
Abstract
Among various methods for measuring the plasma volume (PV), the indocyanine green (ICG) dilution technique is a relatively less invasive method. However, the ICG method is rather cumbersome because 10 blood samples need to be obtained within a short time after ICG administration. Thus, reducing the frequency of blood sampling while maintaining the accuracy would facilitate plasma volume measurement in clinical situations. We here developed a modified method to measure plasma volume using 2260 ICG plasma concentration data from 115 surgical patients. The mean relative error (MRE) and the percentage of cases with relative error (RE) greater than 5% in total (PRE) were used to quantify the difference between plasma volumes obtained by the original and modified methods. RE was determined as follows. RE(%) = (PV obtained by original method (PVoriginal)—PV obtained by modified method (PVmodified))/PVoriginal × 100. PVmodified was assumed to be equal to PVoriginal when the RE was < 5%. When the number of samples selected for the plasma volume estimation was 4 or less, the PRE was mostly 10% or more. Five out of the 10 blood samples (order: 1st, 2nd, 3rd, 9th, and 10th) showed similar accuracies with the plasma volume obtained by the original method (original: 2.72 ± 0.64 l, modified: 2.72 ± 0.65 l). This modified method may be able to aptly replace the original method and lead to a wider clinical application of the ICG dilution technique. Further validation is needed to determine if the results of this study may be applied in other populations.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Maintaining euvolemia in patients is of critical clinical importance, because hypovolemia leads to hypotension or tachycardia, and hypervolemia due to fluid overdose leads to tissue edema or respiratory compromise [1]. Therefore, various efforts have been made to properly maintain the blood volume of patients; unfortunately, no commercial equipment has yet been developed to monitor the plasma volume in real-time.
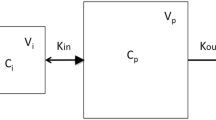
The indocyanine green (ICG) dilution technique has been used to measure the plasma volume (Fig. 1), but the method is quite cumbersome because it requires a total of 10 blood samplings every 20 s for 3 min [2]. If the frequency of blood collection can be reduced, the ICG dilution technique may be applied in a wider range of clinical settings. In our previous study, plasma volumes of 118 surgical patients were measured before and after surgery using the original ICG dilution technique [3]. Using these plasma volume data, we sought to develop a modified method that requires fewer blood samplings for producing comparable measurements.

Estimation of plasma volume using the original indocyanine green (ICG) dilution technique. Cp0 indicates the theoretical concentration at t0 (time of ICG administration). The concentration was derived from mono-exponential extrapolation of concentrations using 10 samples obtained from 2 to 5 min of ICG administration. Each sample was taken at 20-s intervals. Ten samples were named from Cp1 to Cp10. For example, Cp1 and Cp10 indicate plasma concentration at 2 and 5 min after the administration of ICG, respectively. The solid grey line represents the regression line between the 10 plasma concentrations from Cp1 to Cp10
In this study, we aimed to determine how many blood samples can be reduced using the existing plasma volume measurement data. Moreover, we tried to identify the order in which blood samples should be drawn within the same frequency of blood collection that allows for maximum accuracy.
