
Abstract
Laparoscopic surgery is often prolonged and requires positional changes to facilitate surgical access. Previous studies reported intraocular pressure (IOP) changes in one fixed position. This study investigated the effect of desflurane and propofol anesthesia on IOP during repeated positional changes. A total of 46 patients undergoing laparoscopic colorectal surgery were randomized into desflurane or propofol groups. IOP was measured using a handheld tonometer at seven time points: before induction (baseline), after endotracheal intubation, after pneumoperitoneum, after the first Trendelenburg and right tilt position, after reverse Trendelenburg and right tilt position, after the second Trendelenburg and right tilt position and before endotracheal extubation. Trendelenburg positioning raised IOP in both groups. In the desflurane group, IOP at the first Trendelenburg position was 6.27 and 8.48 mmHg higher than baseline IOP in left and right eye, respectively; IOP at the second Trendelenburg position was 7 and 9.44 mmHg higher than baseline in left and right eye, respectively. In the propofol group, IOP at the first Trendelenburg position was 2.04 and 4.04 mmHg higher than baseline in left and right eyes, respectively. It was 3.04 and 4.87 mmHg higher than baseline in left and right eye, respectively, at the second Trendelenburg position. In the desflurane group, 56.52% patients exhibited high IOP (≥ 25 mmHg) compared with 13.04% in the propofol group at the second Trendelenburg position in the right eyes (P = 0.005). There was a positive correlation between IOP and peak inspiratory pressure (P < 0.001). Propofol anesthesia mitigated wide variations in IOP caused by repetitive positional changes during laparoscopic colorectal surgery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
The proportion of elective colorectal or gynecological surgeries performed laparoscopically has increased considerably over the past decade and continues to rise. These surgeries require specific body positioning to use gravity to pull the abdominal viscera away from the operative field. Furthermore, some positions are used in association with pneumoperitoneum, which is usually nonphysiological and may lead to substantial negative effects such as increased intraocular pressure (IOP). Persistently increased IOP can cause retinal and optic nerve damage by decreasing perfusion and resulting in postoperative visual disturbance [1]. Transient elevation of IOP also can lead to glaucoma progression [2].
Laparoscopic colorectal surgery is associated with long durations of anesthesia, and marked positional changes that include steep Trendelenburg and reverse Trendelenburg positioning during pneumoperitoneum. Mizrahi et al. reported the development of bilateral ischemic optic neuropathy after proctocolectomy [3]. Although the steep Trendelenburg position with carbon dioxide (CO2) insufflation increases IOP [4], the magnitude of this increase is not well established as yet particularly during lengthy procedures requiring repeated positional changes in older populations.
Many trials have investigated the effects of different anesthetic agents on IOP. Although opioids have been known to have minimal effects, inhalation and intravenous anesthetics, with exception of ketamine, are known to cause a dose-related reduction in IOP by as much as 30–40% [5]. Propofol reduces IOP more than other intravenous anesthetics [6], and prevents the increase of IOP more effectively than isoflurane or sevoflurane in Trendelenburg position with peumoperitoneum [7, 8].Compared with desflurane, propofol demonstrated comparable effects on IOP in patients undergoing anesthesia in supine and reverse Trendelenburg positions; however, it was more effective in reducing IOP elevation in the Trendelenburg position [9, 10]. Nevertheless, comparative studies investigating the effect of propofol and desflurane on IOP during repetitive positional changes have not been performed. We hypothesized that repetitive positional changes would induce fluctuations of IOP and propofol might attenuate the increase of IOP more effectively than desflurane. Therefore, we aimed to evaluate IOP variation during repetitive changes in surgical positioning (Trendelenburg and reverse Trendelenburg) in the same patient, and to compare the effects of different anesthetics (desflurane vs. propofol) in attenuating IOP variations during laparoscopic colorectal surgery.
2 Materials and methods
2.1 Patients
The study protocol was approved by the Institutional Review Board of St. Vincent’s Hospital, Catholic University of Korea (Suwon, South Korea; IRB No: VC16OISI0143) and registered at Clinicaltrials.gov (NCT03016234). Informed written consent was obtained from all patients.
