
Abstract
A large body of work documents the utility of behavioral risk tasks for making inferences about adolescent risk-taking proclivities and related emotional and motivational correlates. Much less attention has been paid to risk-avoidance during adolescence. We provide validity data for a behavioral measure designed to assess avoidance, the Balloon Risk-Avoidance Task (BRAT). We examined avoidance in 127 youth, ages 10–17 (51% female, 68% Caucasian). Correlation analyses indicated significant positive associations between anxiety, fear, and BRAT avoidance behavior. Providing discriminant validity, avoidance on the BRAT was unrelated to depressive symptoms, depressed mood, or trait surgency (approach motivation). The BRAT was negatively associated with risk-taking behavior on the Balloon Analog Risk Task (BART). IQ and age were not associated with avoidance on the BRAT. We found that females showed significantly more avoidance behavior than males, but sex did not moderate the association between anxiety and avoidance. Cluster-based analyses revealed a subset of youth in mid-to-late adolescence showing significantly greater levels of avoidance behavior on the BRAT. These adolescents had higher levels of reported anxiety symptoms compared to individuals in mid-to-late who show lower levels of avoidance. Findings are discussed in terms of the clinical implications and the potential role that avoidance serves as both protective and risk factors in youth.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
A large body of work examines risk-taking across mental health (e.g., ADHD, conduct disorder, borderline personality) and high-risk domains (e.g., alcohol use, substance use, injury), which is often framed from the perspective of approach motivation and sensation seeking (Coffey et al., 2011; Collado et al., 2014; Jinnah & Stoneman, 2016; Shoham et al., 2016). While the definition of risk can vary depending on who you ask (i.e., economist versus a psychologist), in this context risk is defined as the exposure to possible loss or harm (see Schonberg et al., 2011). Given the rise in the prevalence of anxiety disorders in adolescence (Kessler et al., 2007), we might expect to see greater risk-avoidance among some adolescents (Eisenberg et al., 1998; Lorian & Grisham, 2011; Maner et al., 2007), where risk avoidance is defined as the action of keeping away from or not doing things that expose the individual to loss or harm. Yet, in the pursuit of understanding adolescent development, the field has focused heavily on risk-taking, those behaviors that put the individual at-risk for less favorable outcomes (substance use, unprotected sex, antisocial behavior). At present, a Pubmed search yields 32,000 papers under the search terms “risk-taking” and adolescence whereas “risk-aversion” or “risk avoidance” and adolescence yields approximately 1000 papers. Consideration of avoidance has important consequences for the expression of risk in that both avoidance and approach motivation contribute to the expression of risk behaviors. For instance, a teenager asking someone to the prom may weigh the anticipated joy of securing the date and the potential fun to follow, against the possibility of being declined. At the extreme, clinically anxious individuals engage in avoidance of feared consequences, putatively based on perceived risks, by performing within-situation safety behaviors (Clark & Wells, 1995).
Many studies examine the association between positive reinforcement and risk-taking in children and adolescents (Colder et al., 2013; Lejuez et al., 2002; van Duijvenvoorde et al., 2016), with some work indicating that loss anticipation promotes more conservative choices on risk tasks (Winkielman et al., 2007) and that risk proclivity relates to reported risk-taking behavior, especially in persons low in distress tolerance (MacPherson et al., 2010). Models of risk-taking, particularly prospect theory, propose that, for most people, losses “loom larger” than gains (Kahneman & Tversky, 1990), typically termed loss aversion, which can lead to risk-averse behavior when both gains and losses are possible. That is, given an equal amount to be won or lost, the loss is assigned greater weight by the individual. In the economic literature, risk-aversion refers specifically to the avoidance behavior people engage in when they are exposed to uncertainty, in a financial context.
A conspicuous aspect in some behavioral risk-taking tasks is the mix of approach motivation (e.g., point, prizes, money won) and avoidance motivation (e.g., potential for loss). Two good examples of such tasks are the Balloon Analogue Risk Task (BART, Lejuez et al., 2002) and the Iowa Gambling Task (IGT, Bechara et al., 1994). In the case of the BART, as the individual inflates a balloon with increasing pumps the have the potential to gain more points, but also with the increasing risk of loss due to the balloon exploding. The main outcome variable is mean number of pumps across ~ 30 balloons. On any given trial, the individual may be more motivated by perceived potential loss or gain—more likely some computation, moment to moment, that considers both motivations. Yet, at the end of a typical task run, what is left is a measure of the average risk the individual is willing to take. A low mean number of pumps could reflect risk-avoidance, but also low approach motivation (at the extremes, anxiety, or anhedonia). A high mean number of pumps could reflect greater risk-taking proclivity. In either case, for an individual playing the BART, their behavior is determined by the net effect of their approach motivation and avoidance motivation. Recent work demonstrates individuals adaptively respond to positive and negative outcomes on the BART, engaging reward and aversive processing brain circuitry along the way (McCormick & Telzer, 2017). As well, computational models with the BART, model both reward sensitivity and loss aversion components (Pleskac & Wershbale, 2014; Wallsten et al., 2005). Similarly, in the IGT the individual chooses cards one at a time from one of four decks. Typically, s/he realizes that, in the long run, two of the decks offer higher payoffs, but also greater losses (net loss), whereas the other two decks have smaller immediate payoffs coupled with relatively smaller losses (net gain). Risk-taking behavior is inferred by the tendency to choose the two "high-risk" decks more often (high reward) than the "safe" decks or continuing to prefer/choose these higher reward-higher loss decks for more trials into the task.
Risk-Aversion and Avoidance in Adolescence
Although there is considerable evidence that adolescence is a time of increased risk-taking (Amstadter et al., 2012; Lejuez et al., 2005; Steinberg, 2008), this sentiment has become somewhat of a catch phrase for the field with many papers making this assertion as they introduce the topic. Yet, other epidemiological data suggests this perspective casts an incomplete picture of adolescent development (e.g., Rapee & Spence, 2004). For instance, adolescence is accompanied by an increase in anxiety disorders, particularly social anxiety, social phobia, and generalized anxiety (Beesdo et al., 2010; Ollendick & Hirshfeld-Becker, 2002; Rapee & Spence, 2004; Sumter et al., 2010). Given that anxiety is strongly associated with avoidance, we might expect some adolescents to show increases in avoidance behavior during this time. In a large community sample of youth, Sumter and colleagues (Sumter et al., 2009) found age-related increases in self-reported distress and avoidance in relation to formal speaking and social interactions. More recently, a longitudinal study by Miers et al. (2014) used trajectory analyses to characterize low and high avoidance pathways across development. Although the pathways were comparable in early development, a clear divergence emerged during adolescence such that social anxiety and post-event rumination were characterized by high levels of avoidance (Miers et al., 2014). Recent studies suggest that individuals with severe levels of anxiety, have a “safety bias”, reflected in cross-situational risk-avoidance (Lorian & Grisham, 2010). In turn, this bias may drive widespread avoidance behavior and anxiety maintenance (Maner et al., 2007). Avoidance and safety behaviors are thought to be maintained through negative reinforcement, the process by which removal of an aversive state brings relief to the individual. Taken together, avoidance behavior, risk-avoidance, and anxiety are undoubtedly important facets of motivated decision-making in adolescence and have important implications for self-regulation, anxiety disorder risk and broader psychopathology.