2 Material and methods
2.1 Source of plasma volume measurement data
In order to modify the existing ICG dilution technique, we utilized the data related to plasma volume measurement from a previous study [3]. The previous study was approved by the institutional review board (IRB) of Asan Medical Center (#2012-0169) and registered on an international clinical trials registry platform (https://cris.nih.go.kr; KCT0001788) (Minerva Anestesiol. 2019, https://doi.org/10.23736/S0375-9393.19.13952-1). This current study was approved as a retrospective study by the IRB of Asan Medical Center (#2020-0631). Induction and maintenance of anesthesia were achieved in accordance with the institution's standard operating procedure [3]. Before the induction of anesthesia, a 20-gauge catheter was inserted in a radial artery for frequent blood sampling. In the contralateral arm, a 16-gauge angiocatheter was placed in the antecubital vein for ICG injection. Plasma volume was measured before and after surgery. Preoperative measurements were performed before the induction of anesthesia, and postoperative measurements were performed before transfer to the post-anesthesia care unit. Briefly, the original ICG dilution technique for plasma volume measurement is as follows [3]. ICG powder (25 g) was dissolved in 10 ml distilled water. ICG diluted to 2.5 mg/ml was prepared in a 10 ml syringe. ICG (0.25 mg/kg) was given to each patient as quickly as possible. Two minutes after injection of ICG, 3 ml of arterial blood was sampled using a heparinized syringe every 20 s for 3 min (10 samples total). After separation of plasma by centrifuging for 10 min at 3,500 rpm, the absorbance of the plasma sample at 805 nm was measured using a spectrophotometer (Double beam spectrophotometer U-2900®, Hitachi High-Technologies Global, Tokyo, Japan). Plasma ICG concentrations were estimated using calibration standard curves constructed from ICG solutions prepared to cover a plasma concentration of 0–1 mg/dl. Calibration standard curves were constructed every two weeks, except for periods when there was no patient enrollment. A total of 24 calibration standard curves were obtained throughout the study period, and the coefficient of determination (R2) ranged from 0.997 to 1.000. The measured ICG concentrations were plotted on a semilogarithmic graph. The resulting regression line was extrapolated to t0 (time of ICG administration) at the end of administration, and this theoretical concentration of ICG concentration at t0 (Cp0) was used to calculate the plasma volume. Plasma volume was calculated by dividing ICG amount by Cp0 (Eq. 1).
2.2 Statistical analysis
Statistical analysis was performed using the 236 plasma estimates obtained from 118 patients before and after surgery [3]. If the absolute value of the correlation coefficient between 10 ICG concentrations used to estimate one plasma volume on a semilogarithmic graph was lower than 0.9, it was considered an outlier and excluded from the analysis. In general, the correlation coefficient of the standard curve is higher than 0.95 [3, 4]. Ten of the 236 cases were excluded from the analysis (median absolute correlation coefficient: 0.82). A total of 2,260 plasma concentration data (10 plasma samples per plasma volume measurement × 226 cases) were included in the analysis.
For convenience, 10 plasma samples were named in order from Cp1 to Cp10. For example, Cp1 and Cp4 refer to plasma concentrations at 2 and 3 min after ICG administration, respectively. The original plasma volume (PVoriginal) value calculated using all 10 plasma concentrations were considered as the true value. Plasma volume estimated by reducing the number of samples with various combinations was considered as the modified plasma volume (PVmodified). Table 1 shows the possible number of combinations with which PVmodifed can be calculated; in total, there were 1,012 possible combinations. To define the difference between PVmodified and PVoriginal, the relative error (RE) was calculated for each combination as follows.
where PVorigianl,i is the PVoriginal of the ith case and PVmodified,i,j is the PVmodified of the ith case at the jth combination. There was a total of 228,712 REs (226 cases × 1012 combinations). If RE was less than 5%, PVmodified was assumed to be equal to PVoriginal; this means that if REi,j is greater than 5%, the plasma volume of the ith case at jth combination is clinically different from the original plasma volume, and the ith case of the jth combination is not suitable for substituting of the original ICG dilution technique.
Two parameters—the mean relative error (MRE) and the percentage of cases with RE (PRE) greater than 5% out of 226 in total—were used to quantify the degree of the difference between PVmodified and PVoriginal at each combination. MRE and PRE were defined as follows.
where MREj and PREj are MRE and PRE at the jth combination, respectively. The smaller the MRE and PRE values, the more likely it is to replace the original ICG dilution technique.
Based on the following three principles, we found a modified method that can replace the original method. First, PVmodified should not be clinically different from PVoriginal. Second, MRE and PRE should be as small as possible. Third, if the MRE and PRE are clinically similar, the combination with the smallest number of samples used to estimate the plasma volume is chosen.
Data are expressed as mean ± standard deviation for normally distributed continuous variables, median (25–75%) for non-normally distributed continuous variables, or count and percentage for categorical variables.
