
Abstract
Weight discrimination has adverse effects on health that include increasing the risk factors for developing type 2 diabetes. Preliminary evidence suggests a positive association between weight discrimination and diagnosed diabetes; however, it is unknown whether psychosocial resources may buffer this association. In logistic regressions stratified by gender, we examined links between weight discrimination and diabetes among a nationally representative sample of U.S. adults (the National Social Life, Health, and Aging Project; N = 2,794 adults age 50 and older in 2015-16). We also tested the extent to which trait-resilience and social support from a spouse/partner, family, and friends buffered any observed association. We adjusted for known predictors of diabetes (age, race/ethnicity, Body Mass Index) and conducted sensitivity analyses restricted to men and women with obesity. Net of covariates, in the overall sample, weight discrimination was associated with significantly greater odds of having ever had diabetes among women (OR = 2.00, 95% CI [1.15, 3.47]), but not men. Among women with obesity, weight discrimination was only significantly associated with greater odds of diabetes for those with low resilience (OR = 1.84, 95% CI [1.01, 3.35]). Among men overall, weight discrimination was associated with lower odds of diabetes for those with high family support (OR = 0.03, 95% CI [0.003, 0.25]) as well as those with high friend support (OR = 0.34, 95% CI [0.13, 0.91]); similar effects were observed in men with obesity. These novel findings evince a role for psychosocial resources in buffering associations between weight discrimination and diabetes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The experience of weight discrimination can initiate a cascade of effects that have adverse implications for well-being, physiology, behavior, and physical health (Tomiyama, 2014). Weight discrimination is a stressor, and social-evaluative stressors reliably elicit physiological responses such as cortisol release (Dickerson & Kemeny, 2004). Indeed, weight stigma elicits a psychophysiological stress response (e.g., increased stress-related emotions and blood pressure; Major et al., 2012) and ironically may also spur increased calorie consumption (Major et al., 2014). Furthermore, both elevated cortisol (van der Valk et al., 2021) and increased caloric intake (Katan & Ludwig, 2010) can predict weight gain (Björntorp, 1990), which may exacerbate the experience of weight stigma, further perpetuating this cycle (Tomiyama, 2014). Prior research (Hunger & Tomiyama, 2014; Sutin & Terracciano, 2013) has found prospective associations between weight stigma or discrimination and risk of obesity. Weight discrimination may ultimately lead to a 60% increased risk of mortality after accounting for Body Mass Index (BMI; Sutin et al., 2015).
Notably, many of the harmful effects of weight discrimination (i.e., stress, elevated blood pressure, cortisol dysregulation, dimensions of unhealthy diet, and weight gain) are risk factors for type 2 diabetes (Bellou et al., 2018; Hackett & Steptoe, 2017; Mayo Clinic, 2021; Santos-Lozano et al., 2016). Given this, we investigate: could weight discrimination also place individuals at greater odds of developing type 2 diabetes?
A growing literature has demonstrated linkages between weight discrimination and biomarkers relevant to diabetes etiology. For instance, weight discrimination exacerbates the effects of waist-to-hip ratio on HbA1c among nondiabetic adults (Tsenkova et al., 2011). Another study (Sutin et al., 2014) among adults with overweight and obesity (BMI of ~ 25–40) found that weight discrimination was linked with higher circulating C-reactive protein—an inflammatory marker predictive of type 2 diabetes (Pradhan et al., 2001).
Moving beyond biomarkers to disease outcomes, one study among U.S. older adults found that weight discrimination was associated with greater disease burden (a summary measure of six physical health conditions, including diabetes) both cross-sectionally and 4 years later (Sutin, Stephan, Carretta et al., 2015). However, the contribution of weight discrimination to diabetes in isolation was not examined in this investigation. Several studies have focused more closely on outcomes of diagnosed diabetes. A recent study revealed that pregnancy-related weight stigma may increase odds of gestational diabetes—and that the association was greater than between BMI and gestational diabetes (Nagpal et al., 2021). In addition, a study conducted in 2004-5 among U.S. adults age 18 and older with overweight or obesity (Udo et al., 2016) found that after controlling for BMI, weight discrimination showed a cross-sectional association with diabetes among women, but not men.
In the present study, we build upon this prior research by examining the association between weight discrimination and diabetes in a nationally representative sample of U.S. older adults. Research focusing on this age group is especially warranted, as type 2 diabetes most often develops in people age 45 and older (Mayo Clinic, 2021). Understanding the etiology of type 2 diabetes remains a critical priority, as diabetes is the eighth leading cause of death in the U.S. and affects about 37 million U.S. adults (Centers for Disease Control and Prevention, 2023). This investigation also expands upon extant research (Udo et al., 2016) by including in our analysis individuals with BMIs consistent with underweight or normal weight (i.e., < 25), given that they are not immune to experiencing weight discrimination (e.g., Dutton et al., 2014) and some may nevertheless perceive themselves as overweight—a factor found to be important in predicting responses to weight stigma (Major et al., 2014). We also conduct sensitivity analyses restricted to individuals with obesity to assess whether any relationship between weight discrimination and diabetes is amplified in this sub-group.
The present research also makes a novel contribution to the literature by examining the extent to which psychosocial factors may play a protective role in buffering any association between weight discrimination and diabetes status. Accumulating research has begun to explore moderation of links between weight discrimination and mental health by psychosocial resources (Emmer et al., 2020), but potential moderation of physical health outcomes remains comparatively underexplored in the literature—or entirely absent in the case of diabetes.