Fifty patients aged 40–80 years with an American Society of Anesthesiologists physical status I or II, who were diagnosed with colorectal cancer and scheduled for elective laparoscopic colorectal surgery between September 2016 and March 2017, were enrolled in this prospective, randomized and controlled study. For observation of IOP following applicable positional changes, only two types of laparoscopic colorectal surgery were examined: laparoscopic anterior resection (LAR) of the sigmoid colon; and laparoscopic low anterior resection (LLAR) of the rectum. The study excluded patients who underwent previous eye surgery, or had preexisting eye disease, uncontrolled hypertension, history of hypersensitivity to anesthetics, chronic obstructive lung disease, body mass index (BMI) > 30 kg/m2, or preoperative IOP > 21 mmHg.
2.2 Study protocol
Enrolled patients were randomly assigned to one of two groups using block randomization. On arrival to the operating room, routine monitoring, including electrocardiogram, noninvasive blood pressure, pulse oximetry, and bispectral index (BIS), was performed. All anesthetic management was performed and recorded by one experienced anesthesiologist who was not involved in the analysis of study data. The IOP was measured by another anesthesiologist who had experience in measuring IOP during the preliminary study and did not participate in the data analysis. We used a hand-held tonometer (Tono-Pen® AVIA, Reichert Technologies, Depew, NY, USA). In the desflurane group, anesthesia was induced using intravenous thiopental sodium 5–6 mg/kg and rocuronium 1 mg/kg. After endotracheal intubation, anesthesia was maintained with 5–8 vol% desflurane inhalation and continuous infusion of remifentanil. The desflurane concentration was titrated to maintain BIS values within a target range of 40–60 during the operation. Remifentanil was administered via a target-controlled infusion (TCI) system using a TCI device (Orchestra Base Primea®, Fresenius Kabi, Austria). The target effect site concentration of remifentanil was 3–6 ng/mL. In the propofol group, anesthesia was induced using intravenous 1% propofol 1.5–2.5 mg/kg and rocuronium 1 mg/kg. After endotracheal intubation, anesthesia was maintained using continuous infusion of 2% propofol and remifentanil (target effect site concentration 3–6 ng/mL). Propofol was administered via a TCI system using TCI device (target effect site concentration 2.5–5 µg/mL). The effect-site concentration of propofol was titrated to maintain BIS values within a target range 40–60 during surgery. Mechanical ventilation was maintained using 50% air and 50% oxygen; tidal volume was regulated to maintain an end tidal CO2 (ETCO2) 30–40 mmHg in all patients. Ringer’s lactate solution (3–5 mL/kg/h) and an equal volume of 6% hydroxyethyl starch for blood loss were infused to maintain a target central venous pressure of 10 mmHg, urine output > 0.5 mL/kg and a mean arterial pressure (MAP) between ± 20% of the baseline value.
2.3 Surgical technique
Pneumoperitoneum was created by intraperitoneal insufflation with CO2 with a flow rate of 20 L/min when the patients were supine. Intraperitoneal pressure was maintained at 10–12 mmHg in all patients. Patients were then placed in the steep Trendelenburg position (30°) with right side tilt (10°–15°). After dissecting the Toldt’s fascia to mobilize the sigmoid and descending colon and its mesocolon, patients were placed in the reverse Trendelenburg position (20°–25°) with right tilt to mobilize the distal segment of the transverse colon as well as the splenic flexure. Thereafter, the patient’s position was changed again to steep Trendelenburg with right tilt. For anterior or low anterior resection, the entire procedure, including inferior mesenteric artery ligation, complete left colon mobilization, and transection of colonic segment, was completed laparoscopically. All procedures were performed by two experienced surgeons.
2.4 Data collection
IOP was measured after applying two drops of 0.5% Alcaine (proparacaine HCl 5 mg, Alcon-Couvreur N.V., Puurs, Belgium) for topical anesthesia at seven defined time points as follows: before anesthetic induction (T1); immediately after endotracheal intubation (T2); immediately after creating pneumoperitoneum (T3); 30 min after the first Trendelenburg and right tilt position (T4); 10 min after reverse Trendelenburg and right tilt position (T5); 30 min after the second Trendelenburg and right tilt position (T6); 5 min before endotracheal extubation (T7).