3 Results
A total of 2260 (226 cases × 10 concentrations/case) ICG plasma concentration data from 115 patients were analyzed. The physical characteristics of these patients are shown in Table 2. In the 226 cases, the median (25–75%) absolute value of correlation coefficient between 10 ICG concentrations used to estimate one plasma volume on a logarithm plot was 0.99 (0.98–1.0). The distributions of MRE and PRE in combinations of sample selection for plasma volume estimation are depicted in Fig. 2. As the number of samples selected for plasma volume estimation was increased, the variation of MREs decreased. When nine plasma concentrations were selected, all MREs were less than 5%. Also, the smallest MRE among the combinations of the selected sample numbers gradually decreased as the number of samples included in the plasma volume estimation was increased. On the other hand, the minimum PRE in each combination was 10% or more until four plasma samples were selected, whereas the minimum PRE was at most 1% when selecting five or more plasma samples. Although the plasma volume was estimated using the same number of plasma samples, high variability of MRE and PRE was observed, indicating that the order of samples included in the estimation is also important.

Distribution of the mean residual error (MRE, A) and percentage of cases with relative errors greater than 5% out of 226 (PRE, B) in the combinations of sample selection for plasma volume estimation. Gold circles indicate MRE or PRE in each combination (total number of combinations: 1012). Red squares represent the smallest MRE or PRE value in the combination of the number of samples selected
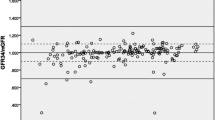
Table 3 shows the combinations with the minimum MRE and PRE for each sample number selected. By taking into account Fig. 2 and Table 3, it was possible to select five plasma samples out of ten, and the order was 1st, 2nd, 3rd, 9th, and 10th. In other words, the first three plasma samples and the latter two plasma sample data could yield similar plasma volume results with the original method in terms of accuracy. The mean ± SD plasma volumes obtained from the original and modified methods were 2.72 ± 0.64 and 2.72 ± 0.65, respectively. The plasma volumes obtained by the original method and the modified method are presented in Fig. 3. In almost all cases, the fold change of the plasma volume obtained by the modified method with respect to the plasma volume obtained by the original method was between 5%.

Plasma volume estimated by the original and modified methods. The solid green line represents the line of identity (y = x). The modified method used a total of five plasma concentrations at the 1st (Cp1), 2nd (Cp2), 3rd (Cp3), 9th (Cp9), and 10th (Cp10) time points
4 Discussion
In this study, we developed a modified ICG dilution method to replace the original technique for estimating plasma volume. Five out of the 10 blood samples showed similar accuracies with the plasma volume obtained by the original method. Of the 10 previous blood samples, the order of the selected samples was 1st, 2nd, 3rd, 9th, and 10th.
It would be beneficial to monitor the blood or plasma volume during fluid therapy. Radio-iodinated serum albumin and Evans blue have been used as tracers to measure the blood or plasma volume [5, 6]. However, these tracers do not allow for making measurements in short intervals due to radioactivity contamination or dye accumulation [7]. ICG is a cyanine dye used in determining the hepatic function and the blood flow in the liver and stomach [8]; ICG tightly binds to plasma proteins and becomes confined to the vascular system, and can thus be reliably used to measure blood or plasma volume. The estimated volume of distribution of ICG is the blood or plasma volume, and the blood volume can be converted to plasma volume using the hematocrit value [2]. Importantly, ICG has a short elimination half-life (approximately 4.7–5 min) [8], and thus has the advantage of being able to repeat plasma volume measurement in short intervals. Despite these characteristics of ICG, clinical application of the ICG dilution technique is still limited due to the complicated process of blood sampling and quantitation of ICG plasma concentration in the laboratory [7]. If the inconvenience of frequent blood collection can be reduced, the ICG dilution technique may be applied in a wider range of clinical settings.
In addition to the methods used in the current study, there are other methods for measuring blood volume. The pulmonary blood volume and circulating blood volume can be measured using the transpulmonary dye dilution method [9]. Since ICG was injected into the right atrium, it is necessary to insert a central venous catheter [9]. Blood volume can also be measured using commercialized PiCCO (Philips IntelliVue MP40 with PiCCO-technology module Philips Healthcare, Cleveland, Ohio, USA), which is a comparatively less invasive method than the pulmonary artery catheter [10]. However, an arterial catheter is placed in the descending artery via the femoral artery in this method [11]. An ultrasound dilution technology can measure the blood volume in critically ill patients by using an extracorporeal arteriovenous loop approach [12]. However, this method is more invasive than the method used in the current study.