The Balloon Risk Avoidance Task (BRAT)
Admittedly, most if not all, behavioral tasks aimed at understanding risk-taking or risk-avoidance can have both approach and avoidance motivation. Our solution to this complexity was to invert the procedure of the BART with our development of the Balloon Risk-Avoidance Task (BRAT). In contrast to behavioral risk-taking tasks such as the BART, the BRAT biases participants towards perception of risk, which we believe has strong potential to capture individual variability in avoidance behavior. In the BRAT, at the outset of each trial, a single lifelike balloon inflates to full value (128 pumps, maximum points for prizes) on a computer screen (Fig. 1). The balloon is at full capacity and is certain to explode if no action is taken. As the balloon inflates, a danger meter next to the balloon rises from safe (blue) to red (danger), proportionately to the inflation of the balloon. During task practice, participants are shown that each balloon is sure to explode if not deflated to some degree by releasing some of the air. If the balloon explodes, the participant loses the opportunity to preserve any points for that balloon. Thus, risk is maximal and certain at the outset of each trial. The participant uses a mouse and a number dial to decide the extent to which they want to deflate the balloon to make it “safer”. However, the more air let out of the balloon, the less valuable it is. The main dependent variable for the BRAT is mean number for deflation, with greater deflation indicating greater risk-avoidance. Important differences between the BRAT and the BART include: (i) the participant is endowed with all the points they can possibly gain (i.e., 128) at the beginning of the trial, (ii) they are asked to give up points to decrease risk of losing all of them, (iii) a “danger meter” reminds the participant that balloons with greater inflation pose more “danger,” and less inflated balloons are “safer,” (iv) and the participant is under mild time pressure to make a decision, as the balloon will explode if they do not respond in a specified time window (6 s). From a prospect theory perspective (Kahneman & Tversky, 1979), participants' reference point is 128 points and for any choice they make they stand to lose from that amount.

Trial sequence of the BRAT. Trial 1 depicted for a single balloon of the 30 played sequentially. The trial begins with a “?”. A mouse click advances to the inflate screen in which the balloon fully inflates before the subject (associated with maximum number of points). The danger meter to the right of the balloon rises from “safe” to “danger”. Participants then have a finite amount of time (6 s) to decide how much they want to deflate a balloon to avoid a certain balloon explosion (Timer screen). A red, segmented timer indicates the elapsed time. On the Timer screen, the mouse cursor appears. The yellow numerical dial is used with the mouse to select the pumps to deflate the balloon, 1–127. The selected number appears beneath the balloon, and “D” executes the deflation, while selecting “clear” clears the selection. The balloon deflates, based on subject input, proportionately shrinking the danger meter. Then an outcome is observed, either points kept safe, or lost when a balloon explodes. Cumulative performance is tracked with the boxes on the right of the screen (Balloons kept, Points kept, Balloon number)
The Present Study
This validation study of the BRAT included community male and female youth ages 10–17 years. We examined the association between our main measure of avoidance, BRAT deflation, and parent report of youth anxiety and fear as indicators of criterion validity. We expected these measures would be positively associated with number of pumps deflated on the BRAT. In terms of discriminant validity, we examined behavior on the BART, as well as depressive symptoms, depressed mood, and the temperament trait of surgency (approach motivation). We expected that these measures would be unrelated to mean avoidance on the BRAT. Given that some work suggests that females may be more risk averse in some circumstances (Byrnes et al., 1999; Groppe et al., 2013; Spreckelmeyer et al., 2013), and at elevated risk for anxiety disorder in adolescence (Grills-Taquechel et al., 2010; McLean et al., 2011; van Oort et al., 2011), we examined sex differences on BRAT avoidance. Finally, given the increased onset of anxiety disorders across puberty, we examined anxiety as a function of avoidance on the BRAT across age and puberty.
Method
Participants
The sample consisted of 127 children and adolescents (67 female), recruited via a mass mailing list provided by a credit mailing company, Experian. For an individual parent to be in this database, they must have a credit history. Through the Experian portal, we specified postal codes for towns surrounding New Haven CT and the search criterion, that households had children in the 10–17 age range. We purchased ~ 5000 address labels and had a 3.9% return rate. Parents received an introductory letter briefly describing the nature of the study and requesting further contact information (cell phone, email, best time to contact) and verifying eligible children were present. Parents who returned the contact sheet were invited via telephone to have their child participate in the present study or other studies occurring in our laboratory. Children were fluent in English and had no evidence of serious mental illness (psychosis, autism, bipolar disorder), assessed via a parental telephone screen. Children were considered ineligible for the study if their caregiver, typically their mother, reported that the child in question was being treated for, or carried a diagnosis of psychosis, autism, or bipolar disorder.
Once recruited into the study and consented, the participant and their parent or guardian participated in-person across three visits over three weeks at the Child Study Center, New Haven, CT. The main aim of the parent study was to examine the impact of stress on children’s psychosocial functioning, substance use risk behavior and reward processing. The first visit, reported here, lasted approximately two hours, and included the parent permission/assent procedure, description of all three visits and focused on characterizing youth via parent report measures, self-report measures and behavioral tasks. Participants completed all surveys via computer and then the behavioral tasks. The second visit, lasting three hours reported elsewhere, included an EEG and the Trier Social Stress Test (Wu et al., 2019). The third visit, lasting 1.5 h, involved youth parent discussion of conflict (Chaplin et al., 2012). Visits were conducted either by an MD or PhD level investigator or a trained post baccalaureate research assistant.
Children were intellectually in the low average to very superior range (verbal IQ mean = 112.25, SD = 12.88, range 82–139) (Wechsler, 1999). The mean age of the children was 13.82 years (SD = 2.03 years, range = 10.10–17.78 years). The reported ethnicity among the final sample of children was as follows: 12% African American, 8.8% Hispanic, 6.4% Asian, 3.2% Native American and 68% White, 1.6% other. This research was approved by the Yale University School of Medicine Human Investigation Committee. Four children lacked a BRAT behavioral assessment, and three children lacked a questionnaire assessment. The order of behavioral tasks were counterbalanced across the sample.
Measures
The Balloon Risk Avoidance Task (BRAT, Fig. 1, see supplementary materials for further details)
The BRAT involves deflating a computer-generated balloon that is sure to pop. The BRAT consists of 30 balloons, played one at a time, each worth 128 points. At the beginning of a trial, the participant is endowed with all the points they could possibly gain (i.e., 128), and they are asked to give up some points to decrease risk of losing all the points for a given balloon. After moving through a set of instruction screens with the experimenter, describing the general principles of the game, the participant practices using the deflate dial and completes two practice trials (both rigged not to pop). Next the participant works through the 30 trials sequentially. Trials follow the following sequence: Begin, Inflate, Timer, Deflate, Outcome (Win or Loss) (Figs. 1, 2). The participant initially sees a question mark in the center of the screen prompting them that the trial is about to begin. Next, the participant watches a balloon inflate to the point of bursting, indicating the maximal level of risk. A meter next to the balloon rises from a safe level (blue) to a red level (danger). The participant has 6 s to deflate the balloon before it bursts. A red, segmented timer indicates the elapsed time. If the participant fails to deflate the balloon before the response deadline, then it immediately explodes. In this automatic version, the participant can deflate the balloon by inputting a number between 1 and 128 into a dial with a mouse (rather than pressing a button for each pump deflated). However, by deflating the balloon the participant also returns some of the points they could possibly earn. For example, if the participant decides to deflate the balloon by 88 points, and the balloon does not pop, then the participant keeps the remaining 40 points. If a balloon is left inflated past its explosion point, then the balloon explodes, and the participant loses all the points for that trial. Explosion points are predetermined, following a normal distribution identical to the BART (Lejuez et al., 2002), with a mean of 64. Relevant dependent measures on this task are number of pumps deflated (risk-avoidance), number of balloons popped and reaction time to key in a deflation amount. Before the game each participant views a prize book, with prizes values associated with points earned (see below for more detail).

