify moderate effects, power was not adequate to identify small effects, given our current sample size. Relatedly, although we were able to confirm the directionality of the results presented here using the complete cases data set, we were unable to match them all in terms of statistical significance at a 95% confidence level, although we confirmed them at a lower confidence level (i.e., 90%). The non-significant findings at this confidence level, given that the numerical estimates were similar in magnitude and direction, highlight that differences were undetected with the complete cases data set possibly due to small sample size, large variations or some additional unidentified factors, rather than highlighting non-existent differences (Amrhein et al. 2019). Sixth, given that the current study examines outcomes from two time points, we are unable to determine causality or temporal precedence. Seventh, we do not include diagnoses for the sample, however the BSI meaningfully demonstrates that on average the level of psychological distress for the sample was clinically significant before beginning psychotherapy. These issues present limitations in our analyses, which should be replicated in future studies with larger samples. Notwithstanding these limitations, the current study contributes meaningfully to the psychotherapy research literature. In spite (or because) of their difficulties with regulation, individuals who report a regulation related treatment goal may respond to the affect aroused by psychological treatments by becoming inattentive of their affective experiences and (temporarily) resistant to trying new and adaptive coping strategies.
There are a number of practical and clinical implications of these findings. Clinicians, especially at the onset of therapeutic training, benefit from insight into the nuance of ways patients seem to respond to the beginning months of treatment. Specifically, for individuals who report regulation-related treatment goals, the integration of skill-building at the onset of psychological treatment may be critical to offset the use of defensive processes (i.e. avoidance) to tolerate the challenging affective experience of therapy. Informed by these data, clinicians can structure the start of treatment by integrating skills and self-awareness of emotional and physical sensations (e.g. mindfulness) prior to or in conjunction with embarking on an open-ended exploratory treatment. Moreover, a psychodynamic focus on the underlying contributors to affect dysregulation would be aided by attention to and containment of patient’s surface level distress, which simultaneously also would meet these patients’ therapeutic goals. We suggest that this approach may allow the therapy to progress in a way that attends to the patient’s emotion regulation difficulties while setting the stage for safer exploration of deeper conflicts that may greatly impact psychological suffering. In this way, a greater appreciation and use of patient reported treatment goals has the potential to inform initial phases of a therapeutic treatment, if not the entire course of treatment, as well as alert the therapist to the ways in which patients’ may respond to the unfolding therapeutic experience.
References
Amrhein, V., Greenland, S., & McShane, B. (2019). Scientists rise up against statistical significance. Nature, 567, 305–307.
Bateman, A., & Fonagy, P. (2016). Mentalization-based treatment for personality disorders. Oxford: Oxford University Press.
Champely, S. (2006). The pwr package: Basic functions for power analysis. R package version 1.0.
Charmaz, K. (2014). Constructing grounded theory (2nd ed.). Thousand Oaks, CA: Sage Publications.
Cooper, A., & Petrides, K. V. (2010). A psychometric analysis of the trait emotional intelligence questionnaire-short form (TEIQue-SF) using item response theory. Journal of Personality Assessment, 92, 449–457. https://doi.org/10.1080/00223891.2010.497426.
Derogatis, L. R. (1993). Brief symptom inventory (BSI): administration scoring and procedures manual (3rd ed.). Minneapolis, MN: National Computer Systems.
Donohue, M. C., Gamst, A., C., & Edland, S. D. (2016). Package longpower: Sample size calculations for longitudinal data. R package version 1.0-16.
Elliot, A., & Prager, J. (2016). The Routledge handbook of psychoanalysis in the social sciences and humanities. New York: Routledge.
Fernández-García, M. P., Vallejo-Seco, G., Livácic-Rojas, P., & Tuero-Herrero, E. (2018). The (ir)responsibility of (under)estimating missing data. Frontiers in Psychology, 9, 556. https://doi.org/10.3389/fpsyg.2018.00556.
Gratz, K. L., & Roemer, E. (2004). Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. Journal of Psychopathology and Behavioral Assessment, 26(1), 41–54. https://doi.org/10.1007/s10862-008-9102-4.
Gugliandolo, M. C., Costa, S., Cuzzocrea, F., Lacran, R., & Petrides, K. V. (2015). Trait emotional intelligence and behavioral problems among adolescents: A cross informant design. Personality and Individual Differences, 74, 16–21.
Hallion, L. S., Steinbman, S. A., Tolin, D. F., & Dieenbach, G. J. (2018). Psychometric properties of the Difficulties in Emotion Regulation Scale (DERS) and its short forms in adults with emotional disorders. Frontiers in Psychology, 9, 1–12. https://doi.org/10.3389/fpsyg.2018.00539.