The elimination pattern of ICG shows mono-exponential decay during the first 5 min after recirculation and then changes to biexponential decay [8, 13]. Therefore, ICG concentrations for 2 to 5 min after administration theoretically form a straight line by logarithmic conversion; in practice, however, the plasma concentrations of ICG obtained from biological samples do not form a perfectly straight line. Therefore, in order to correctly estimate the Cp0, 10 blood samples were taken in the original method. In this current study, when MRE and PRE were considered, we observed that the number of blood sampling of the original method could be reduced in half. A recent study on plasma volume measurement using ICG found that plasma volume can be accurately measured with only five samples [4]; unfortunately, no comparisons were made with the plasma volumes obtained with the original method. The authors argued that randomly selected five blood samples without specific evidence well-explained the decay curve of plasma ICG concentrations. The time point of blood sampling presented by the authors was to collect blood at an interval of 45 s, evenly dividing the 180 s from 2 to 5 min after the administration of ICG. However, as shown in Fig. 2, even with five samplings, the MRE and PRE differed greatly depending on how the order is determined. When the 1st, 3rd, 5th, 7th, and 9th blood sampling combination was selected, the MRE and PRE were 4.4% and 23.3%, respectively. In order to increase the accuracy of plasma volume measurement, the first and the last samples of the 10 samples had to be included, which is in line with previous knowledge that the points at both ends are generally more influential than those in the middle in linear regression [14].
As of yet, there are no clear criteria as to how much difference is to be regarded as the same value when the plasma volume is measured by two different methods. In this study, based on general statistical concepts, the plasma values obtained by the two methods were considered equal when the relative error was less than 5%. When the 1st, 2nd, 3rd, 9th, and 10th blood sampling combination were selected, the mean relative error was 1.3%, which is smaller than the 2.5% accuracy when measuring blood volume with the albumin I-131 kit [15].
The Shiny web application was further developed for the convenience in measuring the plasma volume by the ICG dilution technique (https://ek-lee.shinyapps.io/ICGtechnique/, Inventors: Eun-Hwa Kang and Eun-Kyung Lee). The application was configured to choose between the original method and the modified method, and by entering the ICG dose and concentrations, the Cp0 and plasma volume results can be obtained. The blood collection time is already entered as a default value but can be modified.
There are some limitations to this study. First, the actual time of blood sampling did not exactly match the target time. Blood collection had to be carried out every 20 s from 2 to 5 min after ICG administration, which made it difficult to accurately keep the preset time. Nevertheless, there were no more than 10-s delays beyond the scheduled time, so the analysis was performed according to the order of blood sampling. Second, further validation is needed to determine if the results of this study may be applied in other populations including children. In general, a newly developed method needs to be validated in various populations, but the modified method has yet to be fully validated. Nevertheless, the current results may be considered as the most reliable data on this topic to date because the study included a large number of adults (N = 115) with various physical characteristics.
In conclusion, our newly proposed modified ICG dilution method achieved comparable results with the original method while using only 5 out of the 10 originally needed number of blood samples. Of the 10 blood samples, the order of the 5 selected samples was 1st, 2nd, 3rd, 9th, and 10th. We expect that this modified method may be able to aptly replace the original method and lead to a wider clinical application of the ICG dilution technique for plasma volume measurement.
References
Hopf HW, Morrissey C. Perioperative fluid management: turning art to science. Anesthesiology. 2019;130:677–9. https://doi.org/10.1097/ALN.0000000000002663.
Jacob M, Conzen P, Finsterer U, Krafft A, Becker BF, Rehm M. Technical and physiological background of plasma volume measurement with indocyanine green: a clarification of misunderstandings. J Appl Physiol. 2007;102:1235–42. https://doi.org/10.1152/japplphysiol.00740.2006.