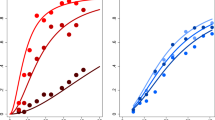
BRAT avoidance plotted against age (top) and puberty (middle). BRAT derived avoidance clusters shows a distinct group of individuals in mid-to-late puberty who are prone to avoidance (bottom)
The Balloon Analog Risk Task (BART) (Lejuez et al., 2002; Pleskac et al., 2008)
The BART involves inflating a computer-generated balloon that can explode if over-inflated. The BART consists of 30 balloons, played one at a time, each worth a maximum of 128 points. On each trial, for this automatic version of BART, the participant is presented with a balloon and must inflate the balloon by inputting a number between 1 and 128 where higher numbers indicate more pumps/inflation and more points. By inflating the balloon the participant also increases the potential risk for explosion and a total loss of points for the current trial. Explosion points are predetermined, following a normal distribution (Lejuez et al., 2002), with a mean of 64. The main dependent measure on this task is the number of pumps inflated (risk taking). Before the game each participant views a prize book, with prizes values associated with points earned. Prizes were gift cards (iTunes, Amazon, Barnes & Noble). At the end of the visit, all participants received the same level of compensation, regardless of their performance, choosing cards equivalent to $40.
Screen for Child Anxiety Related Emotional Disorders—Parent Form (SCARED) (Birmaher et al., 1997; 1999)
The SCARED is a measure assessing anxiety disorder symptoms in children and adolescents ages 8 to 18 years. Composed of 41 items, informants are asked the frequency of each symptom on a 3-point-scale: 0 (almost never), 1 (sometimes), 2 (often). The SCARED has four factors: somatic/panic (12 items), generalized anxiety (9 items), separation anxiety (13 items) and social phobia (7 items), which have shown good reliability, with Cronbach’s alphas ranging from 0.70, –0.78 across scales. Originally devised to screen anxiety disorders in clinical samples (Birmaher et al., 1997, 1999), the SCARED has also proven useful for screening anxiety in community samples (Hale et al., 2005; Muris et al., 1998).
Early Adolescent Temperament Questionnaire—Revised Parent Form (Ellis & Rothbart, 2001)
The EATQ-R is based on an earlier version of the measure, the Early Adolescent Temperament Questionnaire (EATQ, Capaldi & Rothbart, 1992) and has been revised to include aspects of temperament related to self-regulation in adolescents (Ellis & Rothbart, 2001). The questionnaire is used with youth age 9 or older and consists of 103 questions related to 11 temperamental and 2 behavioral domains. Parents are asked to rate how true statements are for their child (e.g., “It often takes very little to make my child feel like crying”) on a 1 to 5 scale, with a score of 1 meaning “always untrue for me” and a score of 5 meaning “always true for me”. The measure has been found to be reliable and valid measure of adolescent temperament (Ellis & Rothbart, 2001). For the purposes of this study, we used fearful temperament as a measure of criterion validity and depressive mood and surgency (which refers to emotional responses to high-intensity stimuli and low levels of fear and shyness) as measures of discriminant validity.
Children’s Symptom Inventory—Parent Form (CSI-4, Gadow & Sprafkin, 1994)
The CSI-4 assesses symptoms related to DSM-IV criteria. For Symptom Severity scores, items are rated from 0 to 3 (0 = never, 3 = very often). For the purposes of this report, we examined anxiety related scales on the CSI as a total anxiety index by summing items from the Generalized Anxiety Disorder (GAD), Separation Anxiety Disorder (SAD), Social Phobia, Specific Phobia scales (20 items total; Cronbach’s alpha = 0.77). For discriminant validity purposes, we examined the Major Depressive Disorder (MDD) scale, which paralleled the depression scale examined on the EATQ. The CSI-4 reliability, and convergent and discriminant validity in community-based normative and clinic-referred samples are well-established (Gadow & Sprafkin, 1997).
Intellectual Functioning
All children completed the Vocabulary and Similarities subscales of the Wechsler Abbreviated Scale of Intelligence (WASI, Wechsler, 1999), which were used to estimate a verbal IQ based on standard norms. Prior validation studies have indicated that the WASI two-subtest IQ shows strong correlations (0.80 or higher) with longer measures of intelligence (Wechsler, 1999).
Adolescents completed the Pubertal Development Scale—Self Report (PDS, Petersen et al., 1988)
The PDS Self Report contains 5 items scored from 1 to 4. The PDS total score estimates the pubertal status of the adolescent based on the presence or absence of developmental features such as growth spurt, pubic hair growth and skin changes in both boys and girls, as well as gender specific pubertal changes. We used the PDS total score as a dimensional measure in this study.
Results
In keeping with a large body of work on the BART, which uses mean number of pumps inflated as a primary indicator of risk-taking, and to reduce possibility of a Type 1 error, we constrained the number of analyses to focus on mean deflation as our index of avoidance on our BRAT. Mean deflation and number of explosions (balloons popped) were highly correlated, r = − 0.92, p < 0.001, whereas the amount of time taken to input a number for deflation was unrelated to either deflation or number of explosions, rs = 0.02, − 0.004, n.s., respectively. We examined the effect of administration order on the BRAT (pumps deflated) vs. the BART (pumps inflated). As expected, the main effect was significant, with pumps deflated consistently producing larger values than pumps inflated, F(1, 125) = 103.97, p < 0.001. The interaction of task and order was not significant F(1, 125) = 1.72, p = 0.19, suggesting order of administration did not impact behavior on the BRAT or BART tasks. Descriptive statistics and correlations among major study variables are presented in Table 1.
Validity Evidence for the BRAT
First, we conducted analyses to assess the criterion validity of the BRAT as a measure of avoidance (i.e., mean deflation). Correlation analyses indicated that avoidance on the BRAT was positively associated with two measures of anxiety (SCARED total; CSI anxiety symptoms) and fearful temperament (EATQ fear), rs = 0.24, 0.22 and 0.25, p’s < 0.05, respectively. These anxiety measures were similarly related to number of explosions, r = − 0.22, r = − 0.24, r = − 0.25, p’s < 0.05, respectively, but less strongly and consistently related to the amount of time taken to input a number for deflation, r = 0.18, p = 0.04, r = 0.17, p = 0.07, r = 0.036, p = 0.70.
We examined discriminant validity in two ways. First, avoidance on the BRAT was unrelated to CSI depressive symptoms, EATQ depressive mood, and EATQ surgency, rs = 0.01, 0.11, − 0.11, ns. Second, we examined the BRAT in relation to the BART. The BRAT was negatively correlated with the BART (mean pumps inflated) as would be expected for a risk-avoidance measure and risk-taking measure (r = − 0.57) that have similar task formats. However, BART risk-taking, unlike BRAT avoidance, was associated with age (r = 0.18) and IQ (r = 0.27) but was inconsistently related to anxiety (SCARED r = − 0.16, n.s., CSI Anxiety r = − 0.09, n.s.) and EATQ fear (r = − 0.19, p = 0.037) measures. Relatedly, when we returned to the correlations between BRAT avoidance and our anxiety and fear measures, covarying BART mean pumps, BRAT avoidance continued to be significantly associated with anxiety (SCARED total; CSI anxiety symptoms) and fearful temperament (EATQ fear), r’s = 0.18, 0.21 and 0.18, p’s < 0.05, respectively.
Sex Effects on Risk-Avoidance
Initially, we evaluated sex differences on the BRAT by way of an independent samples t-test, finding that girls show significantly higher levels of avoidance than boys, t(125) = − 1.983, p = 0.049, Cohen’s d = 0.36, (mean pumps deflated for girls 75.97 vs. boys 71.54, Table 2). For purposes of comparison on the BART, while girls pumped more than boys (47.49 vs. boys 52.18, Table 2), this difference did not reach statistical significance, t(125) = 1.819, p = 0.071. Given that the girls in our sample were also rated as more anxious than the boys on the anxiety composite, t(125) = − 2.34, p = 0.034,, Cohen’s d = 0.42, we conducted a moderator analysis to determine whether or not the association between avoidance on the BRAT and anxiety differed as a function of sex (see Table 3). These analyses indicated that, when sex and anxiety were considered together, only anxiety remained significant in the model (Table 3). Moreover, a moderated effect of sex on the relationship between anxiety was not supported (Table 3). Thus, while females show more avoidance on the BRAT, avoidance relates to anxiety similarly in both males and females.