The tonometer averages readings from six successful measurements and displays the mean value along with the statistical confidence indicator. If the statistical confidence indicator was less than 95%, the value was discarded and measurements were repeated. At the time of each IOP measurement, MAP, ETCO2 and peak inspiratory pressure (PIP) were recorded. After emergence from anesthesia, all patients were asked about ophthalmic complications, such as visual disturbance, in the recovery room.
2.5 Statistical analysis
The number of patients required in each group was determined after a power calculation based on data from a previous study [8], in which the mean IOP in the propofol-based anesthesia group after pneumoperitoneum and steep Trendelenburg positioning was 19.5 mmHg compared with 23 mmHg in the sevoflurane anesthesia group. To detect a mean (± SD) difference in IOP of 3.5 ± 4 mmHg, power estimation analysis suggested that 21 patients per group would be required to obtain a power of 80%, considering a type I error of 0.05. Recruitment was increased by 20% to compensate for unexpected losses.
Statistical analyses were performed using SPSS version 20.0 (SPSS Inc., Chicago, IL, USA) for Windows (Microsoft Corporation, Redmond, WA, USA). Demographic data were analyzed using the χ2 test and t-test. Repeated-measures ANOVA was performed to compare IOP, MAP, PIP, and ETCO2 between the two groups, with ‘group’ and ‘time point’ as independent variables, after confirming normal distribution using the Shapiro–Wilk test (P > 0.05). Differences between the two groups were then calculated using the t-test followed by Bonferroni’s post hoc test (adjusted P value for significance P < 0.007). The Student’s t-test was used to compare initial IOP and IOP at the remainder of the time points. The relationships between PIP and IOP, ETCO2 and IOP, and MAP and IOP were analyzed using Pearson’s correlation test. A P value < 0.05 was considered to be statistically significant.
3 Results
3.1 General information of the patients
Of the 50 patients enrolled in this study, three patients in whom the operation was altered to an open laparotomy and one who underwent unanticipated co-operation of gynecological surgery, were excluded. Therefore, a total of 46 patients completed this study: 23 in desflurane group and 23 in propofol group (Fig. 1).

Consort flow diagram to illustrate the study design. Asterisk represents the three patients were undergone open laparotomy due to changed operation plan and one patient was undergone co-operation of gynecologic surgery
Demographic data and perioperative outcomes were comparable between the two groups, except for operation type (Table 1). No patient complained of any visual disturbance after emerging from anesthesia. During anesthesia, no significant differences were found in MAP, PIP or ETCO2 between the two groups (Table 2).
3.2 Changes in IOP
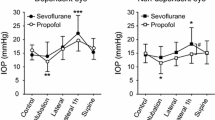
The trends in IOP variation according to positional changes were similar in both groups (Fig. 2; Table 3). IOP increased markedly after position change to the first steep Trendelenburg with right tilt position (T4), and decreased after position change to the reverse Trendelenburg with right tilt position (T5). After adopting the second steep Trendelenburg with right tilt position (T6), IOP increased by approximately 1 mmHg, compared with the IOP measured at the first steep Trendelenburg with right tilt position in both groups, although this difference was not significant. Comparing the two groups, there was no significant difference from the initial baseline IOP to immediately after creating pneumoperitoneum; however, IOP in the propofol group was significantly lower than that in the desflurane group at all times after the first Trendelenburg and right tilt position in both eyes (Fig. 2).

Comparison of intraocular pressure (IOP) between groups in left and right eyes. *Bonferroni correction for multiple comparisons, adjusted P value for significance P < 0.007. *P < 0.007 versus desflurane group, †P < 0.05 versus baseline value (T1) in both groups. T1 before anesthetic induction, T2 immediately after endotracheal intubation, T3 immediately after creating pneumoperitoneum, T4 30 min after the first Trendelenburg and right tilting position; T5 10 min after the reverse trendelenburg and right tilting position, T6 30 min after the second trendelenburg and right tilting position, T7 5 min before endotracheal extubation
In the comparison of baseline IOP and IOP at the remainder of the time points, IOP of both eyes in the desflurane and propofol groups was significantly higher at the first and second Trendelenburg with right tilt position (Fig. 2, P < 0.05). In the desflurane group, IOP at the first Trendelenburg position was 6.27 and 8.48 mmHg higher than baseline IOP in the left and right eye, respectively. Additionally, it was 7 and 9.44 mmHg higher than baseline IOP in left and right eye, respectively, at the second Trendelenburg position (Table 3). In the propofol group, IOP at the first Trendelenburg position was 2.04 and 4.04 mmHg higher than baseline IOP in left and right eyes, respectively. It was 3.04 and 4.87 mmHg higher than baseline IOP in left and right eye, respectively, at the second Trendelenburg position (Table 3).