We hypothesized that social support may buffer the association between weight discrimination and diabetes. Specifically, emotional support entailing empathy, comfort, or compassion (Emmer et al., 2020) may plausibly mitigate the stress elicited by weight discrimination. Preliminary qualitative evidence lends support for this notion; in a recent study among U.S. adults with obesity, those interviewed identified support seeking as one of the most effective methods for coping with weight discrimination (Gerend et al., 2021).
Another factor that could buffer associations between weight discrimination and diabetes is resilience, defined as the capacity to withstand, recover from, and even thrive despite adversity (Hawkley et al., 2021). Individuals with greater resilience may perceive less threat from stressors because they feel better prepared to cope with them (Watson et al., 2018). Here, we focus on trait-resilience, or individual attributes that constitute a resilient personality. Prior research has identified attributes such as self-efficacy, optimism, problem solving skills, and mastery as character strengths of resilient individuals that facilitate their adaptive response to adverse circumstances (Wagnild & Young, 1993). Among older adults, higher trait-like resilience is related to better health across several domains, including better self-rated physical health (Hawkley et al., 2021).
The present investigation uses nationally representative data among U.S. older adults from the National Social Life, Health and Aging Project (NSHAP) to test the following pre-registered hypotheses:
Hypothesis 1
• Those who have (vs. have not) experienced weight discrimination will show greater odds of ever having diabetes, independent of any effect of BMI.
Hypothesis 2
• Those with: (a) greater (vs. lower) social support from a spouse/partner, from family, and from friends; and (b) greater (vs. lower) trait resilience will show an attenuated association between self-reported weight discrimination and ever having diabetes, independent of any effect of BMI.
Method
Study design
The National Social Life, Health, and Aging Project (NSHAP) is a longitudinal study of older adults that conducts regular interviews (“Rounds” of data collection) every 5 years. Data collection began in 2005-06 with in-home interviews of a nationally representative sample of 3005 community-dwelling adults age 57–85. Surviving respondents and their spouses/co-residing romantic partners were also interviewed in 2010-11 and 2015-16. A second cohort was added in 2015-16 (age 50–67), which also included partners and age-eligible household members. Additional methodological information has been reported elsewhere (O’Muircheartaigh et al., 2014; O’Muircheartaigh et al., 2009). Here, we use data for respondents who were age 50 and older at the time of their 2015-16 interview.
Measures
Demographics. Respondents self-reported their gender, date of birth (used to compute age), and race/ethnicity at their first NSHAP interview. In 2015-16, respondents reported their current marital status, which we coded to indicate having a partner (married or living with a partner) versus not (separated, divorced, widowed, or never married).
Ever had diabetes. Any respondents who exhibited one or more of the following three indicators of diabetes were coded as “yes” for having ever had diabetes by 2015-16: (1) In their first year of participation, respondents were asked, “Have you ever had diabetes?” In all future interviews, respondents were asked, “Since your last interview in [month/year], has a doctor told you that you have diabetes or high blood sugar?”; (2) Hba1c was measured via blood samples in 2005-06 and 2010-11;Footnote 1 values of 6.5% or higher were considered indicative of having diabetes; and; (3) Respondents were asked if they were taking any anti-diabetic agent medications in every Round of data collection; an affirmative response was considered indicative of having diabetes.Footnote 2
Notably, respondents who reported a diabetes diagnosis were not asked whether they were diagnosed with type 1 or type 2 diabetes; however, they were asked the age at which they first received the diagnosis. Using these responses, we coded individuals who reported a first diabetes diagnosis of under the age of 40 as “0” (not having diabetes), as our interest in the present investigation is in the specific outcome of type 2 diabetes. Type 1 diabetes often first appears at two noticeable peaks in childhood and adolescence (Mayo Clinic, 2022), whereas type 2 diabetes often develops in people age 45 and older (Mayo Clinic, 2021). In our sample, about 6% of those with a diabetes diagnosis received the diagnosis before age 40; this proportion is consistent with evidence that type 1 diabetes constitutes about 5–10% of all cases of diabetes (Mobasseri et al., 2020).
Weight discrimination. In 2015-16, respondents were asked two questions from the Everyday Discrimination Scale (Williams et al., 1997). The questions asked how often in their day-to-day lives they have been treated with less courtesy than other people and how often people acted as if they were better than them [the respondent] (never to several times a week). Respondents were then asked, “When these things happen in your day-to-day life, what do you think is the main reason(s) for them? Please check all that apply” with options that included “height or weight” (our measure of weight discrimination), among other reasons for discrimination.
Following the approach of a prior investigation (Puhl et al., 2008) that also asked respondents about perceived discrimination based on weight or height, we determined the extent to which self-reported weight/height discrimination may have been primarily driven by weight or height. This entailed comparing average body weight, height, and BMI between participants reporting weight discrimination and the rest of the sample to test if weight was more likely than height to be a source of discrimination. We also examined whether rates of weight discrimination changed in any meaningful way if people with extreme height were excluded (bottom 1% or top 1% height).
On average, mean body weight was higher among those who reported weight/height discrimination, compared to those who did not (217.25 lb. vs. 166.51 lb., p < 0.001 for women; 224.06 vs. 202.20 lb., p = 0.001 for men). Similarly, mean BMI was higher among those who reported weight/height discrimination, compared to those who did not (38.33 vs. 28.87, p < 0.001 for women; 32.93 vs. 29.57, p < 0.001 for men). In contrast, mean height did not differ between those who did and did not report weight/height discrimination (63.27 vs. 63.74 inches, p = 0.16 for women; 68.78 vs. 69.44 inches, p = 0.25 for men); thus, body height alone is not sufficient to account for reported weight/height discrimination. Furthermore, rates of weight/height discrimination were unchanged regardless of whether respondents with extreme height (i.e., bottom 1% or top 1% height) were excluded. Taken together, these analyses suggest that self-reported weight/height discrimination is primarily related to body weight and obesity, rather than height. Given this, we hereafter refer to these reports as weight discrimination.