Holtforth, M. G., Wyss, T., Schulte, D., Trachsel, M., & Michalak, J. (2009). Some like it specific: The difference between treatment goals of anxious and depressed patients. The British Psychological Society, 82, 279–290.
Koole, S. L., & Tschacher, W. (2016). Synchrony in psychotherapy: A review and an integrated framework for the therapeutic alliance. Frontiers in Psychology, 7, 1–17. https://doi.org/10.3389/fpsyg.2016.00862.
Lindhiem, O., Bennett, C. B., Orimoto, T. E., & Kolko, D. J. (2016). A meta-analysis of personalized treatment goals in psychotherapy: A preliminary report and call for more studies. Clinical Psychology: Science and Practice, 23(2), 165–176. https://doi.org/10.1111/cpsp.12153.
Linehan, M. (2015). DBT skills training manual (2nd ed.). New York: Guilford Press.
Muth, C., Bales, K. L., Hinde, K., Maninger, N., Mendoza, S. P., & Ferrer, E. (2016). Alternative models for small samples in psychological research: Applying linear mixed effects and generalized estimating equations to repeated measures data. Educational and Psychological Measurement, 75(1), 64–87.
Neacsiu, A. D., Eberle, J. W., Kramer, R., Wiesman, T., & Linehan, M. M. (2014). Dialectical behavior therapy skills for transdiagnostic emotion dysregulation: A pilot randomized controlled trial. Behaviour Research and Therapy, 59, 40–51. https://doi.org/10.1016/j.brat.2014.05.005.
Owen, J., Adelson, J., Budge, S., Wampold, B., Kopta, M., Minami, T., et al. (2015). Trajectories in change in psychotherapy. Journal of Clinical Psychology, 71(9), 817–827. https://doi.org/10.1002/jclp.22191.
Petrides, K. V., & Furnham, A. (2003). Trait emotional intelligence: Behavioural validation in two studies of emotion recognition and reactivity to mood induction. European Journal of Personality, 17, 39–50. https://doi.org/10.1002/per.446.
Petrides, K. V., Mikolajczak, M., Mavroveli, S., Sanchez-Ruiz, M. J., Furnham, A., & Perez-Gonzales, J. C. (2016). Developments in trait emotional intelligence research. Emotion Review, 8, 335–341.
Petrides, K. V., Stough, C., Saklofske, D. H., & Parker, J. D. (2009). Psychometric properties of the trait emotional intelligence questionnaire (TEIQue). Advances in the assessment of emotional intelligence. New York: Springer.
R Core Team. (2013). R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing.
Rabinovich, M. (2016). Psychodynamic emotion regulation in view of Wolpe’s desensitization model. The American Journal of Psychology, 129(1), 65–79.
Rudenstine, S., & Espinosa, A. (2018). Examining the role of trait emotional intelligence on psychiatric symptom clusters in the context of lifetime trauma. Personality and Individual Differences, 128, 69–74. https://doi.org/10.1016/j.paid.2018.02.029.
Sarrionandia, A., Mikolajczak, M., & Gross, J. J. (2015). Integrating emotion regulation andemotional intelligence traditions: A meta-analysis. Frontiers in Psychology, 6, 1–27. https://doi.org/10.3389/fpsyg.2015.00160.
Schöttke, H., Trame, L., & Sembill, A. (2014). Relevance of therapy goals in outpatient cognitive-behavioral and psychodynamic psychotherapy. Psychotherapy Research, 24(6), 711–723. https://doi.org/10.1080/10503307.2014.881578.
Shedler, J. (2010). The efficacy of psychodynamic psychotherapy. American Psychologist, 65(2), 98–109. https://doi.org/10.1037/a0018378.
Silberschatz, G. (2015). Improving the yield of psychotherapy research. Psychotherapy Research, 27(1), 1–13. https://doi.org/10.1080/10503307.2015.1076202.
Sloan, E., Hall, K., Moulding, R., Bryce, S., Mildred, H., & Staifer, P. K. (2017). Emotion regulation as a transdiagnostic treatment construct across anxiety, depression, substance, eating, and borderline personality disorders: A systematic review. Clinical Psychology Review, 57, 141–163. https://doi.org/10.1016/j.cpr.2017.09.002.
StataCorp. (2015). Stata statistical software: Release 15. College Station, TX: StataCorp.
Acknowledgements
We would like to thank all members of the INTERSECT Lab whose contributions are invaluable to the success of the Psychotherapy Evaluation and Clinical Effectiveness (PEACE) Program.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Rudenstine, S., Espinosa, A., Cancelmo, L. et al. Psychological Correlates of Change in Emotion Regulation Over 8 Months of Psychotherapy. J Contemp Psychother 49, 245–254 (2019). https://doi.org/10.1007/s10879-019-09435-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10879-019-09435-6