The number of patients exhibiting high IOP (≥ 25 mmHg) in the right eye was significantly more in the desflurane group than in the propofol group at both Trendelenburg with right tilt positions (Table 3). In the desflurane group, more than half of patients exhibited high IOP in the right eye at the second Trendelenburg with right tilt position (56.52% in the desflurane group versus 13.04% in the propofol group; difference 43.48%; P = 0.005) (Table 3).
IOP in the right eye was approximately 2 mmHg higher than that in the left eye at the right tilt position (T4–T6) in both groups; however, this difference was not significant (Table 3).
3.3 Correlation of IOP with other variables
PIP was correlated positively with IOP during anesthesia (r = 0.589 and 0.560 for the desflurane and propofol groups, respectively; P < 0.001), as shown in Fig. 3. Neither MAP nor ETCO2 was correlated with IOP in each group (P = 0.301 for MAP and P = 0.253 for ETCO2).

Correlation between peak inspiratory pressure and intraocular pressure. r = 0.589 and 0.560 for desflurane and propofol group respectively. P < 0.001 in the both groups
4 Discussion
The aim of the present study was to evaluate IOP variation during repetitive positional changes in patients undergoing laparoscopic colorectal surgery and to compare the effect of desflurane and propofol anesthesia on IOP change. This study demonstrated that repetitive positional changes in anesthetized patients caused variations in IOP and that IOP increased markedly in the steep Trendelenburg position. We found that IOP values were significantly lower in patients undergoing propofol total intravenous anesthesia (TIVA) than in patients undergoing desflurane anesthesia during intraoperative positional changes. Propofol TIVA was more effective than desflurane-based inhalation anesthesia in attenuating IOP increases during frequent positional changes in long-duration laparoscopic surgeries.
Normal IOP is between 10 and 21 mmHg [5]. Perioperative increases in IOP can be caused by prone or head-down positioning, spine or cardiac surgery, and other long-duration laparocopic or robotic surgeries [3, 4, 11]. In addition to surgical factors, patients with glaucoma, open globe injury, uncontrolled hypertension, arthrosclerosis, and morbid obesity are at risk for potentially damaging IOP elevation [5]. High IOP can impair the blood supply, potentially leading to a loss of optic nerve function. Perioperative ocular hypertension results in serious complications such as glaucoma and postoperative visual loss [1]. Because the patients’ underlying disease or types of operation cannot be controlled, selection of anesthetic agents which can prevent IOP elevation is crucial in patients at risk of ocular hypertension during perioperative periods.
Although the prevalence of postoperative visual loss is not as high as in other nonophthalmic surgeries, such as cardiac or spine surgery, the rate of visual loss during colorectal resection was reported to be 1.24 per 10,000 [11]. Laparoscopic colorectal surgeries usually require positional changes, such as steep Trendelenburg, reverse Trendelenburg or prone position with one side tilted during the operation, and are usually lengthy in duration. Moreover, most individuals undergoing laparoscopic colorectal surgery are elderly and potentially vulnerable to ocular complications [12]. Most studies evaluating IOP variations were performed in one fixed position (i.e., Trendelenburg or reverse Trendelenburg), and were not designed to accurately determine IOP variations following repetitive positional changes. The strength of the present study is that IOP variation was assessed during repetitive positional changes in the same patients.
With respect to IOP differences between the two eyes, IOP of the dependent eye was approximately 2 mmHg higher, on average, than that of the contralateral eye in right tilt positions regardless of the anaesthetic agent. Under normal conditions, IOP values in both eyes typically demonstrate a symmetrical pattern; however, the lateral decubitus position has been reported to be associated with a significant increase in IOP (approximately 3–5 mmHg) in the dependent eye during anesthesia [13]. The present study results demonstrate that a one side tilt position (10°–15°) has only minimal effects on the dependent eye and the effects of propofol and desflurane on IOP are comparable during the 10°–15° one side tilt position.