Body Mass Index (BMI). Respondent weight and height were measured in-person at the home of the respondent by the field interviewer. We utilized the 2015-16 measurement of weight for all respondents. We utilized height data from each respondent’s first interview (2005-6 for Cohort 1; 2015-16 for Cohort 2). For Cohort 1 respondents without a 2005-6 height measurement, height measurements from 2010 to 11 were utilized if available.
We used the standard formula [(weight in pounds/height in inches)2 × 703)] to calculate BMI. Following prior research (Cheng et al., 2016), respondents with biologically implausible height (< 44 inches or > 90 inches; n = 8), weight (< 55 lb. or > 1000 lb., n = 0), or BMI values (< 12 or > 70; n = 4) were excluded; these criteria applied to a combined total of 9 respondents.
Social support. Respondents were asked in 2015-16, “How often can you open up to your partner if you need to talk about your worries?” and “How often can you rely on your partner for help if you have a problem?” (never, hardly ever or rarely, some of the time, or often). Parallel items asked about these dimensions of social support, but for members of their family (excluding their spouse or romantic partner) and their friends (excluding family members or relatives from the prior items).
Resilience. Resilience was measured in 2015-16 by a validated 4-item measure introduced in Round 3 of NSHAP (Hawkley et al., 2021). Respondents were asked to rate how frequently four different statements were true of them: “I bounce back quickly after hard times,” “I take things in stride,” “I am an energetic person,” and “I can do just about anything I really set my mind to.” Response options included: never, some of the time, usually, and always. Responses were summed to compute total resilience scores (range: 0–12), with higher scores representing greater resilience. This resilience scale has demonstrated good reliability, convergent validity, and predictive utility (Hawkley et al., 2021).
Analytic plan
Given that men and women typically have different distributions of BMI (Yi et al., 2015) and preliminary evidence that associations between weight discrimination and diabetes differ by gender (Udo et al., 2016), we stratified all analyses by gender.
To test our first hypothesis, we used logistic regression to simultaneously model the odds of having ever had diabetes on self-reported weight discrimination, BMI, and covariates that include known risk factors for diabetes that are not suspected to be on the causal pathway from weight discrimination to having diabetes (i.e., age, race/ethnicity).
Next, we expanded the logistic regression models above by adding the main effects of the psychosocial factors (i.e., social support and resilience). Models examining main effects and/or interactions with partner support were conducted only among respondents with a spouse/partner. To test for moderation by the psychosocial factors, we tested each potential moderator in a separate model by examining the interaction term for the moderator of interest (continuous) with weight discrimination. Any significant interaction terms were followed with an examination of simple effects of weight discrimination at high and low levels of the moderator.
To follow up on any significant interactions involving the continuous social support measures, we created categorical support variables for each support source by following prior research (Hsieh & Hawkley, 2018).Footnote 3 Within each relationship domain of support, those who said “often” for both of the items (how often do you: a) open up to and b) rely on [spouse/partner, family, friends]) were coded as having high social support. Those who reported a lower frequency (i.e., never, hardly ever or rarely, some of the time) for one or both items were coded as having low social support. To follow up on any significant interactions involving the continuous resilience measure, we created a categorical indicator of high versus low resilience, defined via a median split (mdn = 8 for both men and women). Median split was used because there are no pre-established “high” and “low” levels of resilience for this measure to adopt from prior literature.
Finally, in sensitivity analyses, we repeated all primary analyses noted above, restricting the sample to only those with a BMI consistent with obesity (≥ 30).
Statistical analyses were conducted using Stata/SE 16.1 (StataCorp LLC, College Station, TX). All analyses were weighted by the reciprocal of the probability of selection and adjusted for non-response based on age and urbanicity, permitting the estimation of parameters for the U.S. population of older community-dwelling adults. Significance was set at p < 0.05.
Data and study materials
The analytic code is available upon request. The datasets analyzed are available at:
https://www.icpsr.umich.edu/web/NACDA/studies/20541 (Round 1);
https://www.icpsr.umich.edu/web/NACDA/studies/34921 (Round 2); and
https://www.icpsr.umich.edu/web/NACDA/studies/36873 (Round 3).
The study measures are available at:
https://www.icpsr.umich.edu/web/NACDA/studies/20541 (Round 1);
https://www.icpsr.umich.edu/web/NACDA/studies/34921 (Round 2); and
https://www.icpsr.umich.edu/web/NACDA/studies/36873 (Round 3).
Results
Descriptive results
Table 1 presents demographic and psychosocial characteristics of the analytic sample (N = 2,794), which includes those who were age-eligible; had plausible data for weight, height, and BMI; and who did not have missing data for any of the key variables or covariates for Hypothesis 1. Majorities of the sample were non-Hispanic White, married or living with a partner, had at least some college education, and had a BMI consistent with overweight or obesity. Approximately one-fifth of men and women had ever had diabetes.
Over and above the effects of age, race/ethnicity, marital status, and educational attainment, women were more likely than men to report experiencing weight discrimination (OR = 1.43, 95% CI [1.04, 1.98], p = 0.029); when also adding BMI as a covariate, the effect of gender remained similar (OR = 1.39, 95% CI [1.03, 1.88], p = 0.032).