Age and Puberty Effects on Risk-Avoidance
We considered avoidance on the BRAT as a function of age and pubertal stage to assess whether, for some individuals, there is a tendency to be more risk avoidant during adolescence. These comparisons demonstrated that variance in BRAT avoidance is relatively stable across age but shows a crescendo that is maximal during mid-to-late puberty (Fig. 2). Plotting the variability in BRAT deflate across quartiles for age and puberty (assessed dimensionally) showed a clear peak for avoidance during mid-to-late puberty (Fig. 3). To confirm differences in variability across development, Box's M (1949) was used to test the assumption of equal covariance, across quartiles, in the multivariate models for BRAT deflate, age, and puberty. Given that this test is quite powerful, the alpha level of 0.001 is typically used in hypothesis testing (Tabachnick & Fidell, 2013). This test confirmed that, although variance in BRAT avoidance behavior was comparable across age quartiles, Box’s M = 7.022, (F (9, 158,860.045) = 0.75, p = 0.66), the variance in avoidance behavior was significantly different across puberty, Box’s M = 57.493, F (9, 169,861) = 6.18, p < 0.00001).

Variability in BRAT avoidance plotted by quartiles for age (black) and puberty (grey)
We subsequently conducted analyses to identify pubertal clusters based on avoidance behavior on the BRAT. Following the recommendation of Henry et al. (2005) and others (e.g., Prokasky et al., 2017), we used a two-phased cluster analytic approach with hierarchical clustering followed by k-means clustering. Hierarchical cluster analysis provides flexibility in determining the appropriate number of clusters when the numbers of clusters within the data are unknown. Using standardized variables, we applied Ward’s linkage clustering as our hierarchical cluster analysis method, which relies on squared Euclidean distance, followed by inspection of an output dendrogram tree. Dendrograms descriptively provide a guideline for deciding on the number of clusters that should be verified in a second clustering approach, such as k-means clustering. A priori, k-means cluster analysis requires specification of the number of clusters to calculate. This approach yields clusters that are as homogeneous as possible by minimizing within-cluster variance, while maximizing the between-cluster distance (Eshghi et al., 2011). The clustering approaches identified three groups of youth (Fig. 2, bottom), an early puberty group showing moderate levels of avoidance and two mid-to-late puberty groups, one of which presented with higher levels of avoidance on the BRAT. Our use of the labels for our cluster-derived groups (early puberty, mid-to-late puberty, mid-to-late puberty avoidant) are for descriptive purposes on average at the group level. They are not meant to imply that all individuals in group are at the same pubertal level, as groups overlap in their boundaries along the continuum of pubertal status (see Fig. 2, bottom panel).
Given that anxiety disorders increase during adolescence, and are associated with avoidance behaviors, we tested whether the different avoidance puberty clusters varied with respect to SCARED anxiety, CSI Anxiety and EATQ fear measures (see Fig. 4A). Across all three measures, the mid-to-late puberty avoidance group was significantly more anxious and fearful than the other mid-to-late puberty group (see Table 4). We also applied robust estimation to further visualize the differences in the SCARED anxiety, CSI Anxiety and EATQ fear measures across the groups. Re-sampling with replacement 1000 times revealed a clear separation across the groups, such that mean anxiety/fear scores were consistently larger in the mid-to-late puberty avoidance group compared to the other clusters, which showed considerable overlap in their distribution of means (see Fig. 4B).

Panel A Mid-to-late puberty avoidant cluster (blue) shows significantly greater anxiety scores (across the SCARED, CSI Anxiety and EATQ fear measures) compared to mid-to-late puberty cluster. Error bars represent the 95% CI around the mean. Panel B Kernel density plots of 1000 bootstrapped means shows clear separation in between avoidant mid-to-late puberty cluster and mid-to-late puberty cluster across the scales
Discussion
The overall goal of our study was to assess the validity of the BRAT as a measure of avoidance in a child and adolescent sample. Given that avoidance is an integral part of the approach-withdrawal motivations that influences risk-taking, the BRAT was designed to provide a more direct measure of avoidance in youth compared to other tasks framed more toward favoring risk-taking. We found both criterion and discriminant validity for the BRAT in youth, such that avoidance behavior correlated with parental reports of anxiety and fear, but was unrelated to depressive symptoms, depressed mood, or trait surgency (i.e., emotional responsiveness to high-intensity stimuli and low levels of fear and shyness).
Comparison of the BRAT to the BART, a well-established measure of risk-taking, revealed that the two measures were negatively correlated, sharing 32.5% of variance. The BRAT and the BART diverged in several important ways. Whereas youth anxiety was related to BRAT avoidance, youth anxiety was not related to BART risk-taking behavior. While age and IQ predicted BART risk-taking behavior, the BRAT was not significantly related to either age or IQ. Lastly, only the BRAT predicted anxiety symptoms in our study, an association that remained even after controlling for (covarying) behavior on the BART. However, we should mention that other studies have linked the BART to anxiety, for instance Maner and colleagues (Maner et al., 2007) observed adjusted pumps on the traditional BART task was negatively associated with social anxiety and worry among undergraduates.
Other important individual difference factors emerged for the BRAT. We observed that avoidance behaviors increase and become more variable across the 10–17-year age range. Cluster analyses based on pubertal ratings and BRAT avoidance identified a group of adolescents who show pronounced avoidance corresponding to the mid-to-late puberty range, and who were independently rated as more anxious and fearful. We also observed that females were generally more avoidant than males on the BRAT. In the following sections we discuss our findings in the context of developmental implications, sex factors and clinical implications for future studies.
It is well-established that adolescents display an increase in risk-taking compared to other age groups, particularly in emotional and social contexts (Crone et al., 2016; Steinberg, 2008). However, there is also an increase in anxiety during adolescence (Beesdo et al., 2010), which can be characterized by avoidant and inhibited response styles (Allen et al., 2014; Casey, 2015; Clark & Wells, 1995; Lorian & Grisham, 2010; Maner et al., 2007). We wonder if the greater attention capturing aspect of high-risk behaviors (substance use, risky sex, risky driving, etc.), coupled with the prevailing narrative in the literature and popular culture that adolescence is a time of greater risk-taking, has left out an important part of the story, with a significant portion of youth showing proclivity to avoid risk.
Emerging evidence suggests that these avoidance response styles are associated with negative reinforcement processes, including those implicated in problematic anxiety (Crowley & Silverman, 2016). For example, substance use is associated with dysfunction in limbic and prefrontal structures that mediate risk perception and aversion (Fukunaga et al., 2013). Interestingly, some recent task-based imaging work links adolescent anxiety to altered reward system function (for a review, see Lago et al., 2017), with anxious adolescents showing greater striatal activation, compared to controls on the monetary incentive delay task (Bar-Haim et al., 2009; Guyer et al., 2006, 2012). We suspect these findings may reflect the role of negative reinforcement in problematic anxiety. In particular, anxious youth in these studies may be reacting more strongly in reward circuitry, not because they have been rewarded, but rather because they are relieved at not having not lost. Given the spike in the prevalence of anxiety disorders in adolescence (Otto et al., 2001; Rapee & Spence, 2004), understanding the behavioral and neural correlates of avoidance across development is an important step toward establishing effective therapeutic interventions. The availability of avoidance-based measures such as the BRAT could be useful for understanding how avoidance might relate to anxiety risk.