Lee YH, Jang HW, Park CH, An SM, Lee EK, Choi BM, Noh GJ. Changes in plasma volume before and after major abdominal surgery following stroke volume variation-guided fluid therapy: a randomized controlled trial. Minerva Anestesiol. 2019. https://doi.org/10.23736/S0375-9393.19.13952-1.
Aguree S, Gernand AD. An efficient method for measuring plasma volume using indocyanine green dye. MethodsX. 2019;6:1072–83. https://doi.org/10.1016/j.mex.2019.05.003.
Hart D, Metz J. The estimation of red cell volume with 51Cr-labelled erythrocytes and plasma volume with radioiodinated human serum albumin. J Clin Pathol. 1962;15:459–61. https://doi.org/10.1136/jcp.15.5.459.
Gibson JG, Evans WA. Clinical studies of the blood volume. I. Clinical application of a method employing the azo dye "Evans Blue" and the spectrophotometer. J Clin Investig. 1937;16:301–16. https://doi.org/10.1172/JCI100859.
He YL, Tanigami H, Ueyama H, Mashimo T, Yoshiya I. Measurement of blood volume using indocyanine green measured with pulse-spectrophotometry: its reproducibility and reliability. Crit Care Med. 1998;26:1446–511. https://doi.org/10.1097/00003246-199808000-00036.
Kim GY, Bae KS, Noh GJ, Min WK. Estimation of indocyanine green elimination rate constant k and retention rate at 15 min using patient age, weight, bilirubin, and albumin. J Hepatobiliary Pancreat Surg. 2009;16:521–8. https://doi.org/10.1007/s00534-009-0097-3.
Vos JJ, Scheeren TW, Loer SA, Hoeft A, Wietasch JK. Do intravascular hypo- and hypervolaemia result in changes in central blood volumes? Br J Anaesth. 2016;116:46–53. https://doi.org/10.1093/bja/aev358.
Cottis R, Magee N, Higgins DJ. Haemodynamic monitoring with pulse-induced contour cardiac output (PiCCO) in critical care. Intensive Crit Care Nurs. 2003;19:301–7. https://doi.org/10.1016/s0964-3397(03)00063-6.
Galstyan G, Bychinin M, Alexanyan M, Gorodetsky V. Comparison of cardiac output and blood volumes in intrathoracic compartments measured by ultrasound dilution and transpulmonary thermodilution methods. Intensive Care Med. 2010;36:2140–4. https://doi.org/10.1007/s00134-010-2003-5.
Krivitski NM, Kislukhin VV, Thuramalla NV. Theory and in vitro validation of a new extracorporeal arteriovenous loop approach for hemodynamic assessment in pediatric and neonatal intensive care unit patients. Pediatr Crit Care Med. 2008;9:423–8. https://doi.org/10.1097/01.PCC.0b013e31816c71bc.
Sekimoto M, Fukui M, Fujita K. Plasma volume estimation using indocyanine green with biexponential regression analysis of the decay curves. Anaesthesia. 1997;52:1166–72. https://doi.org/10.1111/j.1365-2044.1997.249-az0389.x.
Nurunnabi AAM, Nasser M, Imon AHMR. Identification and classification of multiple outliers, high leverage points and influential observations in linear regression. J Appl Stat. 2016;43:509–25. https://doi.org/10.1080/02664763.2015.1070806.
Dworkin HJ, Premo M, Dees S. Comparison of red cell and whole blood volume as performed using both chromium-51-tagged red cells and iodine-125-tagged albumin and using I-131-tagged albumin and extrapolated red cell volume. Am J Med Sci. 2007;334:37–40. https://doi.org/10.1097/MAJ.0b013e3180986276.
Acknowledgements
We thank Dr Joon Seo Lim from the Scientific Publications Team at Asan Medical Center for his editorial assistance in preparing this manuscript.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kim, K.M., Park, DY., Kang, EH. et al. A modified method of measuring plasma volume with indocyanine green: reducing the frequency of blood sampling while maintaining accuracy. J Clin Monit Comput 35, 779–785 (2021). https://doi.org/10.1007/s10877-020-00536-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10877-020-00536-5