Table 2 presents logistic regressions of odds of reporting weight discrimination as a function of demographic characteristics, stratified by gender. Among both men and women, lower age and greater BMI were associated with greater odds of reporting weight discrimination, whereas marital/partner status and educational attainment showed no statistically significant associations. Among women, non-Hispanic White respondents were more likely to report weight discrimination than non-Hispanic Black or Hispanic respondents.
Weight discrimination and ever had diabetes
Overall sample. In Table 3 (women) and 4 (men), Model 1 presents a logistic regression of odds of ever having diabetes on weight discrimination, adjusting for covariates. Net of BMI and other covariates, weight discrimination was associated with significantly greater odds of having ever had diabetes among women, but not men.
Sensitivity analyses. Analyses restricted to respondents with obesity showed a similar pattern of results to that of the overall sample. Weight discrimination was associated with significantly greater odds of having ever had diabetes among women with obesity (OR = 2.04, 95% CI [1.14, 3.63], p = 0.016), whereas the two were not significantly related among men with obesity (p = 0.992).
Main effects of social support and trait resilience
Overall sample. Model 2 in Table 3 (women) and 4 (men) adds mains effects for each psychosocial factor among those with a spouse/partner. Among partnered men, greater social support from friends was associated with significantly lower odds of having ever had diabetes. No other significant main effects of psychosocial factors were observed among women or men with a spouse/partner. Similarly, in ancillary analyses, no significant main effects emerged among unpartnered women (ps > 0.144) or men (ps > 0.156).
Sensitivity analyses. No statistically significant main effects of psychosocial factors were observed among women with obesity (ps > 0.229 and ps > 0.055 for those with and without a spouse/partner, respectively) or men with obesity (ps > 0.354 and ps > 0.058 for those with and without a spouse/partner, respectively).
Moderation by social support and trait resilience
Overall sample. Models 3–5 in Table 3 (women) and 4 (men) each add a psychosocial factor’s main effect and its interaction with weight discrimination.
None of the interaction terms in Table 3 were statistically significant, suggesting that among women overall, the association between weight discrimination and odds of ever having diabetes is not moderated by trait resilience, partner support, family support, or friend support.
Among men (Table 4), the interaction terms for family and friend support were statistically significant. Among men with high family support, experiencing weight discrimination was associated with lower odds of having ever had diabetes (OR = 0.03, 95% CI [0.003, 0.25], p = 0.002), whereas there was no significant association between the two among men with low family support (OR = 1.49, 95% CI [0.71, 3.12], p = 0.290). Similarly, weight discrimination was associated with lower odds of having ever had diabetes among men with high friend support (OR = 0.34, 95% CI [0.13, 0.91], p = 0.032), whereas there was no significant association among men with low friend support (OR = 1.39, 95% CI [0.52, 3.71], p = 0.505).
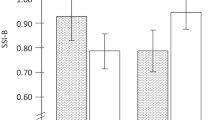
Sensitivity analyses. Analyses among women with obesity revealed one significant interaction for resilience with weight discrimination (OR = 0.72, 95% CI [0.54, 0.97], p = 0.031), such that weight discrimination only showed a statistically significant association with having ever had diabetes for those with low resilience (OR = 1.84, 95% CI [1.01, 3.35], p = 0.045; OR = 1.64, 95% CI [0.61, 4.44], p = 0.323 for those with high resilience).
Analyses among men with obesity revealed statistically significant interactions of family and friend support with weight discrimination (OR = 0.42, 95% CI [0.25, 0.72], p = 0.002; and OR = 0.63, 95% CI [0.44, 0.89], p = 0.010, respectively). Weight discrimination was associated with lower odds of diabetes among men with high family support (OR = 0.04, 95% CI [0.004, 0.46], p = 0.010), whereas no significant association was found among those with low family support (OR = 1.75, 95% CI [0.64, 4.83], p = 0.275). Weight discrimination was not significantly associated with odds of having ever had diabetes for those with high (OR = 0.35, 95% CI [0.11, 1.09], p = 0.070), or low friend support (OR = 1.74, 95% CI [0.52, 5.84], p = 0.369).
No other statistically significant interactions of psychosocial factors with weight discrimination were observed among women or men with obesity.
Discussion
In the present investigation in a nationally representative sample of older adult men and women, we examined the extent to which self-reported weight discrimination was associated with greater odds of having ever had diabetes, over and above any effects of BMI, age, and race/ethnicity. Results indeed revealed that women who had (vs. had not) experienced weight discrimination were twice as likely to have ever had diabetes; a similar association was found when this analysis was restricted to only women with obesity [OR = 2.00 vs. 2.04, respectively). Weight discrimination was not statistically significantly related to odds of ever having diabetes among men. These results mirror those of a cross-sectional study among U.S. adults age 18 and older with overweight or obesity (Udo et al., 2016), wherein after controlling for BMI, weight discrimination was significantly associated with diabetes among women, but not men.
This pattern of results may be explained in part by evidence that in American society, women can face greater criticism for their weight and appearance than men (Roehling, 2012). However, the literature is mixed with regard to whether men are more likely than women to experience weight discrimination (Emmer et al., 2020). Gender differences in weight discrimination prevalence may vary with age in the U.S., with women more likely than men to report weight discrimination at ages 35–54 and no significant gender difference at ages 55–74 (Puhl et al., 2008). Although older adult men in the present study reported lower rates of weight discrimination than women, this alone does not necessarily imply that men are less impacted by experiences with weight discrimination than women (Himmelstein et al., 2019).