Our finding of greater avoidance on the BRAT is in keeping with meta-analytic work indicating less risk-taking in females (Byrnes et al., 1999). Because avoidance is driven by negative reinforcement processes, sex hormones known to influence reward-based striatal function and corresponding dopamine activity (Bazzett & Becker, 1994; Lago et al., 2017; Peper et al., 2011) need consideration, particularly in adolescence. One of the prevailing models of adolescent development proposes that, in addition to the range of pre-frontal-reward circuitry maturational changes occurring, there is an upsurge of sex hormones (estrogen, testosterone, DHE), which are also thought to impact cognitive-hedonic maturation (Galvan, 2010; Galván, 2013). Yet, work in this area considering adolescent development is scarce (Lago et al., 2017; Peper et al., 2011). One exception is a recent study by Forbes et al. (2010) who found that enhanced levels of testosterone were associated with less striatal activity and more medial prefrontal cortical activity when winning monetary rewards. Moreover, testosterone was positively associated with striatal reactivity for boys in reward anticipation and negatively associated with striatal reactivity in girls and boys during reward outcome. The extent to which gonadal hormones modulate reward circuitry for negative reinforcement (escape/avoidance or aversive conditioning) has yet to be tested but could be important for understanding sex differences in avoidance as we observed on the BRAT.
There are important clinical implications of risk-avoidance. Studies on youth risk-taking have focused on the appetitive motivation, yet youth likely bring different combinations of motivation to risky situations. On the one hand avoidance could be a protective factor, leading some youth to be less likely to engage in risk-taking behaviors. For example, avoidance could minimize the initiation of substance use in the same way that anxiety symptoms can be associated with less severe conduct problems (Walker et al., 1991). On the other hand, among some individuals who show a profile of high avoidance motivation coupled with high approach motivation, greater risk is conferred, as was shown among some college students with problem drinking behavior (Wardell et al., 2011). Thus, pairing risk-taking tasks (such as the BART) with risk avoidance tasks (such as the BRAT) in the prediction of youth risk behavior may provide a more comprehensive picture and more accurate prediction.
High levels of avoidance could predict a tendency toward behaviors that confer anxiety disorder risk. Or even among those youth who do not qualify for an anxiety disorder, they could still bring a “proclivity to avoid” to life choices in a way that limits pursuing opportunity and developing potential. For instance not trying out for a team, expanding a friend group, moving away from home or taking other “healthy risks”. Along these lines, recent work frames “failure to launch” (gaining independence from one’s parents) as a form of avoidance linked anxiety in the transition to adulthood (Hoffman et al., 2018; Lebowitz, 2016).
From the perspective of negative reinforcement, high levels of avoidance could place some youth at increased risk for substance use, driven by affect reduction motives (Hussong et al., 2011). Emerging evidence highlights the relevance of negative affect reduction motives for risk-taking behavior and substance use. Consistent with developmental changes in affect regulation beginning in early adolescence, young people are especially prone to engage in risky behaviors and prospective developmental studies support negative emotionality as an antecedent to multiple forms of risky behaviors (e.g., Cooper et al., 2003; Sher & Slutske, 2003; Wills et al., 2006). Given that avoidance is modulated by anxiety and fear, engagement in risky or problematic behaviors may also serve to escape or avoid negative affect in the short run (e.g., Baumeister & Scher, 1988; Sher, 2007). For example, negative reinforcement models emphasize that substance use motivated by the escape or avoidance of negative external stimuli along with corresponding internal affective states (Baker et al., 2004; Solomon & Corbit, 1974; Wikler, 1965). In this way, individuals with anxiety may be more inclined to engaged in deleterious behaviors as a method to cope with potentially aversive outcomes or perceived affective states. Drug seeking and drug use among high anxious, avoidant individuals, initiates a cascade that subsequently impairs self-regulation and effective coping strategies. This is in line with recent evidence showing that avoidance is related to behavioral inhibition and anxiety pathology (Lorian & Grisham, 2010). With the pattern of greater avoidance we are seeing in mid-adolescence, future work could begin to unpack for whom a greater avoidance proclivity could be a protective factor against risk-taking behavior and for whom greater avoidance proclivity could be a risk factor for problematic anxiety and the types of risky behaviors (i.e., substance use) that are aimed at downregulating anxiety and distress.
Limitations and Future Directions
There are several limitations to the current study. First, we based our criterion and discriminant validity analyses on parent report of youth symptoms of global anxiety and temperament. We did not assess anxiety, risk aversion or avoidance via self-report as this was not the focus of the parent study. Future validation work with the BRAT could also include self-report measures, particularly assessments of risk aversion, anxiety and anxiety subfactors (e.g., social anxiety, worry). Relatedly, it is possible that our lack of an observed negative relation between the BART and anxiety was due to informant and choice of assessment scale. Second, while we assessed for the presence of serious mental illness, we did not assess for other clinical problems such as clinical depression known to affect cognitive abilities or other mental health concerns such as ADHD, known to impact risk-taking. Third, our index of avoidance (mean deflation on the BRAT) could be further validated against real-life avoidance behaviors as has been done with the BART and risk-taking. Fourth, we considered a community sample in this study. While our sample did include 9% of youth whose parents rated them at or above the SCARED clinical cutoff > 25, who also tended to show greater avoidance on the BRAT, future work could include clinically anxious participants to further establish validity of the BRAT at the extremes of anxiety. Our task would also be useful for examining subcomponent processes relevant to anxiety such as intolerance to uncertainty, which has been linked to the onset and maintenance of anxiety and psychopathology more broadly (see McEvoy & Carleton, 2016) and anxiety sensitivity which has been related to negative reinforcement motivations in substance use research (Zvolensky et al., 2008). Moreover, it would be interesting to examine how risk-aversion patterns transition from adolescence to adulthood, with particular attention paid to the decision context (e.g., emotionality, decision versus experienced-based priors, etc.). With respect to generalizability of our findings, we also acknowledge that the average IQ in the current sample was 112, which is considered in the high average range. We are currently conducting a test–retest study to demonstrate reliability in BRAT assessments over time, applying sequential modeling (Park et al., 2021) and other studies incorporating our versions suitable for EEG and fMRI. These studies will help link behavior on the BRAT to the neural correlates of risk-avoidance.
In summary, we provide a new behavioral tool for the assessment of avoidance, which is moderately associated with anxiety symptoms, but was unrelated to depressive symptoms or approach motivation. The simplicity of the BRAT as an assessment tool means that it could be portable across multiple platforms including web and app-based assessments. Our data suggest that while many accounts of adolescent development focus on greater risk-taking, greater avoidance behavior may also be in play—likely with implications for unpacking both risk-taking behavior and problematic anxiety risk.
References
Allen, M. T., Myers, C. E., & Servatius, R. J. (2014). Avoidance prone individuals self reporting behavioral inhibition exhibit facilitated acquisition and altered extinction of conditioned eyeblinks with partial reinforcement schedules. Frontiers in Behavioral Neuroscience, 8, 347. https://doi.org/10.3389/fnbeh.2014.00347
Amstadter, A. B., Macpherson, L., Wang, F., Banducci, A. N., Reynolds, E. K., Potenza, M. N., Gelernter, J., & Lejuez, C. W. (2012). The relationship between risk-taking propensity and the COMT Val(158)Met polymorphism among early adolescents as a function of sex. Journal of Psychiatric Research, 46(7), 940–945. https://doi.org/10.1016/j.jpsychires.2012.04.010
Baker, T. B., Piper, M. E., McCarthy, D. E., Majeskie, M. R., & Fiore, M. C. (2004). Addiction motivation reformulated: An affective processing model of negative reinforcement [Journal; Peer Reviewed Journal]. Psychological Review, 111(1), 33–51.