IOP values in both Trendelenburg positions in the desflurane group were higher than those in the propofol group, and most were higher than the normal range. In contrast, most of the IOP values in the Trendelenburg position in the propofol group remained within the normal range. Results of this study are consistent with those of earlier investigations, which reported that propofol TIVA prevented IOP elevation during gynecological laparoscopy and is preferred if control of IOP is required [7, 10]. Yoo et al. also demonstrated that the increase of IOP in steep Trendelenburg position with pneumoperitoneum was lower under propofol anesthesia than sevoflurane anesthesia [8].
Two studies have compared propofol and desflurane in mitigating the effect on IOP [9, 10]. A study comparing the effect of propofol and desflurane on IOP under two different positions concluded that propofol mitigated IOP elevation under Trendelenburg position but had no different effect than desflurane on IOP under reverse Trendelenburg position [10]. Asuman et al. also suggested that desflurane anesthesia maintains IOP at levels similar to propofol TIVA anesthesia in patients undergoing laparoscopic cholecystectomy [9]. However, there has been no study comparing effect of propofol and desflurane on variations in IOP following repetitive position changes (i.e., Trendelenburg and reverse Trendelenburg) in the same patients. Although propofol did not prevent IOP elevation, the degree of IOP increase was less in the propofol group than that in desflurane group in both Trendelenburg position. It is remarkable that the IOP difference between baseline and the second Trendelenburg position in the desflurane group reached 9.43 mmHg and more than half of all patients exhibited high IOP (≥ 25 mmHg) in the dependent eye. On the other hand, patients who underwent propofol anesthesia exhibited a change in IOP between baseline and the second Trendelenburg position by as much as 4.87 mmHg, and only three patients exhibited elevated IOP (≥ 25 mmHg) in the dependent eye. Therefore, propofol TIVA maintained IOP without excessive elevation during prolonged procedures involving repetitive positional changes.
IOP is determined by multiple factors including intraocular fluid volume, choroidal blood volume, scleral rigidity, orbicularis oculi muscle tension, and external pressure [14]. The mechanism of the IOP-mitigating effect of propofol during anesthesia remains unclear, but may be attributable to the inhibition of arginine vasopressin (AVP) release from the supraoptic nucleus [15]. Plasma AVP concentration is increased markedly after insufflation of the pneumoperitoneum during laparoscopic surgery [16,17,18], and AVP can increase IOP in a dose-dependent manner [19, 20]. In addition, propofol mitigates IOP by decreasing the rate of aqueous humor formation to greater extent than it decreases trabecular outflow facility [21]. Consequently, propofol could prevent the increase in IOP during pneumoperitoneum and the Trendelenburg position.
Inhalation anesthetics, including desflurane, also reduce IOP dose-dependently by suppressing the diencephalon, decreasing the production of aqueous humor, increasing the outflow of aqueous humor, and/or relaxation of the extraocular muscles [22]. However, in other studies, inhalation anesthesia of 1–2 minimum alveolar concentration (MAC) for maintaining MAP between ± 20% of the baseline value resulted in IOP increases as much as 11–13 mmHg after steep Trendelenburg positioning with pneumoperitoneum compared with baseline IOP [4, 23]. In the present study, we performed desflurane anesthesia with 1–1.5 MAC and obtained similar results. Although it is not yet clear whether higher concentrations of inhalation can be as effective as propofol, we may deduce that propofol is more effective in preventing IOP elevation than 1–1.5 MAC desflurane.
Aside from surgical positioning, PIP was the only other factor demonstrating significant correlation with IOP during surgery in the present study. An attributable mechanism for a relationship between PIP and IOP is that an increase in intrathoracic pressure may cause increases in central venous pressure, which in turn decreases the outflow of aqueous humor through the episcleral venous system. Although a previous study reported that positive end-expiratory pressure does not pose a significant risk for IOP increase [24], most other studies [4, 23] have reported results similar to ours. In the present study, IOP demonstrated a significant correlation with PIP during anesthesia; however, our r values were lower than those reported in other studies (0.7–0.8) [4, 23]. This may be because these studies primarily investigated one fixed position during surgery, whereas the present study examined positional variation. Further studies would be needed to clarify whether the correlation between PIP and IOP is impacted by different positions.