The second objective of the present research was to test the extent to which any associations between weight discrimination and having ever had diabetes might be attenuated among older adults with higher (vs. lower) trait resilience and social support from a partner, family, and friends. This hypothesis was not supported among women overall; however, some evidence of moderation was found among women with obesity, such that weight discrimination was associated with greater odds of having ever had diabetes for those with low trait resilience, whereas no significant association was observed for those with high resilience.
These findings of moderation by resilience among women with obesity show a similar pattern to other studies of discrimination and health. For instance, one study found a significant positive association between sexist discrimination and psychological distress among bisexual women with low (but not high) resilience (Watson et al., 2018). Findings from another study among transgender individuals revealed that the relationship between anti-transgender discrimination and anxiety through alienation was conditional on low and moderate levels of resilience (Scandurra et al., 2018). This accumulating pattern of results suggests that low levels of resilience may be a risk factor in the context of discrimination, spanning diverse domains of discrimination, sub-populations, and health outcomes.
In the present study, links between weight discrimination and diabetes also differed as a function of family and friend social support among men. In both men overall and among men with obesity, weight discrimination was associated with lower odds of having ever had diabetes among those with high family support; in contrast, weight discrimination was not significantly associated with odds of having ever had diabetes among those with low family support. Similarly, among men overall, weight discrimination was associated with lower odds of diabetes among those with high friend support, whereas no significant association was found among those with low friend support. That is, a high level of family and/or friend support was protective, but a low level was not a risk factor. No other statistically significant moderation was found among for the psychosocial factors of trait resilience and social support from a spouse/partner.
Although the cross-sectional nature of the data precludes causal inferences of causality, one possibility is that high levels of support from friends and/or family may protect older adult men from adverse effects of weight discrimination that culminate in the form of greater odds of diabetes.
In addition and/or alternatively, men with diabetes and high (vs. low) family/and or friend social support could be less likely to experience weight discrimination for several reasons. First, although respondents were not asked who subjected them to weight discrimination, prior research (Himmelstein et al., 2019) has found that among adult men, the most common source is peers, followed by family members. Thus, men with high (vs. low) social support from friends and/or family may plausibly experience less frequent weight discrimination from these top sources. Second, men with diabetes and high (versus low) family/and or friend social support could be less likely to experience weight discrimination if their family/friends are aware they have diabetes. Weight bias can be shaped by beliefs that individuals are in control of and/or personally responsible for their own body weight, thereby eliciting blame and fostering stigmatizing beliefs and stereotypes (Talumaa et al., 2022). Indeed, beliefs that obesity is caused by behavior, a lack of willpower, or personal responsibility predict stronger weight bias, whereas beliefs in physiological causes are associated with lower levels of weight bias (Puhl et al., 2015). However, there is also evidence that U.S. adults with type 2 diabetes report higher rates of weight stigma than the general population (Himmelstein & Puhl, 2020). Future research is needed to identify factors that increase or decrease the odds that individuals with diabetes experience weight discrimination (e.g., others’ awareness (or not) of the diagnosis).
This research is among the first to our knowledge to examine the association between weight discrimination and odds of diabetes in a sample of older adults—including testing for moderation by social support and resilience. This investigation is strengthened by its utilization of a nationally representative sample of U.S. older adults, permitting the generalization of findings to this broader population that is sometimes understudied relative to other age groups in weight discrimination research. Furthermore, the present analyses adjusted for BMI throughout, shedding light on the independent association between weight discrimination and diabetes over and above the well-established predictor of BMI. Finally, this study is strengthened by its incorporation of objective, hemoglobin A1c data in the assessment of diabetes status, building upon prior research that exclusively relied upon self-reports of diabetes diagnoses (Sutin, Stephan, Carretta et al., 2015; Udo et al., 2016).
The primary limitation of the present research is its reliance upon cross-sectional data, which does not provide causal evidence about any potential directionality of the association between weight discrimination and diabetes or information about the position of moderators in potential causal pathways. As noted previously, given the data available, it remains possible that those with a history of diabetes were more likely to experience weight discrimination. Individuals with type 2 diabetes may be at increased risk for weight gain (and thereby weight discrimination) through mechanisms such as use of anti-diabetic medicines (Kalra et al., 2018) or impaired exercise tolerance (Nesti et al., 2020). However, our inclusion of BMI as a covariate statistically adjusts for any potential effects of diabetes on weight discrimination via a pathway of weight. Future investigations should build upon these findings to test the extent to which weight discrimination is associated with incident diabetes. Further research might also examine how diabetes relates to temporal factors such as the age at which weight discrimination was first experienced or the cumulative duration of exposure to weight discrimination across the lifespan.
We also note that the present investigation analytically treats emotional social support as a moderator, with the assumption that this construct exhibits relative stability over time. Indeed, research among older adults suggests that with increasing age, levels of received emotional social support appear to remain stable (Shaw et al., 2007). Consistent with this finding, various scholars and theories have posited that as individuals lose support from more peripheral social ties over the life course, they compensate with gains in emotional support from their remaining, more intimate social ties (Shaw et al., 2007).