Bar-Haim, Y., Fox, N. A., Benson, B., Guyer, A. E., Williams, A., Nelson, E. E., Perez-Edgar, K., Pine, D. S., & Ernst, M. (2009). Neural correlates of reward processing in adolescents with a history of inhibited temperament. Psychological Science, 20(8), 1009–1018. https://doi.org/10.1111/j.1467-9280.2009.02401.x
Baumeister, R. F., & Scher, S. J. (1988). Self-defeating behavior patterns among normal individuals: Review and analysis of common self-destructive tendencies [Journal; Peer Reviewed Journal]. Psychological Bulletin, 104(1), 3–22.
Bazzett, T. J., & Becker, J. B. (1994). Sex differences in the rapid and acute effects of estrogen on striatal D2 dopamine receptor binding. Brain Research, 637(1–2), 163–172.
Bechara, A., Damasio, A. R., Damasio, H., & Anderson, S. W. (1994). Insensitivity to future consequences following damage to human prefrontal cortex. Cognition, 50(1–3), 7–15.
Beesdo, K., Pine, D. S., Lieb, R., & Wittchen, H. U. (2010). Incidence and risk patterns of anxiety and depressive disorders and categorization of generalized anxiety disorder. Archives of General Psychiatry, 67(1), 47–57. https://doi.org/10.1001/archgenpsychiatry.2009.177
Birmaher, B., Brent, D. A., Chiappetta, L., Bridge, J., Monga, S., & Baugher, M. (1999). Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED): A replication study. Journal of the American Academy of Child and Adolescent Psychiatry, 38(10), 1230–1236. https://doi.org/10.1097/00004583-199910000-00011
Birmaher, B., Khetarpal, S., Brent, D., Cully, M., Balach, L., Kaufman, J., & Neer, S. M. (1997). The Screen for Child Anxiety Related Emotional Disorders (SCARED): scale construction and psychometric characteristics. Journal of the American Academy of Child and Adolescent Psychiatry, 36(4), 545–553. https://doi.org/10.1097/00004583-199704000-00018
Box, G. E. P. (1949). A general distribution theory for a class of likelihood criteria. Biometrika, 36, 362–389.
Byrnes, J. P., Miller, D. C., & Schafer, W. D. (1999). Gender differences in risk taking: A meta-analysis [Journal; Peer Reviewed Journal]. Psychological Bulletin, 125(3), 367–383.
Capaldi, D. M., & Rothbart, M. K. (1992). Development and validation of an early adolescent temperament measure. Journal of Early Adolescence, 12(2), 153–173.
Casey, B. J. (2015). Beyond simple models of self-control to circuit-based accounts of adolescent behavior. Annual Review of Psychology, 66, 295–319.
Chaplin, T. M., Sinha, R., Simmons, J. A., Healy, S. M., Mayes, L. C., Hommer, R. E., & Crowley, M. J. (2012). Parent-adolescent conflict interactions and adolescent alcohol use. Addictive Behaviors, 37(5), 605–612. https://doi.org/10.1016/j.addbeh.2012.01.004
Clark, D. M., & Wells, A. (1995). A cognitive model of social phobia. In R. G. Heimberg, M. R. Liebowitz, D. A. Hope, & F. R. Schneier (Eds.), Social phobia: Diagnosis, assessment, and treatment (pp. 69–93). The Guilford Press.
Coffey, S. F., Schumacher, J. A., Baschnagel, J. S., Hawk, L. W., & Holloman, G. (2011). Impulsivity and risk-taking in borderline personality disorder with and without substance use disorders. Personality Disorders, 2(2), 128–141. https://doi.org/10.1037/a0020574
Colder, C. R., Hawk, L. W., Jr., Lengua, L. J., Wiezcorek, W., Eiden, R. D., & Read, J. P. (2013). Trajectories of reinforcement sensitivity during adolescence and risk for substance use. Journal of Research on Adolescence, 23(2), 345–356. https://doi.org/10.1111/jora.12001
Collado, A., Felton, J. W., MacPherson, L., & Lejuez, C. W. (2014). Longitudinal trajectories of sensation seeking, risk taking propensity, and impulsivity across early to middle adolescence. Addictive Behaviors, 39(11), 1580–1588. https://doi.org/10.1016/j.addbeh.2014.01.024
Cooper, M. L., Wood, P. K., Orcutt, H. K., & Albino, A. (2003). Personality and the predisposition to engage in risky or problem behaviors during adolescenc. Journal of Personality and Social Psychology, 84(2), 390–410.
Crone, E. A., van Duijvenvoorde, A. C., & Peper, J. S. (2016). Annual research review: Neural contributions to risk-taking in adolescence–developmental changes and individual differences. Journal of Child Psychology and Psychiatry and Allied Disciplines, 57(3), 353–368. https://doi.org/10.1111/jcpp.12502
Crowley, M. J., & Silverman, W. K. (2016). Coercion dynamics and problematic anxiety in children. In T. J. Dishion & J. Snyder (Eds.), The Oxford handbook of coercive relationship dynamics (pp. 249–259). Oxford University Press.
Eisenberg, A. E., Baron, J., & Seligman, M. E. (1998). Individual differences in risk aversion and anxiety. Psychological Bulletin, 87(1), 245–251.
Ellis, L. S., & Rothbart, M. K. ( 2001). Revision of the early adolescent temperament questionnaire. In Poster presented at the 2001 Biennial Meeting of the Society for Research in Child Development, in Minneapolis, Minnesota.
Eshghi, A., Haughton, D., Legrand, P., Skaletsky, M., & Woolford, S. (2011). Identifying groups: A comparison of methodologies. Journal of Data Science, 9(2), 271–291. https://doi.org/10.6339/jds.2011.09(2).929
Forbes, E. E., Ryan, N. D., Phillips, M. L., Manuck, S. B., Worthman, C. M., Moyles, D. L., Tarr, J. A., Sciarrillo, S. R., & Dahl, R. E. (2010). Healthy adolescents' neural response to reward: associations with puberty, positive affect, and depressive symptoms. Journal of the American Academy of Child and Adolescent Psychiatry, 49(2), 162–172 e161–165. https://www.ncbi.nlm.nih.gov/pubmed/20215938
Fukunaga, R., Bogg, T., Finn, P. R., & Brown, J. W. (2013). Decisions during negatively-framed messages yield smaller risk-aversion-related brain activation in substance-dependent individuals. Psychology of Addictive Behaviors, 27(4), 1141–1152. https://doi.org/10.1037/a0030633
Gadow, K. D., & Sprafkin, J. (1994). Manual for the child symptom inventory (4th ed.). Checkmate Plus.
Gadow, K. D., & Sprafkin, J. (1997). Child symptom inventory (4th ed) norms manual. Checkmate Plus.