This study has a few limitations. First, the proportion of operation types in the two groups was significantly different. Although the number of patients undergoing laparoscopic anterior resection was more than those undergoing laparoscopic low anterior resection in the propofol group, the duration and nature of positional changes in the two types of surgery were similar. Second, we did not measure IOP after endotracheal extubation. Grosso et al. reported that elevated IOP during the Trendelenburg position recovered to baseline level 48 h after the conclusion of anesthesia [25]. Therefore, we can infer that IOP after anesthesia may be similar to baseline value because IOP before extubation was presumably lower than baseline. Third, we did not follow-up IOP on long-term outcomes. Although fluctuation of IOP can be risk factor for glaucoma progression [26], the impact of perioperative fluctuation of IOP on the development or progression of glaucoma remains unknown. If we performed ophthalmological examinations postoperatively, we may have found objective evidence for increased incidence or severity of ophthalmological complications due to perioperative fluctuations in IOP.
5 Conclusion
Propofol TIVA can more effectively mitigate wide variations in IOP caused by repetitive positional changes during laparoscopic surgery compared with desflurane anesthesia. This suggests that propofol TIVA may be a better choice for the maintenance of IOP during laparoscopic colorectal surgeries that involve frequent positional changes.
References
Cheng MA, Sigurdson W, Tempelhoff R, Lauryssen C. Visual loss after spine surgery: a survey. Neurosurgery. 2000;46:625–31.
Law SK, Nguyen AM, Coleman AL, Caprioli J. Severe loss of central vision in patients with advanced glaucoma undergoing trabeculectomy. Arch Ophthalmol. 2007;125:1044–50.
Mizrahi H, Hugkulstone CE, Vyakarnam P, Parker MC. Bilateral ischaemic optic neuropathy following laparoscopic proctocolectomy: a case report. Ann R Coll Surg Engl. 2011;93:e53–54.
Awad H, Santilli S, Ohr M, Roth A, Yan W, Fernandez S, Roth S, Patel V. The effects of steep trendelenburg positioning on intraocular pressure during robotic radical prostatectomy. Anesth Analg. 2009;109:473–8.
Feldman MA. Anesthesia for eye surgery. Miller’s anesthesia. 8th ed. Elsevier, Philadelphia; 2015. pp. 2512–42.
Alipour M, Derakhshan A, Pourmazar R, Abrishami M, Ghanbarabadi VG. Effects of propofol, etomidate, and thiopental on intraocular pressure and hemodynamic responses in phacoemulsification by insertion of laryngeal mask airway. J Ocul Pharmacol Ther. 2014;30:665–9.
Mowafi HA, Al-Ghamdi A, Rushood A. Intraocular pressure changes during laparoscopy in patients anesthetized with propofol total intravenous anesthesia versus isoflurane inhaled anesthesia. Anesth Analg. 2003;97:471–4.
Yoo YC, Shin S, Choi EK, Kim CY, Choi YD, Bai SJ. Increase in intraocular pressure is less with propofol than with sevoflurane during laparoscopic surgery in the steep Trendelenburg position. Can J Anaesth. 2014;61:322–9.
Asuman AO, Baris A, Bilge K, Bozkurt S, Nurullah B, Meliha K, Umit C. Changes in intraocular pressures during laparoscopy: a comparison of propofol total intravenous anesthesia to desflurane-thiopental anesthesia. Middle East J Anaesthesiol. 2013;22:47–52.
Hwang JW, Oh AY, Hwang DW, Jeon YT, Kim YB, Park SH. Does intraocular pressure increase during laparoscopic surgeries? It depends on anesthetic drugs and the surgical position. Surg Laparosc Endosc Percutaneous Tech. 2013;23:229–32.
Shen Y, Drum M, Roth S. The prevalence of perioperative visual loss in the United States: a 10-year study from 1996 to 2005 of spinal, orthopedic, cardiac, and general surgery. Anesth Analg. 2009;109:1534–45.