Additional limitations of this study include the nature of the measures of weight discrimination and diagnosed diabetes. The Everyday Discrimination Scale (Williams et al., 1997) inquires about discrimination related to weight or height; however, this instrument has been used in many studies of weight discrimination to date. Furthermore, when following the analytic approach of prior research (Puhl et al., 2008), our ancillary results suggest that the reported discrimination is more closely related to weight than height, mitigating potential concern about confounding with height discrimination. In addition, the present assessment of diagnosed diabetes did not ask respondents to specify whether they had type 1 or type 2 diabetes. However, the other preliminary studies of weight discrimination and diabetes also did not specify the type of reported diabetes (Sutin, Stephan, Carretta et al., 2015; Udo et al., 2016), and the present investigation took an additional step to address this limitation by conceptualizing diabetes diagnosed before age 40 as type 1 (out of scope), rather than type 2.
Finally, future research might also examine how other types of discrimination (e.g., related to race or ethnicity) might intersect and/or compound with weight discrimination in their associations with diabetes. A large national study among U.S. adults found that those who reported multiple major experiences of discrimination attributed to race or ethnicity (vs. none) showed a 36% greater risk of developing type 2 diabetes (Whitaker et al., 2017). Further research on the physical health of those who report experiencing both weight and racial/ethnic discrimination could yield new information for addressing the longstanding racial and ethnic disparities in diabetes prevalence that persist in the U.S. today (Cheng et al., 2019).
In conclusion, the present findings suggest a positive association between weight discrimination and diabetes among older adult women. This study also provides novel evidence that trait resilience and social support moderate links between weight discrimination and diabetes. We encourage future longitudinal investigations to examine the potential temporality and underlying mechanisms of these relationships. Findings from ongoing research in this area may inform the development of psychosocial interventions to prevent the development of diabetes among individuals who experience weight discrimination.
Data Availability
The datasets analyzed in the current study are available in the NACDA public repository at:
https://www.icpsr.umich.edu/web/NACDA/studies/20541 (Round 1);
https://www.icpsr.umich.edu/web/NACDA/studies/34921 (Round 2); and
https://www.icpsr.umich.edu/web/NACDA/studies/36873 (Round 3).
The study measures are available at in the NACDA public repository at:
https://www.icpsr.umich.edu/web/NACDA/studies/20541 (Round 1);
https://www.icpsr.umich.edu/web/NACDA/studies/34921 (Round 2); and
https://www.icpsr.umich.edu/web/NACDA/studies/36873 (Round 3).
Code Availability
The data code for this work is available upon request.
Notes
Hba1c was also measured in 2015-16; however, assay results are not yet available and are therefore not considered here.
Of the 1,210 respondents who reported taking anti-diabetic agent medications, only ~ 5.8% (n = 70) did not show at least one other indicator of diabetes (i.e., a diagnosis and/or an Hba1c value of 6.5% or higher). In hypothesis testing, the pattern of results remained the same regardless of whether the analyses coded these respondents as having diabetes or not.
When following this categorization, there were two instances in which the statistical program was unable to estimate the models testing the simple effect of weight discrimination among respondents with high friend support due to collinearity. In these instances, to gain some insight into the association, we repeated these models by instead defining high friend support as opening up to and relying on friends “some of the time” or “often”, and low support as doing so “hardly ever or rarely” or “never,” which resulted in complete model estimation.
References
Bellou, V., Belbasis, L., Tzoulake, I., & Evangelous, E. (2018). Risk factors for type 2 Diabetes Mellitus: An exposure-wide umbrella review of meta-analyses. PloS One, 13(3), e0194127. https://doi.org/10.1371/journal.pone.0194127
Björntorp, P. (1990). Portal adipose tissue as a generator of risk factors for Cardiovascular Disease and Diabetes. Arteriosclerosis, 10, 493–496.
Centers for Disease Control and Prevention (2023). What is Diabetes? https://www.cdc.gov/diabetes/basics/diabetes.html
Cheng, F. W., Gao, X., Mitchell, D. C., Wood, C., Still, C. D., Rolston, D., & Jensen, G. L. (2016). Body mass index and all-cause mortality among older adults. Obesity (Silver Spring), 24(10), 2232–2239. https://doi.org/10.1002/oby.21612
Cheng, Y. J., Kanaya, A. M., Araneta, M. R. G., Saydah, S. H., Kahn, H. S., Gregg, E. W., & Imperatore, G. (2019). Prevalence of diabetes by race and ethnicity in the United States, 2011–2016. Journal of the American Medical Association, 322(24), 2389–2398. https://doi.org/10.1001/jama.2019.19365
Dickerson, S. S., & Kemeny, M. E. (2004). Acute stressors and cortisol responses: A theoretical integration and synthesis of laboratory research. Psychological Bulletin, 130(3), 355–391.
Dutton, G. R., Lewis, T. T., Durant, N., Halanych, J., Kiefe, C. I., Sidney, S., & Lewis, C. E. (2014). Perceived weight discrimination in the CARDIA study: Differences by race, sex, and weight status. Obesity (Silver Spring), 22(2), 530–536. https://doi.org/10.1002/oby.20438
Emmer, C., Bosnjak, M., & Mata, J. (2020). The association between weight stigma and mental health: A meta-analysis. Obesity Reviews, 21(1), e12935. https://doi.org/10.1111/obr.12935
Gerend, M. A., Patel, S., Ott, N., Wetzel, K., Sutin, A. R., Terracciano, A., & Maner, J. K. (2021). Coping with weight discrimination: Findings from a qualitative study. Stigma and Health. https://doi.org/10.1037/sah0000335
Hackett, R. A., & Steptoe, A. (2017). Type 2 Diabetes Mellitus and psychological stress — a modifiable risk factor. Nature Reviews Endocrinology, 13, 547–560.