Galvan, A. (2010). Adolescent development of the reward system. Frontiers in Human Neuroscience, 4, 6. https://doi.org/10.3389/neuro.09.006.2010
Galván, A. (2013). The teenage brain. Current Directions in Psychological Science, 22(2), 88–93. https://doi.org/10.1177/0963721413480859
Grills-Taquechel, A. E., Norton, P., & Ollendick, T. H. (2010). A longitudinal examination of factors predicting anxiety during the transition to middle school. Anxiety Stress and Coping, 23(5), 493–513. https://doi.org/10.1080/10615800903494127
Groppe, S. E., Gossen, A., Rademacher, L., Hahn, A., Westphal, L., Grunder, G., & Spreckelmeyer, K. N. (2013). Oxytocin influences processing of socially relevant cues in the ventral tegmental area of the human brain [Peer Reviewed]. Biological Psychiatry, 74(3), 172. https://doi.org/10.1016/j.biopsych.2012.12.02323419544
Guyer, A. E., Choate, V. R., Detloff, A., Benson, B., Nelson, E. E., Perez-Edgar, K., Fox, N. A., Pine, D. S., & Ernst, M. (2012). Striatal functional alteration during incentive anticipation in pediatric anxiety disorders. American Journal of Psychiatry, 169(2), 205–212. https://doi.org/10.1176/appi.ajp.2011.11010006
Guyer, A. E., Nelson, E. E., Perez-Edgar, K., Hardin, M. G., Roberson-Nay, R., Monk, C. S., Bjork, J. M., Henderson, H. A., Pine, D. S., Fox, N. A., & Ernst, M. (2006). Striatal functional alteration in adolescents characterized by early childhood behavioral inhibition. Journal of Neuroscience, 26(24), 6399–6405. https://doi.org/10.1523/JNEUROSCI.0666-06.2006
Hale, W. W., 3rd, Raaijmakers, Q., Muris, P., & Meeus, W. (2005). Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED) in the general adolescent population. Journal of the American Academy of Child and Adolescent Psychiatry, 44(3), 283–290. https://doi.org/10.1097/00004583-200503000-00013
Henry, D. B., Tolan, P. H., & Gorman-Smith, D. (2005). Cluster analysis in family psychology research. Journal of Family Psychology, 19(1), 121–132. https://doi.org/10.1037/0893-3200.19.1.121
Hoffman, L. J., Guerry, J. D., & Albano, A. M. (2018, Mar 27). Launching anxious young adults: A specialized cognitive-behavioral intervention for transitional aged youth. Curr Psychiatry Rep, 20(4), 25. https://doi.org/10.1007/s11920-018-0888-9
Hussong, A. M., Jones, D. J., Stein, G. L., Baucom, D. H., & Boeding, S. (2011). An internalizing pathway to alcohol use and disorder. Psychology of Addictive Behaviors, 25(3), 390–404. https://doi.org/10.1037/a0024519
Jinnah, H. A., & Stoneman, Z. (2016). Youth personality factors as predictors of risky all-terrain vehicle (ATV) driving behaviors. Journal of Agricultural Safety and Health, 22(2), 135–147.
Kahneman, D., & Tversky, A. (1990). Prospect theory: An analysis of decision under risk. In P. K. Moser (Ed.), Rationality in action: Contemporary approaches (pp. 140–170). Cambridge University Press.
Kessler, R. C., Angermeyer, M., Anthony, J. C., Demyttenaere, K., Gasquet, I., Gluzman, S., Gureje, O., Haro, J. M., Kawakami, N., Karam, A., Levinson, D., Medina Mora, M. E., Oakley Browne, M. A., Posada-Villa, J., Stein, D. J., Adley Tsang, C. H., Aguilar-Gaxiola, S., Alonso, J., Lee, S., et al. (2007). Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization’s World Mental Health Survey Initiative. World Psychiatry, 6(3), 168–176.
Lago, T., Davis, A., Grillon, C., & Ernst, M. (2017). Striatum on the anxiety map: Small detours into adolescence. Brain Research, 1654(Pt B), 177–184. https://doi.org/10.1016/j.brainres.2016.06.006
Lebowitz, E. R. (2016). “Failure to launch”: Shaping intervention for highly dependent adult children. Journal of the American Academy of Child and Adolescent Psychiatry, 55(2), 89–90. https://doi.org/10.1016/j.jaac.2015.10.014
Lejuez, C. W., Aklin, W., Bornovalova, M., & Moolchan, E. T. (2005). Differences in risk-taking propensity across inner-city adolescent ever- and never-smokers. Nicotine & Tobacco Research, 7(1), 71–79.
Lejuez, C. W., Read, J. P., Kahler, C. W., Richards, J. B., Ramsey, S. E., Stuart, G. L., Strong, D. R., & Brown, R. A. (2002). Evaluation of a behavioral measure of risk taking: The Balloon Analogue Risk Task (BART). Journal of Experimental Psychology: Applied, 8(2), 75–84. https://doi.org/10.1037//1076-898x.8.2.75
Lorian, C. N., & Grisham, J. R. (2011). Clinical implications of risk aversion: An online study of risk-avoidance and treatment utilization in pathological anxiety. Journal of Anxiety Disorders, 25(6), 840–848.
Lorian, C. N., & Grisham, J. R. (2010). The safety bias: Risk-avoidance and social anxiety pathology. Behaviour Change, 27(1), 29–41. https://doi.org/10.1375/bech.27.1.29
MacPherson, L., Reynolds, E. K., Daughters, S. B., Wang, F., Cassidy, J., Mayes, L. C., & Lejuez, C. W. (2010). Positive and negative reinforcement underlying risk behavior in early adolescents. Prevention Science, 11(3), 331–342. https://doi.org/10.1007/s11121-010-0172-7
Maner, J. K., Richey, J. A., Cromer, K., Mallott, M., Lejuez, C. W., Joiner, T. E., & Schmidt, N. B. (2007). Dispositional anxiety and risk-avoidant decision-making. Personality and Individual Differences, 42(4), 665–675. https://doi.org/10.1016/j.paid.2006.08.016
McCormick, E. M., & Telzer, E. H. (2017). Adaptive adolescent flexibility: Neurodevelopment of decision-making and learning in a risky context. Journal of Cognitive Neuroscience, 29(3), 413–423. https://doi.org/10.1162/jocn_a_01061
McEvoy, P. M., & Carleton, R. N. (2016). The wonder and angst of exploring the unknown: Introduction to the special issue on intolerance of uncertainty. Journal of Anxiety Disorders, 41, 1–4. https://doi.org/10.1016/j.janxdis.2016.06.004
McLean, C. P., Asnaani, A., Litz, B. T., & Hofmann, S. G. (2011). Gender differences in anxiety disorders: Prevalence, course of illness, comorbidity and burden of illness. Journal of Psychiatric Research, 45(8), 1027–1035. https://doi.org/10.1016/j.jpsychires.2011.03.006
Miers, A. C., Blöte, A. W., Heyne, D. A., & Westenberg, P. M. (2014). Developmental pathways of social avoidance across adolescence: The role of social anxiety and negative cognition. Journal of Anxiety Disorders, 28(8), 787–794. https://doi.org/10.1016/j.janxdis.2014.09.008
Muris, P., Merckelbach, H., Mayer, B., van Brakel, A., Thissen, S., Moulaert, V., & Gadet, B. (1998). The Screen for Child Anxiety Related Emotional Disorders (SCARED) and traditional childhood anxiety measures. Journal of Behavior Therapy and Experimental Psychiatry, 29(4), 327–339. http://www.ncbi.nlm.nih.gov/pubmed/10037229
Ollendick, T. H., & Hirshfeld-Becker, D. R. (2002). The developmental psychopathology of social anxiety disorder. Biological Psychiatry, 51(1), 44–58.
Otto, M. W., Pollack, M. H., Maki, K. M., Gould, R. A., Worthington, J. J., III., Smoller, J. W., & Rosenbaum, J. F. (2001). Childhood history of anxiety disorders among adults with social phobia: Rates, correlates, and comparisons with patients with panic disorder. Depression and Anxiety, 14(4), 209–213.
Park, H., Yang, J., Vassileva, J., & Ahn, W.-Y. (2021). Development of a novel computational model for the Balloon Analogue Risk Task: The exponential-weight mean–variance model. Journal of Mathematical Psychology. https://doi.org/10.1016/j.jmp.2021.102532
Peper, J. S., Hulshoff Pol, H. E., Crone, E. A., & van Honk, J. (2011). Sex steroids and brain structure in pubertal boys and girls: A mini-review of neuroimaging studies. Neuroscience, 191, 28–37. https://doi.org/10.1016/j.neuroscience.2011.02.014
Petersen, A. C., Crockett, L. J., Richards, M. H., & Boxer, A. M. (1988). Measuring pubertal status: Reliability and validity of a self-report measure. Journal of Youth and Adolescence, 7, 117–133.