He Z, Vingrys AJ, Armitage JA, Bui BV. The role of blood pressure in glaucoma. Clin Exp Optom. 2011;94:133–49.
Yamada MH, Takazawa T, Iriuchijima N, Horiuchi T, Saito S. Changes in intraocular pressure during surgery in the lateral decubitus position under sevoflurane and propofol anesthesia. J Clin Monit Comput. 2016;30:869–74.
Cunningham AJ, Barry P. Intraocular pressure physiology and implications for anaesthetic management. Can Anaesth Soc J. 1986;33:195–220.
Inoue Y, Shibuya I, Kabashima N, Noguchi J, Harayama N, Ueta Y, Sata T, Shigematsu A, Yamashita H. The mechanism of inhibitory actions of propofol on rat supraoptic neurons. Anesthesiology. 1999;91:167–78.
Stone J, Dyke L, Fritz P, Reigle M, Verrill H, Bhakta K, Boike G, Graham J, Gerbasi F. Hemodynamic and hormonal changes during pneumoperitoneum and trendelenburg positioning for operative gynecologic laparoscopy surgery. Prim Care Update Ob Gyns. 1998;5:155.
Joris JL, Chiche JD, Canivet JL, Jacquet NJ, Legros JJ, Lamy ML. Hemodynamic changes induced by laparoscopy and their endocrine correlates: effects of clonidine. J Am Coll Cardiol. 1998;32:1389–96.
Berg K, Wilhelm W, Grundmann U, Ladenburger A, Feifel G, Mertzlufft F. Laparoscopic cholecystectomy–effect of position changes and CO2 pneumoperitoneum on hemodynamic, respiratory and endocrinologic parameters. Zentralbl Chir. 1997;122:395–404.
Wallace I, Moolchandani J, Krupin T, Wulc A, Stone RA. Effects of systemic desmopressin on aqueous humor dynamics in rabbits. Investig Ophthalmol Vis Sci. 1988;29:406–10.
Krupin T, Webb GW, Barbosa AT, Gulli B, Levine J, Becker B. Central effects of thyrotropin-releasing hormone and arginine vasopressin on intraocular pressure in rabbits. Investig Ophthalmol Vis Sci. 1984;25:932–7.
Artru AA. Trabecular outflow facility and formation rate of aqueous humor during propofol, nitrous oxide, and halothane anesthesia in rabbits. Anesth Analg. 1993;77:564–9.
Park JT, Lim HK, Jang KY, Um DJ. The effects of desflurane and sevoflurane on the intraocular pressure associated with endotracheal intubation in pediatric ophthalmic surgery. Korean J anesthesiol. 2013;64:117–21.
Joo J, Koh H, Lee K, Lee J. Effects of systemic administration of dexmedetomidine on intraocular pressure and ocular perfusion pressure during laparoscopic surgery in a steep trendelenburg position: prospective, randomized, double-blinded study. J Korean Med Sci. 2016;31:989–96.
Teba L, Viti A, Banks DE, Fons A, Barbera M, Hshieh PB. Intraocular pressure during mechanical ventilation with different levels of positive end-expiratory pressure. Crit Care Med. 1993;21:867–70.
Grosso A, Scozzari G, Bert F, Mabilia MA, Siliquini R, Morino M. Intraocular pressure variation during colorectal laparoscopic surgery: standard pneumoperitoneum leads to reversible elevation in intraocular pressure. Surg Endosc. 2013;27:3370–6.
Sultan MB, Mansberger SL, Lee PP. Understanding the importance of IOP variables in glaucoma: a systematic review. Surv Ophthalmol. 2009;54:643–62.
Funding
This research was supported by a Grant from Saint Vincent’s Hospital, Research Institute of Medical Science Foundation (SVHR-2016-05).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest to declare.
Rights and permissions
About this article

Cite this article
Seo, K.H., Kim, YS., Joo, J. et al. Variation in intraocular pressure caused by repetitive positional changes during laparoscopic colorectal surgery: a prospective, randomized, controlled study comparing propofol and desflurane anesthesia. J Clin Monit Comput 32, 1101–1109 (2018). https://doi.org/10.1007/s10877-018-0116-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10877-018-0116-5