Hawkley, L., Wroblewski, K., Cagney, K., & Waite, L. J. (2021). Resilience and social support-giving scales: Conceptual and empirical validation. Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 76(Supplement_3), S238–S250. https://doi.org/10.1093/geronb/gbab091
Himmelstein, M. S., & Puhl, R. M. (2020). At multiple fronts: Diabetes stigma and weight stigma in adults with type 2 Diabetes. Diabetic Medicine, 38(1), e14387. https://doi.org/10.1111/dme.14387
Himmelstein, M. S., Puhl, R. M., & Quinn, D. M. (2019). Overlooked and understudied: Health consequences of weight stigma in men. Obesity (Silver Spring), 27(10), 1598–1605. https://doi.org/10.1002/oby.22599
Hsieh, N., & Hawkley, L. (2018). Loneliness in the older adult marriage: Associations with dyadic aversion, indifference, and ambivalence. Journal of Social and Personal Relationships, 35(10), 1319–1338. https://doi.org/10.1177/0265407517712480
Hunger, J. M., & Tomiyama, A. J. (2014). Weight labeling and obesity: A longitudinal study of girls aged 10 to 19 years. JAMA Pediatrics, 168(6), 579–580. https://doi.org/10.1001/jamapediatrics.2014.122
Kalra, S., Bahendeka, S., Sahay, R., Ghosh, S., Md, F., Orabi, A., & Das, A. K. (2018). Consensus recommendations on sulfonylurea and sulfonylurea combinations in the management of type 2 Diabetes Mellitus–international Task Force. Indian Journal of Endocrinology and Metabolism, 22(1), 132–157. https://doi.org/10.4103/ijem.IJEM_556_17
Katan, M. B., & Ludwig, D. S. (2010). Extra calories cause weight gain—but how much? Journal of the American Medical Association, 303(1), 65–66. https://doi.org/10.1001/jama.2009.1912
Major, B., Eliezer, D., & Rieck, H. (2012). The psychological weight of weight stigma. Social Psychological and Personality Science, 3(6), 651–658. https://doi.org/10.1177/1948550611434400
Major, B., Hunger, J. M., Bunyan, D. P., & Miller, C. T. (2014). The ironic effects of weight stigma. Journal of Experimental Social Psychology, 51, 74–80. https://doi.org/10.1016/j.jesp.2013.11.009
Mayo Clinic (2021). Type 2 diabetes. Retrieved November 8, 2021 from https://www.mayoclinic.org/diseases-conditions/type-2-diabetes/symptoms-causes/syc-20351193
Mayo Clinic (2022). July 7, 2022). Type 1 diabetes. https://www.mayoclinic.org/diseases-conditions/type-1-diabetes/symptoms-causes/syc-20353011
Mobasseri, M., Shirmohammadi, M., Amiri, T., Vahed, N., Fard, H. H., & Ghojazadeh, M. (2020). Prevalence and incidence of type 1 Diabetes in the world: A systematic review and meta-analysis. Health Promotion Perspectives, 10(2), 98–115. https://doi.org/10.34172/hpp.2020.18
Nagpal, T. S., Tomiyama, A. J., & Rodriguez, A. C. I. (2021). Beyond BMI: Pregnancy-related weight stigma increases risk of gestational Diabetes. Primary Care Diabetes. https://doi.org/10.1016/j.pcd.2021.07.002
Nesti, L., Pugliese, N. R., Sciuto, P., & Natali, A. (2020). Type 2 Diabetes and reduced exercise tolerance: A review of the literature through an integrated physiology approach. Cardiovascular Diabetology, 19(1), 1–17. https://doi.org/10.1186/s12933-020-01109-1
O’Muircheartaigh, C., English, N., Pedlow, S., & Kwok, P. K. (2014). Sample design, sample augmentation, and estimation for Wave 2 of the NSHAP. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 69(S2), S15–S26. https://doi.org/10.1093/geronb/gbu053
O’Muircheartaigh, C., Eckman, S., & Smith, S. (2009). Statistical design and estimation for the National Social Life, Health, and Aging Project. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 64B(suppl 1), i12–i19. https://doi.org/10.1093/geronb/gbp045
Pradhan, A. D., Manson, J. E., Rifai, N., Buring, J. E., & Ridker, P. M. (2001). Creactive protein, interleukin 6, and risk of developing type 2 Diabetes Mellitus. Journal of the American Medical Association, 286(3), 327–334. https://doi.org/10.1001/jama.286.3.327
Puhl, R. M., Andreyeva, T., & Brownell, K. D. (2008). Perceptions of weight discrimination: Prevalence and comparison to race and gender discrimination in America. International Journal of Obesity, 32(6), 992–1000. https://doi.org/10.1038/ijo.2008.22
Puhl, R. M., Latner, J. D., O’Brien, K., Luedicke, J., Daníelsdóttir, S., & Forhan, M. (2015). A multinational examination of weight bias: Predictors of anti-fat attitudes across four countries. International Journal of Obesity, 39(7), 1166–1173. https://doi.org/10.1038/ijo.2015.32
Roehling, P. V. (2012). Fat is a Feminist issue, but it is complicated: Commentary on Fikkan and Rothblum. Sex Roles, 66(9), 593–599. https://doi.org/10.1007/s11199-011-0059-5
Santos-Lozano, A., Pareja-Galeano, H., Sanchis-Gomar, F., Quindós-Rubial, M., Fuiza-Luces, C., Cristi-Montero, C., & Luica, A. (2016). Physical activity and Alzheimer disease: A protective association. Mayo Clinic Proceedings, 91(8), 999–1020.