Pleskac, T. J., Wallsten, T. S., Wang, P., & Lejuez, C. W. (2008). Development of an automatic response mode to improve the clinical utility of sequential risk-taking tasks. Experimental and Clinical Psychopharmacology, 16(6), 555–564. https://doi.org/10.1037/a0014245
Pleskac, T. J., & Wershbale, A. (2014). Making assessments while taking repeated risks: A pattern of multiple response pathways. Journal of Experimental Psychology: General, 143(1), 142–162. https://doi.org/10.1037/a0031106
Prokasky, A., Rudasill, K., Molfese, V. J., Putnam, S., Gartstein, M., & Rothbart, M. (2017). Identifying child temperament types using cluster analysis in three samples. Journal of Research in Personality. https://doi.org/10.1016/j.jrp.2016.10.008
Rapee, R. M., & Spence, S. H. (2004). The etiology of social phobia: Empirical evidence and an initial model. Clinical Psychology Review, 24(7), 737–767. https://doi.org/10.1016/j.cpr.2004.06.004
Schonberg, T., Fox, C. R., & Poldrack, R. A. (2011). Mind the gap: Bridging economic and naturalistic risk-taking with cognitive neuroscience. Trends in Cognitive Sciences, 15(1), 11–19. https://doi.org/10.1016/j.tics.2010.10.002
Sher, K. J. (2007). Neurobiology of substance dependence: Not just for scientists anymore. PsycCRITIQUES, 52(40), 2007.
Sher, K. J., & Slutske, W. (2003). Disorders of impulse control. In G. Stricker, T. A. Widiger, & I. B. Weiner (Eds.), Comprehensive handbook of psychology (Vol. 8, pp. 195–228). Wiley.
Shoham, R., Sonuga-Barke, E. J., Aloni, H., Yaniv, I., & Pollak, Y. (2016). ADHD-associated risk taking is linked to exaggerated views of the benefits of positive outcomes. Scientific Reports, 6, 34833. https://doi.org/10.1038/srep34833
Solomon, R. L., & Corbit, J. D. (1974). An opponent-process theory of motivation. I. Temporal dynamics of affect. Psychological Review, 81(2), 119–145.
Spreckelmeyer, K. N., Rademacher, L., Paulus, F. M., & Grunder, G. (2013). Neural activation during anticipation of opposite-sex and same-sex faces in heterosexual men and women [Peer Reviewed]. NeuroImage, 66, 223–231. https://doi.org/10.1016/j.neuroimage.2012.10.068
Steinberg, L. (2008). A social neuroscience perspective on adolescent risk-taking. Developmental Review, 28(1), 78–106. https://doi.org/10.1016/j.dr.2007.08.002
Sumter, S. R., Bokhorst, C. L., Miers, A. C., Van Pelt, J., & Westenberg, P. M. (2010). Age and puberty differences in stress responses during a public speaking task: Do adolescents grow more sensitive to social evaluation? Psychoneuroendocrinology, 35(10), 1510–1516. https://doi.org/10.1016/j.psyneuen.2010.05.004
Sumter, S. R., Bokhorst, C. L., & Westenberg, P. M. (2009). Social fears during adolescence: Is there an increase in distress and avoidance? Journal of Anxiety Disorders, 23(7), 897–903. https://doi.org/10.1016/j.janxdis.2009.05.004
Tabachnick, B. G., & Fidell, L. S. (2013). Using multivariate statistics (6th ed.). Boston: Pearson Education.
van Duijvenvoorde, A. C., Peters, S., Braams, B. R., & Crone, E. A. (2016). What motivates adolescents? Neural responses to rewards and their influence on adolescents’ risk taking, learning, and cognitive control. Neuroscience and Biobehavioral Reviews, 70, 135–147. https://doi.org/10.1016/j.neubiorev.2016.06.037
van Oort, F. V., Greaves-Lord, K., Ormel, J., Verhulst, F. C., & Huizink, A. C. (2011). Risk indicators of anxiety throughout adolescence: The TRAILS study. Depression and Anxiety, 28(6), 485–494. https://doi.org/10.1002/da.20818
Walker, J. L., Lahey, B. B., Russo, M. F., Frick, P. J., Christ, M. A. G., McBurnett, K., Loeber, R., Stouthamer-Loeber, M., & Green, S. M. (1991). Anxiety, inhibition, and conduct disorder in children: I. Relations to social impairment. Journal of the American Academy of Child and Adolescent Psychiatry, 30(2), 187–191.
Wallsten, T. S., Pleskac, T. J., & Lejuez, C. W. (2005). Modeling behavior in a clinically diagnostic sequential risk-taking task. Psychological Review, 112(4), 862–880. https://doi.org/10.1037/0033-295X.112.4.862
Wardell, J. D., O’Connor, R. M., Read, J. P., & Colder, C. R. (2011). Behavioral approach system moderates the prospective association between the behavioral inhibition system and alcohol outcomes in college students. Journal of Studies on Alcohol and Drugs, 72(6), 1028–1036. https://doi.org/10.15288/jsad.2011.72.1028
Wechsler, D. (1999). Wechsler abbreviated scale of intelligence. Psychological Corporation.
Wikler, A. (1965). Conditioning factors in opiate addictions and relapse. In D. M. Wilner & G. G. Kassebaum (Eds.), Narcotics (pp. 85–100). McGraw-Hill.
Wills, T. A., Walker, C., Mendoza, D., & Ainette, M. G. (2006). Behavioral and emotional self-control: Relations to substance use in samples of middle and high school students. Psychology of Addictive Behaviors, 20(3), 265–278.
Winkielman, P., Knutson, B., Paulus, M., & Trujillo, J. L. (2007). Affective influence on judgments and decisions: Moving towards core mechanisms. Review of General Psychology, 11(2), 179–192. https://doi.org/10.1037/1089-2680.11.2.179
Wu, J., Phillip, T. M., Doretto, V., van Noordt, S., Chaplin, T. M., Hommer, R. E., Mayes, L. C., & Crowley, M. J. (2019). An inactive control of the 'Trier Social Stress Test' for Youth 10-17 years: Neuroendocrine, cardiac, and subjective responses. Psychoneuroendocrinology, 104, 152–164. https://doi.org/10.1016/j.psyneuen.2019.02.027
Zvolensky, M. J., Bernstein, A., & Marshall, E. C. (2008). Anxiety vulnerability factors and disorders and tobacco and marijuana use and disorders: Emerging theory and research explicating their relations. Addictive Behaviors, 33(11), 1383–1384. https://doi.org/10.1016/j.addbeh.2008.08.005
Acknowledgements
This research was supported by the T32 MH18268 (PJC), NARSAD Young Investigator Award (MJC), Yale Interdisciplinary Research Consortium on Stress, Self-Control and Addiction Pilot project funding (MJC), K01DA034125 (MJC), 1UL1RR024925-01 (R. Sinha); RO1-DA-06025 (LCM), DA017863 (LCM), the Gustavus and Louise Pfeiffer Research Foundation (LCM), and a Natural Sciences and Engineering Research Council of Canada (NSERC) Postdoctoral Fellowship (SJRVN). This publication was also made possible by CTSA Grant Number UL1 RR024139 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of NCRR or NIH.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Conflict of Interest
The authors have no conflicts of interest to declare that are relevant to the content of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Crowley, M.J., van Noordt, S.J.R., Castagna, P.J. et al. Avoidance in Adolescence: The Balloon Risk Avoidance Task (BRAT). J Psychopathol Behav Assess 44, 297–311 (2022). https://doi.org/10.1007/s10862-021-09928-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10862-021-09928-6