Scandurra, C., Bochicchio, V., Amodeo, A. L., Esposito, C., Valerio, P., Maldonato, N. M., & Vitelli, R. (2018). Internalized transphobia, resilience, and mental health: Applying the Psychological Mediation Framework to Italian transgender individuals. International Journal of Environmental Research and Public Health, 15(3), 508. https://doi.org/10.3390/ijerph15030508
Shaw, B. A., Krause, N., Liang, J., & Bennett, J. (2007). Tracking changes in social relations throughout late life. Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 62(2), S90–S99. https://doi.org/10.1093/geronb/62.2.S90
Sutin, A. R., & Terracciano, A. (2013). Perceived weight discrimination and obesity. PloS One, 8(7), e70048. https://doi.org/10.1371/journal.pone.0070048
Sutin, A. R., Stephan, Y., Luchetti, M., & Terracciano, A. (2014). Perceived weight discrimination and C-reactive protein. Obesity (Silver Spring), 22(9), 1959–1961. https://doi.org/10.1002/oby.20789
Sutin, A. R., Stephan, Y., Carretta, H., & Terracciano, A. (2015). Perceived discrimination and physical, cognitive, and emotional health in older adulthood. The American Journal of Geriatric Psychiatry, 23(2), 171–179. https://doi.org/10.1016/j.jagp.2014.03.007
Sutin, A. R., Stephan, Y., & Terracciano, A. (2015). Weight discrimination and risk of mortality. Psychological Science, 26(11), 1803–1811. https://doi.org/.
Talumaa, B., Brown, A., Batterham, R. L., & Kalea, A. Z. (2022). Effective strategies in ending weight stigma in healthcare. Obesity Reviews, 23(10), e13494. https://doi.org/10.1111/obr.13494
Tomiyama, A. J. (2014). Weight stigma is stressful. A review of evidence for the cyclic Obesity/Weight-Based stigma model. Appetite, 82, 8–15. https://doi.org/10.1016/j.appet.2014.06.108
Tsenkova, V. K., Carr, D., Schoeller, D. A., & Ryff, C. D. (2011). Perceived weight discrimination amplifies the link between central adiposity and nondiabetic glycemic control (HbA1c). Annals of Behavioral Epidemiology, 41(2), 243–251. https://doi.org/10.1007/s12160-010-9238-9
Udo, T., Purcell, K., & Grilo, C. M. (2016). Perceived weight discrimination and chronic medical conditions in adults with overweight and obesity. International Journal of Clinical Practice, 70(12), 1003–1011. https://doi.org/10.1111/ijcp.12902
van der Valk, E. S., van der Voorn, B., Iyer, A. M., Mohseni, M., Leenen, P. J., Dik, W. A., & van Rossum, E. F. (2021). Hair cortisol, obesity and the immune system: Results from a 3 year longitudinal study. Psychoneuroendocrinology, 134, 105422. https://doi.org/10.1016/j.psyneuen.2021.105422
Wagnild, G. M., & Young, H. M. (1993). Development and psychometric evaluation of the Resilience Scale. Journal of Nursing Measurement, 1(2), 165–178.
Watson, L. B., Morgan, S. K., & Craney, R. (2018). Bisexual women’s discrimination and mental health outcomes: The roles of resilience and collective action. Psychology of Sexual Orientation and Gender Diversity, 5(2), 182–193. https://doi.org/10.1037/sgd0000272
Whitaker, K. M., Everson-Rose, S. A., Pankow, J. S., Rodriguez, C. J., Lewis, T. T., Kershaw, K. N., & Lutsey, P. L. (2017). Experiences of discrimination and incident type 2 Diabetes Mellitus: The multi-ethnic study of Atherosclerosis (MESA). American Journal of Epidemiology, 186(4), 445–455. https://doi.org/10.1093/aje/kwx047
Williams, D. R., Yu, Y., Jackson, J. S., & Anderson, N. B. (1997). Racial differences in physical and mental health, socio-economic status, stress, and discrimination. Journal of Health Psychology, 2(3), 335–351. doi: 10.1177/135910539700200305
Yi, S. W., Ohrr, H., Shin, S. A., & Yi, J. J. (2015). Sex-age-specific association of body mass index with all-cause mortality among 12.8 million Korean adults: A prospective cohort study. International Journal of Epidemiology, 44(5), 1696–1705. https://doi.org/10.1093/ije/dyv138
Acknowledgements
The authors gratefully thank Kristen Wroblewski for her feedback on the manuscript.
Funding
This work was supported by the National Institute on Aging (5R01AG060756-04). The National Social Life, Health and Aging Project is also supported by the National Institute on Aging and the National Institutes of Health (R01AG021487, R37AG030481, R01AG033903, R01AG043538, and R01AG048511). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author information
Authors and Affiliations
Contributions
LEF generated study hypotheses, analyzed the data, and drafted the manuscript. LEF and LCH designed the study, interpreted the data, edited the manuscript, and approved the final manuscript for submission. LPS, MKM, JI, and ESH interpreted the data and approved the final manuscript for submission.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to disclose.
Ethics approval
Not applicable; this work comprises secondary data analysis of de-identified existing public data.
Consent to participate
All respondents provided their informed consent to participate in the study.
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Finch, L.E., Hawkley, L.C., Schumm, L.P. et al. Moderation of associations between weight discrimination and diabetes status by psychosocial factors. J Behav Med 47, 244–254 (2024). https://doi.org/10.1007/s10865-023-00454-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10865-023-00454-2